
Validation of the German Version of the P4 Suicidality Tool

 , ,
, ,
Abstract
1. Introduction
2. Material and Methods
2.1. Study Design and Setting
2.2. Recruitment and Data Collection
2.3. Study Population
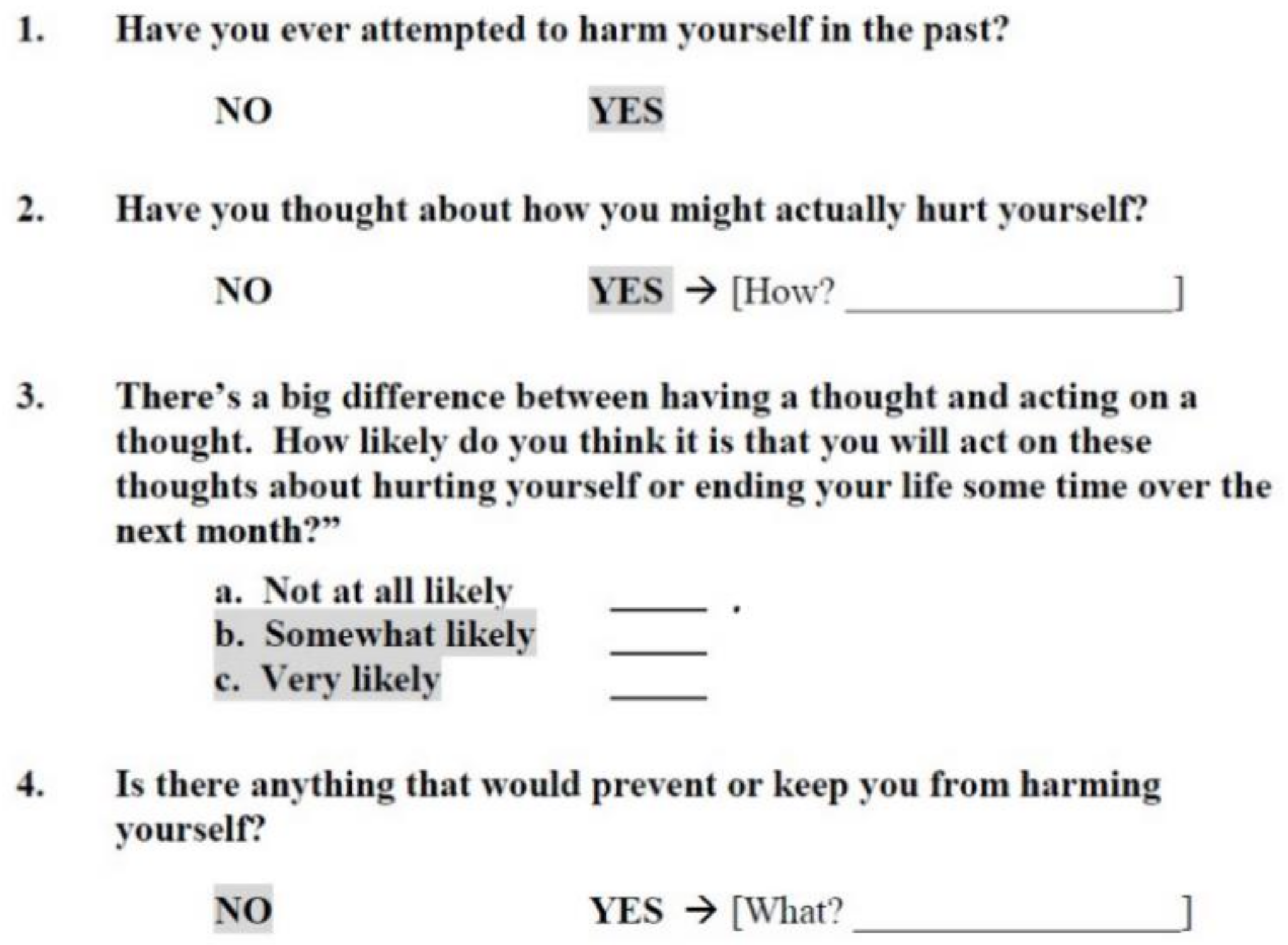
2.4. The P4 Questionnaire
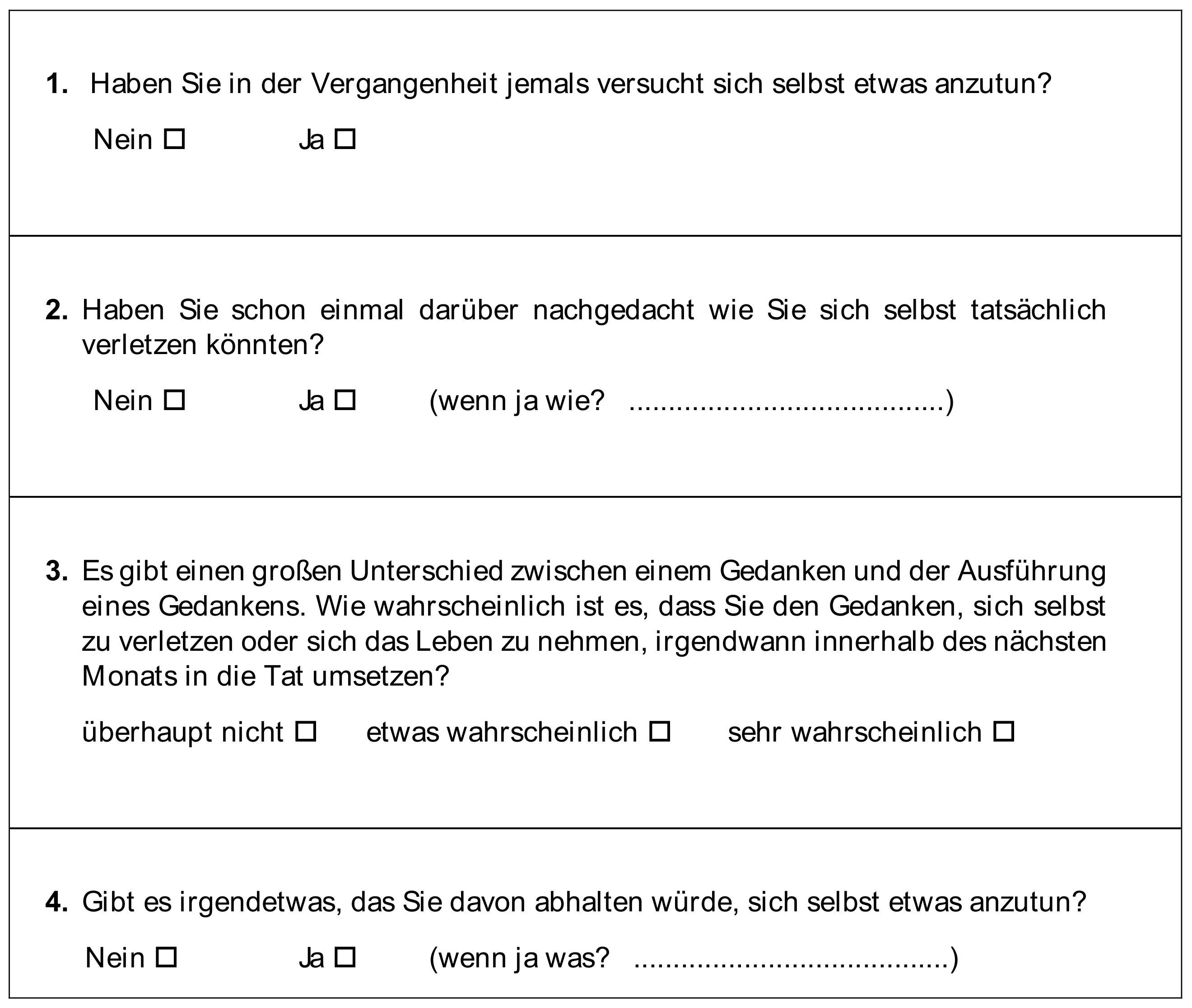
2.5. The German Translation
2.6. Other Instruments
2.7. Data Analysis
3. Results
3.1. P4 Results
3.2. Suicide Plan and Preventive Factors
3.3. Subgroup Analyses
4. Discussion
4.1. Suicidal Risk Stratification
4.2. Strengths, Limitations, and Future Development
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| GP | General practitioner |
| PHQ-9 | Patient Health Questionnaire-9 |
| PMH | Positive mental health-scale |
| SBQ-R | Suicide Behaviors Questionnaire-Revised |
| SI | Suicide ideations |
References
- Harmer, B.; Lee, S.; TvH, D.; Saadabadi, A. Suicidal Ideation. 2020. Available online: https://europepmc.org/article/nbk/nbk565877 (accessed on 1 May 2023).
- Carrasco-Barrios, M.T.; Huertas, P.; Martin, P.; Martin, C.; Castillejos, M.C.; Petkari, E.; Moreno-Kustner, B. Determinants of Suicidality in the European General Population: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public. Health 2020, 17, 4115. [Google Scholar] [CrossRef] [PubMed]
- Klonsky, E.D.; May, A.M.; Saffer, B.Y. Suicide, Suicide Attempts, and Suicidal Ideation. Annu. Rev. Clin. Psychol. 2016, 12, 307–330. [Google Scholar] [CrossRef] [PubMed]
- Hubers, A.A.M.; Moaddine, S.; Peersmann, S.H.M.; Stijnen, T.; van Duijn, E.; van der Mast, R.C.; Dekkers, O.M.; Giltay, E.J. Suicidal ideation and subsequent completed suicide in both psychiatric and non-psychiatric populations: A meta-analysis. Epidemiol. Psychiatr. Sci. 2018, 27, 186–198. [Google Scholar] [CrossRef] [PubMed]
- Jordans, M.; Rathod, S.; Fekadu, A.; Medhin, G.; Kigozi, F.; Kohrt, B.; Luitel, N.; Petersen, I.; Shidhaye, R.; Ssebunnya, J.; et al. Suicidal ideation and behaviour among community and health care seeking populations in five low- and middle-income countries: A cross-sectional study. Epidemiol. Psychiatr. Sci. 2018, 27, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Younes, N.; Melchior, M.; Turbelin, C.; Blanchon, T.; Hanslik, T.; Chee, C.C. Attempted and completed suicide in primary care: Not what we expected? J. Affect. Disord. 2015, 170, 150–154. [Google Scholar] [CrossRef]
- Wiborg, J.F.; Gieseler, D.; Lowe, B. Suicidal ideation in German primary care. Gen. Hosp. Psychiatry 2013, 35, 366–369. [Google Scholar] [CrossRef]
- Dueweke, A.R.; Bridges, A.J. Suicide interventions in primary care: A selective review of the evidence. Fam. Syst. Health 2018, 36, 289–302. [Google Scholar] [CrossRef]
- Gensichen, J.; Lukaschek, K.; Jung-Sievers, C.; Falkai, P.; Schmitt, A.; Henningsen, P.; Dreischulte, T.; Pitschel-Walz, G.; Krcmar, H.; Böhm, M. Predictors and outcomes in primary depression care (POKAL)–a research training group develops an innovative approach to collaborative care. BMC Prim. Care 2022, 23, 1–10. [Google Scholar] [CrossRef]
- Kammer, J.; Rahman, M.; Finnerty, M.; Layman, D.; Vega, K.; Galfalvy, H.; Labouliere, C.; Brown, G.K.; Green, K.; Cummings, A. Most individuals are seen in outpatient medical settings prior to intentional self-harm and suicide attempts treated in a hospital setting. J. Behav. Health Serv. Res. 2021, 48, 306–319. [Google Scholar] [CrossRef]
- Houston, K.; Haw, C.; Townsend, E.; Hawton, K. General practitioner contacts with patients before and after deliberate self harm. Br. J. Gen. Pract. 2003, 53, 365–370. [Google Scholar]
- Hallford, D.; Rusanov, D.; Winestone, B.; Kaplan, R.; Fuller-Tyszkiewicz, M.; Melvin, G. Disclosure of suicidal ideation and behaviours: A systematic review and meta-analysis of prevalence. Clin. Psychol. Rev. 2023, 101, 102272. [Google Scholar] [CrossRef]
- Terrill, D.R.; Rodriguez-Seijas, C.; Zimmerman, M. Assessing Suicidal Ideation Using a Brief Self-Report Measure. Psychiatry Res. 2021, 297, 113737. [Google Scholar] [CrossRef]
- Bundesärztekammer (BÄK) KBK, Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF). Nationale VersorgungsLeitlinie Unipolare Depression—Langfassung, Version 3.0. 2022. Available online: www.leitlinien.de/depression (accessed on 7 November 2022).
- Lukaschek, K.; Frank, M.; Halfter, K.; Schneider, A.; Gensichen, J. Kurze Screener für Suizidalität in der Allgemeinmedizin. MMW Fortschritte Med. 2021, 163, 9–18. [Google Scholar] [CrossRef]
- Thom, R.; Hogan, C.; Hazen, E. Suicide Risk Screening in the Hospital Setting: A Review of Brief Validated Tools. Psychosomatics 2020, 61, 1–7. [Google Scholar] [CrossRef]
- Dixon, M.A.; Hyer, S.M.; Snowden, D.L. Suicide in primary care: How to screen and intervene. Int. J. Psychiatry Med. 2021, 56, 344–353. [Google Scholar] [CrossRef]
- Forkmann, T.T.T.; Glaesmer, H. Diagnostik von Suizidalität; Hogrefe Verlag GmbH & Co.KG: Gottingen, Germany, 2016. [Google Scholar]
- Dube, P.; Kurt, K.; Bair, M.J.; Theobald, D.; Williams, L.S. The p4 screener: Evaluation of a brief measure for assessing potential suicide risk in 2 randomized effectiveness trials of primary care and oncology patients. Prim. Care Companion J. Clin. Psychiatry 2010, 12, 27151. [Google Scholar] [CrossRef]
- Paykel, E.S.; Myers, J.K.; Lindenthal, J.J.; Tanner, J. Suicidal feelings in the general population: A prevalence study. Br. J. Psychiatry 1974, 124, 460–469. [Google Scholar] [CrossRef]
- Metalsky, G.I.; Joiner, T.E. The Hopelessness Depression Symptom Questionnaire. Cogn. Ther. Res. 1997, 21, 359–384. [Google Scholar] [CrossRef]
- Osman, A.; Bagge, C.L.; Gutierrez, P.M.; Konick, L.C.; Kopper, B.A.; Barrios, F.X. The Suicidal Behaviors Questionnaire-Revised (SBQ-R): Validation with clinical and nonclinical samples. Assessment 2001, 8, 443–454. [Google Scholar] [CrossRef]
- Von Glischinski, M.; Teismann, T.; Prinz, S.; Gebauer, J.E.; Hirschfeld, G. Depressive Symptom Inventory Suicidality Subscale: Optimal Cut Points for Clinical and Non-Clinical Samples. Clin. Psychol. Psychother. 2016, 23, 543–549. [Google Scholar] [CrossRef]
- Glaesmer, H.; Kapusta, N.D.; Teismann, T.; Wagner, B.; Hallensleben, N.; Spangenberg, L.; Forkmann, T. Psychometric Properties of the German Version of the Suicide Behaviors Questionnaire Revised (SBQ-R). Psychother. Psychosom. Med. Psychol. 2018, 68, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Teismann, T.; Forkmann, T.; Brailovskaia, J.; Siegmann, P.; Glaesmer, H.; Margraf, J. Positive mental health moderates the association between depression and suicide ideation: A longitudinal study. Int. J. Clin. Health Psychol. 2018, 18, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Brailovskaia, J.; Forkmann, T.; Glaesmer, H.; Paashaus, L.; Rath, D.; Schönfelder, A.; Juckel, G.; Teismann, T. Positive mental health moderates the association between suicide ideation and suicide attempts. J. Affect. Disord. 2019, 245, 246–249. [Google Scholar] [CrossRef] [PubMed]
- Sanftenberg, L.; Dreischulte, T.; Härdtlein, A.; Kosub, H.; Gagyor, I.; Kurotschka, P.K.; Kühlein, T.; Burggraf, L.; Eck, S.; Roos, M. Process evaluation in practice based research networks: A study protocol for a mixed-methods implementation study. BMJ Open 2023, 13, e065947. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B. Validation and utility of a self-report version of PRIME-MD: The PHQ primary care study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA 1999, 282, 1737–1744. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.; Löwe, B. The Patient Health Questionnaire Somatic, Anxiety, and Depressive Symptom Scales: A systematic review. Gen. Hosp. Psychiatry 2010, 32, 345–359. [Google Scholar] [CrossRef]
- Hirschtritt, M.E.; Kroenke, K. Screening for Depression. JAMA 2017, 318, 745–746. [Google Scholar] [CrossRef]
- Lukat, J.; Margraf, J.; Lutz, R.; van der Veld, W.M.; Becker, E.S. Psychometric properties of the Positive Mental Health Scale (PMH-scale). BMC Psychol. 2016, 4, 8. [Google Scholar] [CrossRef]
- Terwee, C.B.; Bot, S.D.; de Boer, M.R.; van der Windt, D.A.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef]
- Bortz, J.; Lienert, G.A. Kurzgefasste Statistik für die Klinische Forschung Leitfaden für die Verteilungsfreie Analyse kleiner Stichproben: Übereinstimmungsmaße für Subjektive Merkmalsbeurteilungen; Springer: Berlin/Heidelberg, Germany, 2008. [Google Scholar]
- Watling, D.; Preece, M.; Hawgood, J.; Bloomfield, S.; Kõlves, K. Developing an Intervention for Suicide Prevention: A Rapid Review of Lived Experience Involvement. Arch. Suicide Res. Off. J. Int. Acad. Suicide Res. 2022, 26, 465–480. [Google Scholar] [CrossRef]
- Schneider, B.; Reif, A.; Wagner, B.; Wolfersdorf, M. Warum brauchen wir Leitlinien für Suizidprävention? Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2022, 65, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Richards, J.E.; Hohl, S.D.; Whiteside, U.; Ludman, E.J.; Grossman, D.C.; Simon, G.E.; Shortreed, S.M.; Lee, A.K.; Parrish, R.; Shea, M. If you listen, I will talk: The experience of being asked about suicidality during routine primary care. J. Gen. Intern. Med. 2019, 34, 2075–2082. [Google Scholar] [CrossRef]
- Christensen-LeCloux, M.; Weimer, M.; Bjorkgren, K.; Booker, W.; Campo, J.V. Universal suicide risk screening: Views of rural adults on acceptability and implementation in primary care. Gen. Hosp. Psychiatry 2021, 71, 102–107. [Google Scholar] [CrossRef]
- Woodford, R.; Spittal, M.J.; Milner, A.; McGill, K.; Kapur, N.; Pirkis, J.; Mitchell, A.; Carter, G. Accuracy of clinician predictions of future self-harm: A systematic review and meta-analysis of predictive studies. Suicide Life Threat. Behav. 2019, 49, 23–40. [Google Scholar] [CrossRef]
- Large, M.M. The role of prediction in suicide prevention. Dialogues Clin. Neurosci. 2018, 20, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Haas, C.; Sterner, P.; Brand, C.; Younesi, P.; Gensichen, J.; Lukaschek, K.; for the POKAL Group. Development of a brief suicide prevention questionnaire for primary care, including pa-tients’ and general practitioners’ perspectives—Concept for a validation study. Suizidprophylaxe 2023, 193, 56–62. [Google Scholar]



{kind=link}
{kind=link}
| Total (n = 222) * | Women (n = 138) | Men (n = 84) | ||||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |
| Age (n = 220) | 47.61 | 15.1 | 47.88 | 15.70 | 47.17 | 14.15 |
| % | N | % | N | % | N | |
| Setting | ||||||
| Primary care | 46.7 | 104 | 48.6 | 67 | 42.9 | 36 |
| Specialized care | 53.4 | 119 | 51.5 | 71 | 57.1 | 48 |
| Main diagnosis | ||||||
| F3 | 46.9 | 104 | 47.1 | 65 | 46.4 | 39 |
| F4 | 7.2 | 16 | 6.5 | 9 | 8.3 | 7 |
| Both F3 and F4 | 27.0 | 60 | 28.3 | 39 | 25.0 | 21 |
| No F diagnosis | 15.8 | 35 | 14.5 | 20 | 17.9 | 15 |
| Other F diagnosis | 3.2 | 7 | 3.6 | 5 | 2.4 | 2 |
| Marital status | ||||||
| Married/relationship | 40.5 | 90 | 38.4 | 53 | 44.1 | 37 |
| Separated/divorced/widowed | 21.6 | 48 | 27.5 | 38 | 11.8 | 10 |
| Single | 37.8 | 84 | 34.1 | 47 | 44.1 | 37 |
| Parenthood | ||||||
| Yes | 53.2 | 118 | 57.2 | 79 | 46.4 | 39 |
| No | 46.9 | 104 | 42.8 | 59 | 53.6 | 45 |
| Total (n = 223) | Women (n = 139) | Men (n = 84) | ||||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |
| Scale scores (range) | ||||||
| PHQ-9 depression (0–27) | 15.00 | 4.36 | 15.10 | 4.45 | 14.90 | 4.21 |
| SBQ-R (3–18) | 7.38 | 4.16 | 7.36 | 4.13 | 7.37 | 4.23 |
| PMH (0–27) | 8.18 | 7.00 | 8.26 | 7.23 | 8.06 | 6.68 |
| Total (n = 223) * | Women (n = 139) | Men (n = 84) | Intercorrelations (Convergent Validity) * | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No Risk | Risk | No Risk | Risk | No Risk | Risk | SBQ-R_1 (Lifetime SI/Attempts) | SBQ-R_2 (12 Month SI) | SBQ-R_3 (Threatened Suicide) | SBQ-R_4 (Suicide Likelihood) | SBQ-R _sum | PMH _sum | PHQ9 _sum | PHQ9_09 | |
| P4_1 (past attempt) | 159 (71.3%) | 64 (28.7%) | 95 (68.8%) | 43 (31.2%) | 64 (78.2%) | 20 (23.8%) | 0.696 | 0.292 | 0.282 | 0.267 | 0.465 | 0.016 | 0.118 | 0.238 |
| P4_2 (suicide plan) | 84 (37.7%) | 139 (62.3%) | 46 (33.3%) | 92 (66.7%) | 38 (45.2%) | 46 (54.8%) | 0.588 | 0.556 | 0.510 | 0.205 | 0.580 | −0.015 | 0.130 | 0.220 |
| P4_3 (suicide likelihood) | 200 (89.7%) | 23 (10.3%) | 123 (89.1%) | 15 (10.9%) | 76 (90.5%) | 8 (9.5%) | 0.178 | 0.248 | 0.193 | 0.355 | 0.329 | −0.108 | 0.240 | 0.364 |
| P4_4 (preventive factors) | 202 (90.6%) | 21 (9.4%) | 127 (92.0%) | 11 (8.0%) | 74 (88.1%) | 10 (11.9%) | 0.024 | 0.047 | 0.043 | 0.051 | 0.550 | 0.191 | 0.053 | 0.121 |
| P4_risk | minimal: 68 (30.5%) | lower: 120 (53.8%) higher: 35 (15.7%) | minimal: 36 (26.1%) | lower: 81 (58.7%) higher: 21 (15.2%) | minimal: 32 (38.1%) | lower: 38 (45.2%) higher: 14 (16.7%) | 0.683 | 0.512 | 0.464 | 0.365 | 0.634 | −0.095 | 0.219 | 0.383 |
| Suicide Plan | N | % |
|---|---|---|
| Medication overdose | 47 | 28.8 |
| Intentional vehicular accident | 29 | 17.8 |
| Cutting oneself | 29 | 17.8 |
| Others | 21 | 12.9 |
| Falls | 14 | 8.6 |
| No answer | 12 | 7.4 |
| Hanging | 9 | 5.5 |
| Using a gun | 2 | 1.2 |
| Total | 163 | 100 |
| Preventive Factors | N | % |
| Family | 147 | 67.4 |
| Future hope | 33 | 15.1 |
| Faith | 12 | 5.5 |
| Fear of failing | 8 | 3.7 |
| Others | 18 | 8.3 |
| Total | 218 | 100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schluessel, S.; Halfter, K.; Haas, C.; Kroenke, K.; Lukaschek, K.; Gensichen, J., on behalf of the POKAL-Group. Validation of the German Version of the P4 Suicidality Tool. J. Clin. Med. 2023, 12, 5047. https://doi.org/10.3390/jcm12155047
Schluessel S, Halfter K, Haas C, Kroenke K, Lukaschek K, Gensichen J on behalf of the POKAL-Group. Validation of the German Version of the P4 Suicidality Tool. Journal of Clinical Medicine. 2023; 12(15):5047. https://doi.org/10.3390/jcm12155047
Chicago/Turabian StyleSchluessel, Sabine, Kathrin Halfter, Carolin Haas, Kurt Kroenke, Karoline Lukaschek, and Jochen Gensichen on behalf of the POKAL-Group. 2023. "Validation of the German Version of the P4 Suicidality Tool" Journal of Clinical Medicine 12, no. 15: 5047. https://doi.org/10.3390/jcm12155047
APA StyleSchluessel, S., Halfter, K., Haas, C., Kroenke, K., Lukaschek, K., & Gensichen, J., on behalf of the POKAL-Group. (2023). Validation of the German Version of the P4 Suicidality Tool. Journal of Clinical Medicine, 12(15), 5047. https://doi.org/10.3390/jcm12155047