
Urgent Implantation of Peritoneal Dialysis Catheter in Chronic Kidney Disease and Acute Kidney Injury—A Review
 , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Technique and Preparation for USPD
3.1.1. Preoperative Measures for USPD
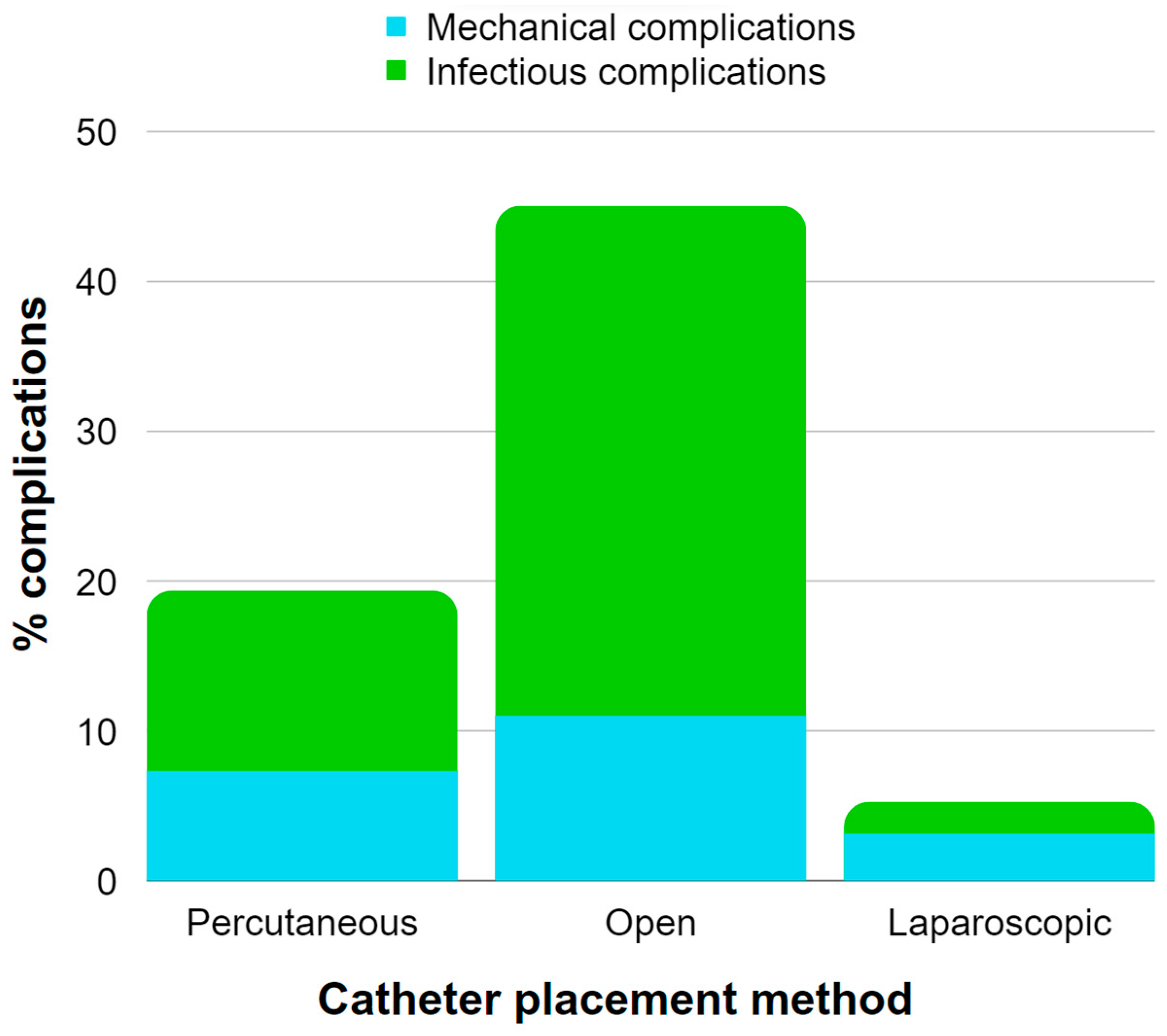
3.1.2. Insertion and Selection of Dialysis Catheter for USPD

| Paper | AKI/CKD | Catheter Placement Method | Mechanical Complications | Infectious Complications | Other Complications |
|---|---|---|---|---|---|
| I. Kaplan Bulut (2016) [33] | AKI (in children) | percutaneous | catheter malfunction (19.6%) | peritonitis (6%), catheter exit-site infection (6%) | no other complications reported |
| P. Choudhary (2021) [34] | AKI (in children) | percutaneous | hemorrhagic effluent and obstruction in flow (6%), pericatheter leakage (4%) | peritonitis (4%) | no other complications reported |
| P. Coccia (2021) [32] | AKI (in children) | open (84%) laparoscopic (7.6%) percutaneous (8.4%) | catheter malfunction (24%), fluid leakage (11.5%) | peritonitis (19%), | bleeding events (6%), hyperglycemia (2%) |
| A. Al-Hwiesh (2018) [35] | AKI | percutaneous | no mechanical complications reported | Infections (9.5%) | hypotension (15.9%), bleeding events (6.3%), arrhythmias (7.9%), hypoglycemia (4.8%), hypomagnesemia (11.1%), hypocalcemia (9.5%), hypophosphatemia (11.1%), thrombocytopenia (4.8%) |
| D. Gabriel (2009) [36] | AKI | percutaneous | no mechanical complications reported | peritonitis (18%) | no other complications reported |
| D. Ponce (2012) [37] | AKI | percutaneous | mechanical complications (7.3%) | peritonitis (12%) | no other complications reported |
| D. Ponce (2013) [38] | AKI | percutaneous | no mechanical complications reported | peritonitis (16.3%) | no other complications reported |
| N. Caplin (2020) [39] | AKI | percutaneous | leakage (23%) poor flow (5%) | no infectious complications reported | bleeding (15%) |
| Q. Soomro (2021) [40] | AKI | percutaneous | leakage (13.16%) | no infectious complications reported | no other complications reported |
| S. Cho (2017) [41] | AKI | percutaneous | leakage (8%) mechanical obstruction (4%) | no infectious complications reported | no other complications reported |
| T. Panaput (2021) [42] | AKI | percutaneous | no mechanical complications reported | catheter infection (1.6%) | no other complications reported |
| H. Ye (2019) [43] | CKD | open | abdominal wall complications (0.07%) | peritonitis (0.01%) | no other complications reported |
| E. Wojtaszek (2019) [44] | CKD | open | leakage (11%) | peritonitis (34%) | bleeding (9%) |
| W. Parapiboon (2022) [45] | CKD | percutaneous | pericatheter leakage (5%) | no infectious complications reported | hemoperitoneum (5%) |
| H. Jin (2016) [46] | CKD | laparoscopic | catheter malposition (3.1%) | peritonitis (2.1%) | no other complications reported |
| M. Koch (2012) [47] | CKD | laparoscopic | no mechanical complications reported | peritonitis (1.5%) | no other complications reported |

3.1.3. Initiation of Treatment and Aftercare in USPD
3.1.4. Dialysis Modes for Urgent Start
3.2. Peritoneal Dialysis in Management of Acute Kidney Injury
3.2.1. Indications for USPD Utilization in the Management of AKI
Indications for USPD in the Pediatric Population with AKI
Indications for USPD in the Adult Population with AKI
3.2.2. Contraindications for USPD Utilization in the Management of AKI
3.2.3. Underlying Comorbidities in AKI
3.2.4. Outcomes of USPD in AKI Management
Outcomes of USPD in Children with AKI
Outcomes of USPD in Adults with AKI
3.2.5. Other Factors Influencing USPD in AKI Management
3.3. Peritoneal Dialysis in Management of Chronic Kidney Disease
3.3.1. Indications for Dialysis Treatment in CKD Management
3.3.2. Contraindications for Peritoneal Dialysis in CKD Management
3.3.3. Underlying Comorbidities in CKD
3.3.4. Urgent vs. Conventional Start Dialysis in CKD Patients
| Paper | Number of Patients | Country | USPD/PD | Mechanical Complications | Infectious Complications | Other Complications |
|---|---|---|---|---|---|---|
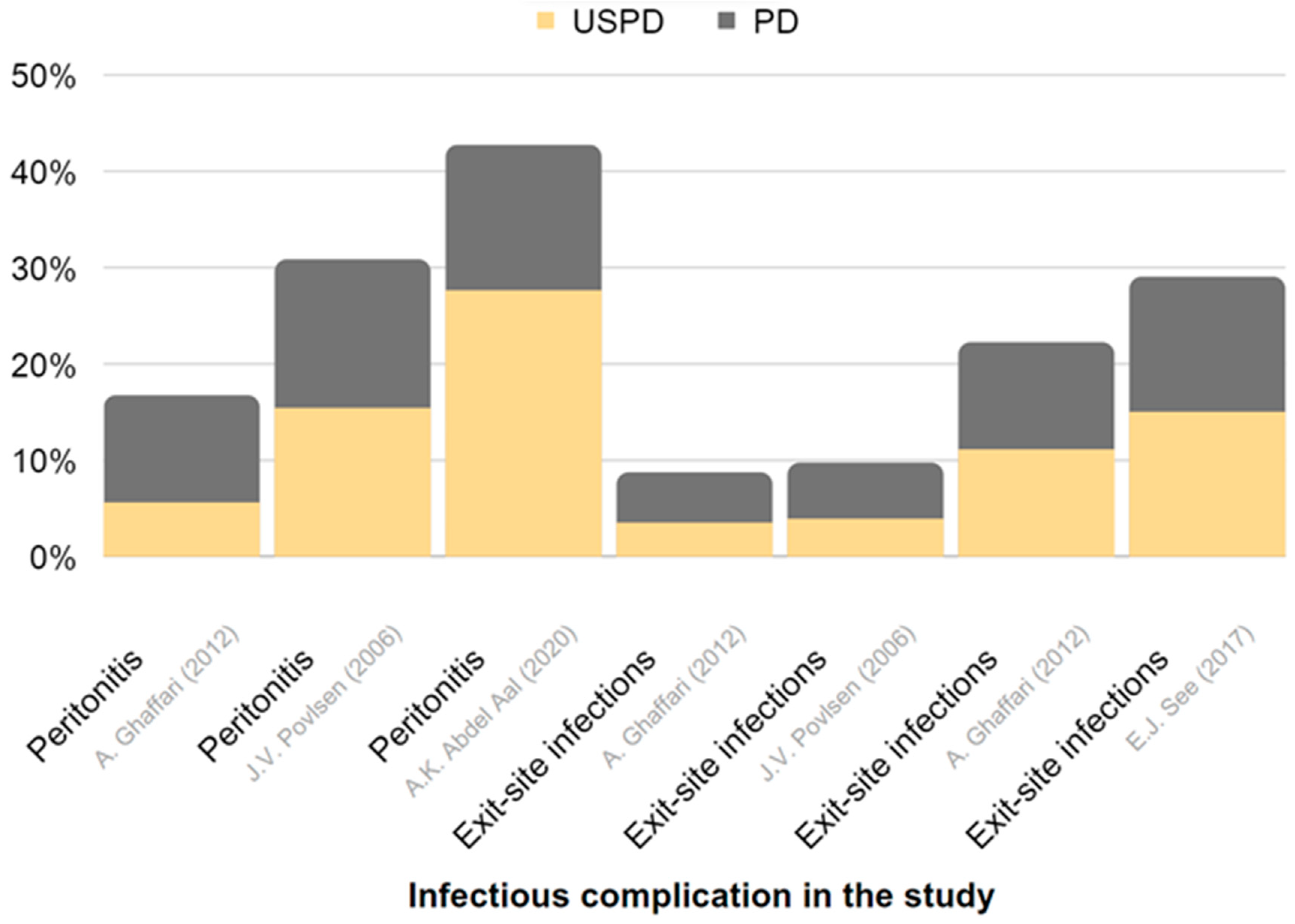
| Arshia Ghaffari (2012) [114] | 18 | USA | USPD | minor leaks (22.2%) | peritonitis (5.6%) exit-site infections (11.1%) | hematoma (5.6%) |
| 9 | USA | PD | major leaks (11.1%) | peritonitis (11.1%) exit-site infections (11.1%) | no complications reported | |
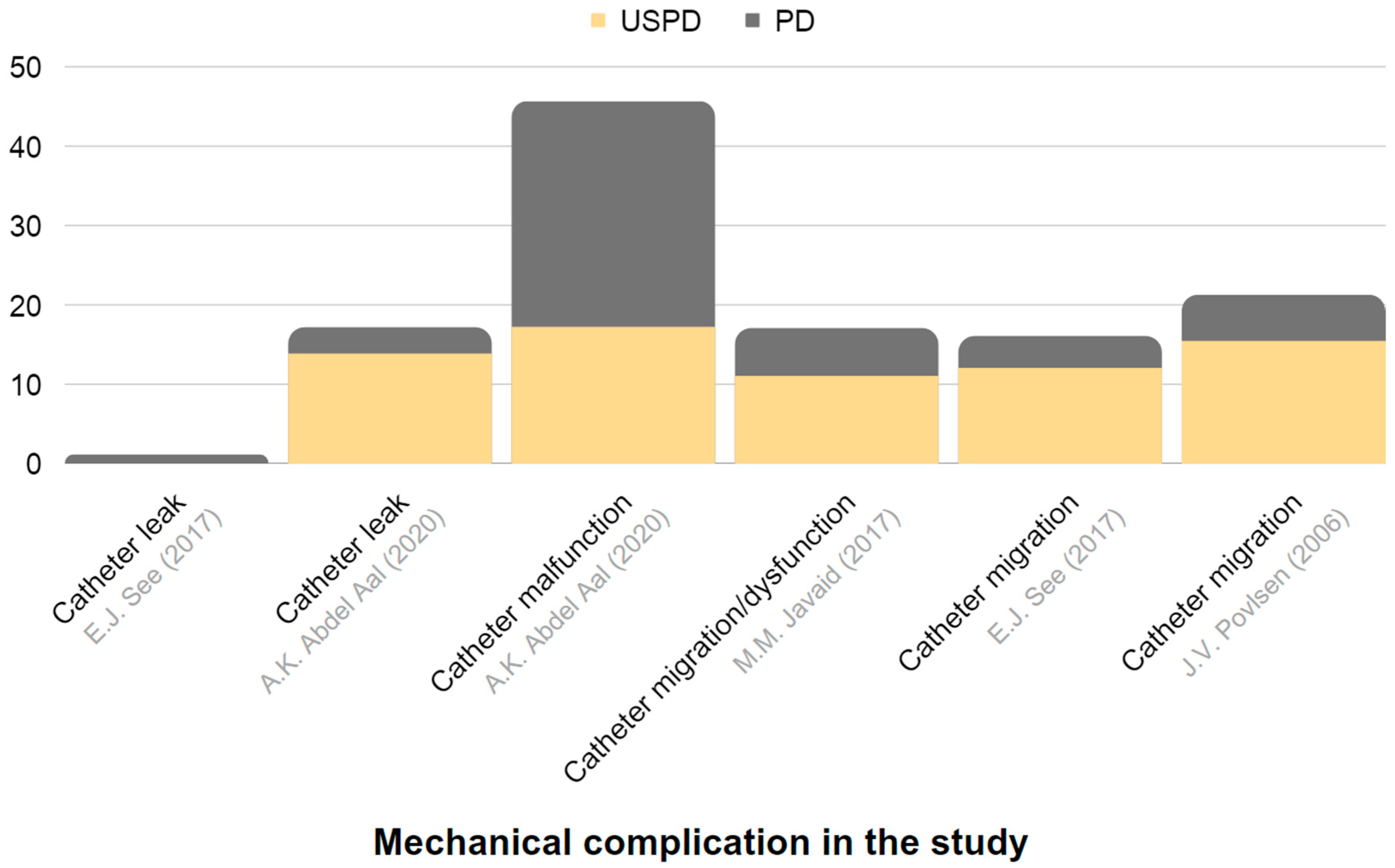
| Abdel-Aal (2020) [115] | 29 | USA | USPD | catheter malfunction (17.2%) catheter leak (13.8%) | peritonitis (27.6%) exit-site infections (3.5%) | hernia (10.3%) |
| 211 | USA | PD | catheter malfunction (28.4%) catheter leak (3.3%) | peritonitis (15.1%) exit-site infections (5.2%) | hernia (4.3%) muscle hematoma/bleeding (2.8%) | |
| Javaid et al. (2017) [116] | 17 | Singapore | USPD | catheter migration/dysfunction (11.0%) | no complications reported | no complications reported |
| 33 | Singapore | PD | catheter migration/dysfunction (6.0%) | no complications reported | no complications reported | |
| See et al. (2017) [113] | 26 | Australia | USPD | catheter leak (12%) catheter migration (12%) | exit-site infection (15%) | no complications reported |
| 78 | Australia | PD | catheter leak (1%) catheter migration (4%) | exit-site infection (14%) peritonitis (3%) | no complications reported | |
| Povlsen et al. (2006) [117] | 52 | Denmark | USPD | catheter leak (7.7%) catheter dysfunction (15.4%) | peritonitis (15.4%) exit-site infection (3.9%) | no complications reported |
| 88 | Denmark | PD | catheter migration (5.8%) | peritonitis (15.4%) exit-site infection (5.8%) | no complications reported |


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
3.3.5. Outcomes of USPD in CKD Management
4. Conclusions
5. Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- The United States Renal Data System. 2022 Annual Data Report. Available online: https://usrds-adr.niddk.nih.gov/2022/ (accessed on 9 March 2023).
- Raport 2019. Ogólnopolskie Badanie Pacjentów Nefrologicznych Kidney Disease: A Population-Based Polish Nationwide Study. Forum Nefrol. 2020, 13, 149–163.
- Dębska-Ślizień, A.; Rutkowski, B.; Jagodziński, P.; Rutkowski, P.; Przygoda, J.; Lewandowska, D.; Czerwiński, J.; Kamiński, A.; Gellert, R. Current status of renal replacement therapy in Poland in 2020. Nefrol. Dial. Pol. 2021, 25, 7–20. [Google Scholar]
- Statystyka Przeszczepiania Narządów 2020 r. Available online: https://www.poltransplant.org.pl/statystyka_2020.html (accessed on 9 March 2023).
- Marrón, B.; Ostrowski, J.; Török, M.; Timofte, D.; Orosz, A.; Kosicki, A.; Całka, A.; Moro, D.; Kosa, D.; Redl, J.; et al. Type of Referral, Dialysis Start and Choice of Renal Replacement Therapy Modality in an International Integrated Care Setting. PLoS ONE 2016, 11, e0155987. [Google Scholar] [CrossRef]
- Villa, G.; Fernández–Ortiz, L.; Cuervo, J.; Rebollo, P.; Selgas, R.; González, T.; Arrieta, J. Cost-Effectiveness Analysis of the Spanish Renal Replacement Therapy Program. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2012, 32, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Ledebo, I.; Ronco, C. The Best Dialysis Therapy? Results from an International Survey among Nephrology Professionals. NDT Plus 2008, 1, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Alain, M.; Adelaide, P.; Sahar, B.; Cécile, C.; Thierry, H.; Cécile, V. Deleterious Effects of Dialysis Emergency Start, Insights from the French REIN Registry. BMC Nephrol. 2018, 19, 233. [Google Scholar] [CrossRef]
- Crabtree, J.H.; Chow, K.-M. Peritoneal Dialysis Catheter Insertion. Semin. Nephrol. 2017, 37, 17–29. [Google Scholar] [CrossRef]
- Lobbedez, T.; Lecouf, A.; Ficheux, M.; Henri, P.; Hurault de Ligny, B.; Ryckelynck, J.P. Is Rapid Initiation of Peritoneal Dialysis Feasible in Unplanned Dialysis Patients? A Single-Centre Experience. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc.-Eur. Ren. Assoc. 2008, 23, 3290–3294. [Google Scholar] [CrossRef]
- Ghaffari, A.; Kalantar-Zadeh, K.; Lee, J.; Maddux, F.; Moran, J.; Nissenson, A. PD First: Peritoneal Dialysis as the Default Transition to Dialysis Therapy. Semin. Dial. 2013, 26, 706–713. [Google Scholar] [CrossRef]
- Rajora, N.; Shastri, S.; Pirwani, G.; Saxena, R. How To Build a Successful Urgent-Start Peritoneal Dialysis Program. Kidney360 2020, 1, 1165–1177. [Google Scholar] [CrossRef]
- McCullough, P.A.; Choi, J.P.; Feghali, G.A.; Schussler, J.M.; Stoler, R.M.; Vallabahn, R.C.; Mehta, A. Contrast-Induced Acute Kidney Injury. J. Am. Coll. Cardiol. 2016, 68, 1465–1473. [Google Scholar] [CrossRef] [PubMed]
- Peerapornratana, S.; Manrique-Caballero, C.L.; Gómez, H.; Kellum, J.A. Acute Kidney Injury from Sepsis: Current Concepts, Epidemiology, Pathophysiology, Prevention and Treatment. Kidney Int. 2019, 96, 1083–1099. [Google Scholar] [CrossRef] [PubMed]
- Ricci, Z.; Ronco, C.; D’Amico, G.; De Felice, R.; Rossi, S.; Bolgan, I.; Bonello, M.; Zamperetti, N.; Petras, D.; Salvatori, G.; et al. Practice Patterns in the Management of Acute Renal Failure in the Critically Ill Patient: An International Survey. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc.-Eur. Ren. Assoc. 2006, 21, 690–696. [Google Scholar] [CrossRef]
- Yeates, K.; Cruz, D.N.; Finkelstein, F.O. Re-Examination of the Role of Peritoneal Dialysis to Treat Patients with Acute Kidney Injury. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2012, 32, 238–241. [Google Scholar] [CrossRef]
- Crabtree, J.H. Peritoneal Dialysis Catheter Implantation: Avoiding Problems and Optimizing Outcomes. Semin. Dial. 2015, 28, 12–15. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Aal, A.K.; Dybbro, P.; Hathaway, P.; Guest, S.; Neuwirth, M.; Krishnamurthy, V. Best Practices Consensus Protocol for Peritoneal Dialysis Catheter Placement by Interventional Radiologists. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2014, 34, 481–493. [Google Scholar] [CrossRef]
- Ash, S.; Sequeira, A.; Narayan, R. Imaging and Peritoneal Dialysis Catheters. Semin. Dial. 2017, 30, 338–346. [Google Scholar] [CrossRef]
- Esagian, S.M.; Sideris, G.A.; Bishawi, M.; Ziogas, I.A.; Lehrich, R.W.; Middleton, J.P.; Suhocki, P.V.; Pappas, T.N.; Economopoulos, K.P. Surgical versus Percutaneous Catheter Placement for Peritoneal Dialysis: An Updated Systematic Review and Meta-Analysis. J. Nephrol. 2021, 34, 1681–1696. [Google Scholar] [CrossRef]
- Francois, K.; Clerck, D.D.; Robberechts, T.; Hulle, F.V.; Cauwelaert, S.V.; Luyten, I.; Jacobs-Tulleneers-Thevissen, D. Percutaneous Insertion of Peritoneal Dialysis Catheters by the Nephrologist (Modified Seldinger Technique). Bull. Dial. Domic. 2021, 4, 277–288. [Google Scholar] [CrossRef]
- Yu, Y.; Xie, Q.; Chen, Y.; Hu, W.; Zhang, P.; Huang, S.; Yang, F.; He, Y.; Yi, Y.; Zhou, J.; et al. Ultrasound-Guided Modified Seldinger Placement of Tenckhoff Catheters in Pediatric Patients Undergoing Peritoneal Dialysis: Single Center Experience. Front. Pediatr. 2022, 10, 1–6. [Google Scholar] [CrossRef]
- Reddy, C.; Dybbro, P.E.; Guest, S. Fluoroscopically Guided Percutaneous Peritoneal Dialysis Catheter Placement: Single Center Experience and Review of the Literature. Ren. Fail. 2010, 32, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Maya, I.D. Ultrasound/Fluoroscopy-Assisted Placement of Peritoneal Dialysis Catheters. Semin. Dial. 2007, 20, 611–615. [Google Scholar] [CrossRef] [PubMed]
- Cao, W.; Tu, C.; Jia, T.; Liu, C.; Zhang, L.; Zhao, B.; Liu, J.; Zhang, L. Prophylactic Laparoscopic Omentopexy: A New Technique for Peritoneal Dialysis Catheter Placement. Ren. Fail. 2019, 41, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Danielsson, A.; Blohmé, L.; Tranaeus, A.; Hylander, B. A Prospective Randomized Study of the Effect of a Subcutaneously “Buried” Peritoneal Dialysis Catheter Technique versus Standard Technique on the Incidence of Peritonitis and Exit-Site Infection. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2002, 22, 211–219. [Google Scholar] [CrossRef]
- Minguela, I.; Lanuza, M.; Ruiz de Gauna, R.; Rodado, R.; Alegría, S.; Andreu, A.J.; González, M.J.; Rodríguez, B.; Vítores, J.M.; Castellanos, T.; et al. Lower Malfunction Rate with Self-Locating Catheters. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2001, 3 (Suppl. S21), S209–S212. [Google Scholar] [CrossRef]
- Kang, S.H.; Park, J.W.; Cho, K.H.; Do, J.Y. Comparison of Peritoneal Dialysis Catheter Insertion Techniques by Nephrologists: Surgical vs Blind Methods. Semin. Dial. 2021, 34, 31–37. [Google Scholar] [CrossRef]
- Crabtree, J.H.; Shrestha, B.M.; Chow, K.-M.; Figueiredo, A.E.; Povlsen, J.V.; Wilkie, M.; Abdel-Aal, A.; Cullis, B.; Goh, B.-L.; Briggs, V.R.; et al. Creating and Maintaining Optimal Peritoneal Dialysis Access in the Adult Patient: 2019 Update. Perit. Dial. Int. 2019, 39, 414–436. [Google Scholar] [CrossRef]
- Blake, P. Drain Pain, Overfill, and How They Are Connected. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2014, 34, 342–344. [Google Scholar] [CrossRef]
- Javaid, M.M.; Khan, B.A.; Subramanian, S. Is Surgical PD Catheter Insertion Safe for Urgent-start Peritoneal Dialysis? Semin. Dial. 2019, 32, 225–228. [Google Scholar] [CrossRef]
- Coccia, P.A.; Ramírez, F.B.; Suárez, A.D.C.; Alconcher, L.F.; Balestracci, A.; García Chervo, L.A.; Principi, I.; Vázquez, A.; Ratto, V.M.; Planells, M.C.; et al. Acute Peritoneal Dialysis, Complications and Outcomes in 389 Children with STEC-HUS: A Multicenter Experience. Pediatr. Nephrol. Berl. Ger. 2021, 36, 1597–1606. [Google Scholar] [CrossRef]
- Kaplan Bulut, I.; Kara, O.D.; Ozdemir, K.; Dincel, N.; Yilmaz, E.; Bulut, M.O.; Sozeri, B.; Bicer, H.; Mir, S. Are We Late for the Diagnosis of Acute Kidney Injury in the Intensive Care Units in Pediatric Patients? A Preliminary, Retrospective Observational Study among 66 Patients. Minerva Pediatr. 2016, 68, 256–261. [Google Scholar]
- Choudhary, P.; Kumar, V.; Saha, A.; Thakur, A. Peritoneal Dialysis in Critically Ill Children in Resource-Limited Setting: A Prospective Cohort Study. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2021, 41, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Al-Hwiesh, A.; Abdul-Rahman, I.; Finkelstein, F.; Divino-Filho, J.; Qutub, H.; Al-Audah, N.; Abdelrahman, A.; El-Fakhrany, N.; Nasr El-Din, M.; El-Salamony, T.; et al. Acute Kidney Injury in Critically Ill Patients: A Prospective Randomized Study of Tidal Peritoneal Dialysis Versus Continuous Renal Replacement Therapy. Ther. Apher. Dial. 2018, 22, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, D.P.; Caramori, J.T.; Martin, L.C.; Barretti, P.; Balbi, A.L. Continuous Peritoneal Dialysis Compared with Daily Hemodialysis in Patients with Acute Kidney Injury. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2009, 29 (Suppl. S2), S62–S71. [Google Scholar] [CrossRef]
- Ponce, D.; Berbel, M.N.; Regina de Goes, C.; Almeida, C.T.P.; Balbi, A.L. High-Volume Peritoneal Dialysis in Acute Kidney Injury: Indications and Limitations. Clin. J. Am. Soc. Nephrol. CJASN 2012, 7, 887–894. [Google Scholar] [CrossRef]
- Ponce, D.; Berbel, M.N.; Abrão, J.M.G.; Goes, C.R.; Balbi, A.L. A Randomized Clinical Trial of High Volume Peritoneal Dialysis versus Extended Daily Hemodialysis for Acute Kidney Injury Patients. Int. Urol. Nephrol. 2013, 45, 869–878. [Google Scholar] [CrossRef] [PubMed]
- Caplin, N.J.; Zhdanova, O.; Tandon, M.; Thompson, N.; Patel, D.; Soomro, Q.; Ranjeeta, F.; Joseph, L.; Scherer, J.; Joshi, S.; et al. Acute Peritoneal Dialysis During the COVID-19 Pandemic at Bellevue Hospital in New York City. Kidney360 2020, 1, 1345–1352. [Google Scholar] [CrossRef]
- Soomro, Q.H.; Mukherjee, V.; Amerling, R.; Caplin, N. Case Series of Acute Peritoneal Dialysis in the Prone Position for Acute Kidney Injury during the Covid-19 Pandemic: Prone to Complications? Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2021, 41, 328–332. [Google Scholar] [CrossRef]
- Cho, S.; Lee, Y.-J.; Kim, S.-R. Acute Peritoneal Dialysis in Patients with Acute Kidney Injury. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2017, 37, 529–534. [Google Scholar] [CrossRef]
- Panaput, T.; Peerapornratana, S.; Sirivongrangson, P.; Kulvichit, W.; Lumlertgul, N.; Jonny, J.; Praditpornsilpa, K.; Tungsanga, K.; Eiam-Ong, S.; Srisawat, N. Modalities of Renal Replacement Therapy and Clinical Outcomes of Patients with Acute Kidney Injury in a Resource-Limited Setting: Results from a SEA-AKI Study. J. Crit. Care 2021, 65, 18–25. [Google Scholar] [CrossRef]
- Ye, H.; Yang, X.; Yi, C.; Guo, Q.; Li, Y.; Yang, Q.; Chen, W.; Mao, H.; Li, J.; Qiu, Y.; et al. Urgent-Start Peritoneal Dialysis for Patients with End Stage Renal Disease: A 10-Year Retrospective Study. BMC Nephrol. 2019, 20, 238. [Google Scholar] [CrossRef] [PubMed]
- Wojtaszek, E.; Grzejszczak, A.; Grygiel, K.; Małyszko, J.; Matuszkiewicz-Rowińska, J. Urgent-Start Peritoneal Dialysis as a Bridge to Definitive Chronic Renal Replacement Therapy: Short- and Long-Term Outcomes. Front. Physiol. 2018, 9, 1830. [Google Scholar] [CrossRef]
- Parapiboon, W.; Sangsuk, J.; Nopsopon, T.; Pitsawong, W.; Tatiyanupanwong, S.; Kanjanabuch, T.; Johnson, D.W. Randomized Study of Urgent-Start Peritoneal Dialysis Versus Urgent-Start Temporary Hemodialysis in Patients Transitioning to Kidney Failure. Kidney Int. Rep. 2022, 7, 1866–1877. [Google Scholar] [CrossRef] [PubMed]
- Jin, H.; Fang, W.; Zhu, M.; Yu, Z.; Fang, Y.; Yan, H.; Zhang, M.; Wang, Q.; Che, X.; Xie, Y.; et al. Urgent-Start Peritoneal Dialysis and Hemodialysis in ESRD Patients: Complications and Outcomes. PLoS ONE 2016, 11, e0166181. [Google Scholar] [CrossRef] [PubMed]
- Koch, M.; Kohnle, M.; Trapp, R.; Haastert, B.; Rump, L.C.; Aker, S. Comparable Outcome of Acute Unplanned Peritoneal Dialysis and Haemodialysis. Nephrol. Dial. Transplant. 2012, 27, 375–380. [Google Scholar] [CrossRef]
- Ma, Y.; Liu, S.; Yang, M.; Zou, Y.; Xue, D.; Liu, Y.; Wang, Y.; Xie, X.; Chen, H. Association between Different Peritoneal Dialysis Catheter Placement Methods and Short-Term Postoperative Complications. BMC Nephrol. 2021, 22, 151. [Google Scholar] [CrossRef]
- Hayat, A.; Collins, J.; Saweirs, W. Study of Early Complications Associated with Peritoneal Dialysis Catheters: An Analysis of the New Zealand Peritoneal Dialysis Registry Data. Int. Urol. Nephrol. 2021, 53, 1705–1711. [Google Scholar] [CrossRef]
- Li, P.K.-T.; Szeto, C.C.; Piraino, B.; de Arteaga, J.; Fan, S.; Figueiredo, A.E.; Fish, D.N.; Goffin, E.; Kim, Y.-L.; Salzer, W.; et al. ISPD Peritonitis Recommendations: 2016 Update on Prevention and Treatment. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2016, 36, 481–508. [Google Scholar] [CrossRef]
- Brodalka, E.; Suchowierska, E.; Naumnik, B. Is It Mandatory to Apply Dressing on the Exit Site of the Tenckhoff Catheter? Ren. Dis. Transplant. Forum 2022, 15, 32–35. [Google Scholar] [CrossRef]
- Xu, D.; Liu, T.; Dong, J. Urgent-Start Peritoneal Dialysis Complications: Prevalence and Risk Factors. Am. J. Kidney Dis. 2017, 70, 102–110. [Google Scholar] [CrossRef]
- Chiu, M.; Jain, A.K.; Blake, P.G. Truly Urgent “Urgent-Start” Peritoneal Dialysis. Kidney Int. Rep. 2020, 5, 1625–1626. [Google Scholar] [CrossRef] [PubMed]
- Van Biesen, W.; Verger, C.; Heaf, J.; Vrtovsnik, F.; Britto, Z.M.L.; Do, J.-Y.; Prieto-Velasco, M.; Martínez, J.P.; Crepaldi, C.; De Los Ríos, T.; et al. Evolution Over Time of Volume Status and PD-Related Practice Patterns in an Incident Peritoneal Dialysis Cohort. Clin. J. Am. Soc. Nephrol. CJASN 2019, 14, 882–893. [Google Scholar] [CrossRef]
- Phongphithakchai, A.; Dandecha, P.; Raksasuk, S.; Srithongkul, T. Urgent-Start Peritoneal Dialysis for End-Stage Renal Disease Patients: Literature Review and Worldwide Evidence-Based Practice. Ren. Replace. Ther. 2021, 7, 65. [Google Scholar] [CrossRef]
- Parapiboon, W.; Jamratpan, T. Intensive Versus Minimal Standard Dosage for Peritoneal Dialysis in Acute Kidney Injury: A Randomized Pilot Study. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2017, 37, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Goossen, K.; Becker, M.; Marshall, M.R.; Bühn, S.; Breuing, J.; Firanek, C.A.; Hess, S.; Nariai, H.; Sloand, J.A.; Yao, Q.; et al. Icodextrin Versus Glucose Solutions for the Once-Daily Long Dwell in Peritoneal Dialysis: An Enriched Systematic Review and Meta-Analysis of Randomized Controlled Trials. Am. J. Kidney Dis. 2020, 75, 830–846. [Google Scholar] [CrossRef]
- Roumeliotis, A.; Roumeliotis, S.; Leivaditis, K.; Salmas, M.; Eleftheriadis, T.; Liakopoulos, V. APD or CAPD: One Glove Does Not Fit All. Int. Urol. Nephrol. 2021, 53, 1149–1160. [Google Scholar] [CrossRef]
- Xie, J.; Wang, H.; Li, S.; Zuo, Y.; Wang, Y.; Zhang, Y.; Liang, T.; Li, J.; Wang, L.; Feng, Z.; et al. Low-Volume Tidal Peritoneal Dialysis Is a Preferable Mode in Patients Initiating Urgent-Start Automated Peritoneal Dialysis: A Randomized, Open-Label, Prospective Control Study. Ther. Apher. Dial. 2019, 23, 409–417. [Google Scholar] [CrossRef]
- Rabindranath, K.S.; Adams, J.; Ali, T.Z.; MacLeod, A.M.; Vale, L.; Cody, J.D.; Wallace, S.A.; Daly, C. Continuous Ambulatory Peritoneal Dialysis versus Automated Peritoneal Dialysis for End-stage Renal Disease. Cochrane Database Syst. Rev. 2007, 2007, CD006515. [Google Scholar] [CrossRef]
- Brown, E.A.; Davies, S.J.; Heimbürger, O.; Meeus, F.; Mellotte, G.; Rosman, J.; Rutherford, P.; Van Bree, M.; European Automated Peritoneal Dialysis Outcomes Study (EAPOS) Investigators. Adequacy Targets Can Be Met in Anuric Patients by Automated Peritoneal Dialysis: Baseline Data from EAPOS. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2001, 21 (Suppl. S3), S133–S137. [Google Scholar] [CrossRef]
- Cullis, B.; Al-Hwiesh, A.; Kilonzo, K.; McCulloch, M.; Niang, A.; Nourse, P.; Parapiboon, W.; Ponce, D.; Finkelstein, F.O. ISPD Guidelines for Peritoneal Dialysis in Acute Kidney Injury: 2020 Update (Adults). Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2021, 41, 15–31. [Google Scholar] [CrossRef]
- Nourse, P.; Cullis, B.; Finkelstein, F.; Numanoglu, A.; Warady, B.; Antwi, S.; McCulloch, M. ISPD Guidelines for Peritoneal Dialysis in Acute Kidney Injury: 2020 Update (Paediatrics). Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2021, 41, 139–157. [Google Scholar] [CrossRef]
- Jetton, J.G.; Boohaker, L.J.; Sethi, S.K.; Wazir, S.; Rohatgi, S.; Soranno, D.E.; Chishti, A.S.; Woroniecki, R.; Mammen, C.; Swanson, J.R.; et al. Incidence and Outcomes of Neonatal Acute Kidney Injury (AWAKEN): A Multicentre, Multinational, Observational Cohort Study. Lancet Child Adolesc. Health 2017, 1, 184–194. [Google Scholar] [CrossRef]
- Kellum, J.A.; Lameire, N. Diagnosis, Evaluation, and Management of Acute Kidney Injury: A KDIGO Summary (Part 1). Crit. Care 2013, 17, 204. [Google Scholar] [CrossRef]
- Sutherland, S.M.; Byrnes, J.J.; Kothari, M.; Longhurst, C.A.; Dutta, S.; Garcia, P.; Goldstein, S.L. AKI in Hospitalized Children: Comparing the PRIFLE, AKIN, and KDIGO Definitions. Clin. J. Am. Soc. Nephrol. 2015, 10, 554–561. [Google Scholar] [CrossRef]
- Sethi, S.K.; Wazir, S.; Sahoo, J.; Agrawal, G.; Bajaj, N.; Gupta, N.P.; Mirgunde, S.; Balachandran, B.; Afzal, K.; Shrivastava, A.; et al. Risk Factors and Outcomes of Neonates with Acute Kidney Injury Needing Peritoneal Dialysis: Results from the Prospective TINKER (The Indian PCRRT-ICONIC Neonatal Kidney Educational Registry) Study. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2022, 42, 460–469. [Google Scholar] [CrossRef] [PubMed]
- Evans, R.D.R.; Docherty, M.; Seeley, A.; Craik, A.; Mpugna, M.; Mann, S.; Dube, Q.; Dreyer, G.; Hemmila, U. Incidence, Etiology, and Outcomes of Community-Acquired Acute Kidney Injury in Pediatric Admissions in Malawi. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2018, 38, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Hirano, D.; Ito, A.; Yamada, A.; Kakegawa, D.; Miwa, S.; Umeda, C.; Chiba, K.; Takemasa, Y.; Tokunaga, A.; Ida, H. Independent Risk Factors and 2-Year Outcomes of Acute Kidney Injury after Surgery for Congenital Heart Disease. Am. J. Nephrol. 2017, 46, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Bojan, M.; Vicca, S.; Lopez-Lopez, V.; Mogenet, A.; Pouard, P.; Falissard, B.; Journois, D. Predictive Performance of Urine Neutrophil Gelatinase-Associated Lipocalin for Dialysis Requirement and Death Following Cardiac Surgery in Neonates and Infants. Clin. J. Am. Soc. Nephrol. 2014, 9, 285–294. [Google Scholar] [CrossRef]
- Wang, F.; Hong, D.; Wang, Y.; Feng, Y.; Wang, L.; Yang, L. Renal Replacement Therapy in Acute Kidney Injury from a Chinese Cross-Sectional Study: Patient, Clinical, Socioeconomic and Health Service Predictors of Treatment. BMC Nephrol. 2017, 18, 152. [Google Scholar] [CrossRef]
- Nawaz, S.; Afzal, K. Pediatric Acute Kidney Injury in North India: A Prospective Hospital-Based Study. Saudi J. Kidney Dis. Transplant. 2018, 29, 689–697. [Google Scholar] [CrossRef]
- Lombardi, R.; Rosa-Diez, G.; Ferreiro, A.; Greloni, G.; Yu, L.; Younes-Ibrahim, M.; Burdmann, E.A.; Acute Kidney Injury Committee of the Latin American Society of Nephrology and Hypertension Working Group. Acute Kidney Injury in Latin America: A View on Renal Replacement Therapy Resources. Nephrol. Dial. Transplant. 2014, 29, 1369–1376. [Google Scholar] [CrossRef] [PubMed]
- Riley, A.A.; Jefferies, J.L.; Nelson, D.P.; Bennett, M.R.; Blinder, J.J.; Ma, Q.; Devarajan, P.; Goldstein, S.L. Peritoneal Dialysis Does Not Adversely Affect Kidney Function Recovery after Congenital Heart Surgery. Int. J. Artif. Organs 2014, 37, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-de-Toledo, J.; Perez-Ortiz, A.; Gil, L.; Baust, T.; Linés-Palazón, M.; Perez-Hoyos, S.; Gran, F.; Abella, R.F. Early Initiation of Renal Replacement Therapy in Pediatric Heart Surgery Is Associated with Lower Mortality. Pediatr. Cardiol. 2016, 37, 623–628. [Google Scholar] [CrossRef]
- Dittrich, S.; Vogel, M.; Dähnert, I.; Haas, N.A.; Alexi-Meskishvili, V.; Lange, P.E. Acute Hemodynamic Effects of Post Cardiotomy Peritoneal Dialysis in Neonates and Infants. Intensiv. Care Med. 2000, 26, 101–104. [Google Scholar] [CrossRef]
- Sourial, M.; Gone, A.; Uribarri, J.; Srivatana, V.; Sharma, S.; Shimonov, D. Outcomes of PD for AKI Treatment during COVID-19 in New York City: A Multicenter Study. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2023, 43, 13–22. [Google Scholar] [CrossRef]
- Garg, N.; Kumar, V.; Sohal, P.M.; Jain, D.; Jain, A.; VikasMakkar; Mehta, S. Efficacy and Outcome of Intermittent Peritoneal Dialysis in Patients with Acute Kidney Injury: A Single-Center Experience. Saudi J. Kidney Dis. Transplant. 2020, 31, 423–430. [Google Scholar] [CrossRef]
- Chan, L.; Chaudhary, K.; Saha, A.; Chauhan, K.; Vaid, A.; Zhao, S.; Paranjpe, I.; Somani, S.; Richter, F.; Miotto, R.; et al. AKI in Hospitalized Patients with COVID-19. J. Am. Soc. Nephrol. 2021, 32, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Spector, B.L.; Misurac, J.M. Renal Replacement Therapy in Neonates. Neoreviews 2019, 20, e697–e710. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.-K.; Kao, C.-C.; Tseng, C.-H.; Hsu, C.-E.; Lin, Y.-J.; Chen, Y.-C.; Lin, C.; Huang, C.-Y. Noninvasive Hemodynamic Profiles during Hemodialysis in Patients with and without Heart Failure. Cardiorenal Med. 2020, 10, 243–256. [Google Scholar] [CrossRef]
- Warady, B.A.; Schaefer, F.; Bagga, A.; Cano, F.; McCulloch, M.; Yap, H.-K.; Shroff, R. Prescribing Peritoneal Dialysis for High-Quality Care in Children. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2020, 40, 333–340. [Google Scholar] [CrossRef]
- Prasad, N.; Gupta, A.; Mathew, M.; Abraham, G. Access-Related Complications in Peritoneal Dialysis in Developing Countries. Adv. Ren. Replace. Ther. 2002, 9, 144–148. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.; Jha, V. Community-Acquired AKI in Asia: An Update. Semin. Nephrol. 2020, 40, 456–467. [Google Scholar] [CrossRef] [PubMed]
- Lameire, N.; Kellum, J.A. Contrast-Induced Acute Kidney Injury and Renal Support for Acute Kidney Injury: A KDIGO Summary (Part 2). Crit. Care 2013, 17, 205. [Google Scholar] [CrossRef] [PubMed]
- George, J.; Varma, S.; Kumar, S.; Thomas, J.; Gopi, S.; Pisharody, R. Comparing Continuous Venovenous Hemodiafiltration and Peritoneal Dialysis in Critically Ill Patients with Acute Kidney Injury: A Pilot Study. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2011, 31, 422–429. [Google Scholar] [CrossRef]
- Basu, B.; Mahapatra, T.K.S.; Roy, B.; Schaefer, F. Efficacy and Outcomes of Continuous Peritoneal Dialysis versus Daily Intermittent Hemodialysis in Pediatric Acute Kidney Injury. Pediatr. Nephrol. 2016, 31, 1681–1689. [Google Scholar] [CrossRef]
- Guzzo, I.; de Galasso, L.; Mir, S.; Bulut, I.K.; Jankauskiene, A.; Burokiene, V.; Cvetkovic, M.; Kostic, M.; Bayazit, A.K.; Yildizdas, D.; et al. Acute Dialysis in Children: Results of a European Survey. J. Nephrol. 2019, 32, 445–451. [Google Scholar] [CrossRef]
- Obiagwu, P.N.; Abdu, A. Peritoneal Dialysis vs. Haemodialysis in the Management of Paediatric Acute Kidney Injury in Kano, Nigeria: A Cost Analysis. Trop. Med. Int. Health 2015, 20, 2–7. [Google Scholar] [CrossRef]
- Sourial, M.Y.; Sourial, M.H.; Dalsan, R.; Graham, J.; Ross, M.; Chen, W.; Golestaneh, L. Urgent Peritoneal Dialysis in Patients with COVID-19 and Acute Kidney Injury: A Single-Center Experience in a Time of Crisis in the United States. Am. J. Kidney Dis. 2020, 76, 401–406. [Google Scholar] [CrossRef]
- Bello, A.; Levin, A.; Lunney, M.; Osman, M.; Ye, F. Global Kidney Health Atlas: A Report by the International Society of Nephrology on the Global Burden of End-Stage Kidney Disease and Capacity for Kidney Replacement Therapy and Conservative Care across World Countries and Regions. 2019. Available online: https://www.theisn.org/wp-content/uploads/2021/05/GKHAtlas_2019_WebFIle-1.pdf (accessed on 9 March 2023).
- Kovesdy, C.P. Epidemiology of Chronic Kidney Disease: An Update 2022. Kidney Int. Suppl. 2022, 12, 7–11. [Google Scholar] [CrossRef]
- Chronic Kidney Disease Prognosis Consortium; Matsushita, K.; van der Velde, M.; Astor, B.C.; Woodward, M.; Levey, A.S.; de Jong, P.E.; Coresh, J.; Gansevoort, R.T. Association of Estimated Glomerular Filtration Rate and Albuminuria with All-Cause and Cardiovascular Mortality in General Population Cohorts: A Collaborative Meta-Analysis. Lancet 2010, 375, 2073–2081. [Google Scholar] [CrossRef]
- GBD 2013 Mortality and Causes of Death Collaborators Global, Regional, and National Age-Sex Specific All-Cause and Cause-Specific Mortality for 240 Causes of Death, 1990-2013: A Systematic Analysis for the Global Burden of Disease Study 2013. Lancet 2015, 385, 117–171. [CrossRef] [PubMed]
- ISN. Summary of Recommendation Statements. Kidney Int. Suppl. 2013, 3, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Anderson, S.; Halter, J.B.; Hazzard, W.R.; Himmelfarb, J.; Horne, F.M.; Kaysen, G.A.; Kusek, J.W.; Nayfield, S.G.; Schmader, K.; Tian, Y.; et al. Prediction, Progression, and Outcomes of Chronic Kidney Disease in Older Adults. J. Am. Soc. Nephrol. 2009, 20, 1199–1209. [Google Scholar] [CrossRef]
- Cooper, B.A.; Branley, P.; Bulfone, L.; Collins, J.F.; Craig, J.C.; Fraenkel, M.B.; Harris, A.; Johnson, D.W.; Kesselhut, J.; Li, J.J.; et al. A Randomized, Controlled Trial of Early versus Late Initiation of Dialysis. N. Engl. J. Med. 2010, 363, 609–619. [Google Scholar] [CrossRef]
- Zhao, Y.; Pei, X.; Zhao, W. Timing of Dialysis Initiation and Mortality Risk in Chronic Kidney Disease: A Meta-Analysis. Ther. Apher. Dial. 2018, 22, 600–608. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Xu, X.D.; Guo, L.L.; Cai, L.L.; Jin, H.M. Association of Early versus Late Initiation of Dialysis with Mortality: Systematic Review and Meta-Analysis. Nephron Clin. Pract. 2012, 120, c121–c131. [Google Scholar] [CrossRef]
- Okuda, Y.; Soohoo, M.; Tang, Y.; Obi, Y.; Laster, M.; Rhee, C.M.; Streja, E.; Kalantar-Zadeh, K. Estimated GFR at Dialysis Initiation and Mortality in Children and Adolescents. Am. J. Kidney Dis. 2019, 73, 797–805. [Google Scholar] [CrossRef]
- Abdulkarim, S.; Shah, J.; Twahir, A.; Sokwala, A.P. Eligibility and Patient Barriers to Peritoneal Dialysis in Patients with Advanced Chronic Kidney Disease. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2021, 41, 463–471. [Google Scholar] [CrossRef]
- Jonny; Violetta, L.; Kusumaningrum, V.F. Peritoneal Dialysis in Indonesia: Current Status, Challenges and Prospects. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2022, 42, 428–433. [Google Scholar] [CrossRef]
- Eroglu, E.; Heimbürger, O.; Lindholm, B. Peritoneal Dialysis Patient Selection from a Comorbidity Perspective. Semin. Dial. 2022, 35, 25–39. [Google Scholar] [CrossRef]
- Xie, X.-S.; Xie, Z.-T.; Xiang, S.-L.; Yan, X.-Q.; Zhang, X.-H.; Shou, Z.-F.; Chen, J.-H. Peritoneal Dialysis for Autosomal Dominant Polycystic Kidney Disease: A Retrospective Study. J. Zhejiang Univ. B 2016, 17, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Griva, K.; Yu, Z.; Chan, S.; Krisnasamy, T.; Yamin, R.B.A.; Zakaria, F.B.; Wu, S.Y.; Oei, E.; Foo, M. Age Is Not a Contraindication to Home-Based Dialysis-Quality-of-Life Outcomes Favour Older Patients on Peritoneal Dialysis Regimes Relative to Younger Patients. J. Adv. Nurs. 2014, 70, 1902–1914. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, S.; Niwa, T. Advanced Glycation End-Products and Peritoneal Sclerosis. Semin. Nephrol. 2004, 24, 502–505. [Google Scholar] [CrossRef] [PubMed]
- Milan Manani, S.; Rosner, M.H.; Virzì, G.M.; Giuliani, A.; Berti, S.; Crepaldi, C.; Ronco, C. Longitudinal Experience with Remote Monitoring for Automated Peritoneal Dialysis Patients. Nephron 2019, 142, 1–9. [Google Scholar] [CrossRef]
- Al-Dorzi, H.M.; Al-Sum, H.; Alqurashi, S.; Aljaser, S.J.; Arabi, Y.M. Severe Hypoglycemia in Peritoneal Dialysis Patients Due to Overestimation of Blood Glucose by the Point-of-Care Glucometer. Saudi J. Kidney Dis. Transplant. 2011, 22, 764–768. [Google Scholar]
- Kiran, V.R.; Zhu, T.Y.; Yip, T.; Lui, S.L.; Lo, W.K. Body Mass Index and Mortality Risk in Asian Peritoneal Dialysis Patients in Hong Kong—Impact of Diabetes and Cardiovascular Disease Status. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2014, 34, 390–398. [Google Scholar] [CrossRef]
- McDonald, S.P.; Collins, J.F.; Rumpsfeld, M.; Johnson, D.W. Obesity Is a Risk Factor for Peritonitis in the Australian and New Zealand Peritoneal Dialysis Patient Populations. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2004, 24, 340–346. [Google Scholar] [CrossRef]
- Heimbürger, O. Obesity on PD Patients: Causes and Management. Contrib. Nephrol. 2003, 140, 91–97. [Google Scholar] [CrossRef]
- Phang, C.C.; Foo, M.W.Y.; Johnson, D.W.; Wu, S.Y.; Hao, Y.; Jayaballa, M.; Koniman, R.; Chan, C.M.; Oei, E.L.; Chong, T.T.; et al. Comparison of Outcomes of Urgent-Start and Conventional-Start Peritoneal Dialysis: A Single-Centre Experience. Int. Urol. Nephrol. 2021, 53, 583–590. [Google Scholar] [CrossRef]
- See, E.J.; Cho, Y.; Hawley, C.M.; Jaffrey, L.R.; Johnson, D.W. Early and Late Patient Outcomes in Urgent-Start Peritoneal Dialysis. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2017, 37, 414–419. [Google Scholar] [CrossRef]
- Ghaffari, A. Urgent-Start Peritoneal Dialysis: A Quality Improvement Report. Am. J. Kidney Dis. 2012, 59, 400–408. [Google Scholar] [CrossRef]
- Abdel Aal, A.K.; Mahmoud, K.; Moustafa, A.S.; Aboueldahab, N.A.; Souid, A.; Gunn, A.; Li, Y.; Wang, Z.; Almehmi, A. Comparative Study on the Outcomes of Elective-Start versus Urgent-Start Peritoneal Dialysis Catheter Placement. Radiol. Res. Pract. 2020, 2020, 3751827. [Google Scholar] [CrossRef]
- Javaid, M.M.; Lee, E.; Khan, B.A.; Subramanian, S. Description of an Urgent-Start Peritoneal Dialysis Program in Singapore. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2017, 37, 500–502. [Google Scholar] [CrossRef] [PubMed]
- Povlsen, J.V.; Ivarsen, P. How to Start the Late Referred ESRD Patient Urgently on Chronic APD. Nephrol. Dial. Transplant. 2006, 21 (Suppl. S2), ii56–ii59. [Google Scholar] [CrossRef]
- Mendes, M.L.; Alves, C.A.; Marinho, L.C.R.; Dias, D.B.; Ponce, D. Unplanned vs. Planned Peritoneal Dialysis as Initial Therapy for Dialysis Patients in Chronic Kidney Replacement Therapy. Int. Urol. Nephrol. 2022, 54, 1417–1425. [Google Scholar] [CrossRef] [PubMed]
- Htay, H.; Johnson, D.W.; Craig, J.C.; Teixeira-Pinto, A.; Hawley, C.M.; Cho, Y. Urgent-start Peritoneal Dialysis versus Haemodialysis for People with Chronic Kidney Disease. Cochrane Database Syst. Rev. 2021, 2021, CD012899. [Google Scholar] [CrossRef]
- Machowska, A.; Alscher, M.D.; Vanga, S.R.; Koch, M.; Aarup, M.; Qureshi, A.R.; Lindholm, B.; Rutherford, P. Dialysis Access, Infections, and Hospitalisations in Unplanned Dialysis Start Patients: Results from the Options Study. Int. J. Artif. Organs 2017, 40, 48–59. [Google Scholar] [CrossRef] [PubMed]
- Pilatti, M.; Theodorovitz, V.C.; Hille, D.; Sevignani, G.; Ferreira, H.C.; Vieira, M.A.; Calice-Silva, V.; França, P.H.C. de Urgent vs. Planned Peritoneal Dialysis Initiation: Complications and Outcomes in the First Year of Therapy. Braz. J. Nephrol. 2022, 44, 482–489. [Google Scholar] [CrossRef]
- Chan, C.T.; Blankestijn, P.J.; Dember, L.M.; Gallieni, M.; Harris, D.C.H.; Lok, C.E.; Mehrotra, R.; Stevens, P.E.; Wang, A.Y.-M.; Cheung, M.; et al. Dialysis Initiation, Modality Choice, Access, and Prescription: Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2019, 96, 37–47. [Google Scholar] [CrossRef]



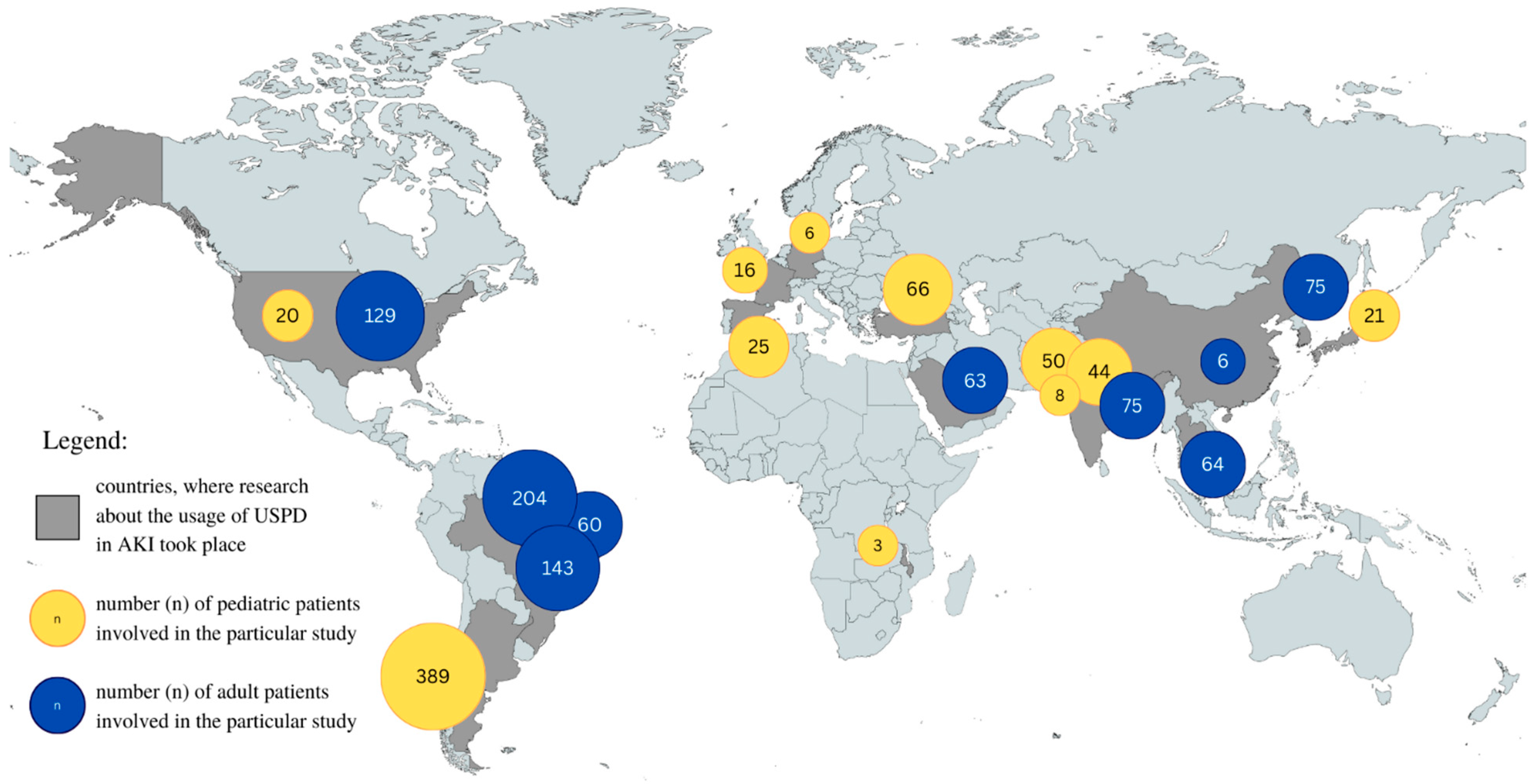
| Paper | Patients Type | Number of Patients | Country | Continent |
|---|---|---|---|---|
| A. Riley (2015) [74] | Children | 20 | USA | North America |
| D. Hirano (2017) [69] | Children | 21 | Japan | Asia |
| I. Kaplan Bulut (2016) [33] | Children | 66 | Turkey | Asia |
| J. Sanchez-de-Toledo (2016) [75] | Children | 25 | Spain | Europe |
| M. Bojan (2014) [70] | Children | 16 | Paris | Europe |
| P. Choudhary (2021) [34] | Children | 50 | India | Asia |
| P. Coccia (2021) [32] | Children | 389 | Argentina | South America |
| R. Evans (2018) [68] | Children | 3 | Malawi | Africa |
| S. Dittrich (2000) [76] | Children | 6 | Berlin | Europe |
| S. Sethi (2022) [67] | Children | 44 | India | Asia |
| S. Nawaz (2018) [72] | Children | 8 | India | Asia |
| A. Al-Hwiesh (2018) [34] | Adult | 63 | Saudi Arabia | Asia |
| D. Gabriel (2009) [36] | Adult | 60 | Brazil | South America |
| D. Ponce (2012) [37] | Adult | 204 | Brazil | South America |
| D. Ponce (2013) [38] | Adult | 143 | Brazil | South America |
| F. Wang (2017) [71] | Adult | 6 | China | Asia |
| M. Sourial (2022) [77] | Adult | 93 | USA | North America |
| N. Caplin (2020) [39] | Adult | 29 | USA | North America |
| N. Garg (2020) [78] | Adult | 75 | India | Asia |
| Q. Soomro (2021) [40] | Adult | 7 | USA | North America |
| S. Cho (2017) [41] | Adult | 75 | Korea | Asia |
| T. Panaput (2021) [42] | Adult | 64 | Thailand, Indonesia | Asia |
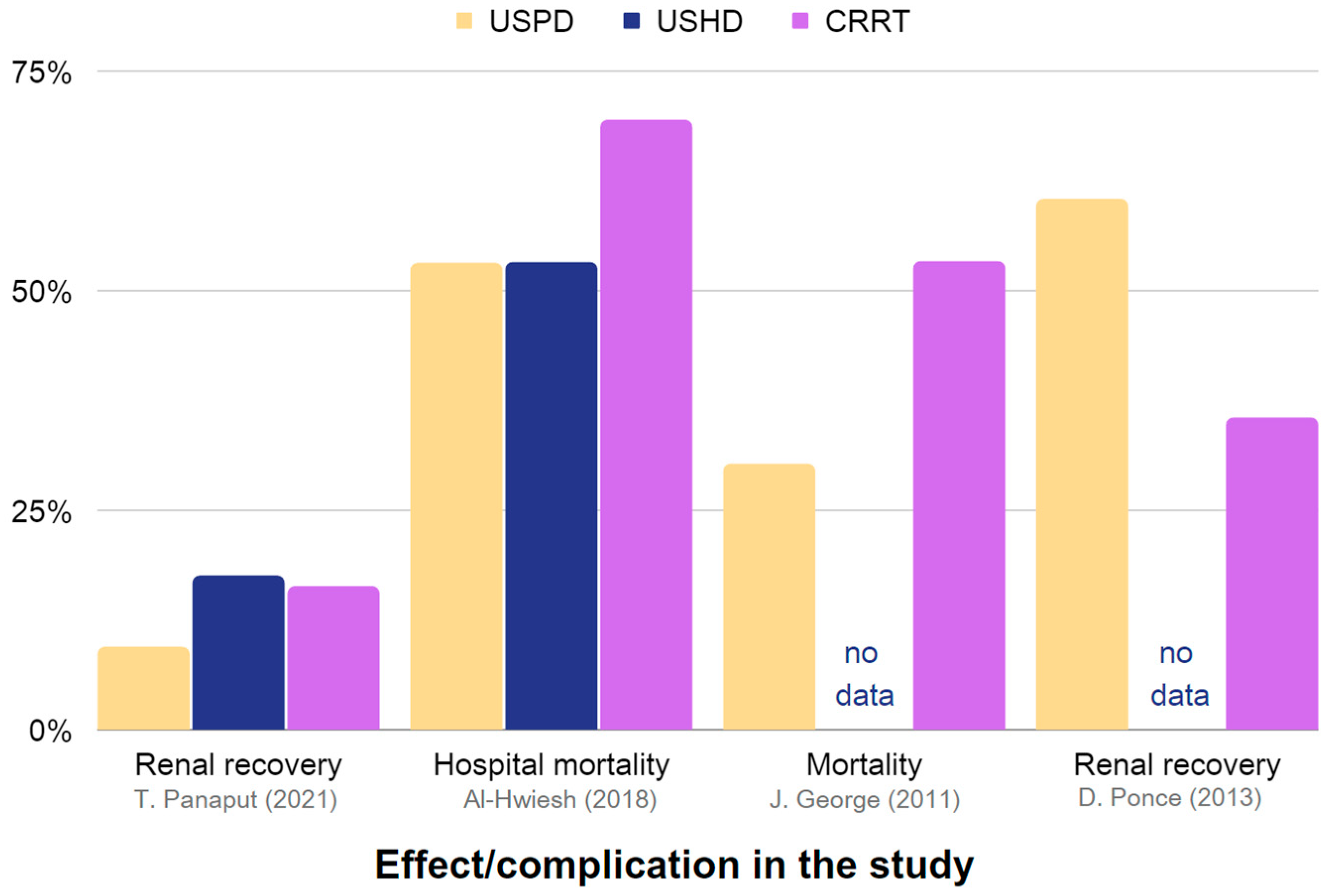
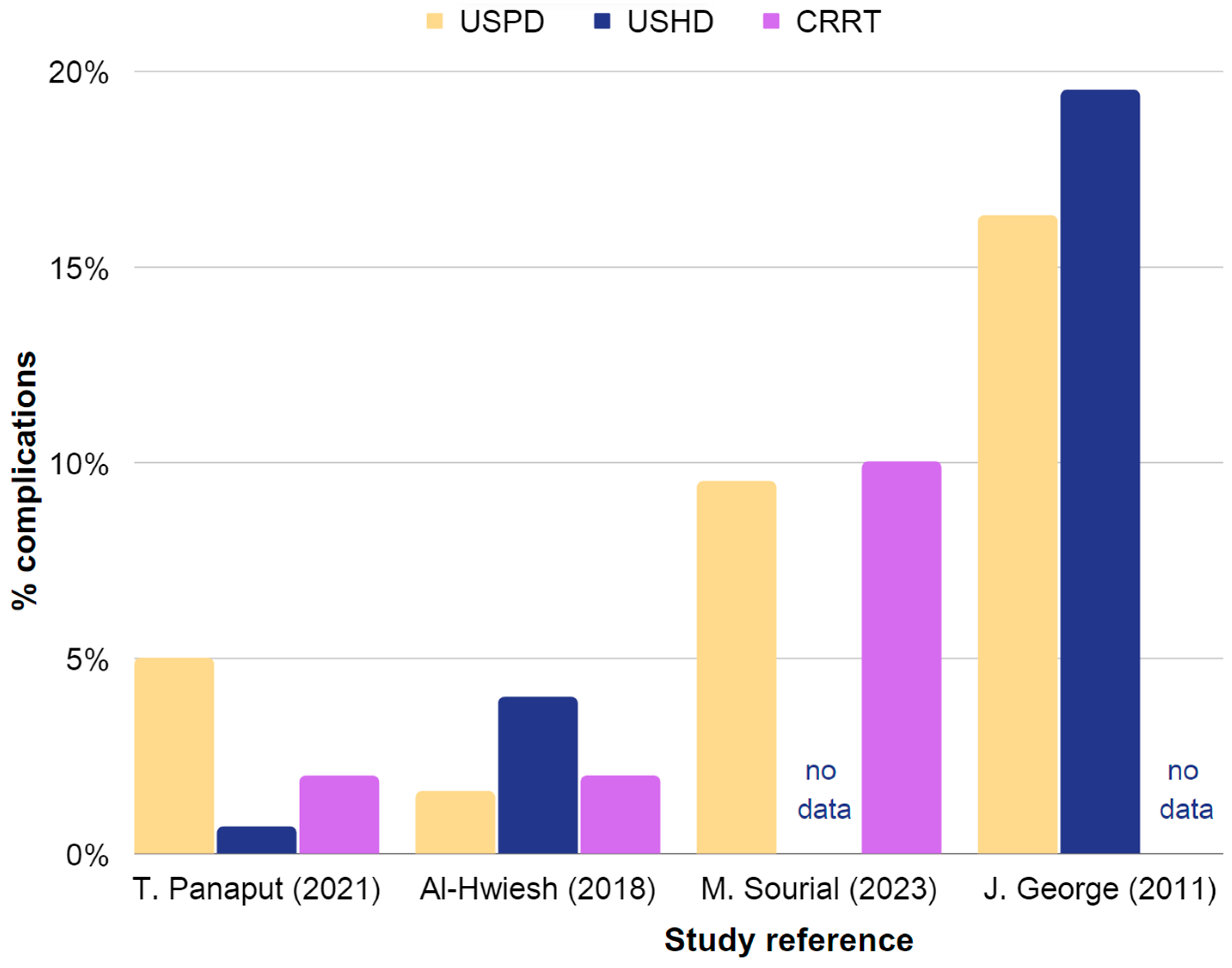
| Paper | USPD in AKI | USHD in AKI | CRRT in AKI | |||
|---|---|---|---|---|---|---|
| Effectiveness | Complications | Effectiveness | Complications | Effectiveness | Complications | |
| T. Panaput (2021) [42] | 9.4% renal recovery | 5% air embolism | 17.5% renal recovery | 0.7% bleeding | 16.3% renal recovery | 2% major arrhythmia |
| A. Al-Hwiesh (2018) [35] | 53.1% hospital mortality | 1.6% catheter infection | 53.2% hospital mortality | 4% major arrhythmia | 69.4% hospital mortality | 2% catheter malfunction |
| M. Sourial (2022) [77] | 9 days LOS | 9.5% infectious complications | 16 days LOS | no data | 17 days LOS | 10% hypertension |
| D. Ponce (2013) [38] | 60.3% renal recovery | no data | no data | no data | 35.5% renal recovery | 17.7% infectious complications |
| J. George (2011) [86] | 30.2% mortality | 16.3% infectious complications | 20% renal recovery | 19.5% infectious complications | 53.2% mortality | no data |
| B. Basu (2017) [87] | 9-day ICU LOS | 4% hypotension | 60% mortality | no data | 19-day ICU LOS | no data |
| Advantages of USPD in AKI | Disadvantages of USPD in AKI |
|---|---|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cholerzyńska, H.; Zasada, W.; Michalak, H.; Miedziaszczyk, M.; Oko, A.; Idasiak-Piechocka, I. Urgent Implantation of Peritoneal Dialysis Catheter in Chronic Kidney Disease and Acute Kidney Injury—A Review. J. Clin. Med. 2023, 12, 5079. https://doi.org/10.3390/jcm12155079
Cholerzyńska H, Zasada W, Michalak H, Miedziaszczyk M, Oko A, Idasiak-Piechocka I. Urgent Implantation of Peritoneal Dialysis Catheter in Chronic Kidney Disease and Acute Kidney Injury—A Review. Journal of Clinical Medicine. 2023; 12(15):5079. https://doi.org/10.3390/jcm12155079
Chicago/Turabian StyleCholerzyńska, Hanna, Wiktoria Zasada, Hanna Michalak, Miłosz Miedziaszczyk, Andrzej Oko, and Ilona Idasiak-Piechocka. 2023. "Urgent Implantation of Peritoneal Dialysis Catheter in Chronic Kidney Disease and Acute Kidney Injury—A Review" Journal of Clinical Medicine 12, no. 15: 5079. https://doi.org/10.3390/jcm12155079
APA StyleCholerzyńska, H., Zasada, W., Michalak, H., Miedziaszczyk, M., Oko, A., & Idasiak-Piechocka, I. (2023). Urgent Implantation of Peritoneal Dialysis Catheter in Chronic Kidney Disease and Acute Kidney Injury—A Review. Journal of Clinical Medicine, 12(15), 5079. https://doi.org/10.3390/jcm12155079