
The Role of Prophylactic and Adjuvant Hyperthermic Intraperitoneal Chemotherapy (HIPEC) in Prevention of Peritoneal Metastases in Advanced Colorectal Cancer
Abstract
1. Introduction
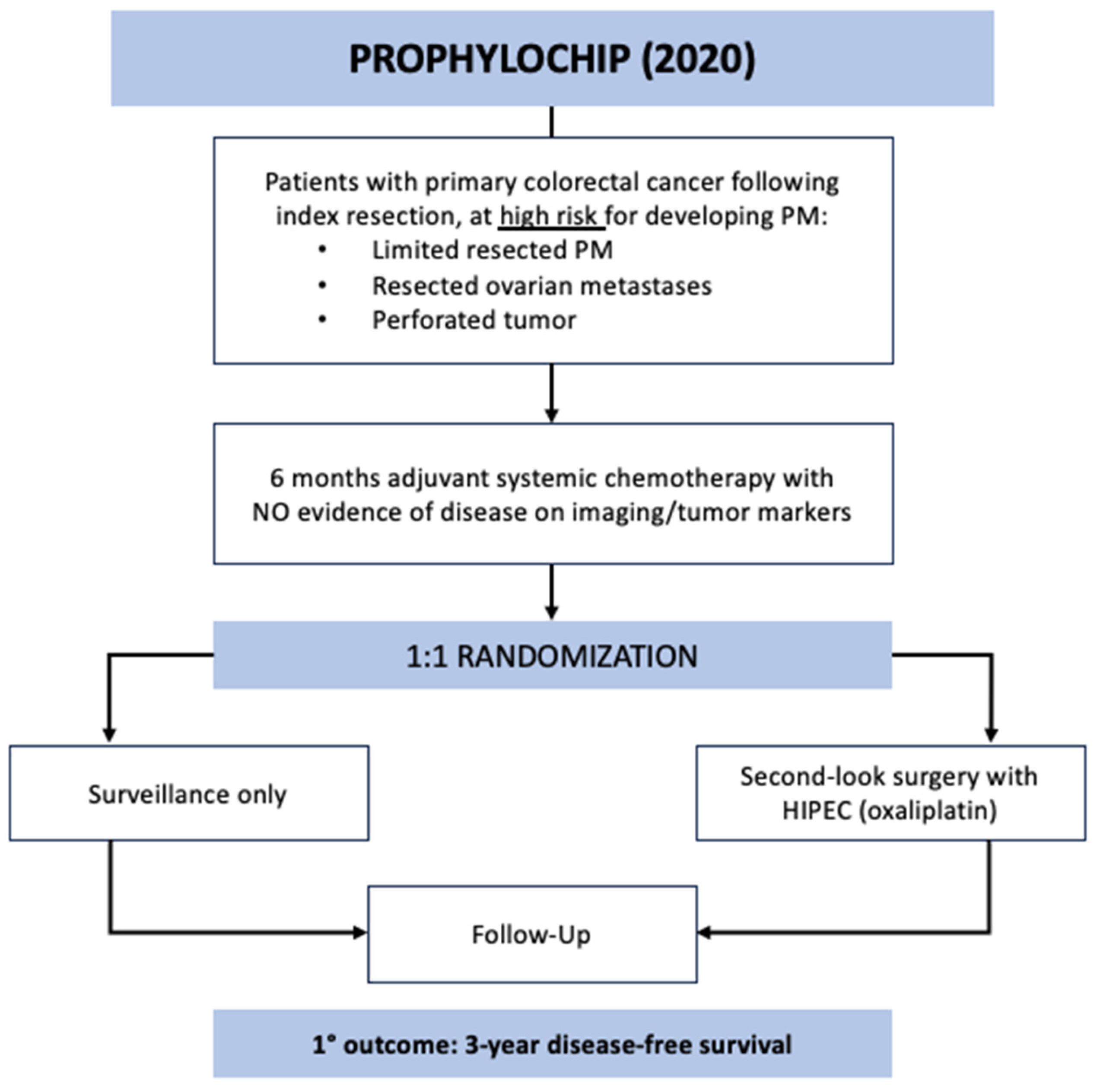
2. PROPHYLOCHIP-PRODIGE 15 (France, 2020)
2.1. Trial Design and Results
2.2. Strengths and Contributions
2.3. Limitations and Discussion
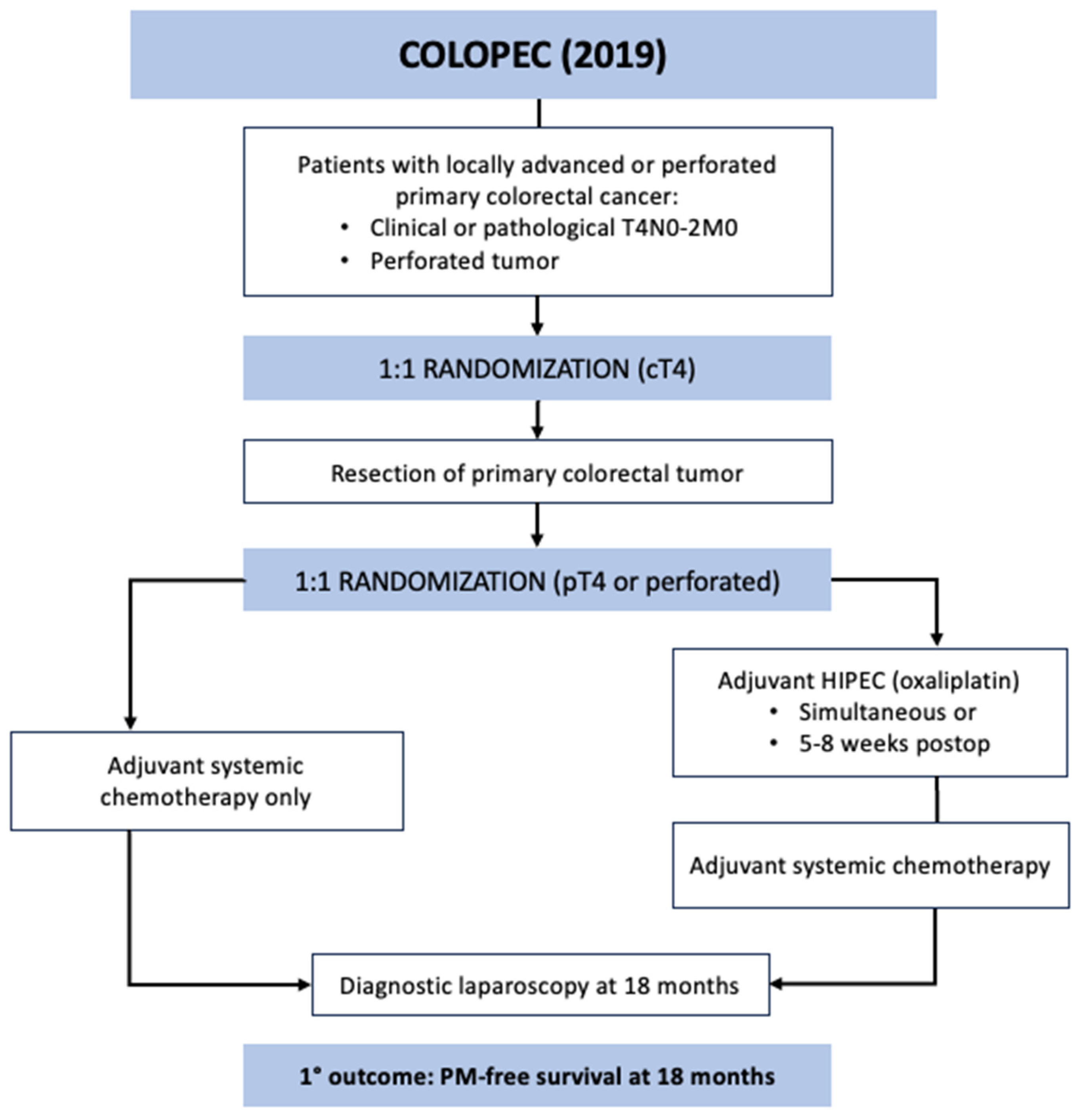
3. COLOPEC (The Netherlands, 2019)
3.1. Trial Design and Results
3.2. Strengths and Contributions
3.3. Limitations and Discussion
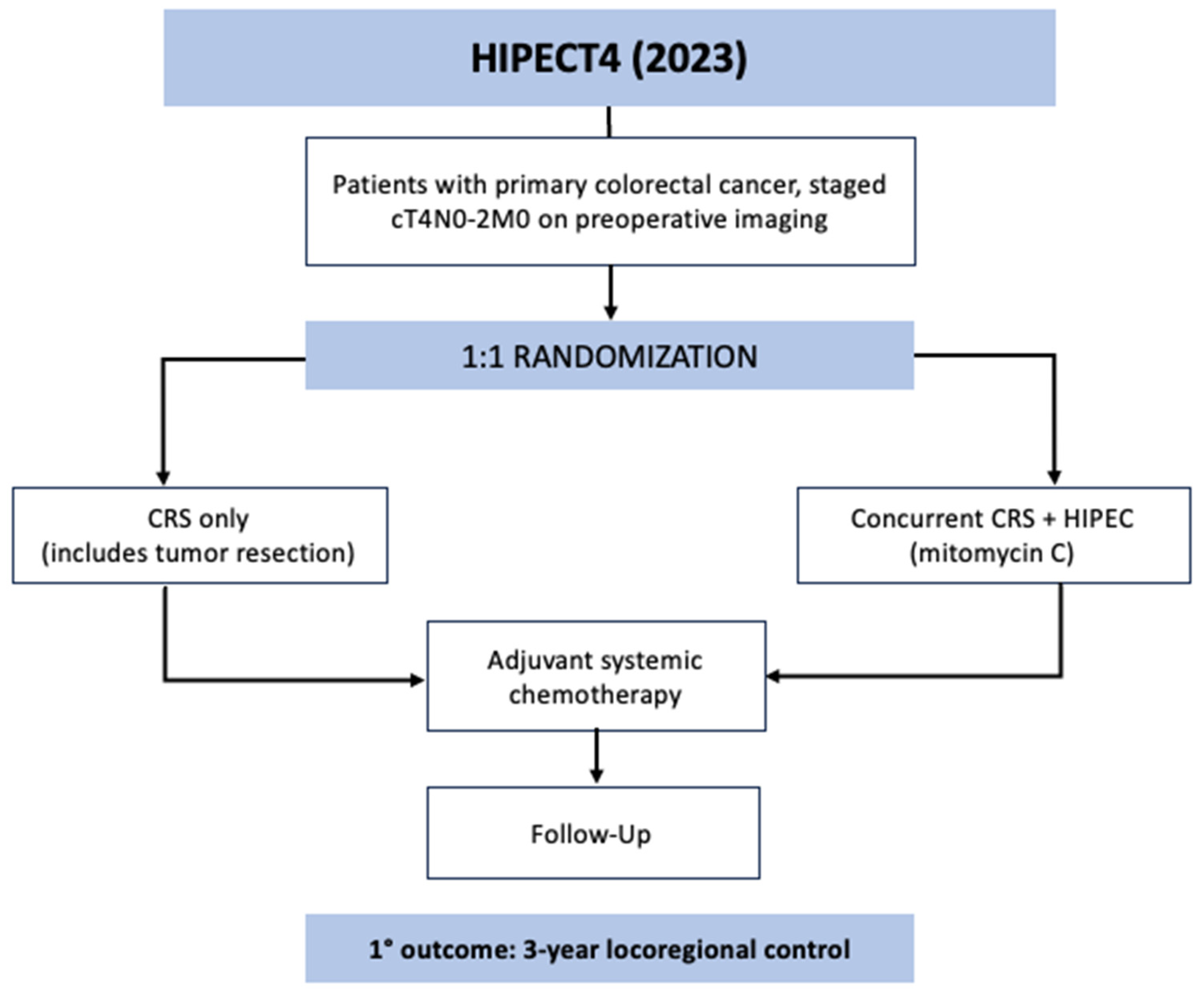
4. HIPECT4 (Spain, 2023)
4.1. Trial Design and Results
4.2. Strengths and Contributions
4.3. Limitations and Discussion
5. Implications and Ongoing Trials
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Segelman, J.; Granath, F.; Holm, T.; Machado, M.; Mahteme, H.; Martling, A. Incidence, prevalence and risk factors for peritoneal carcinomatosis from colorectal cancer. Br. J. Surg. 2012, 99, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Marin, D.; Catalano, C.; Baski, M.; Di Martino, M.; Geiger, D.; Di Giorgio, A.; Sibio, S.; Passariello, R. 64-Section multi-detector row CT in the preoperative diagnosis of peritoneal carcinomatosis: Correlation with histopathological findings. Abdom. Imaging 2010, 35, 694–700. [Google Scholar] [CrossRef] [PubMed]
- Franko, J.; Shi, Q.; Meyers, J.P.; Geiger, D.; Di Giorgio, A.; Sibio, S.; Passariello, R. Prognosis of patients with peritoneal metastatic colorectal cancer given systemic therapy: An analysis of individual patient data from prospective randomised trials from the Analysis and Research in Cancers of the Digestive System (ARCAD) database. Lancet Oncol. 2016, 17, 1709–1719. [Google Scholar] [CrossRef] [PubMed]
- Franko, J. Therapeutic efficacy of systemic therapy for colorectal peritoneal carcinomatosis: Surgeon’s perspective. Pleura Peritoneum 2018, 3, 20180102. [Google Scholar] [CrossRef]
- Quénet, F.; Elias, D.; Roca, L.; Goéré, D.; Ghouti, L.; Pocard, M.; Facy, O.; Arvieux, C.; Lorimier, G.; Pezet, D.; et al. Cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy versus cytoreductive surgery alone for colorectal peritoneal metastases (PRODIGE 7): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 256–266. [Google Scholar] [CrossRef]
- Verwaal, V.J.; van Ruth, S.; de Bree, E.; van Slooten, G.W.; van Tinteren, H.; Boot, H.; Zoetmulder, F.A. Randomized Trial of Cytoreduction and Hyperthermic Intraperitoneal Chemotherapy Versus Systemic Chemotherapy and Palliative Surgery in Patients With Peritoneal Carcinomatosis of Colorectal Cancer. J. Clin. Oncol. 2003, 21, 3737–3743. [Google Scholar] [CrossRef]
- Glehen, O.; Kwiatkowski, F.; Sugarbaker, P.H.; Elias, D.; Levine, E.A.; De Simone, M.; Barone, R.; Yonemura, Y.; Cavaliere, F.; Quenet, F.; et al. Cytoreductive Surgery Combined With Perioperative Intraperitoneal Chemotherapy for the Management of Peritoneal Carcinomatosis From Colorectal Cancer: A Multi-Institutional Study. J. Clin. Oncol. 2004, 22, 3284–3292. [Google Scholar] [CrossRef]
- Van De Vlasakker, V.C.J.; Lurvink, R.J.; Cashin, P.H.; Ceelen, W.; Deraco, M.; Goéré, D.; González-Moreno, S.; Lehmann, K.; Li, Y.; Moran, B.; et al. The impact of PRODIGE 7 on the current worldwide practice of CRS-HIPEC for colorectal peritoneal metastases: A web-based survey and 2021 statement by Peritoneal Surface Oncology Group International (PSOGI). Eur. J. Surg. Oncol. 2021, 47, 2888–2892. [Google Scholar] [CrossRef]
- Goéré, D.; Malka, D.; Tzanis, D.; Gava, V.; Boige, V.; Eveno, C.; Maggiori, L.; Dumont, F.; Ducreux, M.; Elias, D. Is There a Possibility of a Cure in Patients With Colorectal Peritoneal Carcinomatosis Amenable to Complete Cytoreductive Surgery and Intraperitoneal Chemotherapy? Ann. Surg. 2013, 257, 1065–1071. [Google Scholar] [CrossRef]
- Honoré, C.; Goéré, D.; Souadka, A.; Dumont, F.; Elias, D. Definition of Patients Presenting a High Risk of Developing Peritoneal Carcinomatosis After Curative Surgery for Colorectal Cancer: A Systematic Review. Ann. Surg. Oncol. 2013, 20, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Honoré, C.; Gelli, M.; Francoual, J.; Benhaim, L.; Elias, D.; Goéré, D. Ninety percent of the adverse outcomes occur in 10% of patients: Can we identify the populations at high risk of developing peritoneal metastases after curative surgery for colorectal cancer? Int. J. Hyperth. 2017, 33, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Sammartino, P.; Sibio, S.; Biacchi, D.; Cardi, M.; Accarpio, F.; Mingazzini, P.; Rosati, M.S.; Cornali, T.; Di Giorgio, A. Prevention of Peritoneal Metastases from Colon Cancer in High-Risk Patients: Preliminary Results of Surgery plus Prophylactic HIPEC. Gastroenterol. Res. Pract. 2012, 2012, 141585. [Google Scholar] [CrossRef]
- Sammartino, P.; Sibio, S.; Biacchi, D.; Cardi, M.; Mingazzini, P.; Rosati, M.S.; Cornali, T.; Sollazzo, B.; Atta, J.M.; Di Giorgio, A. Long-term results after proactive management for locoregional control in patients with colonic cancer at high risk of peritoneal metastases. Int. J. Color. Dis. 2014, 29, 1081–1089. [Google Scholar] [CrossRef]
- Baratti, D.; Kusamura, S.; Iusco, D.; Gimondi, S.; Pietrantonio, F.; Milione, M.; Guaglio, M.; Bonomi, S.; Grassi, A.; Virzì, S.; et al. Hyperthermic Intraperitoneal Chemotherapy (HIPEC) at the Time of Primary Curative Surgery in Patients with Colorectal Cancer at High Risk for Metachronous Peritoneal Metastases. Ann. Surg. Oncol. 2017, 24, 167–175. [Google Scholar] [CrossRef]
- Klaver, C.E.L.; Stam, R.; Sloothaak, D.A.M.; Crezee, J.; Bemelman, W.A.; Punt, C.J.; Tanis, P.J. Colorectal cancer at high risk of peritoneal metastases: Long term outcomes of a pilot study on adjuvant laparoscopic HIPEC and future perspectives. Oncotarget 2017, 8, 51200–51209. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Elias, D.; Honoré, C.; Dumont, F.; Ducreux, M.; Boige, V.; Malka, D.; Burtin, P.; Dromain, C.; Goéré, D. Results of Systematic Second-look Surgery Plus HIPEC in Asymptomatic Patients Presenting a High Risk of Developing Colorectal Peritoneal Carcinomatosis. Ann. Surg. 2011, 254, 289–293. [Google Scholar] [CrossRef] [PubMed]
- Goéré, D.; Glehen, O.; Quenet, F.; Guilloit, J.-M.; Bereder, J.-M.; Lorimier, G.; Thibaudeau, E.; Ghouti, L.; Pinto, A.; Tuech, J.-J.; et al. Second-look surgery plus hyperthermic intraperitoneal chemotherapy versus surveillance in patients at high risk of developing colorectal peritoneal metastases (PROPHYLOCHIP-PRODIGE 15): A randomised, phase 3 study. Lancet Oncol. 2020, 21, 1147–1154. [Google Scholar] [CrossRef]
- Cashin, P.; Sugarbaker, P.H. Hyperthermic intraperitoneal chemotherapy (HIPEC) for colorectal and appendiceal peritoneal metastases: Lessons learned from PRODIGE 7. J. Gastrointest. Oncol. 2021, 12 (Suppl. S1), S120–S128. [Google Scholar] [CrossRef]
- Van Eden, W.J.; Kok, N.F.M.; Woensdregt, K.; Huitema, A.D.R.; Boot, H.; Aalbers, A.G.J. Safety of intraperitoneal Mitomycin C versus intraperitoneal oxaliplatin in patients with peritoneal carcinomatosis of colorectal cancer undergoing cytoreductive surgery and HIPEC. Eur. J. Surg. Oncol. 2018, 44, 220–227. [Google Scholar] [CrossRef]
- Leung, V.; Huo, Y.R.; Liauw, W.; Morris, D.L. Oxaliplatin versus Mitomycin C for HIPEC in colorectal cancer peritoneal carcinomatosis. Eur. J. Surg. Oncol. 2017, 43, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Benzaquen, E.; Wang, Y.; Wiseman, S.; Rosenfeld, V.; Sideris, L.; Dubé, P.; Pelletier, J.-S.; Vanounou, T. Morbidity associated with the use of oxaliplatin versus mitomycin C in hyperthermic intraperitoneal chemotherapy (HIPEC) for peritoneal carcinomatosis of colorectal or appendiceal origin: A multi-institutional comparative study. Cancer J. Surg. 2021, 64, E111–E118. [Google Scholar] [CrossRef] [PubMed]
- Prabhu, A.; Brandl, A.; Wakama, S.; Rosenfeld, V.; Sideris, L.; Dubé, P.; Pelletier, J.-S.; Vanounou, T. Effect of oxaliplatin-based chemotherapy on chemosensitivity in patients with peritoneal metastasis from colorectal cancer treated with cytoreductive surgery and hyperthermic intraperitoneal chemotherapy: Proof-of-concept study. BJS Open 2021, 5, zraa075. [Google Scholar] [CrossRef] [PubMed]
- Nagourney, R.A.; Evans, S.; Tran, P.H.; Nagourney, A.J.; Sugarbaker, P.H. Colorectal cancer cells from patients treated with FOLFOX or CAPOX are resistant to oxaliplatin. Eur. J. Surg. Oncol. 2021, 47, 738–742. [Google Scholar] [CrossRef]
- Strohlein, M.A.; Heiss, M.M. Limitations of the PRODIGE 7 trial. Lancet Oncol. 2021, 22, e178. [Google Scholar] [CrossRef]
- Delhorme, J.B.; Triki, E.; Romain, B.; Meyer, N.; Rohr, S.; Brigand, C. Routine second-look after surgical treatment of colonic peritoneal carcinomatosis. J. Visc. Surg. 2015, 152, 149–154. [Google Scholar] [CrossRef]
- Cortes-Guiral, D.; Elias, D.; Cascales-Campos, P.A.; Yébenes, A.B.; Castellano, I.G.; Carbonero, A.I.L.; Valadés, J.I.M.; Garcia-Foncillas, J.; Garcia-Olmo, D. Second-look surgery plus hyperthermic intraperitoneal chemotherapy for patients with colorectal cancer at high risk of peritoneal carcinomatosis: Does it really save lives? World J. Gastroenterol. 2017, 23, 377–381. [Google Scholar] [CrossRef]
- Passot, G.; Dumont, F.; Goéré, D.; Arvieux, C.; Rousset, P.; Regimbeau, J.; Elias, D.; Villeneuve, L.; Glehen, O.; Abba, J.; et al. Multicentre study of laparoscopic or open assessment of the peritoneal cancer index (BIG-RENAPE). Br. J. Surg. 2018, 105, 663–667. [Google Scholar] [CrossRef]
- Elkrief, A.; Redstone, G.; Petruccelli, L.; Ali, A.; Thomas, D.; Fernandez, M.; Rousseau, C.; Aleynikova, O.; Anderson, D.; Ghitulescu, G.; et al. Reasons for delay in timely administration of adjuvant chemotherapy for patients with stage III colon cancer: A multicentre cohort study from the McGill University Department of Oncology. BMJ Open Qual. 2021, 10, e000934. [Google Scholar] [CrossRef]
- Klaver, C.E.L.; Wisselink, D.D.; Punt, C.J.A.; Snaebjornsson, P.; Crezee, J.; Aalbers, A.G.J.; Brandt, A.; Bremers, A.J.A.; Burger, J.W.A.; Fabry, H.F.J.; et al. Adjuvant hyperthermic intraperitoneal chemotherapy in patients with locally advanced colon cancer (COLOPEC): A multicentre, open-label, randomised trial. Lancet Gastroenterol. Hepatol. 2019, 4, 761–770. [Google Scholar] [CrossRef]
- Ozcelik, M.; Oyman, A.; Cil, I.; Duzgun, O.; Ozkan, O.F.; Ayhan, M. Cytoreductive Surgery versus Systemic Chemotherapy alone in Isolated Peritoneal Carcinomatosis of Colorectal Origin. J. Coll. Physicians Surg. Pak. 2021, 31, 1308–1313. [Google Scholar] [CrossRef] [PubMed]
- Glehen, O.; Osinsky, D.; Cotte, E.; Kwiatkowski, F.; Freyer, G.; Isaac, S.; Trillet-Lenoir, V.; Sayag-Beaujard, A.C.; François, Y.; Vignal, J.; et al. Intraperitoneal Chemohyperthermia Using a Closed Abdominal Procedure and Cytoreductive Surgery for the Treatment of Peritoneal Carcinomatosis: Morbidity and Mortality Analysis of 216 Consecutive Procedures. Ann. Surg. Oncol. 2003, 10, 863–869. [Google Scholar] [CrossRef] [PubMed]
- Webb, C.; Day, R.; Velazco, C.S.; Pockaj, B.A.; Gray, R.J.; Stucky, C.-C.; Young-Fadok, T.; Wasif, N. Implementation of an Enhanced Recovery After Surgery (ERAS) Program is Associated with Improved Outcomes in Patients Undergoing Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy. Ann. Surg. Oncol. 2020, 27, 303–312. [Google Scholar] [CrossRef]
- Foster, J.M.; Sleightholm, R.; Patel, A.; Shostrom, V.; Hall, B.; Neilsen, B.; Bartlett, D.; Smith, L. Morbidity and Mortality Rates Following Cytoreductive Surgery Combined With Hyperthermic Intraperitoneal Chemotherapy Compared With Other High-Risk Surgical Oncology Procedures. JAMA Netw. Open 2019, 2, e186847. [Google Scholar] [CrossRef] [PubMed]
- Berger, Y.; Jacoby, H.; Kaufmann, M.I.; Ben-Yaacov, A.; Westreich, G.; Sharon, I.; Barda, L.; Sharif, N.; Nadler, R.; Horesh, N.; et al. Correlation Between Intraoperative and Pathological Findings for Patients Undergoing Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy. Ann. Surg. Oncol. 2019, 26, 1103–1109. [Google Scholar] [CrossRef] [PubMed]
- Benson, A.B. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines)—Colon Cancer. Natl. Compr. Cancer Netw. 2023, 2, 2023. Available online: https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf (accessed on 16 July 2023).
- Lemoine, L.; Sugarbaker, P.; Van der Speeten, K. Pathophysiology of colorectal peritoneal carcinomatosis: Role of the peritoneum. World J. Gastroenterol. 2016, 22, 7692–7707. [Google Scholar] [CrossRef]
- Shen, P.; Stewart, J.H.; Levine, E.A. Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy for Peritoneal Surface Malignancy: Overview and Rationale. Curr. Probl. Cancer 2009, 33, 125–141. [Google Scholar] [CrossRef]
- Yan, T.D. A pharmacological review on intraperitoneal chemotherapy for peritoneal malignancy. World J. Gastrointest. Oncol. 2010, 2, 109–116. [Google Scholar] [CrossRef]
- González-Moreno, S. Hyperthermic intraperitoneal chemotherapy: Rationale and technique. World J. Gastrointest. Oncol. 2010, 2, 68. [Google Scholar] [CrossRef]
- Arjona-Sánchez, A.; Espinosa-Redondo, E.; Gutiérrez-Calvo, A.; Segura-Sampedro, J.J.; Pérez-Viejo, E.; Concepción-Martín, V.; Sánchez-García, S.; García-Fadrique, A.; Prieto-Nieto, I.; Barrios-Sanchez, P.; et al. Efficacy and Safety of Intraoperative Hyperthermic Intraperitoneal Chemotherapy for Locally Advanced Colon Cancer: A Phase 3 Randomized Clinical Trial. JAMA Surg. 2023, 158, 683–691. [Google Scholar] [CrossRef]
- Vatandoust, S.; Price, T.J.; Karapetis, C.S. Colorectal cancer: Metastases to a single organ. World J. Gastroenterol. 2015, 21, 11767–11776. [Google Scholar] [CrossRef]
- Kow, A.W.C. Hepatic metastasis from colorectal cancer. J. Gastrointest. Oncol. 2019, 10, 1274–1298. [Google Scholar] [CrossRef]
- Patel, C.M.; Sahdev, A.; Reznek, R.H. CT, MRI and PET imaging in peritoneal malignancy. Cancer Imaging 2011, 11, 123–139. [Google Scholar] [CrossRef]
- Dromain, C.; Leboulleux, S.; Auperin, A.; Goere, D.; Malka, D.; Lumbroso, J.; Schumberger, M.; Sigal, R.; Elias, D. Staging of peritoneal carcinomatosis: Enhanced CT vs. PET/CT. Abdom. Imaging 2008, 33, 87–93. [Google Scholar] [CrossRef]
- Zwanenburg, E.S.; Wisselink, D.D.; Klaver, C.E.L.; Brandt, A.R.M.; Bremers, A.J.A.; Burger, J.W.A.; van Grevenstein, W.M.U.; Hemmer, P.H.J.; de Hingh, I.H.J.T.; Kok, N.F.M.; et al. Adhesion formation after surgery for locally advanced colonic cancer in the COLOPEC trial. Br. J. Surg. 2022, 109, 315–318. [Google Scholar] [CrossRef]
- Moris, D.; Chakedis, J.; Rahnemai-Azar, A.A.; Wilson, A.; Hennessy, M.M.; Athanasiou, A.; Beal, E.W.; Argyrou, C.; Felekouras, E.; Pawlik, T.M. Postoperative Abdominal Adhesions: Clinical Significance and Advances in Prevention and Management. J. Gastrointest. Surg. 2017, 21, 1713–1722. [Google Scholar] [CrossRef]
- Arung, W.; Meurisse, M.; Detry, O. Pathophysiology and prevention of postoperative peritoneal adhesions. World J. Gastroenterol. 2011, 17, 4545–4553. [Google Scholar] [CrossRef]
- Ellis, H.; Moran, B.J.; Thompson, J.N.; Parker, M.C.; Wilson, M.S.; Menzies, D.; McGuire, A.; Lower, A.M.; Hawthorn, R.J.; O’Brien, F.; et al. Adhesion-related hospital readmissions after abdominal and pelvic surgery: A retrospective cohort study. Lancet 1999, 353, 1476–1480. [Google Scholar] [CrossRef]
- Parker, M.C.; Wilson, M.S.; Menzies, D.; Sunderland, G.; Clark, D.N.; Knight, A.D.; Crowe, A.M.; The Surgical and Clinical Adhesions Research (SCAR) Group. The SCAR-3 study: 5-year adhesion-related readmission risk following lower abdominal surgical procedures. Color. Dis. 2005, 7, 551–558. [Google Scholar] [CrossRef]
- Ten Broek, R.P.G.; Issa, Y.; van Santbrink, E.J.P.; Bouvy, N.D.; Kruitwagen, R.F.P.M.; Jeekel, J.; Bakkum, E.A.; Rovers, M.M.; van Goor, H. Burden of adhesions in abdominal and pelvic surgery: Systematic review and met-analysis. BMJ 2013, 347, f5588. [Google Scholar] [CrossRef]
- Van Der Krabben, A.A.; Dijkstra, F.R.; Nieuwenhuijzen, M.; Reijnen, M.M.P.J.; Schaapveld, M.; Van Goor, H. Morbidity and mortality of inadvertent enterotomy during adhesiotomy. Br. J. Surg. 2002, 87, 467–471. [Google Scholar] [CrossRef]
- Ouaïssi, M.; Gaujoux, S.; Veyrie, N.; Denève, E.; Brigand, C.; Castel, B.; Duron, J.; Rault, A.; Slim, K.; Nocca, D. Post-operative adhesions after digestive surgery: Their incidence and prevention: Review of the literature. J. Visc. Surg. 2012, 149, e104–e114. [Google Scholar] [CrossRef]
- Goodman, M.D.; McPartland, S.; Detelich, D.; Saif, M.W. Chemotherapy for intraperitoneal use: A review of hyperthermic intraperitoneal chemotherapy and early post-operative intraperitoneal chemotherapy. J. Gastrointest. Oncol. 2016, 7, 45–57. [Google Scholar]
- Raa, S.T.; Oosterling, S.J.; van der Kaaij, N.P.; Tol, M.v.D.; Beelen, R.; Meijer, S.; van Eijck, C.; van der Sijp, J.; van Egmond, M.; Jeekel, J. Surgery promotes implantation of disseminated tumor cells, but does not increase growth of tumor cell clusters. J. Surg. Oncol. 2005, 92, 124–129. [Google Scholar] [CrossRef]
- Sugarbaker, P.H. Peritoneum as the first-line of defense in carcinomatosis. J. Surg. Oncol. 2007, 95, 93–96. [Google Scholar] [CrossRef]
- Segura-Sampedro, J.J.; Morales-Soriano, R. Prophylactic HIPEC with oxaliplatin might be of benefit in T4 and perforated colon cancer: Another possible interpretation of the COLOPEC results. Rev. Esp. Enferm. Dig. 2020, 112, 666. [Google Scholar] [CrossRef]
- Bonavina, L.; Incarbone, R.; Lattuada, E.; Segalin, A.; Cesana, B.; Peracchia, A. Preoperative laparoscopy in management of patients with carcinoma of the esophagus and of the esophagogastric junction. J. Surg. Oncol. 1997, 65, 171–174. [Google Scholar] [CrossRef]
- Contreras, C.M.; Stanelle, E.J.; Mansour, J.; Hinshaw, J.L.; Rikkers, L.F.; Rettammel, R.; Mahvi, D.M.; Cho, C.S.; Weber, S.M. Staging laparoscopy enhances the detection of occult metastases in patients with pancreatic adenocarcinoma. J. Surg. Oncol. 2009, 100, 663–669. [Google Scholar] [CrossRef]
- Helderman, R.F.C.P.A.; Löke, D.R.; Verhoeff, J.; Rodermond, H.M.; van Bochove, G.G.; Boon, M.; van Kesteren, S.; Vallejo, J.J.G.; Kok, H.P.; Tanis, P.J.; et al. The Temperature-Dependent Effectiveness of Platinum-Based Drugs Mitomycin-C and 5-FU during Hyperthermic Intraperitoneal Chemotherapy (HIPEC) in Colorectal Cancer Cell Lines. Cells 2020, 9, 1775. [Google Scholar] [CrossRef]
- Pereira, F.; Serrano, A.; Manzanedo, I.; Pérez-Viejo, E.; González-Moreno, S.; González-Bayón, L.; Arjona-Sánchez, A.; Torres, J.; Ramos, I.; Barrios, M.E.; et al. GECOP-MMC: Phase IV randomized clinical trial to evaluate the efficacy of hyperthermic intraperitoneal chemotherapy (HIPEC) with mytomicin-C after complete surgical cytoreduction in patients with colon cancer peritoneal metastases. BMC Cancer 2022, 22, 536. [Google Scholar] [CrossRef]
- Klaver, C.E.L.; Gietelink, L.; Bemelman, W.A.; Wouters, M.W.; Wiggers, T.; Tollenaar, R.A.; Tanis, P.J.; on behalf of the Dutch Surgical Colorectal Audit Group. Locally Advanced Colon Cancer: Evaluation of Current Clinical Practice and Treatment Outcomes at the Population Level. J. Nat. Compr. Cancer Netw. 2017, 15, 181–190. [Google Scholar] [CrossRef]
- Kim, S.; Huh, J.W.; Lee, W.Y.; Yun, S.H.; Kim, H.C.; Cho, Y.B.; Park, Y.A.; Shin, J.K. Oncologic outcomes of pathologic T4 and T3 colon cancer patients diagnosed with clinical T4 stage disease using preoperative computed tomography scan. Surg. Oncol. 2022, 41, 101749. [Google Scholar] [CrossRef]
- Nakafusa, Y.M.D.; Tanaka, T.M.D.; Tanaka, M.M.D.; Kitajima, Y.M.D.; Sato, S.M.D.; Miyazaki, K.M.D. Comparison of Multivisceral Resection and Standard Operation for Locally Advanced Colorectal Cancer: Analysis of Prognostic Factors for Short-Term and Long-Term Outcome. Dis. Colon Rectum. 2004, 47, 2055–2063. [Google Scholar] [CrossRef]
- Dubé, P.; Sideris, L.; Law, C.; Mack, L.; Haase, E.; Giacomantonio, C.; Govindarajan, A.; Krzyzanowska, M.; Major, P.; McConnell, Y.; et al. Guidelines on the use of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in patients with peritoneal surface malignancy arising from colorectal or appendiceal neoplasms. Curr. Oncol. 2015, 22, e100–e112. [Google Scholar] [CrossRef]
- Sueda, T.; Tei, M.; Nishida, K.; Yoshikawa, Y.; Matsumura, T.; Koga, C.; Wakasugi, M.; Miyagaki, H.; Kawabata, R.; Tsujie, M.; et al. Oncological outcomes following laparoscopic surgery for pathological T4 colon cancer: A propensity score-matched analysis. Surg. Today 2021, 51, 404–414. [Google Scholar] [CrossRef]
- Aoki, T.; Matsuda, T.; Hasegawa, H.; Yamashita, K.; Sumi, Y.; Ishida, R.; Yamamoto, M.; Kanaji, S.; Oshikiri, T.; Nakamura, T.; et al. Outcomes of laparoscopic surgery for pathological T4 colon cancer. Int. J. Color. Dis. 2019, 34, 1259–1265. [Google Scholar] [CrossRef]
- Levine, E.A.; Votanopoulos, K.I.; Shen, P.; Russell, G.; Fenstermaker, J.; Mansfield, P.; Bartlett, D.; Stewart, J.H. A Multi-Center Randomized Trial to Evaluate Hematologic Toxicities after Hyperthermic Intraperitoneal Chemotherapy with Oxaliplatin or Mitomycin in Patients with Appendiceal Tumors. J. Am. Coll. Surg. 2018, 226, 434–443. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Trial | Study Type | Patient Selection | Trial Arms | HIPEC Regimen | Primary End Point and Findings |
|---|---|---|---|---|---|
| PROPHYLOCHIP (France) | Phase III RCT: 2010–2015 Adjuvant HIPEC | High risk (resected limited PM or ovarian metastases, perforated tumor); 6 months adjuvant chemotherapy with no evidence of recurrence | Surveillance only vs. Second-look surgery with CRS–HIPEC | Oxaliplatin (460 mg/m2 or 300–360 mg/m2 + irinotecan) for 30 min | 3-year disease-free survival No significant difference (53% vs. 44%, p = 0.82) |
| COLOPEC (The Netherlands) | Phase III RCT: 2015–2017 Adjuvant HIPEC | Locally advanced or perforated colorectal cancer (clinical or pathologic T4N02M0) | Adjuvant chemotherapy only vs. Adjuvant HIPEC followed by chemotherapy | Oxaliplatin (460 mg/m2) for 30 min | 18-month PM-free survival No significant difference (76.2% vs. 80.9%, p = 0.28) |
| HIPECT4 (Spain) | Phase III RCT: 2015–2021 Prophylactic HIPEC | Locally advanced colon cancer (clinical T4N02M0) | CRS only vs. Concurrent CRS–HIPEC | Mitomycin C (30 mg/m2) for 60 min | 3-year locoregional control (LC) Improved LC rate after HIPEC (97.6% vs. 87.6%, p = 0.03) |
| Trial | Study Type | Projected Inclusion and Enrollment | Trial Arms | HIPEC Regimen | Primary End Point |
|---|---|---|---|---|---|
| (China) NCT02179489 | Phase III RCT, Adjuvant HIPEC | Colorectal cancer: cT4, perforation, minimal PM, or ovarian metastases; after surgical resection + 6 months chemotherapy 271 total, randomized into 2 arms | Surveillance only vs. Second look surgery with HIPEC | Mitomycin C (30 mg/m2) for 60 min | Disease-free survival (3 years) |
| APEC Study (China) NCT02965248 | Phase III RCT, Prophylactic HIPEC | Colorectal cancer: any cT4 or cT3 with mucinous or signet ring cell 147 total, randomized | Surgery + adjuvant chemotherapy vs. Surgery with HIPEC + adjuvant chemotherapy | Raltitrexed (3 mg/m2) for 60 min or Oxaliplatin (130 mg/m2) for 30 min | Rate of PM (3 years) |
| CHECK Study (Italy) NCT03914820 | Phase III RCT, Prophylactic HIPEC | Colorectal cancer: cT4, perforation, limited peritumor PM, or ovarian metastases 330 total, randomized into 2 arms | Standard surgery + adjuvant chemotherapy vs. Prophylactic surgery + HIPEC CO2 | Mitomycin C (35 mg/m2) for 60 min | Local recurrence-free survival (3 years) |
| (China) NCT04370925 | Phase III RCT, Prophylactic HIPEC | Colorectal cancer: cT4N0-2M0 without perforation 688 total, randomized into 2 arms | Surgery + adjuvant chemotherapy vs. Surgery with HIPEC + adjuvant chemotherapy | Mitomycin C (30 mg/m2) for 90 min | PM-free survival (3 years) |
| WUHIPEC02 (China) NCT04845490 | Phase II RCT, Prophylactic HIPEC | Colorectal cancer: cT3 or cT4 without metastases 201 total, randomized into 3 arms | Surgery with hyperthermic saline (repeat at 48 h) + chemotherapy vs. Surgery with HIPEC (repeat at 48 h) + chemotherapy | Mitomycin C (30 mg/m2) for 60 min or Lobaplatin (50 mg/m2) 60 min | PM-free survival (3 years) |
| PROMENADE (Italy) NCT02974556 | Phase III RCT, Prophylactic HIPEC | Colorectal cancer: cT3 or cT4 without metastases undergoing curative resection 140 total, randomized into 2 arms | Standard surgery + adjuvant chemotherapy vs. Extensive cytoreduction with HIPEC + adjuvant chemotherapy | Oxaliplatin (460 mg/m2) for 30 min | Rate of PM (3 years) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, B.J.; Daniel, S.K.; Lee, B. The Role of Prophylactic and Adjuvant Hyperthermic Intraperitoneal Chemotherapy (HIPEC) in Prevention of Peritoneal Metastases in Advanced Colorectal Cancer. J. Clin. Med. 2023, 12, 6443. https://doi.org/10.3390/jcm12206443
Sun BJ, Daniel SK, Lee B. The Role of Prophylactic and Adjuvant Hyperthermic Intraperitoneal Chemotherapy (HIPEC) in Prevention of Peritoneal Metastases in Advanced Colorectal Cancer. Journal of Clinical Medicine. 2023; 12(20):6443. https://doi.org/10.3390/jcm12206443
Chicago/Turabian StyleSun, Beatrice J., Sara K. Daniel, and Byrne Lee. 2023. "The Role of Prophylactic and Adjuvant Hyperthermic Intraperitoneal Chemotherapy (HIPEC) in Prevention of Peritoneal Metastases in Advanced Colorectal Cancer" Journal of Clinical Medicine 12, no. 20: 6443. https://doi.org/10.3390/jcm12206443
APA StyleSun, B. J., Daniel, S. K., & Lee, B. (2023). The Role of Prophylactic and Adjuvant Hyperthermic Intraperitoneal Chemotherapy (HIPEC) in Prevention of Peritoneal Metastases in Advanced Colorectal Cancer. Journal of Clinical Medicine, 12(20), 6443. https://doi.org/10.3390/jcm12206443