


The Impact of COVID-19 on Carotid–Femoral Pulse Wave Velocity: A Systematic Review and Meta-Analysis
 , , ,
, , ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction and Quality Assessment
2.5. Statistical Analysis
3. Results
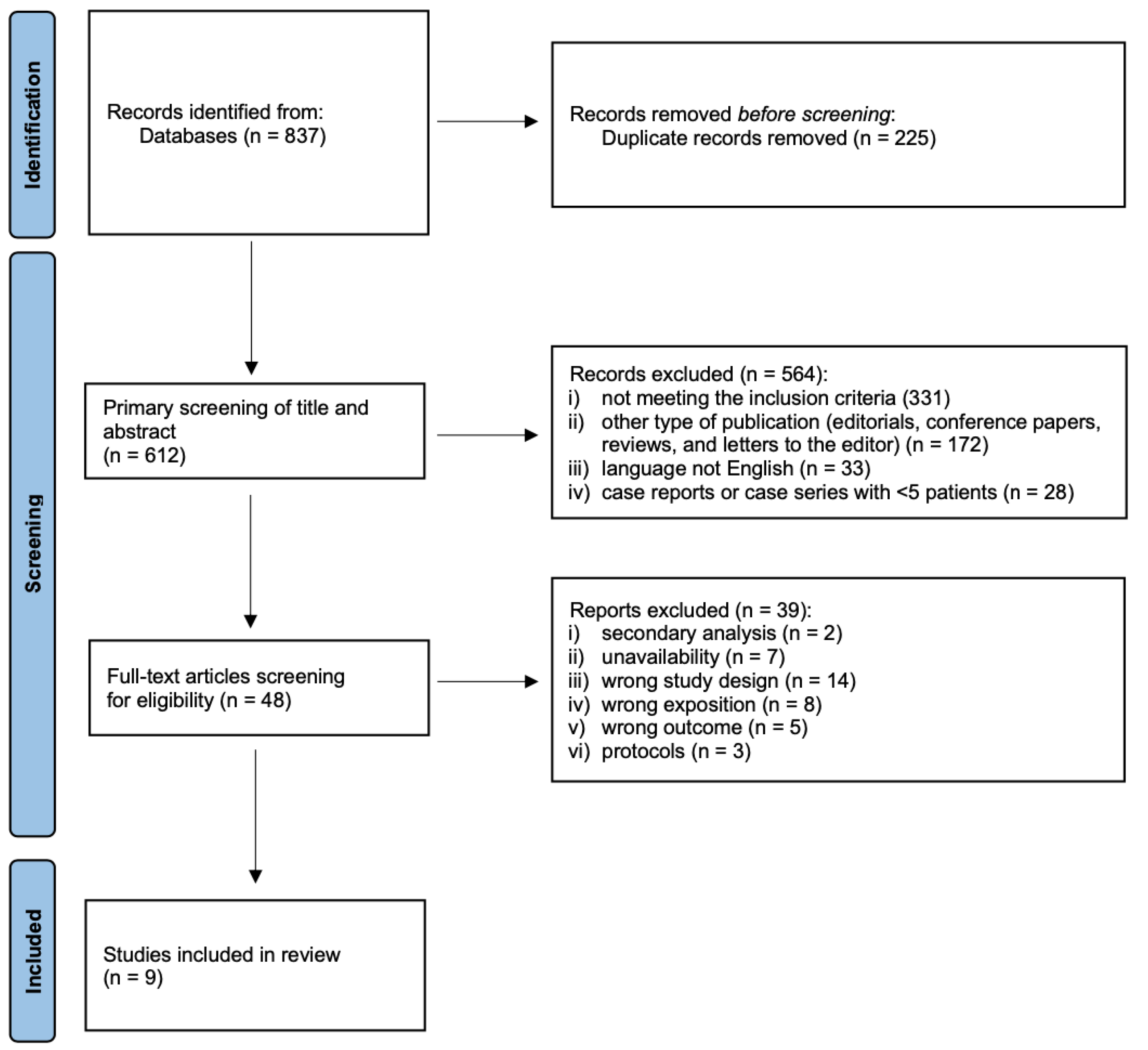
3.1. Study Selection and Characteristics
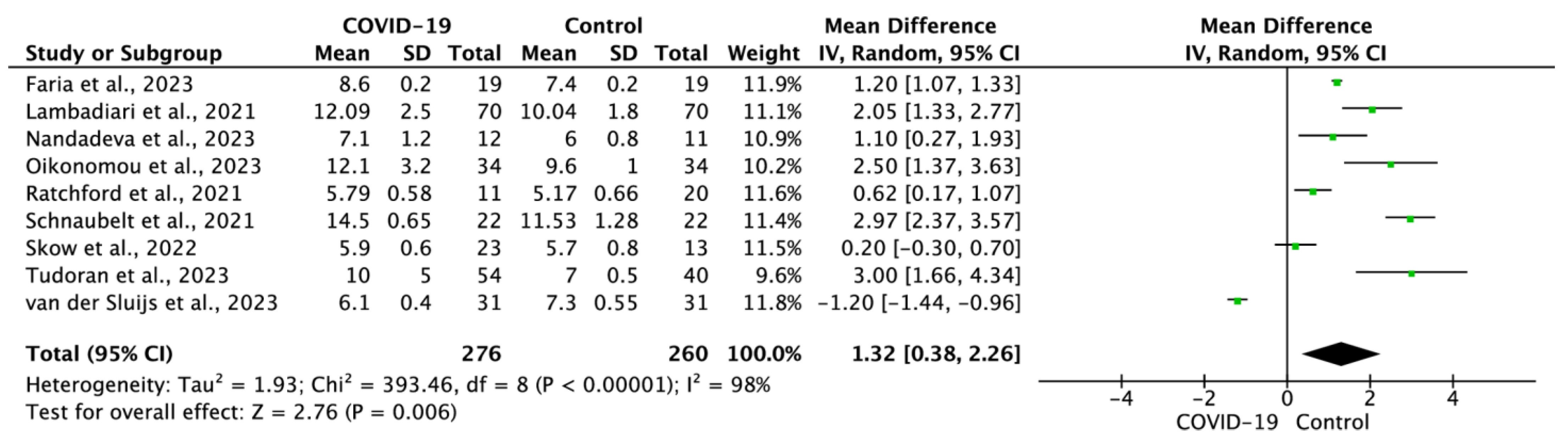
3.2. Meta-Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organisation. WHO Coronavirus Disease Dashboard. 2021. Available online: https://covid19.who.int/ (accessed on 12 June 2023).
- Smereka, J.; Szarpak, L.; Filipiak, K.J. Modern Medicine in the COVID-19 Era. Disaster Emerg. Med. J. 2020, 5, 103–105. [Google Scholar] [CrossRef]
- Berry, C.; Mangion, K. Multisystem Involvement Is Common in Post-COVID-19 Syndrome. Nat. Med. 2022, 28, 1139–1140. [Google Scholar] [CrossRef]
- Gasecka, A.; Pruc, M.; Kukula, K.; Gilis-Malinowska, N.; Filipiak, K.J.; Jaguszewski, M.J.; Szarpak, L. Post-Covid-19 Heart Syndrome. Cardiol. J. 2021, 28, 353–354. [Google Scholar] [CrossRef] [PubMed]
- Guzik, T.J.; Mohiddin, S.A.; Dimarco, A.; Patel, V.; Savvatis, K.; Marelli-Berg, F.M.; Madhur, M.S.; Tomaszewski, M.; Maffia, P.; D’Acquisto, F.; et al. COVID-19 and the Cardiovascular System: Implications for Risk Assessment, Diagnosis, and Treatment Options. Cardiovasc. Res. 2020, 116, 1666–1687. [Google Scholar] [CrossRef]
- Wang, W.; Wang, C.Y.; Wang, S.I.; Wei, J.C.C. Long-Term Cardiovascular Outcomes in COVID-19 Survivors among Non-Vaccinated Population: A Retrospective Cohort Study from the TriNetX US Collaborative Networks. eClinicalMedicine 2022, 53, 101619. [Google Scholar] [CrossRef]
- Szarpak, L.; Pruc, M.; Filipiak, K.J.; Popieluch, J.; Bielski, A.; Jaguszewski, M.J.; Gilis-Malinowska, N.; Chirico, F.; Rafique, Z.; Peacock, F.W. Myocarditis: A Complication of COVID-19 and Long-COVID-19 Syndrome as a Serious Threat in Modern Cardiology. Cardiol. J. 2022, 29, 178–179. [Google Scholar] [CrossRef]
- Zanoli, L.; Gaudio, A.; Mikhailidis, D.P.; Katsiki, N.; Castellino, N.; Lo Cicero, L.; Geraci, G.; Sessa, C.; Fiorito, L.; Marino, F.; et al. Vascular Dysfunction of COVID-19 Is Partially Reverted in the Long-Term. Circ. Res. 2022, 130, 1276–1285. [Google Scholar] [CrossRef]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Author Correction: Long COVID: Major Findings, Mechanisms and Recommendations (Nature Reviews Microbiology, (2023), 21, 3, (133-146), 10.1038/S41579-022-00846-2). Nat. Rev. Microbiol. 2023, 21, 408. [Google Scholar] [CrossRef]
- Ballering, A.V.; van Zon, S.K.R.; olde Hartman, T.C.; Rosmalen, J.G.M. Persistence of Somatic Symptoms after COVID-19 in the Netherlands: An Observational Cohort Study. Lancet 2022, 400, 452–461. [Google Scholar] [CrossRef]
- Szarpak, L.; Filipiak, K.J.; Skwarek, A.; Pruc, M.; Rahnama, M.; Denegri, A.; Jachowicz, M.; Dawidowska, M.; Gasecka, A.; Jaguszewski, M.J.; et al. Outcomes and Mortality Associated with Atrial Arrhythmias among Patients Hospitalized with COVID-19: A Systematic Review and Meta-Analysis. Cardiol. J. 2022, 29, 33–43. [Google Scholar] [CrossRef]
- Szarpak, L.; Mierzejewska, M.; Jurek, J.; Kochanowska, A.; Gasecka, A.; Truszewski, Z.; Pruc, M.; Blek, N.; Rafique, Z.; Filipiak, K.J.; et al. Effect of Coronary Artery Disease on COVID-19—Prognosis and Risk Assessment: A Systematic Review and Meta-Analysis. Biology 2022, 11, 221. [Google Scholar] [CrossRef] [PubMed]
- Libby, P.; Lüscher, T. COVID-19 Is, in the End, an Endothelial Disease. Eur. Heart J. 2020, 41, 3038–3044. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial Cell Infection and Endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Çiftel, M.; Ateş, N.; Yılmaz, O. Investigation of Endothelial Dysfunction and Arterial Stiffness in Multisystem Inflammatory Syndrome in Children. Eur. J. Pediatr. 2022, 181, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Chang, R.; Mamun, A.; Dominic, A.; Le, N.T. SARS-CoV-2 Mediated Endothelial Dysfunction: The Potential Role of Chronic Oxidative Stress. Front. Physiol. 2021, 11, 605908. [Google Scholar] [CrossRef]
- Ambardar, S.R.; Hightower, S.L.; Huprikar, N.A.; Chung, K.K.; Singhal, A.; Collen, J.F. Post-COVID-19 Pulmonary Fibrosis: Novel Sequelae of the Current Pandemic. J. Clin. Med. 2021, 10, 2452. [Google Scholar] [CrossRef]
- Thijssen, D.H.J.; Bruno, R.M.; Van Mil, A.C.C.M.; Holder, S.M.; Faita, F.; Greyling, A.; Zock, P.L.; Taddei, S.; Deanfield, J.E.; Luscher, T.; et al. Expert Consensus and Evidence-Based Recommendations for the Assessment of Flow-Mediated Dilation in Humans. Eur. Heart J. 2019, 40, 2534–2547. [Google Scholar] [CrossRef]
- Laurent, S.; Boutouyrie, P.; Cunha, P.G.; Lacolley, P.; Nilsson, P.M. Concept of Extremes in Vascular Aging: From Early Vascular Aging to Supernormal Vascular Aging. Hypertension 2019, 74, 218–228. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; De Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for Themanagement of Arterial Hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Ben-Shlomo, Y.; Spears, M.; Boustred, C.; May, M.; Anderson, S.G.; Benjamin, E.J.; Boutouyrie, P.; Cameron, J.; Chen, C.H.; Cruickshank, J.K.; et al. Aortic Pulse Wave Velocity Improves Cardiovascular Event Prediction: An Individual Participant Meta-Analysis of Prospective Observational Data from 17,635 Subjects. J. Am. Coll. Cardiol. 2014, 63, 636–646. [Google Scholar] [CrossRef] [PubMed]
- Van Bortel, L.M.; Laurent, S.; Boutouyrie, P.; Chowienczyk, P.; Cruickshank, J.K.; De Backer, T.; Filipovsky, J.; Huybrechts, S.; Mattace-Raso, F.U.; Protogerou, A.D.; et al. Expert consensus document on the Measurement of Aortic Stiffness in Daily Practice Using Carotid-Femoral Pulse Wave Velocity. J. Hypertens. 2012, 30, 445–448. [Google Scholar] [CrossRef] [PubMed]
- Raisi-Estabragh, Z.; McCracken, C.; Cooper, J.; Fung, K.; Paiva, J.M.; Khanji, M.Y.; Rauseo, E.; Biasiolli, L.; Raman, B.; Piechnik, S.K.; et al. Adverse Cardiovascular Magnetic Resonance Phenotypes Are Associated with Greater Likelihood of Incident Coronavirus Disease 2019: Findings from the UK Biobank. Aging Clin. Exp. Res. 2021, 33, 1133–1144. [Google Scholar] [CrossRef] [PubMed]
- Szeghy, R.E.; Province, V.M.; Stute, N.L.; Augenreich, M.A.; Koontz, L.K.; Stickford, J.L.; Stickford, A.S.L.; Ratchford, S.M. Carotid Stiffness, Intima–Media Thickness and Aortic Augmentation Index among Adults with SARS-CoV-2. Exp. Physiol. 2022, 107, 694–707. [Google Scholar] [CrossRef] [PubMed]
- Rodilla, E.; López-Carmona, M.D.; Cortes, X.; Cobos-Palacios, L.; Canales, S.; Sáez, M.C.; Campos Escudero, S.; Rubio-Rivas, M.; Díez Manglano, J.; Freire Castro, S.J.; et al. Impact of Arterial Stiffness on All-Cause Mortality in Patients Hospitalized With COVID-19 in Spain. Hypertension 2021, 77, 856–867. [Google Scholar] [CrossRef]
- Aydın, E.; Kant, A.; Yilmaz, G. Evaluation of the Cardio-Ankle Vascular Index in COVID-19 Patients. Rev. Assoc. Med. Bras. 2022, 68, 73–76. [Google Scholar] [CrossRef]
- Bruno, R.M.; Nilsson, P.M.; Engström, G.; Wadström, B.N.; Empana, J.P.; Boutouyrie, P.; Laurent, S. Early and Supernormal Vascular Aging: Clinical Characteristics and Association With Incident Cardiovascular Events. Hypertension 2020, 76, 1616–1624. [Google Scholar] [CrossRef]
- Vlachopoulos, C.; Aznaouridis, K.; Stefanadis, C. Prediction of Cardiovascular Events and All-Cause Mortality With Arterial Stiffness. A Systematic Review and Meta-Analysis. J. Am. Coll. Cardiol. 2010, 55, 1318–1327. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Stang, A. Critical Evaluation of the Newcastle-Ottawa Scale for the Assessment of the Quality of Nonrandomized Studies in Meta-Analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the Mean and Variance from the Median, Range, and the Size of a Sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring Inconsistency in Meta-Analyses. Br. Med. J. 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Faria, D.; Moll-Bernardes, R.J.; Testa, L.; Moniz, C.M.V.; Rodrigues, E.C.; Rodrigues, A.G.; Araujo, A.; Alves, M.J.N.N.; Ono, B.E.; Izaias, J.E.; et al. Sympathetic Neural Overdrive, Aortic Stiffening, Endothelial Dysfunction, and Impaired Exercise Capacity in Severe COVID-19 Survivors: A Mid-Term Study of Cardiovascular Sequelae. Hypertension 2023, 80, 470–481. [Google Scholar] [CrossRef] [PubMed]
- Tudoran, C.; Bende, F.; Bende, R.; Giurgi-Oncu, C.; Dumache, R.; Tudoran, M. Correspondence between Aortic and Arterial Stiffness, and Diastolic Dysfunction in Apparently Healthy Female Patients with Post-Acute COVID-19 Syndrome. Biomedicines 2023, 11, 492. [Google Scholar] [CrossRef] [PubMed]
- Nandadeva, D.; Skow, R.J.; Stephens, B.Y.; Grotle, A.K.; Georgoudiou, S.; Barshikar, S.; Seo, Y.; Fadel, P.J. Cardiovascular and Cerebral Vascular Health in Females with Postacute Sequelae of COVID-19. Am. J. Physiol. Heart Circ. Physiol. 2023, 324, H713–H720. [Google Scholar] [CrossRef]
- Oikonomou, E.; Lampsas, S.; Theofilis, P.; Souvaliotis, N.; Papamikroulis, G.A.; Katsarou, O.; Kalogeras, K.; Pantelidis, P.; Papaioannou, T.G.; Tsatsaragkou, A.; et al. Impaired Left Ventricular Deformation and Ventricular-Arterial Coupling in Post-COVID-19: Association with Autonomic Dysregulation. Heart Vessels 2023, 38, 381–393. [Google Scholar] [CrossRef]
- van der Sluijs, K.M.; Bakker, E.A.; Schuijt, T.J.; Joseph, J.; Kavousi, M.; Geersing, G.J.; Rutten, F.H.; Hartman, Y.A.W.; Thijssen, D.H.J.; Eijsvogels, T.M.H. Long-Term Cardiovascular Health Status and Physical Functioning of Nonhospitalized Patients with COVID-19 Compared with Non-COVID-19 Controls. Am. J. Physiol.—Heart Circ. Physiol. 2023, 324, H47–H56. [Google Scholar] [CrossRef]
- Skow, R.J.; Nandadeva, D.; Grotle, A.K.; Stephens, B.Y.; Wright, A.N.; Fadel, P.J. Impact of Breakthrough COVID-19 Cases during the Omicron Wave on Vascular Health and Cardiac Autonomic Function in Young Adults. Am. J. Physiol.—Heart Circ. Physiol. 2022, 323, H59–H64. [Google Scholar] [CrossRef]
- Lambadiari, V.; Mitrakou, A.; Kountouri, A.; Thymis, J.; Katogiannis, K.; Korakas, E.; Varlamos, C.; Andreadou, I.; Tsoumani, M.; Triantafyllidi, H.; et al. Association of COVID-19 with Impaired Endothelial Glycocalyx, Vascular Function and Myocardial Deformation 4 Months after Infection. Eur. J. Heart Fail. 2021, 23, 1916–1926. [Google Scholar] [CrossRef]
- Ratchford, S.M.; Stickford, J.L.; Province, V.M.; Stute, N.; Augenreich, M.A.; Koontz, L.K.; Bobo, L.K.; Stickford, A.S.L. Vascular Alterations among Young Adults with SARS-CoV-2. Am. J. Physiol.—Heart Circ. Physiol. 2021, 320, H404–H410. [Google Scholar] [CrossRef]
- Schnaubelt, S.; Oppenauer, J.; Tihanyi, D.; Mueller, M.; Maldonado-Gonzalez, E.; Zejnilovic, S.; Haslacher, H.; Perkmann, T.; Strassl, R.; Anders, S.; et al. Arterial Stiffness in Acute COVID-19 and Potential Associations with Clinical Outcome. J. Intern. Med. 2021, 290, 437–443. [Google Scholar] [CrossRef]
- Oliveira, A.C.; Cunha, P.M.G.M.; Vitorino, P.V.d.O.; Souza, A.L.L.; Deus, G.D.; Feitosa, A.; Barbosa, E.C.D.; Gomes, M.M.; Jardim, P.C.B.V.; Barroso, W.K.S. Vascular Aging and Arterial Stiffness. Arq. Bras. Cardiol. 2022, 119, 604–615. [Google Scholar] [CrossRef]
- Townsend, R.R. Arterial Stiffness: Recommendations and Standardization. Pulse 2016, 4, 3–7. [Google Scholar] [CrossRef]
- Vrints, C.J.M.; Krychtiuk, K.A.; Van Craenenbroeck, E.M.; Segers, V.F.; Price, S.; Heidbuchel, H. Endothelialitis Plays a Central Role in the Pathophysiology of Severe COVID-19 and Its Cardiovascular Complications. Acta Cardiol. 2021, 76, 109–124. [Google Scholar] [CrossRef]
- Montazersaheb, S.; Hosseiniyan Khatibi, S.M.; Hejazi, M.S.; Tarhriz, V.; Farjami, A.; Ghasemian Sorbeni, F.; Farahzadi, R.; Ghasemnejad, T. COVID-19 Infection: An Overview on Cytokine Storm and Related Interventions. Virol. J. 2022, 19, 92. [Google Scholar] [CrossRef]
- Merad, M.; Martin, J.C. Pathological Inflammation in Patients with COVID-19: A Key Role for Monocytes and Macrophages. Nat. Rev. Immunol. 2020, 20, 355–362. [Google Scholar] [CrossRef]
- Martel, J.; Ko, Y.F.; Young, J.D.; Ojcius, D.M. Could Nasal Nitric Oxide Help to Mitigate the Severity of COVID-19? Microbes Infect. 2020, 22, 168–171. [Google Scholar] [CrossRef]
- Vlachopoulos, C.; Dima, I.; Aznaouridis, K.; Vasiliadou, C.; Ioakeimidis, N.; Aggeli, C.; Toutouza, M.; Stefanadis, C. Acute Systemic Inflammation Increases Arterial Stiffness and Decreases Wave Reflections in Healthy Individuals. Circulation 2005, 112, 2193–2200. [Google Scholar] [CrossRef]
- Van Sloten, T.T.; Sedaghat, S.; Laurent, S.; London, G.M.; Pannier, B.; Ikram, M.A.; Kavousi, M.; Mattace-Raso, F.; Franco, O.H.; Boutouyrie, P.; et al. Carotid Stiffness Is Associated with Incident Stroke A Systematic Review and Individual Participant Data Meta-Analysis. J. Am. Coll. Cardiol. 2015, 66, 2116–2125. [Google Scholar] [CrossRef]
- Menezes, R.G.; Alabduladhem, T.O.; Siddiqi, A.K.; Maniya, M.T.; Al Dahlawi, A.M.; Almulhim, M.W.A.; Almulhim, H.W.; Saeed, Y.A.A.; Alotaibi, M.S.; Alarifi, S.S.; et al. Infezioni in Medicina. Infez. Med. 2023, 31, 140–150. [Google Scholar] [CrossRef]
- Maruhashi, T.; Higashi, Y. Pathophysiological Association of Endothelial Dysfunction with Fatal Outcome in Covid-19. Int. J. Mol. Sci. 2021, 22, 5131. [Google Scholar] [CrossRef]
- Kumar, N.; Kumar, S.; Kumar, A.; Bhushan, D.; Kumar, A.; Kumar, A.; Singh, V.; Singh, P.K. The Cosevast Study Outcome: Evidence of Covid-19 Severity Proportionate to Surge in Arterial Stiffness. Indian J. Crit. Care Med. 2021, 25, 1111–1117. [Google Scholar] [CrossRef]
- Ikonomidis, I.; Lambadiari, V.; Mitrakou, A.; Kountouri, A.; Katogiannis, K.; Thymis, J.; Korakas, E.; Pavlidis, G.; Kazakou, P.; Panagopoulos, G.; et al. Myocardial Work and Vascular Dysfunction Are Partially Improved at 12 Months after COVID-19 Infection. Eur. J. Heart Fail. 2022, 24, 727–729. [Google Scholar] [CrossRef]
- Gounaridi, M.I.; Vontetsianos, A.; Oikonomou, E.; Theofilis, P.; Chynkiamis, N.; Lampsas, S.; Anastasiou, A.; Papamikroulis, G.A.; Katsianos, E.; Kalogeras, K.; et al. The Role of Rehabilitation in Arterial Function Properties of Convalescent COVID-19 Patients. J. Clin. Med. 2023, 12, 2233. [Google Scholar] [CrossRef]
- Teixeira Do Amaral, V.; Viana, A.A.; Heubel, A.D.; Linares, S.N.; Martinelli, B.; Witzler, P.H.C.; Orikassa De Oliveira, G.Y.; Zanini, G.D.S.; Borghi Silva, A.; Mendes, R.G.; et al. Cardiovascular, Respiratory, and Functional Effects of Home-Based Exercise Training after COVID-19 Hospitalization. Med. Sci. Sports Exerc. 2022, 54, 1795–1803. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Study | Country | Study Group | No. of Patients | Age | Sex, Male | NOS Scale |
|---|---|---|---|---|---|---|
| Faria et al., 2023 [34] | Brazil | COVID-19 | 19 | 47 ± 8 | 12 (63.2%) | 8 |
| Control | 19 | 43 ± 10 | 11 (57.9%) | |||
| Tudoran et al., 2023 [35] | Romania | COVID-19 | 54 | 47.76 ± 5.43 | NS | 7 |
| Control | 40 | 49.47 ± 5.14 | NS | |||
| Nandadeva et al., 2023 [36] | United States | COVID-19 | 12 | 48 ± 9 | NS | 7 |
| Control | 11 | 50 ± 13 | NS | |||
| Oikonomou et al., 2023 [37] | Greece | COVID-19 | 34 | 57.2 ± 12.9 | 26 (76.5%) | 8 |
| Control | 34 | 57.4 ± 12.8 | 23 (67.6%) | |||
| Van der Sluijs et al., 2023 [38] | The Netherlands | COVID-19 | 31 | 57.5 ± 3.0 | 17 (54.8%) | 7 |
| Control | 31 | 56.5 ± 3.0 | 17 (54.8%) | |||
| Skow et al., 2022 [39] | United States | COVID-19 | 23 | 23 ± 3 | 9 (39.1%) | 8 |
| Control | 13 | 26 ± 4 | 6 (46.2%) | |||
| Lambadiari et al., 2021 [40] | Greece | COVID-19 | 70 | 54.53 ± 9.07 | 44 (62.85%) | 9 |
| Control | 70 | 54.77 ± 8.95 | 44 (62.85%) | |||
| Control | 34 | 57.4 ± 12.8 | 23 (67.6%) | |||
| Ratchford et al., 2021 [41] | United States | COVID-19 | 11 | 20.1 ± 1.1 | NS | 9 |
| Control | 20 | 23.0 ± 1.3 | NS | |||
| Schnaubelt et al., 2021 [42] | Austria | COVID-19 | 22 | 76.0 ± 4.25 | 11 (50.0%) | 8 |
| Control | 22 | 75.8 ± 4.0 | 10 (45.5%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jannasz, I.; Pruc, M.; Rahnama-Hezavah, M.; Targowski, T.; Olszewski, R.; Feduniw, S.; Petryka, K.; Szarpak, L. The Impact of COVID-19 on Carotid–Femoral Pulse Wave Velocity: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 5747. https://doi.org/10.3390/jcm12175747
Jannasz I, Pruc M, Rahnama-Hezavah M, Targowski T, Olszewski R, Feduniw S, Petryka K, Szarpak L. The Impact of COVID-19 on Carotid–Femoral Pulse Wave Velocity: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(17):5747. https://doi.org/10.3390/jcm12175747
Chicago/Turabian StyleJannasz, Iwona, Michal Pruc, Mansur Rahnama-Hezavah, Tomasz Targowski, Robert Olszewski, Stepan Feduniw, Karolina Petryka, and Lukasz Szarpak. 2023. "The Impact of COVID-19 on Carotid–Femoral Pulse Wave Velocity: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 17: 5747. https://doi.org/10.3390/jcm12175747
APA StyleJannasz, I., Pruc, M., Rahnama-Hezavah, M., Targowski, T., Olszewski, R., Feduniw, S., Petryka, K., & Szarpak, L. (2023). The Impact of COVID-19 on Carotid–Femoral Pulse Wave Velocity: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 12(17), 5747. https://doi.org/10.3390/jcm12175747