
The Efficacy of Daily Local Antibiotic Lavage via an Epidural Suction–Irrigation Drainage Technique in Spondylodiscitis and Isolated Spinal Epidural Empyema: A 20-Year Experience of a Single Spine Center

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Data
2.1.1. Study Design
2.1.2. Institutional Review Board and Electronic Patient Data Software
2.1.3. Patient Data
2.2. Clinical Management and Microbiological Assessment
2.2.1. Assessment of Clinical, Microbiological, and Radiological Diagnostics
2.2.2. Antibiotic and Surgical Management
Surgical Treatment
Choice between ESID and NON-ESID Techniques in ISEE and SD
Epidural Suction–Irrigation Drainage
Antibiotic Treatment
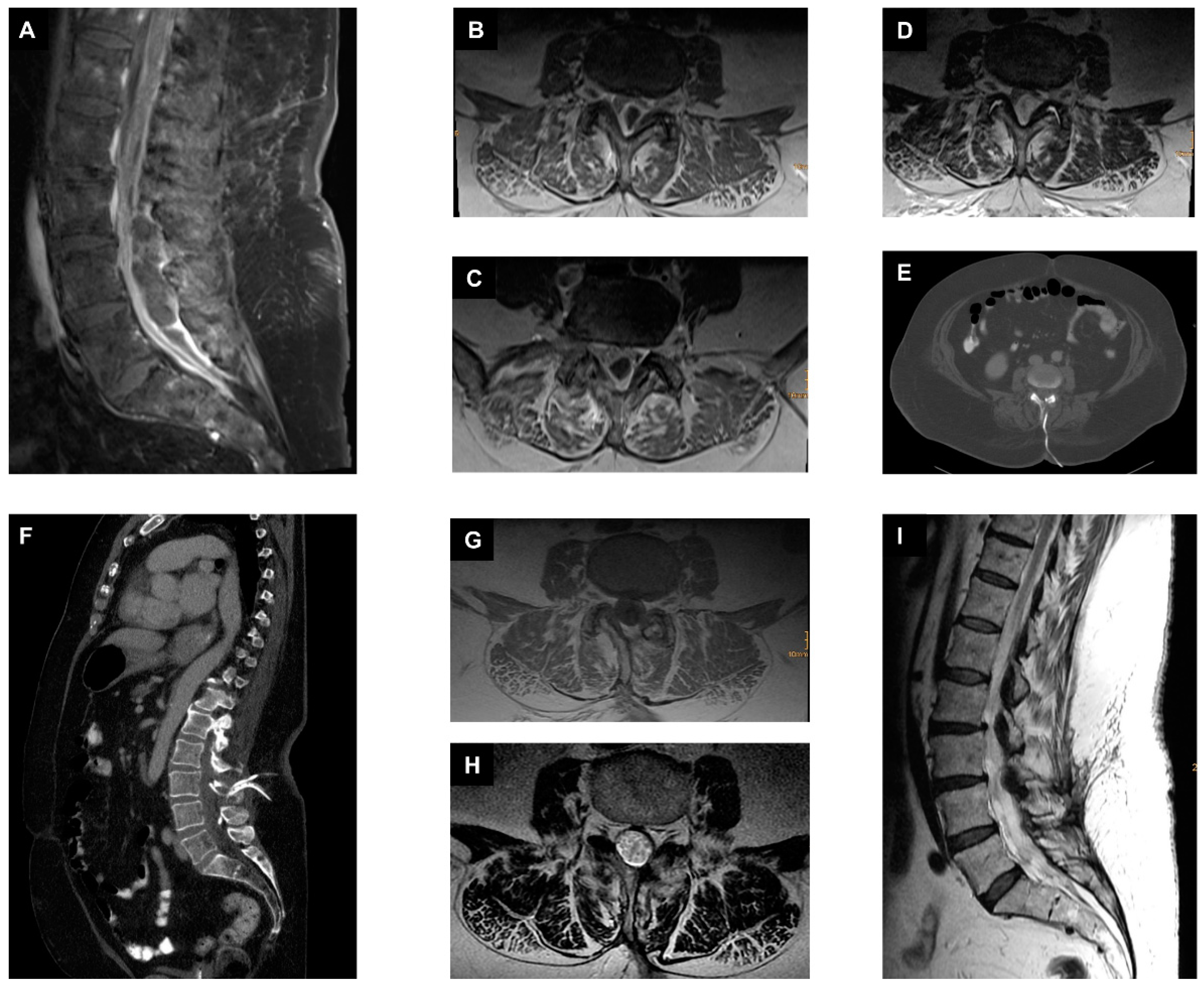
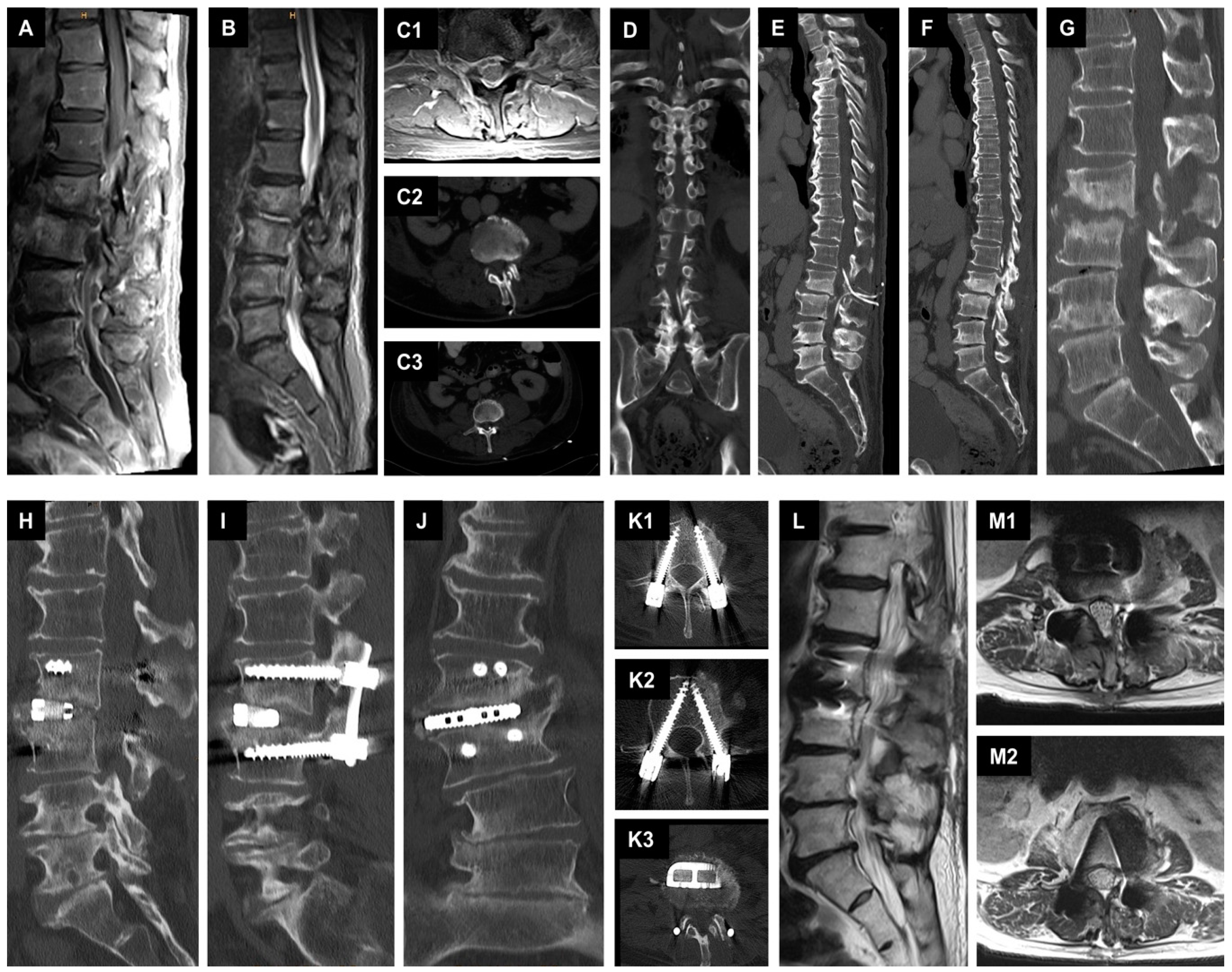
2.3. Illustrative Cases
2.3.1. First Case with Isolated Spinal Epidural Empyema
2.3.2. Second Case with Spondylodiscitis and Epidural Empyema
2.4. Statistical Analysis
3. Results
3.1. General Baseline Characteristics
3.2. ESID Group vs. NON-ESID Group
3.2.1. Baseline Factors
3.2.2. Risk Factors
3.2.3. Disease-Related Complications
3.3. ESID Group vs. NON-ESID Group in Spondylodiscitis
3.3.1. Baseline Factors
3.3.2. Risk Factors
3.3.3. Disease-Related Complications
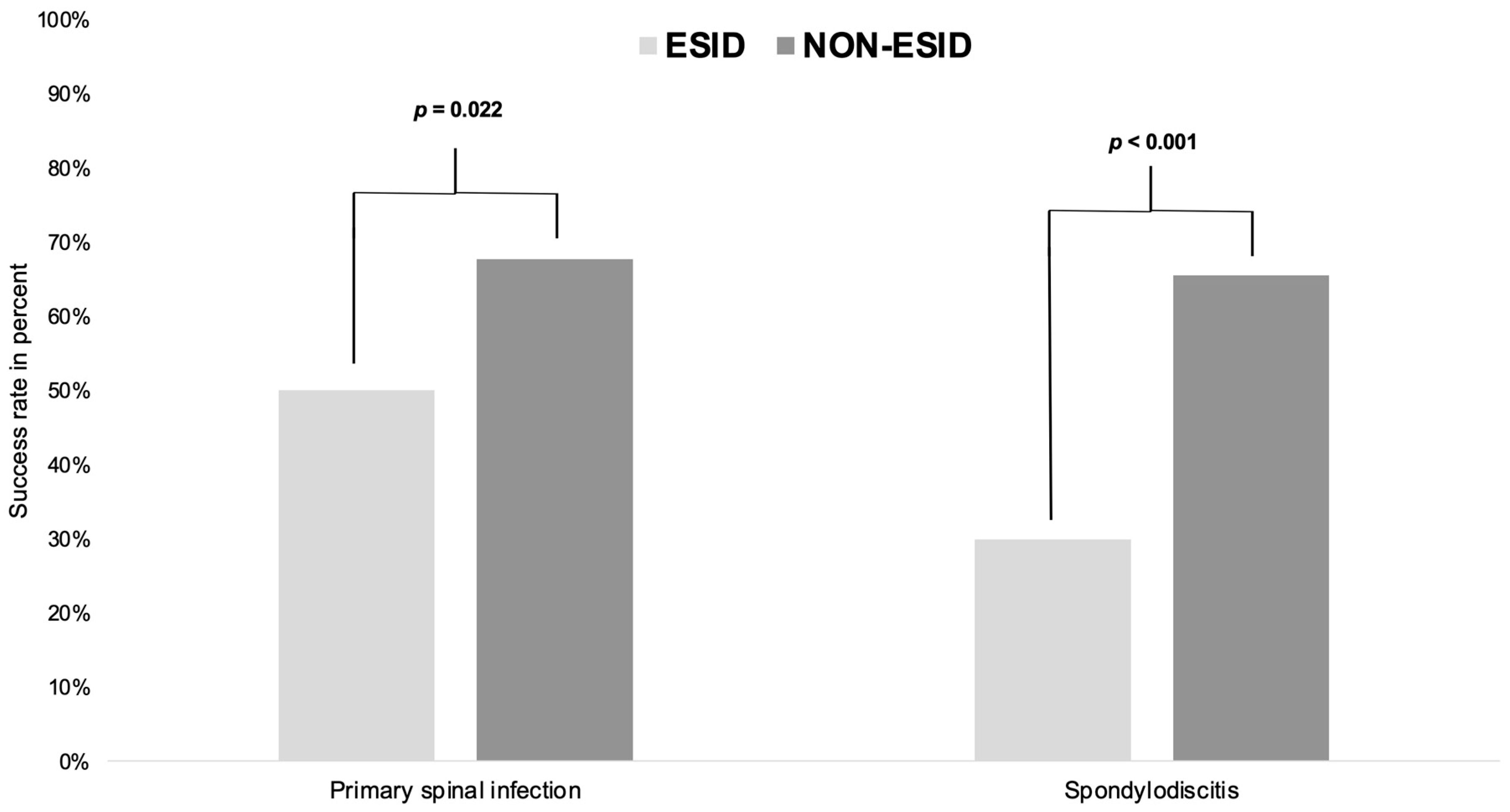
3.4. Success Rate
3.5. Multivariate Analyses
4. Discussion
- Baseline factors:
- Risk factors:
- Disease-related complications:
- Success rate:
- Multivariate analyses:
- Limitations and strengths of this study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lener, S.; Hartmann, S.; Barbagallo, G.M.V.; Certo, F.; Thome, C.; Tschugg, A. Management of spinal infection: A review of the literature. Acta Neurochir. 2018, 160, 487–496. [Google Scholar] [CrossRef] [PubMed]
- Fleege, C.; Rauschmann, M.; Arabmotlagh, M.; Rickert, M. Development and current use of local antibiotic carriers in spondylodiscitis: Pilot study on reduction of duration of systemic treatment. Orthopade 2020, 49, 714–723. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.; Kang, Y.J.; Chen, W.H. Continuous Epidural Irrigation and Drainage Combined with Posterior Debridement and Posterior Lumbar Inter-Body Fusion for the Management of Single-Segment Lumbar Pyogenic Spondylodiscitis. Surg. Infect. 2020, 21, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Tschoeke, S.K.; Kayser, R.; Gulow, J.; Hoeh, N.; Salis-Soglio, G.; Heyde, C. Single-stage epidural catheter lavage with posterior spondylodesis in lumbar pyogenic spondylodiscitis with multilevel epidural abscess formation. J. Neurol. Surg. A Cent. Eur. Neurosurg. 2014, 75, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Mauer, U.M.; Kunz, U. Spinal epidural empyema. Limited surgical treatment combined with continuous irrigation and drainage. Unfallchirurg 2007, 110, 250–254. [Google Scholar] [CrossRef] [PubMed]
- Ran, B.; Chen, X.; Zhong, Q.; Fu, M.; Wei, J. CT-guided minimally invasive treatment for an extensive spinal epidural abscess: A case report and literature review. Eur. Spine J. 2018, 27, 380–385. [Google Scholar] [CrossRef]
- Ito, M.; Abumi, K.; Kotani, Y.; Kadoya, K.; Minami, A. Clinical outcome of posterolateral endoscopic surgery for pyogenic spondylodiscitis: Results of 15 patients with serious comorbid conditions. Spine 2007, 32, 200–206. [Google Scholar] [CrossRef]
- Yang, S.C.; Fu, T.S.; Chen, H.S.; Kao, Y.H.; Yu, S.W.; Tu, Y.K. Minimally invasive endoscopic treatment for lumbar infectious spondylitis: A retrospective study in a tertiary referral center. BMC Musculoskelet Disord. 2014, 15, 105. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.; Humphrey, J.S.; Schenkman, D.I.; Seaber, A.V.; Vail, T.P. Gentamicin distribution from a collagen carrier. J. Orthop. Res. 1996, 14, 749–754. [Google Scholar] [CrossRef]
- Ascherl, R.; Stemberg, A.; Lechner, F.; Blumel, G. Local treatment of infection with collagen gentamicin. Aktuelle Probl. Chir. Orthop. 1990, 34, 85–93. [Google Scholar]
- Lohr, M.; Reithmeier, T.; Ernestus, R.I.; Ebel, H.; Klug, N. Spinal epidural abscess: Prognostic factors and comparison of different surgical treatment strategies. Acta Neurochir. 2005, 147, 159–166; discussion 166. [Google Scholar] [CrossRef] [PubMed]
- Hijazi, M.M.; Siepmann, T.; El-Battrawy, I.; Glatte, P.; Eyupoglu, I.; Schackert, G.; Juratli, T.A.; Podlesek, D. Clinical phenotyping of spondylodiscitis and isolated spinal epidural empyema: A 20-year experience and cohort study. Front. Surg. 2023, 10, 1200432. [Google Scholar] [CrossRef] [PubMed]
- Ryang, Y.M.; Akbar, M. Pyogenic spondylodiscitis: Symptoms, diagnostics and therapeutic strategies. Orthopade 2020, 49, 691–701. [Google Scholar] [CrossRef] [PubMed]
- Herren, C.; Jung, N.; Pishnamaz, M.; Breuninger, M.; Siewe, J.; Sobottke, R. Spondylodiscitis: Diagnosis and Treatment Options. Dtsch. Arztebl. Int. 2017, 114, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Tsai, T.T.; Yang, S.C.; Niu, C.C.; Lai, P.L.; Lee, M.H.; Chen, L.H.; Chen, W.J. Early surgery with antibiotics treatment had better clinical outcomes than antibiotics treatment alone in patients with pyogenic spondylodiscitis: A retrospective cohort study. BMC Musculoskelet. Disord. 2017, 18, 175. [Google Scholar] [CrossRef] [PubMed]
- Homagk, L.; Homagk, N.; Klauss, J.R.; Roehl, K.; Hofmann, G.O.; Marmelstein, D. Spondylodiscitis severity code: Scoring system for the classification and treatment of non-specific spondylodiscitis. Eur. Spine J. 2016, 25, 1012–1020. [Google Scholar] [CrossRef] [PubMed]
- Pojskic, M.; Carl, B.; Schmockel, V.; Vollger, B.; Nimsky, C.; Sabeta, B. Neurosurgical Management and Outcome Parameters in 237 Patients with Spondylodiscitis. Brain Sci. 2021, 11, 1019. [Google Scholar] [CrossRef] [PubMed]
- Bydon, M.; De la Garza-Ramos, R.; Macki, M.; Naumann, M.; Sciubba, D.M.; Wolinsky, J.P.; Bydon, A.; Gokaslan, Z.L.; Witham, T.F. Spinal instrumentation in patients with primary spinal infections does not lead to greater recurrent infection rates: An analysis of 118 cases. World Neurosurg. 2014, 82, e807–e814. [Google Scholar] [CrossRef] [PubMed]
- Dietz, N.; Sharma, M.; Alhourani, A.; Ugiliweneza, B.; Wang, D.; Nuno, M.; Drazin, D.; Boakye, M. Outcomes of decompression and fusion for treatment of spinal infection. Neurosurg. Focus 2019, 46, E7. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Baseline Factors | ESID (n = 146, 70.2%) | NON-ESID (n = 62, 29.8%) | p-Value |
|---|---|---|---|
| Age > 65 years | 74/146 (50.7%) | 39/62 (62.9%) | 0.128 (1) |
| Gender | F: 55 vs. M: 91 | F: 17 vs. M: 45 | 0.202 (1) |
| EAT | 105/146 (71.9%) | 35/62 (56.5%) | 0.036 (1) |
| TAT | 41/146 (28.1%) | 27/62 (43.5%) | |
| Paravertebral psoas abscesses | 92/146 (63.0%) | 36/62 (58.1%) | 0.535 (1) |
| Pleural abscesses | 28/146 (19.2%) | 14/62 (22.6%) | 0.576 (1) |
| CS | 43/146 (29.5%) | 18/62 (29.0%) | 1.000 (1) |
| TS | 58/146 (39.7%) | 24/62 (38.7%) | 1.000 (1) |
| LS | 101/146 (69.2%) | 36/62 (58.1%) | 0.150 (1) |
| More than one part of spine | 43/146 (29.5%) | 14/62 (22.6%) | 0.396 (1) |
| MSSA (n = 187) | 82/135 (60.7%) | 18/52 (34.6%) | 0.002 (1) |
| SE (n = 187) | 19/135 (14.1%) | 12/52 (23.1%) | 0.187 (1) |
| Enterobacterales (n = 187) | 12/135 (8.9%) | 8/52 (15.4%) | 0.198 (1) |
| CoNS (n = 187) | 12/135 (8.9%) | 8/52 (15.4%) | 0.198 (1) |
| Primary infectious sources (n = 145) | -- | -- | 0.143 (2) |
| Time to surgery | 2 [1–4] d * | 4 [1–13] d * | <0.001 (2) |
| Time to pathogen detection | 4 [3–7] d * | 5 [3–10] d * | 0.198 (2) |
| Incidental dural tears | 16/146 (11.0%) | 10/62 (16.1%) | 0.360 (1) |
| Intraoperative antibiotic Irrigation | 129/146 (88.4%) | 44/62 (71.0%) | 0.004 (1) |
| Only abscess evacuation | 82/146 (56.2%) | 11/62 (17.7%) | <0.001 (1) |
| One-stage surgery | 32/146 (21.9%) | 46/62 (74.2%) | <0.001 (1) |
| Two-stage surgery | 32/146 (21.9%) | 5/62 (8.1%) | 0.017 (1) |
| Risk Factors | ESID (n = 146, 70.2%) | NON-ESID (n = 62, 29.8%) | p-Value |
|---|---|---|---|
| Immunosuppression | 22/146 (15.1%) | 13/62 (21.0%) | 0.315 (1) |
| Diabetes mellitus | 52/146 (36.6%) | 25/62 (40.3%) | 0.534 (1) |
| Obesity (BMI > 30 kg/m2) | 48/146 (32.9%) | 18/62 (29.0%) | 0.628 (1) |
| Malignancy | 25/146 (17.1%) | 13/62 (21.0%) | 0.558 (1) |
| Hepatic cirrhosis | 32/146 (21.9%) | 13/62 (21.0%) | 1.000 (1) |
| Dialysis | 5/146 (3.4%) | 3/62 (4.8%) | 0.698 (1) |
| Stent or vascular prosthesis | 13/146 (8.9%) | 4/62 (6.5%) | 0.783 (1) |
| Artificial heart valve replacement | 5/146 (3.4%) | 7/62 (11.3%) | 0.045 (1) |
| Osteoporosis (n = 189) | 51/129 (39.5%) | 31/60 (51.7%) | 0.156 (1) |
| RA or increased RF (n = 91) | 29/67 (43.3%) | 8/24 (33.3%) | 0.472 (1) |
| Gout or increased uric acid (n = 92) | 28/63 (44.4%) | 17/29 (58.6%) | 0.263 (1) |
| Chronic venous insufficiency | 5/146 (3.4%) | 2/62 (3.2%) | 1.000 (1) |
| Peripheral artery disease | 7/146 (4.8%) | 6/62 (9.7%) | 0.214 (1) |
| Atrial fibrillation | 31/146 (21.2%) | 20/62 (32.3%) | 0.113 (1) |
| Variable | ESID (n = 146, 70.2%) | NON-ESID (n = 62, 29.8%) | p-Value |
|---|---|---|---|
| Sepsis | 69/146 (47.3%) | 37/62 (59.7%) | 0.129 (1) |
| Septic embolism (n = 165) | 34/108 (31.5%) | 22/57 (38.6%) | 0.390 (1) |
| Meningism (n = 202) | 22/141 (15.6%) | 15/61 (24.6%) | 0.165 (1) |
| Endocarditis with vegetation (n = 177) | 17/121 (14.0%) | 7/56 (12.5%) | 1.000 (1) |
| SSI | 29/146 (19.9%) | 4/62 (6.5%) | 0.021 (1) |
| Reoperation due SSI | 24/146 (16.4%) | 3/62 (4.8%) | 0.024 (1) |
| Reoperation (empyema or instability) | 41/146 (28.1%) | 12/62 (19.4%) | 0.225 (1) |
| Relapse rate (n = 138) | 25/98 (25.5%) | 6/40 (15.0%) | 0.261 (1) |
| Mortality | 6/146 (4.1%) | 6/62 (9.7%) | 0.189 (1) |
| Hospital stay | 31 [22–48] d * | 35 [24–49] d * | 0.512 (2) |
| ICU stay | 1 [0–8] d * | 2 [0–13] d * | 0.423 (2) |
| Intravenous antibiotic duration | 4 [3–6] w * | 4 [3–6] w * | 0.426 (2) |
| Total antibiotic duration | 8 [6–12] w * | 10 [6–12] w * | 0.301 (2) |
| Baseline Factors | SD (n = 142, 68.3%) | ||
|---|---|---|---|
| ESID (n = 87, 61.3%) | NON-ESID (n = 55, 38.7%) | p-Value | |
| Age > 65 years | 53/87 (60.9%) | 35/55 (63.6%) | 0.859 (1) |
| Gender | F: 29 vs. M: 58 | F: 12 vs. M: 43 | 0.184 (1) |
| EAT | 58/87 (66.7%) | 31/55 (56.4%) | 0.285 (1) |
| TAT | 29/87 (33.3%) | 24/55 (43.6%) | |
| Paravertebral psoas abscesses | 62/87 (71.3%) | 33/55 (60.0%) | 0.201 (1) |
| Pleural abscesses | 20/87 (23.0%) | 13/55 (23.6%) | 1.000 (1) |
| CS | 24/87 (27.6%) | 15/55 (27.3%) | 1.000 (1) |
| TS | 30/87 (34.5%) | 19/55 (34.5%) | 1.000 (1) |
| LS | 62/87 (71.3%) | 34/55 (61.8%) | 0.272 (1) |
| More than one part of spine | 25/87 (28.7%) | 11/55 (20.0%) | 0.322 (1) |
| MSSA (n= 187) | 44/80 (55.0%) | 13/45 (28.9%) | 0.005 (1) |
| SE (n = 187) | 14/80 (17.5%) | 12/45 (26.7%) | 0.255 (1) |
| Enterobacterales (n= 187) | 8/80 (10.0%) | 8/45 (17.8%) | 0.267 (1) |
| CoNS (n = 187) | 8/80 (10.0%) | 7/45 (15.6%) | 0.397 (1) |
| Primary infectious sources (n = 145) | -- | -- | 0.676 (2) |
| Time to surgery | 2 [1–6] d * | 5 [2–14] d * | 0.004 (2) |
| Time to pathogen detection | 5 [3–8] d * | 6 [3–11] d * | 0.470 (2) |
| Incidental dural tears | 11/87 (12.6%) | 8/55 (14.5%) | 0.803 (1) |
| Intraoperative antibiotic Irrigation | 80/87 (92.0%) | 40/55 (72.7%) | 0.004 (1) |
| Only abscess evacuation | 25/87 (28.7%) | 5/55 (9.1%) | 0.006 (1) |
| One-stage surgery | 30/87 (34.5%) | 45/55 (81.8%) | <0.001 (1) |
| Two-stage surgery | 32/87 (36.8%) | 5/55 (9.1%) | <0.001 (1) |
| Risk Factors | SD (n = 142, 68.3%) | ||
|---|---|---|---|
| ESID (n = 87, 61.3%) | NON-ESID (n = 55, 38.7%) | p-Value | |
| Immunosuppression | 16/87 (18.4%) | 12/55 (21.8%) | 0.668 (1) |
| Diabetes Mellitus | 35/87 (40.2%) | 24/55 (43.6%) | 0.729 (1) |
| Obesity (BMI > 30 kg/m2) | 23/87 (26.4%) | 14/55 (25.5%) | 1.000 (1) |
| Malignancy | 14/87 (16.1%) | 12/55 (21.8%) | 0.505 (1) |
| Hepatic cirrhosis | 25/87 (28.7%) | 13/55 (23.6%) | 0.563 (1) |
| Dialysis | 4/87 (4.6%) | 3/55 (5.5%) | 1.000 (1) |
| Stent or vascular prosthesis | 11/87 (12.6%) | 4/55 (7.3%) | 0.406 (1) |
| Artificial heart valve replacement | 3/87 (3.4%) | 7/55 (12.7%) | 0.046 (1) |
| Osteoporosis (n = 189) | 33/76 (43.4%) | 30/55 (54.5%) | 0.221 (1) |
| RA or increased RF (n = 91) | 20/44 (45.5%) | 8/22 (36.4%) | 0.600 (1) |
| Gout or increased uric acid (n = 92) | 19/42 (45.2%) | 17/29 (58.6%) | 0.337 (1) |
| Chronic venous insufficiency | 1/87 (1.1%) | 2/55 (3.6%) | 0.560 (1) |
| Peripheral artery disease | 5/87 (5.7%) | 6/55 (10.9%) | 0.337 (1) |
| Atrial fibrillation | 23/87 (26.4%) | 20/55 (36.4%) | 0.261 (1) |
| Variable | SD (n = 142, 68.3%) | ||
|---|---|---|---|
| ESID (n = 87, 61.3%) | NON-ESID (n = 55, 38.7%) | p-Value | |
| Sepsis | 59/87 (67.8%) | 35/55 (37.2%) | 0.716 (1) |
| Septic embolism (n = 165) | 31/67 (46.3%) | 21/50 (42.0%) | 0.709 (1) |
| Meningism (n = 202) | 12/83 (14.5%) | 13/54 (24.1%) | 0.178 (1) |
| Endocarditis with vegetation (n = 177) | 16/75 (21.3%) | 7/50 (14.0%) | 0.352 (1) |
| SSI | 22/87 (25.3%) | 3/55 (5.5%) | 0.003 (1) |
| Reoperation due SSI | 20/87 (23.0%) | 2/55 (3.6%) | 0.002 (1) |
| Reoperation (empyema or instability) | 37/87 (42.5%) | 12/55 (21.8%) | 0.012 (1) |
| Relapse rate (n = 138) | 21/56 (37.5%) | 6/36 (16.7%) | 0.037 (1) |
| Mortality | 5/87 (5.7%) | 6/55 (10.9%) | 0.337 (1) |
| Hospital stay | 40 [31–56] d * | 35 [26–51] d * | 0.139 (2) |
| ICU stay | 3 [0–13] d * | 2 [0–12] d * | 0.893 (2) |
| Intravenous antibiotic duration | 5 [4–6] w * | 4 [3–7] w * | 0.189 (2) |
| Total antibiotic duration | 10 [8–12] w * | 10 [7–12] w * | 0.789 (2) |
| Infection | ESID | NON-ESID | p-Value |
|---|---|---|---|
| Primary spinal infection (n = 208) | 73/146 (50.0%) | 42/62 (67.7%) | 0.022 (1) |
| Spondylodiscitis (n = 142) | 26/87 (29.9%) | 36/55 (65.5%) | <0.001 (1) |
| Variables | Multivariate Logistic Regression | |
|---|---|---|
| OR (95% CI) | p-Value | |
| Males | 0.487 (0.200–1.185) | 0.113 |
| Age > 65 years | 0.629 (0.257–1.542) | 0.311 |
| Methicillin-sensitive Staphylococcus aureus | 0.928 (0.370–2.329) | 0.874 |
| Time to pathogen detection | 0.938 (0.877–1.002) | 0.058 |
| Empirical antibiotic therapy | 1.707 (0.738–3.948) | 0.211 |
| Time to surgery | 0.992 (0.947–1.040) | 0.748 |
| Diabetes mellitus | 0.612 (0.265–1.415) | 0.251 |
| Hepatic cirrhosis | 0.895 (0.312–2.568) | 0.837 |
| Malignancy | 0.539 (0.174–1.676) | 0.286 |
| Paravertebral psoas abscess | 0.468 (0.208–1.053) | 0.067 |
| Pleural abscess | 0.472 (0.174–1.281) | 0.141 |
| Incidental dural tears | 0.382 (0.111–1.315) | 0.127 |
| Epidural suction-irrigation drainage | 0.201 (0.089–0.451) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hijazi, M.M.; Siepmann, T.; El-Battrawy, I.; Schröttner, P.; Podlesek, D.; Engellandt, K.; Schackert, G.; Juratli, T.A.; Eyüpoglu, I.Y.; Filis, A. The Efficacy of Daily Local Antibiotic Lavage via an Epidural Suction–Irrigation Drainage Technique in Spondylodiscitis and Isolated Spinal Epidural Empyema: A 20-Year Experience of a Single Spine Center. J. Clin. Med. 2023, 12, 5078. https://doi.org/10.3390/jcm12155078
Hijazi MM, Siepmann T, El-Battrawy I, Schröttner P, Podlesek D, Engellandt K, Schackert G, Juratli TA, Eyüpoglu IY, Filis A. The Efficacy of Daily Local Antibiotic Lavage via an Epidural Suction–Irrigation Drainage Technique in Spondylodiscitis and Isolated Spinal Epidural Empyema: A 20-Year Experience of a Single Spine Center. Journal of Clinical Medicine. 2023; 12(15):5078. https://doi.org/10.3390/jcm12155078
Chicago/Turabian StyleHijazi, Mido Max, Timo Siepmann, Ibrahim El-Battrawy, Percy Schröttner, Dino Podlesek, Kay Engellandt, Gabriele Schackert, Tareq A. Juratli, Ilker Y. Eyüpoglu, and Andreas Filis. 2023. "The Efficacy of Daily Local Antibiotic Lavage via an Epidural Suction–Irrigation Drainage Technique in Spondylodiscitis and Isolated Spinal Epidural Empyema: A 20-Year Experience of a Single Spine Center" Journal of Clinical Medicine 12, no. 15: 5078. https://doi.org/10.3390/jcm12155078
APA StyleHijazi, M. M., Siepmann, T., El-Battrawy, I., Schröttner, P., Podlesek, D., Engellandt, K., Schackert, G., Juratli, T. A., Eyüpoglu, I. Y., & Filis, A. (2023). The Efficacy of Daily Local Antibiotic Lavage via an Epidural Suction–Irrigation Drainage Technique in Spondylodiscitis and Isolated Spinal Epidural Empyema: A 20-Year Experience of a Single Spine Center. Journal of Clinical Medicine, 12(15), 5078. https://doi.org/10.3390/jcm12155078