
Targeted Radiation Exposure Induces Accelerated Aortic Valve Remodeling in ApoE−/− Mice
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Three-Dimensional Anatomic Atlas of Aortic Valve
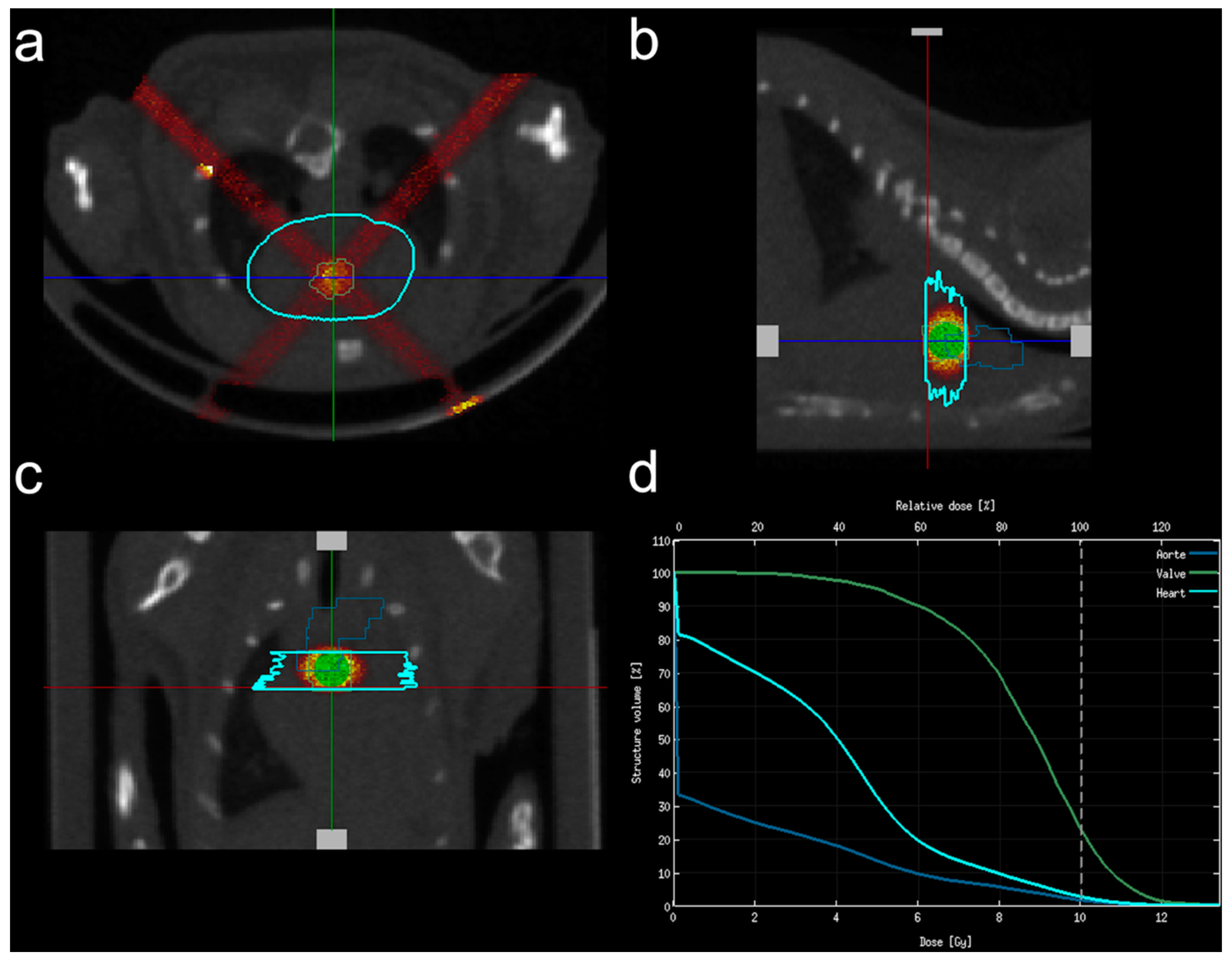
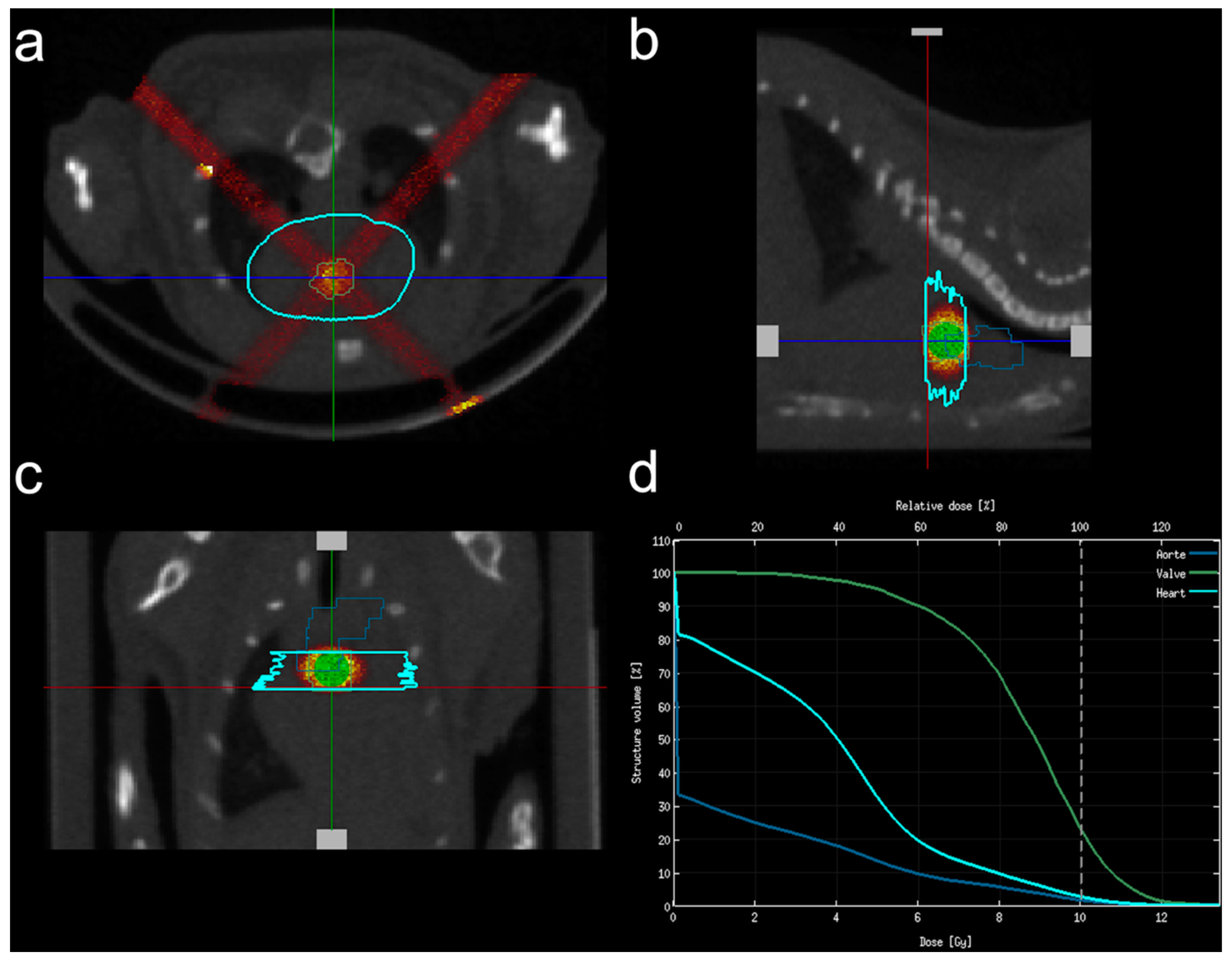
2.3. In Vivo Irradiation Protocol
2.4. Echocardiography
2.5. Magnetic Resonance Imaging of Aortic Inflammation
2.6. Histological Analysis
2.7. Irradiation of Human Aortic Valvular Interstitial Cells
2.8. Statistical Analysis
3. Results
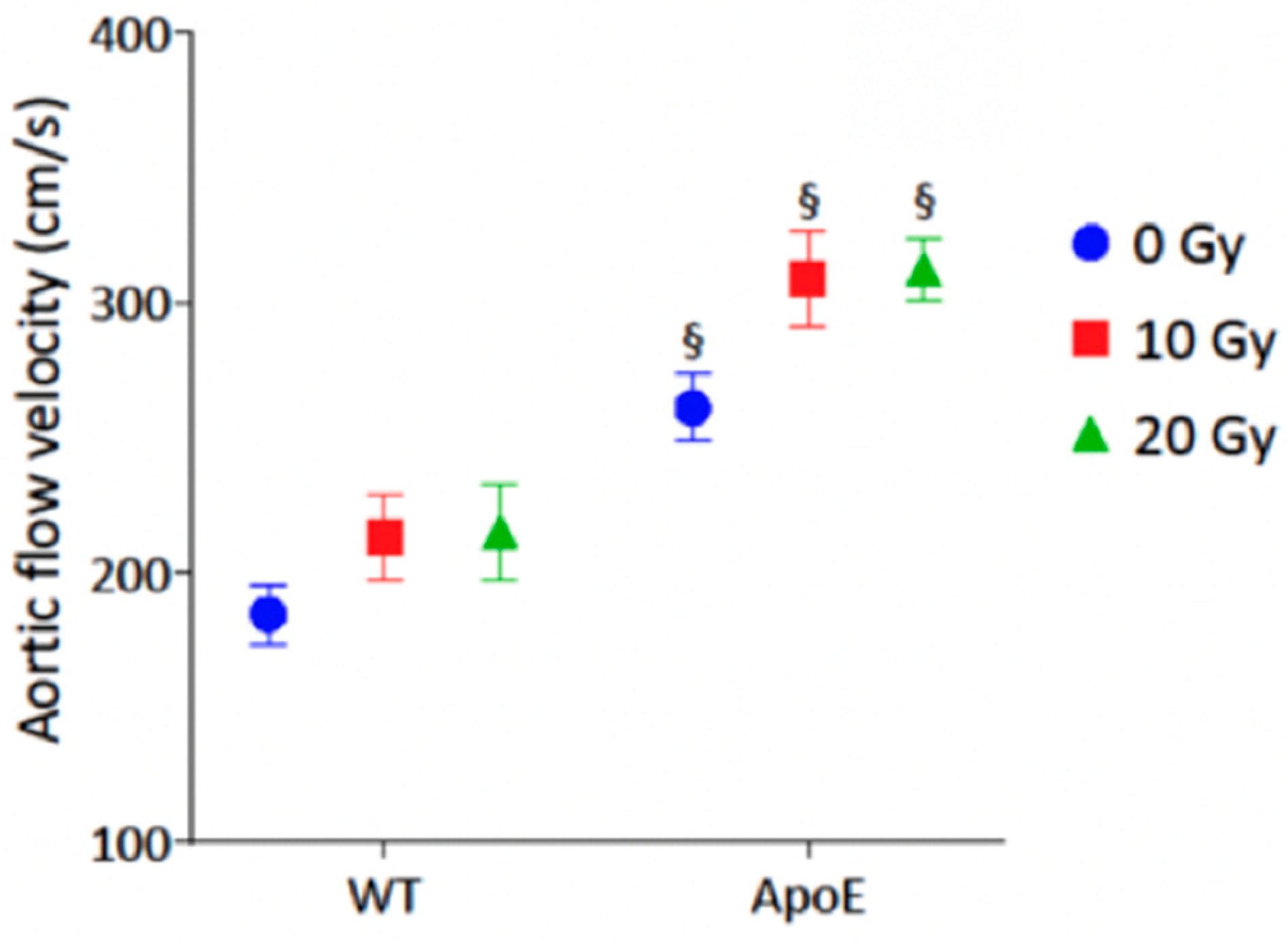
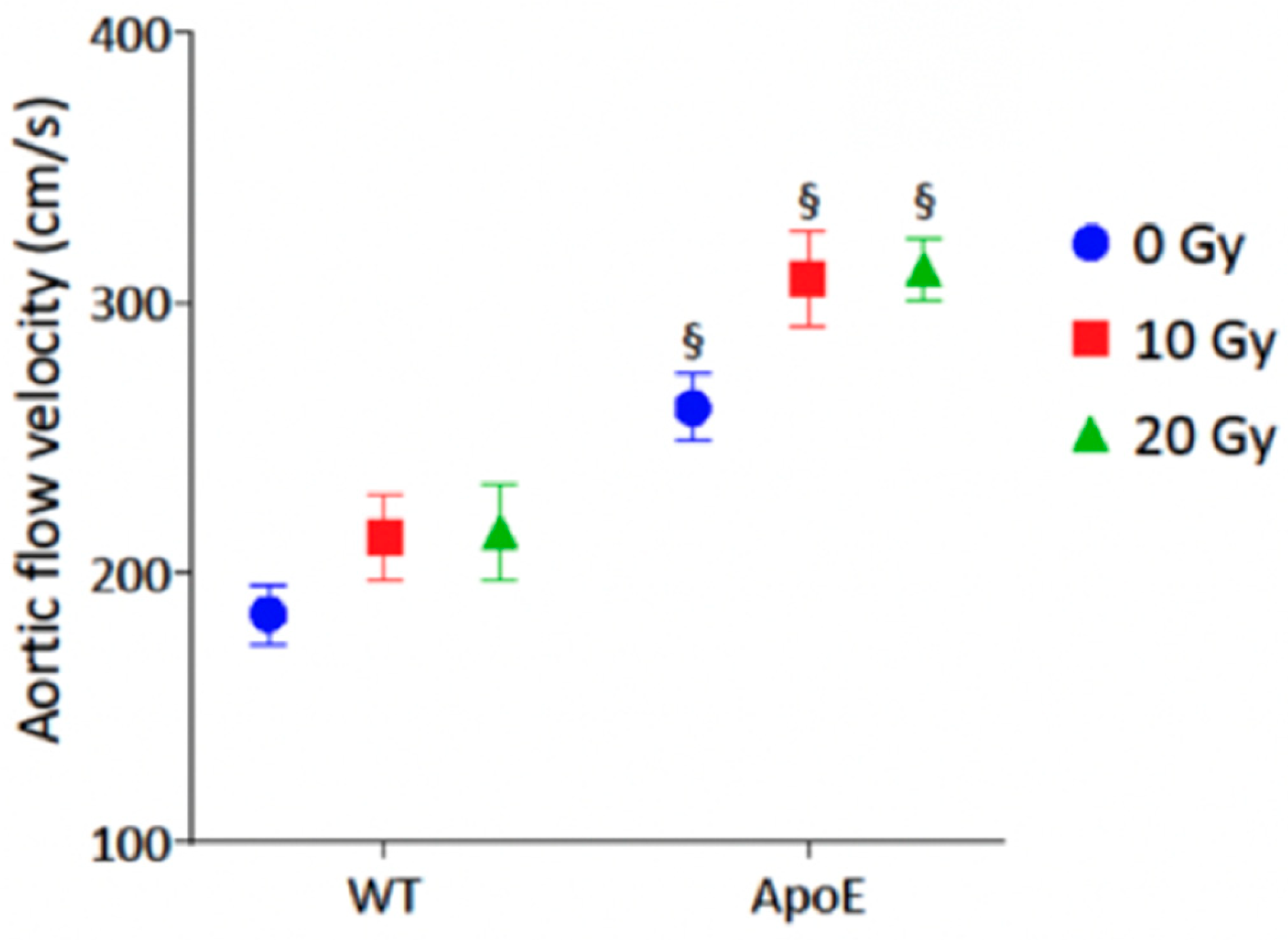
3.1. Echocardiography
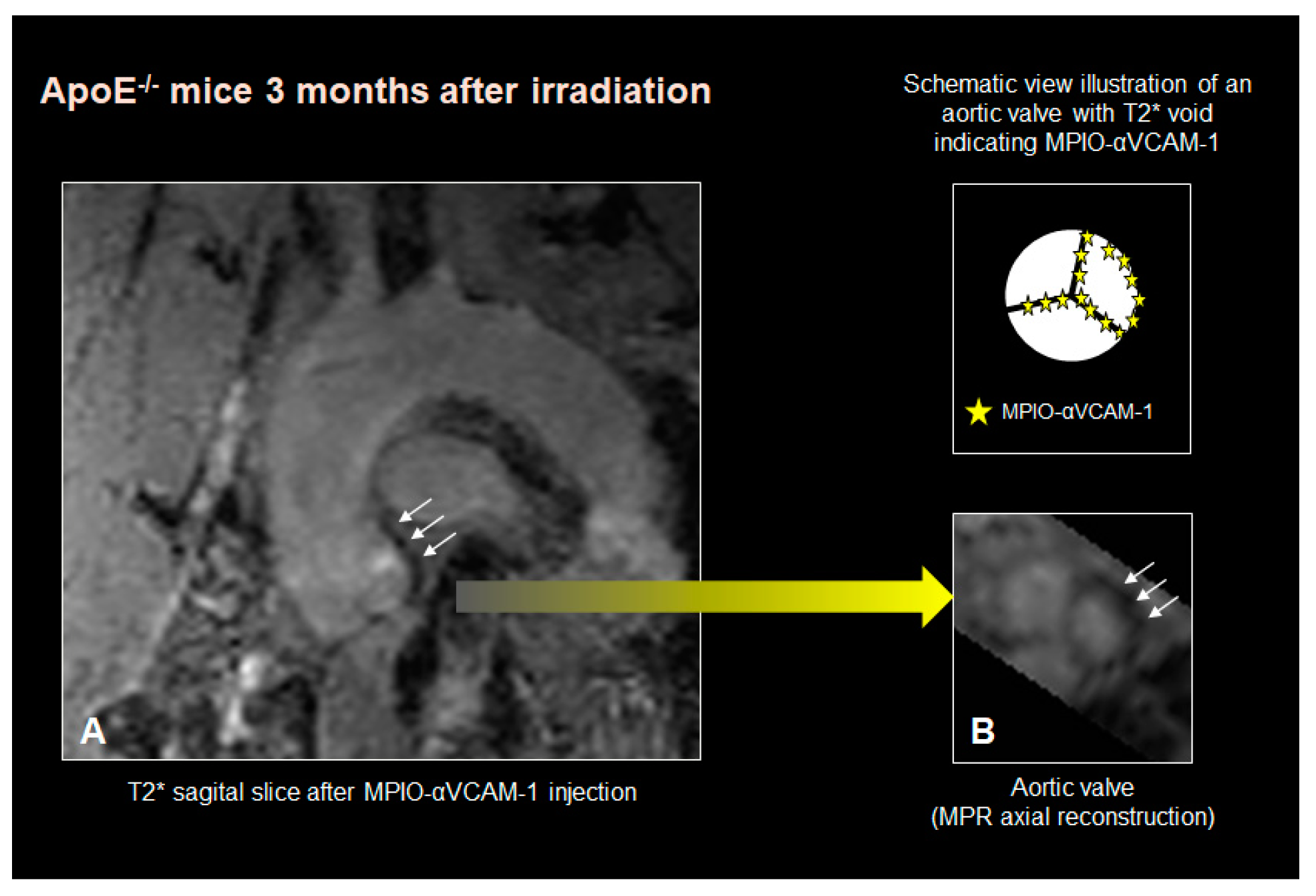
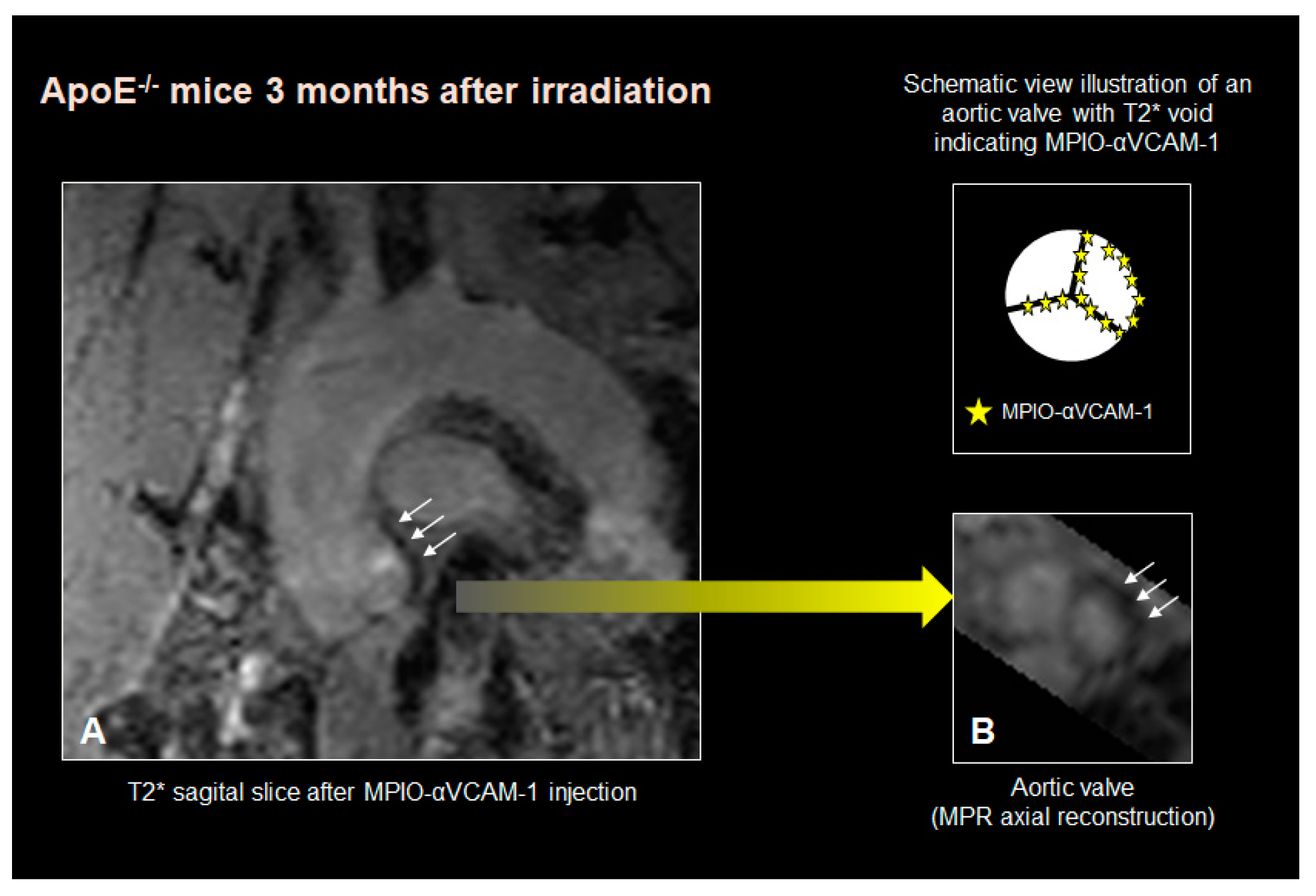
3.2. α-VCAM MPIO MR Imaging Findings
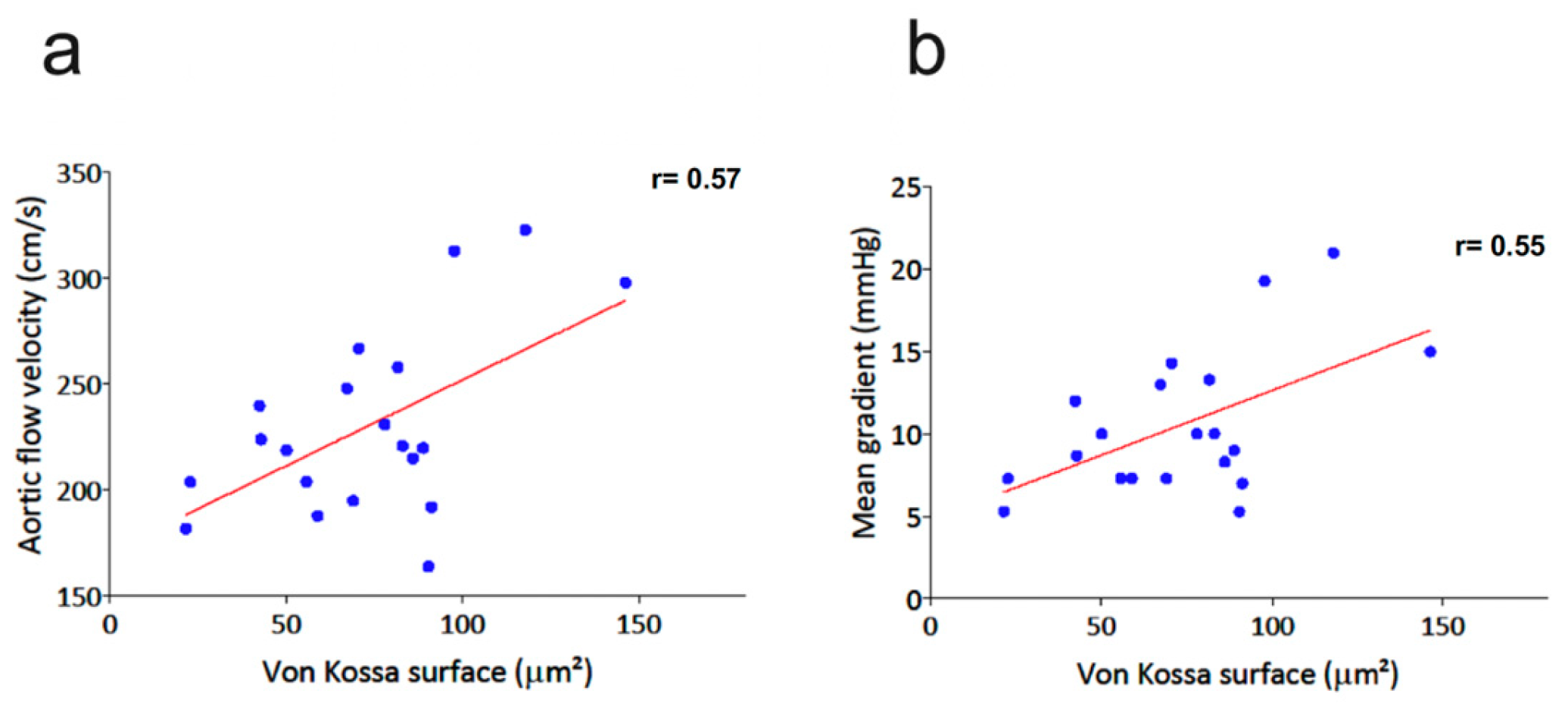
3.3. Histological Analysis
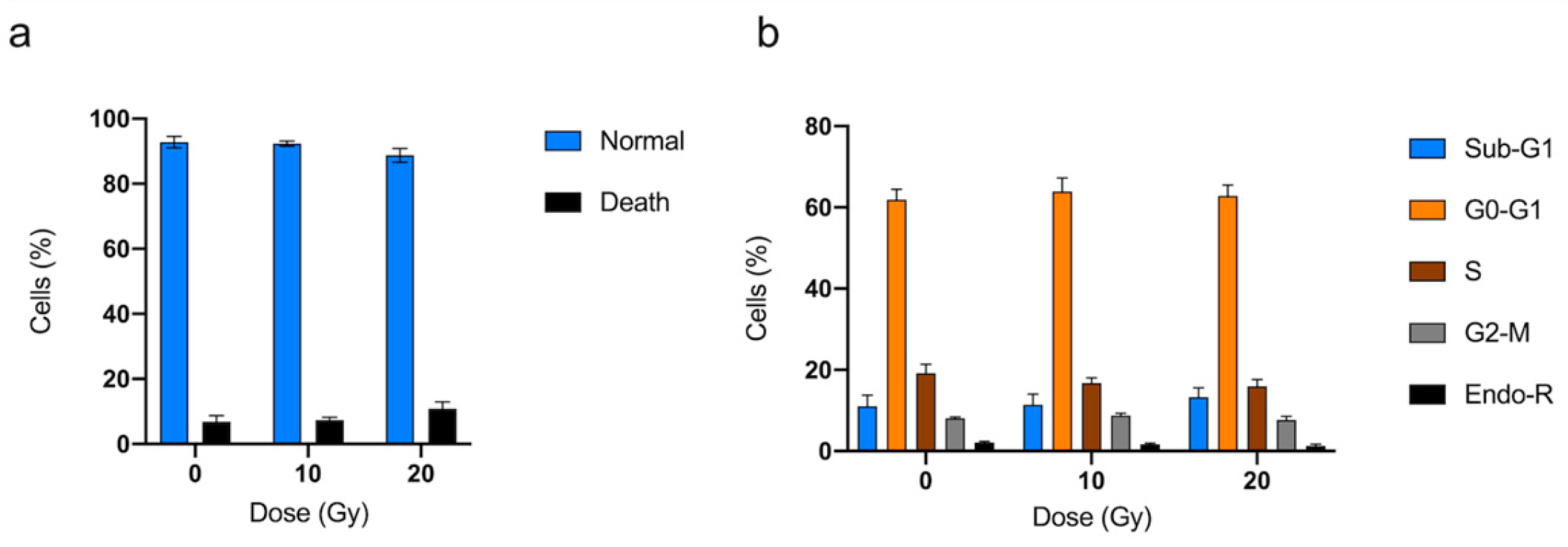
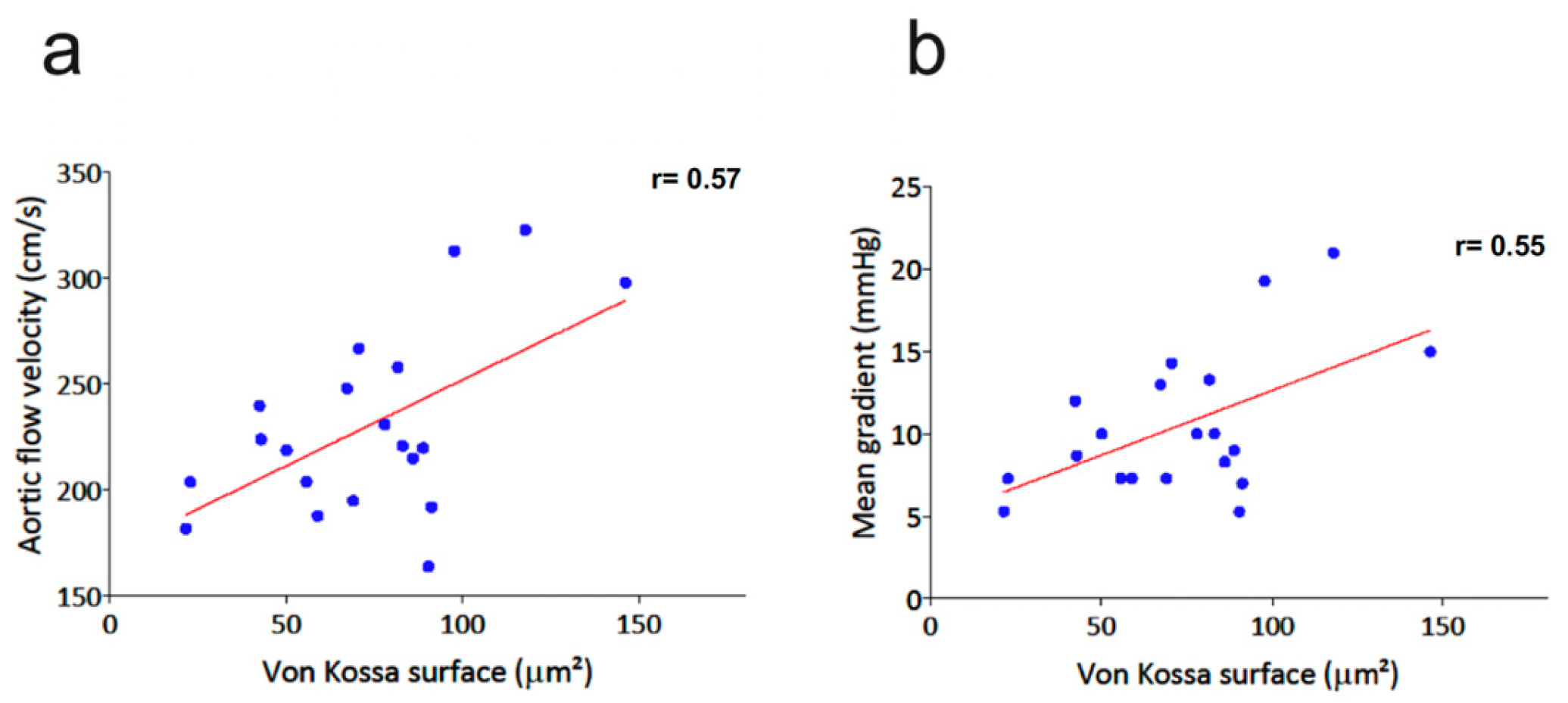
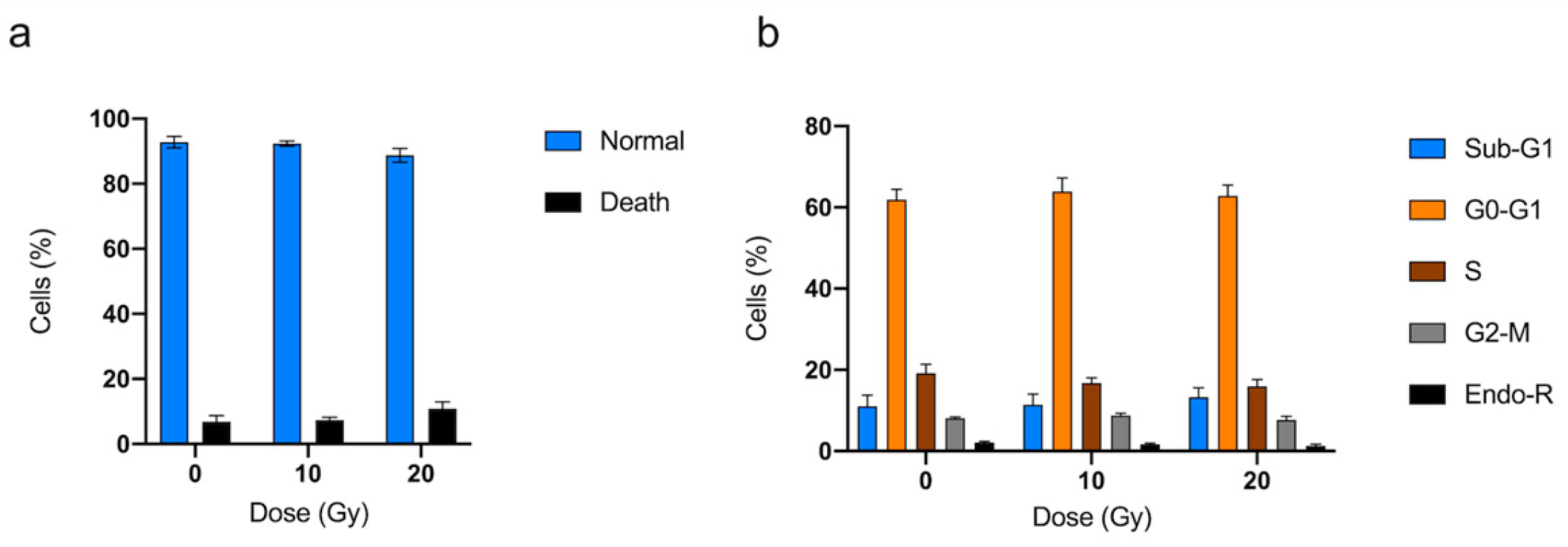
3.4. hVICs Analysis
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Belzile-Dugas, E.; Eisenberg, M.J. Radiation-Induced Cardiovascular Disease: Review of an Underrecognized Pathology. J. Am. Heart Assoc. 2021, 10, e021686. [Google Scholar] [CrossRef] [PubMed]
- Nkomo, V.T.; Gardin, J.M.; Skelton, T.N.; Gottdiener, J.S.; Scott, C.G.; Enriquez-Sarano, M. Burden of Valvular Heart Diseases: A Population-Based Study. Lancet 2006, 368, 1005–1011. [Google Scholar] [CrossRef] [PubMed]
- Coffey, S.; Cox, B.; Williams, M.J.A. The Prevalence, Incidence, Progression, and Risks of Aortic Valve Sclerosis: A Systematic Review and Meta-Analysis. J. Am. Coll. Cardiol. 2014, 63, 2852–2861. [Google Scholar] [CrossRef] [PubMed]
- Donnellan, E.; Griffin, B.P.; Johnston, D.R.; Popovic, Z.B.; Alashi, A.; Kapadia, S.R.; Tuzcu, E.M.; Krishnaswamy, A.; Mick, S.; Svensson, L.G.; et al. Rate of Progression of Aortic Stenosis and its Impact on Outcomes in Patients with Radiation-Associated Cardiac Disease. JACC Cardiovasc. Imaging 2018, 11, 1072–1080. [Google Scholar] [CrossRef] [PubMed]
- McGuirt, W.F.; Feehs, R.S.; Strickland, H.L.; Bond, G.; McKinney, W.M. Irradiation-Induced Atherosclerosis: A Factor in Therapeutic Planning. Ann. Otol. Rhinol. Laryngol. 1992, 101, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Finch, W.; Mahmud, E. Cardiovascular Complications of Radiotherapy. Am. J. Cardiol. 2013, 112, 1688–1696. [Google Scholar] [CrossRef]
- Yarnold, J.; Brotons, M.-C.V. Pathogenetic Mechanisms in Radiation Fibrosis. Radiother. Onco.l 2010, 97, 149–161. [Google Scholar] [CrossRef]
- Simard, C.; Magaud, C.; Adjlane, R.; Dupas, Q.; Sallé, L.; Manrique, A.; Bois, P.; Faivre, J.-F.; Guinamard, R. TRPM4 Non-Selective Cation Channel in Human Atrial Fibroblast Growth. Pflugers Arch. 2020, 472, 1719–1732. [Google Scholar] [CrossRef]
- Mpweme Bangando, H.; Simard, C.; Aize, M.; Lebrun, A.; Manrique, A.; Guinamard, R.; On Behalf of The Stop-As Investigators. TRPM4 Participates in Irradiation-Induced Aortic Valve Remodeling in Mice. Cancers 2022, 14, 4477. [Google Scholar] [CrossRef]
- Nadlonek, N.A.; Weyant, M.J.; Yu, J.A.; Cleveland, J.C.; Reece, T.B.; Meng, X.; Fullerton, D.A. Radiation Induces Osteogenesis in Human Aortic Valve Interstitial Cells. J. Thorac. Cardiovasc. Surg. 2012, 144, 1466–1470. [Google Scholar] [CrossRef]
- Lindman, B.R.; Clavel, M.-A.; Mathieu, P.; Iung, B.; Lancellotti, P.; Otto, C.M.; Pibarot, P. Calcific Aortic Stenosis. Nat. Rev. Dis. Primers 2016, 2, 16006. [Google Scholar] [CrossRef] [PubMed]
- Jurado, J.A.; Bashir, R.; Burket, M.W. Radiation-Induced Peripheral Artery Disease. Catheter. Cardiovasc. Interv. 2008, 72, 563–568. [Google Scholar] [CrossRef] [PubMed]
- Nakashima, Y.; Plump, A.S.; Raines, E.W.; Breslow, J.L.; Ross, R. ApoE-Deficient Mice Develop Lesions of All Phases of Atherosclerosis throughout the Arterial Tree. Arterioscler. Thromb. A J. Vasc. Biol. 1994, 14, 133–140. [Google Scholar] [CrossRef]
- Tanaka, K.; Sata, M.; Fukuda, D.; Suematsu, Y.; Motomura, N.; Takamoto, S.; Hirata, Y.; Nagai, R. Age-associated aortic stenosis in apolipoprotein E-deficient mice. J. Am. Coll. Cardiol. 2005, 46, 134–141. [Google Scholar] [CrossRef]
- Belliere, J.; Martinez de Lizarrondo, S.; Choudhury, R.P.; Quenault, A.; Le Béhot, A.; Delage, C.; Chauveau, D.; Schanstra, J.P.; Bascands, J.-L.; Vivien, D.; et al. Unmasking Silent Endothelial Activation in the Cardiovascular System Using Molecular Magnetic Resonance Imaging. Theranostics 2015, 5, 1187–1202. [Google Scholar] [CrossRef] [PubMed]
- Goode, A.; Gilbert, B.; Harkes, J.; Jukic, D.; Satyanarayanan, M. OpenSlide: A Vendor-Neutral Software Foundation for Digital Pathology. J. Pathol. Inform. 2013, 4, 27. [Google Scholar] [CrossRef] [PubMed]
- Morvan, M.; Arangalage, D.; Franck, G.; Perez, F.; Cattan-Levy, L.; Codogno, I.; Jacob-Lenet, M.-P.; Deschildre, C.; Choqueux, C.; Even, G.; et al. Relationship of Iron Deposition to Calcium Deposition in Human Aortic Valve Leaflets. J. Am. Coll. Cardiol. 2019, 73, 1043–1054. [Google Scholar] [CrossRef]
- Chen, J.-H.; Yip, C.Y.Y.; Sone, E.D.; Simmons, C.A. Identification and Characterization of Aortic Valve Mesenchymal Progenitor Cells with Robust Osteogenic Calcification Potential. Am. J. Pathol. 2009, 174, 1109–1119. [Google Scholar] [CrossRef]
- Wethal, T.; Lund, M.-B.; Edvardsen, T.; Fosså, S.D.; Pripp, A.H.; Holte, H.; Kjekshus, J.; Fosså, A. Valvular Dysfunction and Left Ventricular Changes in Hodgkin’s Lymphoma Survivors. A Longitudinal Study. Br. J. Cancer 2009, 101, 575–581. [Google Scholar] [CrossRef]
- Handa, N.; McGregor, C.G.A.; Danielson, G.K.; Orszulak, T.A.; Mullany, C.J.; Daly, R.C.; Dearani, J.A.; Anderson, B.J.; Puga, F.J. Coronary Artery Bypass Grafting in Patients with Previous Mediastinal Radiation Therapy. J. Thorac. Cardiovasc. Surg. 1999, 117, 1136–1143. [Google Scholar] [CrossRef]
- Meerman, M.; Driessen, R.; van Engeland, N.C.A.; Bergsma, I.; Steenhuijsen, J.L.G.; Kozono, D.; Aikawa, E.; Hjortnaes, J.; Bouten, C.V.C. Radiation Induces Valvular Interstitial Cell Calcific Response in an in vitro Model of Calcific Aortic Valve Disease. Front. Cardiovasc. Med. 2021, 8, 1070. [Google Scholar] [CrossRef] [PubMed]
- Peltier, M.; Trojette, F.; Sarano, M.E.; Grigioni, F.; Slama, M.A.; Tribouilloy, C.M. Relation between Cardiovascular Risk Factors and Nonrheumatic Severe Calcific Aortic Stenosis among Patients with a Three-Cuspid Aortic Valve. Am. J. Cardiol. 2003, 91, 97–99. [Google Scholar] [CrossRef]
- Aikawa, E.; Nahrendorf, M.; Sosnovik, D.; Lok, V.M.; Jaffer, F.A.; Aikawa, M.; Weissleder, R. Multimodality Molecular Imaging Identifies Proteolytic and Osteogenic Activities in Early Aortic Valve Disease. Circulation 2007, 115, 377–386. [Google Scholar] [CrossRef] [PubMed]
- Scatena, M.; Jackson, M.F.; Speer, M.Y.; Leaf, E.M.; Wallingford, M.C.; Giachelli, C.M. Increased Calcific Aortic Valve Disease in Response to a Diabetogenic, Procalcific Diet in the LDLr−/− ApoB100/100 Mouse Model. Cardiovasc. Pathol. 2018, 34, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, Y.; Adams, V.; Jacob, S.; Mangner, N.; Schuler, G.; Linke, A. Regular Exercise Training Prevents Aortic Valve Disease in Low-Density Lipoprotein-Receptor-Deficient Mice. Circulation 2010, 121, 759–767. [Google Scholar] [CrossRef]
- Mehrabian, M.; Demer, L.L.; Lusis, A.J. Differential Accumulation of Intimal Monocyte-Macrophages Relative to Lipoproteins and Lipofuscin Corresponds to Hemodynamic Forces on Cardiac Valves in Mice. Arterioscler. Thromb. J. Vasc. Biol. 1991, 11, 947–957. [Google Scholar] [CrossRef]
- Cheng, V.W.T.; de Pennington, N.; Zakaria, R.; Larkin, J.R.; Serres, S.; Sarkar, M.; Kirkman, M.A.; Bristow, C.; Croal, P.; Plaha, P.; et al. VCAM-1-Targeted MRI Improves Detection of the Tumor-Brain Interface. Clin. Cancer Res. 2022, 28, 2385–2396. [Google Scholar] [CrossRef]
- Chan, J.M.S.; Jin, P.S.; Ng, M.; Garnell, J.; Ying, C.W.; Tec, C.T.; Bhakoo, K. Development of Molecular Magnetic Resonance Imaging Tools for Risk Stratification of Carotid Atherosclerotic Disease Using Dual-Targeted Microparticles of Iron Oxide. Transl. Stroke Res. 2022, 13, 245–256. [Google Scholar] [CrossRef]
- Candellier, A.; Issa, N.; Grissi, M.; Brouette, T.; Avondo, C.; Gomila, C.; Blot, G.; Gubler, B.; Touati, G.; Bennis, Y.; et al. Indoxyl-Sulfate Activation of the AhR- NF-ΚB Pathway Promotes Interleukin-6 Secretion and the Subsequent Osteogenic Differentiation of Human Valvular Interstitial Cells from the Aortic Valve. J. Mol. Cell Cardiol. 2023, 179, 18–29. [Google Scholar] [CrossRef]
- Monaco, C.; Paleolog, E. Nuclear Factor ΚB: A Potential Therapeutic Target in Atherosclerosis and Thrombosis. Cardiovasc. Res. 2004, 61, 671–682. [Google Scholar] [CrossRef]
- Li, S.-J.; Cheng, W.-L.; Kao, Y.-H.; Chung, C.-C.; Trang, N.N.; Chen, Y.-J. Melatonin Inhibits NF-ΚB/CREB/Runx2 Signaling and Alleviates Aortic Valve Calcification. Front. Cardiovasc. Med. 2022, 9, 885293. [Google Scholar] [CrossRef] [PubMed]
- Amin, A.R.; Attur, M.G.; Pillinger, M.; Abramson, S.B. The Pleiotropic Functions of Aspirin: Mechanisms of Action. Cell Mol. Life Sci. 1999, 56, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.; Zhou, Y.; Ling, P.; Feng, X.; Luo, S.; Zheng, X.; Little, P.J.; Xu, S.; Weng, J. Metformin in Cardiovascular Diabetology: A Focused Review of Its Impact on Endothelial Function. Theranostics 2021, 11, 9376–9396. [Google Scholar] [CrossRef] [PubMed]
- Walls, G.M.; O’Kane, R.; Ghita, M.; Kuburas, R.; McGarry, C.K.; Cole, A.J.; Jain, S.; Butterworth, K.T. Murine Models of Radiation Cardiotoxicity: A Systematic Review and Recommendations for Future Studies. Radiother. Oncol. 2022, 173, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Delanian, S. Is Radiation-Induced Arteriopathy in Long-Term Breast Cancer Survivors an Underdiagnosed Situation?: Critical and Pragmatic Review of Available Literature. Radiother. Oncol. 2021, 157, 163–174. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline | 3-Month | p-Values | ||||||
|---|---|---|---|---|---|---|---|---|
| WT | ApoE−/− | WT | ApoE−/− | Global p-Value | Time Effect | Genotype Effect | Radiation Effect | |
| IVSd (mm) | 0.72 ± 0.02 | 0.75 ± 0.01 | 0.67 ± 0.02 | 0.68 ± 0.01 | 0.0009 | 0.0002 | ns | ns |
| IVSs (mm) | 0.89 ± 0.05 | 0.8 ± 0.02 | 0.72 ± 0.02 | 0.76 ± 0.03 | 0.01 | 0.0005 | ns | ns |
| LVDd (mm) | 3.70 ± 0.06 | 3.75 ± 0.09 | 3.95 ± 0.06 | 4.12 ± 0.09 | <0.01 | 0.0002 | ns | ns |
| LVDs (mm) | 2.48 ± 0.07 | 2.59 ± 0.08 | 2.84 ± 0.06 | 3.13 ± 0.1 | <0.0001 | <0.0001 | 0.01 | ns |
| LVPWd (mm) | 0.75 ± 0.02 | 0.86 ± 0.04 | 0.82 ± 0.03 | 0.83 ± 0.03 | ns | nd | nd | nd |
| LVPWs (mm) | 0.98 ± 0.03 | 1.07 ± 0.04 | 0.98 ± 0.03 | 0.98 ± 0.04 | ns | nd | nd | nd |
| FS (%) | 33.13 ± 1.32 | 31.15 ± 1.08 | 28.27 ± 0.67 | 24.40 ± 1.23 | <0.0001 | <0.0001 | <0.01 | ns |
| WT | ApoE−/− | p-Value | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Radiation Dose | 0 Gy | 10 Gy | 20 Gy | 0 Gy | 10 Gy | 20 Gy | Global p-Value | Genotype Effect | Radiation Effect |
| Flow velocity (cm/s) | 184 ± 5 | 213 ± 10 | 214 ± 2 | 261 ± 17 § | 308 ± 20 § | 312 ± 15 *§ | <0.0001 | <0.0001 | <0.001 |
| Mean gradient (mmHg) | 6.33 ± 0.46 | 8.53 ± 0.93 | 8.83 ± 0.44 | 13.58 ± 1.69 § | 16.92 ± 1.71 § | 20.57 ± 2.04 §* | <0.0001 | <0.0001 | <0.01 |
| Max gradient (mmHg) | 13.68 ± 0.78 | 18.36 ± 1.88 | 18.45 ± 0.4 | 28.05 ± 3.53 § | 38.57 ± 5.02 § | 39.75 ± 3.84 § | <0.0001 | <0.0001 | <0.01 |
| Aortic Sinus | Aortic Valve Leaflets | |||||
|---|---|---|---|---|---|---|
| MPIO-αVCAM-1 | Negative | Positive | Total | Negative | Positive | Total |
| RT- | 4 | 2 | 6 | 4 | 2 | 6 |
| RT+ | 4 | 13 | 17 | 1 | 16 | 17 |
| Total | 8 | 15 | 23 | 5 | 18 | 23 |
| WT | ApoE−/− | p-Values | |||||||
|---|---|---|---|---|---|---|---|---|---|
| 0 Gy | 10 Gy | 20 Gy | 0 Gy | 10 Gy | 20 Gy | Global | Genotype | Radiation | |
| Leaflet area (mm2) | 0.144 ± 0.006 | 0.161 ± 0.015 | 0.166 ± 0.015 | 0.115 ± 0.005 | 0.164 ± 0.008 * | 0.195 ± 0.019 * | 0.0001 | ns | 0.0001 |
| Sinus tissue area (mm2) | 0.253 ± 0.010 | 0.245 ± 0.009 | 0.217 ± 0.022 | 0.473 ± 0.030 § | 0.484 ± 0.026 § | 0.697 ± 0.034 *†§ | <0.0001 | <0.0001 | <0.05 |
| von Kossa area (%) | 4.187 ± 11.7 | 3.809 ± 4.4 | 5.224 ± 1.62 | 4.224 ± 6.76 | 7.027 ± 10.287 * | 4.027 ± 4.584 *† | <0.0001 | ns | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rucher, G.; Prigent, K.; Simard, C.; Frelin, A.-M.; Coquemont-Guyot, M.; Elie, N.; Delcroix, N.; Perzo, N.; Guinamard, R.; Berger, L.; et al. Targeted Radiation Exposure Induces Accelerated Aortic Valve Remodeling in ApoE−/− Mice. J. Clin. Med. 2023, 12, 5854. https://doi.org/10.3390/jcm12185854
Rucher G, Prigent K, Simard C, Frelin A-M, Coquemont-Guyot M, Elie N, Delcroix N, Perzo N, Guinamard R, Berger L, et al. Targeted Radiation Exposure Induces Accelerated Aortic Valve Remodeling in ApoE−/− Mice. Journal of Clinical Medicine. 2023; 12(18):5854. https://doi.org/10.3390/jcm12185854
Chicago/Turabian StyleRucher, Guillaume, Kevin Prigent, Christophe Simard, Anne-Marie Frelin, Maëlle Coquemont-Guyot, Nicolas Elie, Nicolas Delcroix, Nicolas Perzo, Romain Guinamard, Ludovic Berger, and et al. 2023. "Targeted Radiation Exposure Induces Accelerated Aortic Valve Remodeling in ApoE−/− Mice" Journal of Clinical Medicine 12, no. 18: 5854. https://doi.org/10.3390/jcm12185854
APA StyleRucher, G., Prigent, K., Simard, C., Frelin, A.-M., Coquemont-Guyot, M., Elie, N., Delcroix, N., Perzo, N., Guinamard, R., Berger, L., Manrique, A., & on behalf of the STOP-AS Investigators. (2023). Targeted Radiation Exposure Induces Accelerated Aortic Valve Remodeling in ApoE−/− Mice. Journal of Clinical Medicine, 12(18), 5854. https://doi.org/10.3390/jcm12185854