
Echocardiographic Parameters for Risk Prediction in Borderline Right Ventricle: Review with Special Emphasis on Pulmonary Atresia with Intact Ventricular Septum and Critical Pulmonary Stenosis


 , ,
, ,  ,
,  ,
, 
Abstract
1. Background
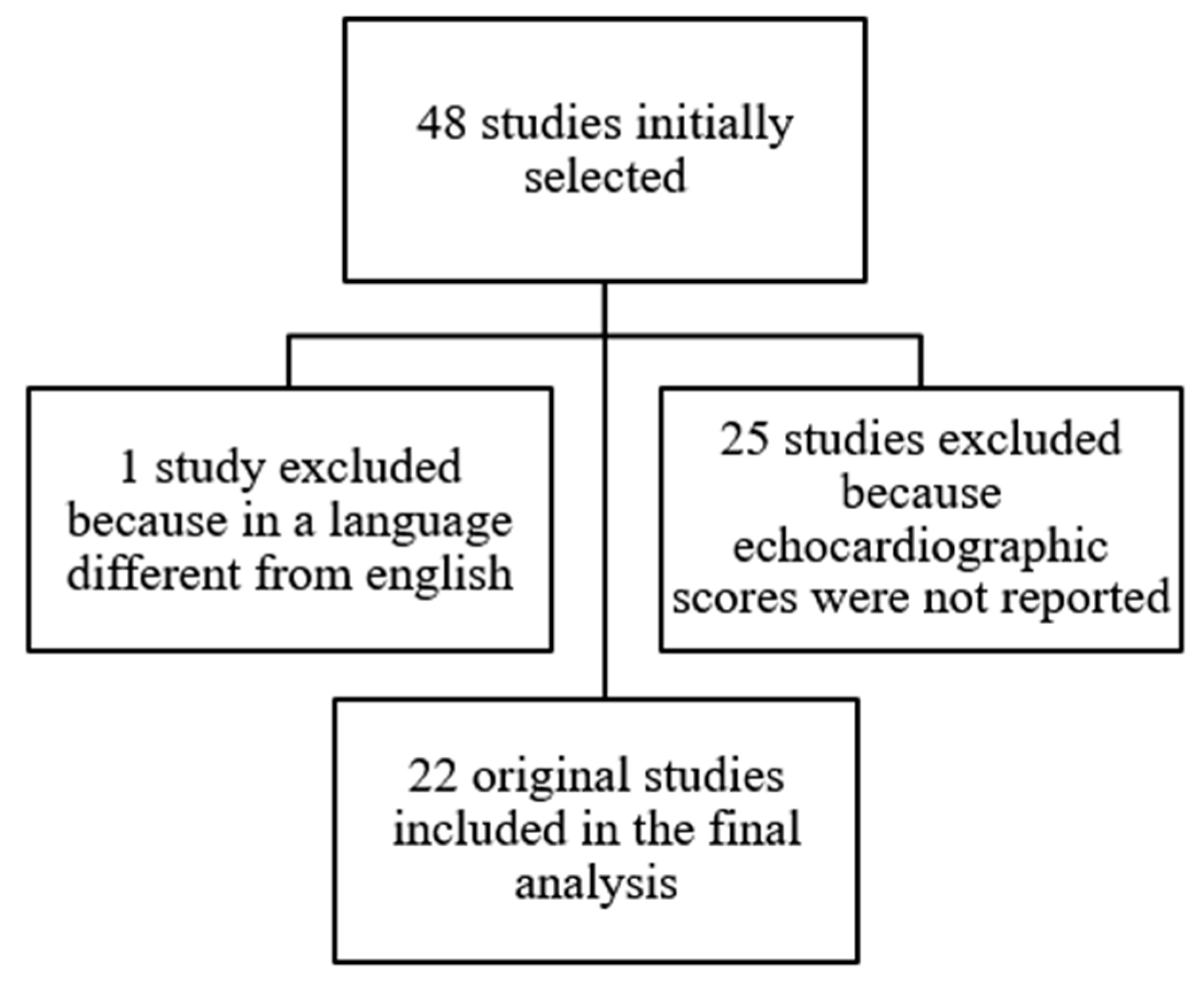
2. Methods
3. Results
3.1. Pulmonary Atresia with Intact Ventricular Septum and Critical Pulmonary Stenosis
3.1.1. General Methodological Limitations
3.1.2. Echocardiographic Parameters Evaluated
The Tricuspid Valve
- Tricuspid valve Z-score
- TV/MV annular ratio
- Tricuspid regurgitation
Right Ventricle Size
- RV diameters
- Right ventricle end-diastolic (RVED) area
- Composite scores and other indices
4. Severe Ebstein’s Anomaly
5. Unbalanced AVSD
6. Discussion
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maskatia, S.A.; Petit, C.J.; Travers, C.D.; Goldberg, D.J.; Rogers, L.S.; Glatz, A.C.; Qureshi, A.M.; Goldstein, B.H.; Ao, J.; Sachdeva, R. Echocardiographic parameters associated with biventricular circulation and right ventricular growth following right ventricular decompression in patients with pulmonary atresia and intact ventricular septum: Results from a multicenter study. Congenit. Heart Dis. 2018, 13, 892–902. [Google Scholar] [CrossRef] [PubMed]
- Petit, C.J.; Glatz, A.C.; Qureshi, A.M.; Sachdeva, R.; Maskatia, S.A.; Justino, H.; Goldberg, D.J.; Mozumdar, N.; Whiteside, W.; Rogers, L.S.; et al. Outcomes After Decompression of the Right Ventricle in Infants with Pulmonary Atresia with Intact Ventricular Septum Are Associated with Degree of Tricuspid Regurgitation: Results from the Congenital Catheterization Research Collaborative. Circ. Cardiovasc. Interv. 2017, 10, e004428. [Google Scholar] [CrossRef] [PubMed]
- Giordano, M.; Santoro, G.; Gaio, G.; Bigazzi, M.C.; Esposito, R.; Marzullo, R.; Di Masi, A.; Palladino, M.T.; Russo, M.G. Novel echocardiographic score to predict duct-dependency after percutaneous relief of critical pulmonary valve stenosis/atresia. Echocardiography 2022, 39, 724–731. [Google Scholar] [CrossRef] [PubMed]
- Cho, M.-J.; Ban, K.-H.; Kim, M.-J.; Park, J.-A.; Lee, H.-D. Catheter-based Treatment in Patients with Critical Pulmonary Stenosis or Pulmonary Atresia with Intact Ventricular Septum: A Single Institute Experience with Comparison between Patients with and without Additional Procedure for Pulmonary Flow. Congenit. Heart Dis. 2013, 8, 440–449. [Google Scholar] [CrossRef]
- Chen, R.H.S.; KT Chau, A.; Chow, P.C.; Yung, T.C.; Cheung, Y.F.; Lun, K.S. Achieving biventricular circulation in patients with moderate hypoplastic right ventricle in pulmonary atresia intact ventricular septum after transcatheter pulmonary valve perforation. Congenit. Heart Dis. 2018, 13, 884–891. [Google Scholar] [CrossRef]
- Yucel, I.K.; Bulut, M.O.; Kucuk, M.; Balli, S.; Celebi, A. Intervention in Patients with Critical Pulmonary Stenosis in the Ductal Stenting Era. Pediatr. Cardiol. 2016, 37, 1037–1045. [Google Scholar] [CrossRef]
- Kovalchin, J.P.; Forbes, T.J.; Nihill, M.R.; Geva, T. Echocardiographic Determinants of Clinical Course in Infants with Critical and Severe Pulmonary Valve Stenosis. J. Am. Coll. Cardiol. 1997, 29, 1095–1101. [Google Scholar] [CrossRef]
- Alwi, M.; Kandavello, G.; Choo, K.-K.; Aziz, B.A.; Samion, H.; Latiff, H.A. Risk factors for augmentation of the flow of blood to the lungs in pulmonary atresia with intact ventricular septum after radiofrequency valvotomy. Cardiol. Young 2005, 15, 141–147. [Google Scholar] [CrossRef]
- Drighil, A.; Aljufan, M.; Slimi, A.; Yamani, S.; Mathewson, J.; Alfadly, F. Echocardiographic determinants of successful balloon dilation in pulmonary atresia with intact ventricular septum. Eur. Heart J. Cardiovasc. Imaging 2009, 11, 172–175. [Google Scholar] [CrossRef]
- Schwartz, M.C.; Glatz, A.C.; Dori, Y.; Rome, J.J.; Gillespie, M.J. Outcomes and Predictors of Reintervention in Patients with Pulmonary Atresia and Intact Ventricular Septum Treated with Radiofrequency Perforation and Balloon Pulmonary Valvuloplasty. Pediatr. Cardiol. 2013, 35, 22–29. [Google Scholar] [CrossRef]
- Cleuziou, J.; Schreiber, C.; Eicken, A.; Hörer, J.; Busch, R.; Holper, K.; Lange, R. Predictors for Biventricular Repair in Pulmonary Atresia with Intact Ventricular Septum. Thorac. Cardiovasc. Surg. 2010, 58, 339–344. [Google Scholar] [CrossRef]
- Hanley, F.L.; Sade, R.M.; Blackstone, E.H.; Kirklin, J.W.; Freedom, R.M.; Nanda, N.C. Outcomes in neonatal pulmonary atresia with intact ventricular septum. A multiinstitutional study. J. Thorac. Cardiovasc. Surg. 1993, 105, 406–427. [Google Scholar] [CrossRef] [PubMed]
- Minich, L.; Tani, L.Y.; Ritter, S.; Williams, R.V.; Shaddy, R.E.; Hawkins, J.A. Usefulness of the preoperative tricuspid/mitral valve ratio for predicting outcome in pulmonary atresia with intact ventricular septum. Am. J. Cardiol. 2000, 85, 1325–1328. [Google Scholar] [CrossRef] [PubMed]
- Sainathan, S.; Silva, L.D.F.D.; da Silva, J.P. Ebstein’s anomaly: Contemporary management strategies. J. Thorac. Dis. 2020, 12, 1161–1173. [Google Scholar] [CrossRef] [PubMed]
- Baek, J.S.; Yu, J.J.; Im, Y.M.; Yun, T.J. Outcomes of neonatal Ebstein’s anomaly without right ventricular forward flow. J. Thorac. Cardiovasc. Surg. 2016, 152, 516–521. [Google Scholar] [CrossRef]
- Sano, S.; Fujii, Y.; Kasahara, S.; Kuroko, Y.; Tateishi, A.; Yoshizumi, K.; Arai, S. Repair of Ebstein’s anomaly in neonates and small infants: Impact of right ventricular exclusion and its indications. Eur. J. Cardiothorac. Surg. 2014, 45, 549–555. [Google Scholar] [CrossRef]
- Mizuno, M.; Hoashi, T.; Sakaguchi, H.; Kagisaki, K.; Kitano, M.; Kurosaki, K.; Yoshimatsu, J.; Shiraishi, I.; Ichikawa, H. Application of Cone Reconstruction for Neonatal Ebstein Anomaly or Tricuspid Valve Dysplasia. Ann. Thorac. Surg. 2016, 101, 1811–1817. [Google Scholar] [CrossRef]
- Celermajer, D.S.; Cullen, S.; Sullivan, I.D.; Spiegelhalter, D.J.; Wyse, R.K.; Deanfield, J.E. Outcome in neonates with Ebstein’s anomaly. J. Am. Coll. Cardiol. 1992, 19, 1041–1046. [Google Scholar] [CrossRef]
- Cieplucha, A.; Trojnarska, O.; Bartczak-Rutkowska, A.; Kociemba, A.; Rajewska-Tabor, J.; Kramer, L.; Pyda, M. Severity Scores for Ebstein Anomaly: Credibility and Usefulness of Echocardiographic vs. Magnetic Resonance Assessments of the Celermajer Index. Can. J. Cardiol. 2019, 35, 1834–1841. [Google Scholar] [CrossRef]
- Prota, C.; Di Salvo, G.; Sabatino, J.; Josen, M.; Paredes, J.; Sirico, D.; Pernia, M.U.; Hoschtitzky, A.; Michielon, G.; Citro, R.; et al. Prognostic value of echocardiographic parameters in pediatric patients with Ebstein’s anomaly. Int. J. Cardiol. 2019, 278, 76–83. [Google Scholar] [CrossRef]
- Yu, J.J.; Yun, T.-J.; Won, H.-S.; Im, Y.M.; Lee, B.S.; Kang, S.Y.; Ko, H.K.; Park, C.S.; Park, J.-J.; Gwak, M.; et al. Outcome of Neonates with Ebstein’s Anomaly in the Current Era. Pediatr. Cardiol. 2013, 34, 1590–1596. [Google Scholar] [CrossRef] [PubMed]
- Freud, L.R.; Escobar-Diaz, M.C.; Kalish, B.T.; Komarlu, R.; Puchalski, M.D.; Jaeggi, E.T.; Szwast, A.L.; Freire, G.; Levasseur, S.M.; Kavanaugh-McHugh, A.; et al. Outcomes and Predictors of Perinatal Mortality in Fetuses with Ebstein Anomaly or Tricuspid Valve Dysplasia in the Current Era: A Multicenter Study. Circulation 2015, 132, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Cantinotti, M.; Marchese, P.; Giordano, R.; Franchi, E.; Assanta, N.; Koestenberger, M.; Jani, V.; Duignan, S.; Kutty, S.; McMahon, C.J. Echocardiographic scores for biventricular repair risk prediction of congenital heart disease with borderline left ventricle: A review. Heart Fail. Rev. 2022, 28, 63–76. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.S.; Jacobs, M.L.; Weinberg, P.M.; Rychik, J. Morphometric Analysis of Unbalanced Common Atrioventricular Canal Using Two-Dimensional Echocardiography. J. Am. Coll. Cardiol. 1996, 28, 1017–1023. [Google Scholar] [CrossRef]
- Jegatheeswaran, A.; Pizarro, C.; Caldarone, C.A.; Cohen, M.S.; Baffa, J.M.; Gremmels, D.B.; Mertens, L.; Morell, V.O.; Williams, W.G.; Blackstone, E.H.; et al. Echocardiographic definition and surgical decision-making in unbalanced atrioventricular septal defect: A Congenital Heart Surgeons’ Society multi-institutional study. Circulation 2010, 122, S209–S215. [Google Scholar] [CrossRef]
- Nathan, M.; Liu, H.; Pigula, F.A.; Fynn-Thompson, F.; Emani, S.; Baird, C.A.; Marx, G.; Mayer, J.E.; del Nido, P.J. Biventricular Conversion after Single-Ventricle Palliation in Unbalanced Atrioventricular Canal Defects. Ann. Thorac. Surg. 2013, 95, 2086–2096. [Google Scholar] [CrossRef]
- Cantinotti, M.; Scalese, M.; Giordano, R.; Assanta, N.; Marchese, P.; Franchi, E.; Viacava, C.; Koestenberger, M.; Jani, V.; Kutty, S. A statistical comparison of reproducibility in current pediatric two-dimensional echocardiographic nomograms. Pediatr. Res. 2020, 89, 579–590. [Google Scholar] [CrossRef]
- Daubeney, P.E.F.; Blackstone, E.H.; Weintraub, R.G.; Slavik, Z.; Scanlon, J.; Webber, S.A. Relationship of the dimension of cardiac structures to body size: An echocardiographic study in normal infants and children. Cardiol. Young 1999, 9, 402–410. [Google Scholar] [CrossRef]
- Rowlatt, J.F.; Rimoldi, M.J.A.; Lev, M. The quantitative anatomy of the normal child’s heart. Pediatr. Clin. North Am. 1963, 10, 499–588. [Google Scholar] [CrossRef]
- Snider, A.R.; Serwer, G.A.; Ritter, S.B. Echocardiography in Pediatric Heart Disease; Mosby: St. Louis, MO, USA, 1997; pp. 137–142. [Google Scholar]
- Pettersen, M.D.; Du, W.; Skeens, M.E.; Humes, R.A. Regression Equations for Calculation of Z Scores of Cardiac Structures in a Large Cohort of Healthy Infants, Children, and Adolescents: An Echocardiographic Study. J. Am. Soc. Echocardiogr. 2008, 21, 922–934. [Google Scholar] [CrossRef]
- Lopez, L.; Frommelt, P.C.; Colan, S.D.; Trachtenberg, F.L.; Gongwer, R.; Stylianou, M.; Bhat, A.; Burns, K.M.; Cohen, M.S.; Dragulescu, A.; et al. Pediatric Heart Network Echocardiographic Z Scores: Comparison with Other Published Models. J. Am. Soc. Echocardiogr. 2020, 34, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Lopez, L.; Colan, S.D.; Frommelt, P.C.; Ensing, G.J.; Kendall, K.; Younoszai, A.K.; Lai, W.W.; Geva, T. Recommendations for Quantification Methods during the Performance of a Pediatric Echocardiogram: A Report from the Pediatric Measurements Writing Group of the American Society of Echocardiography Pediatric and Congenital Heart Disease Council. J. Am. Soc. Echocardiogr. 2010, 23, 465–495. [Google Scholar] [CrossRef] [PubMed]
- Cantinotti, M.; Giordano, R.; Koestenberger, M.; Voges, I.; Santoro, G.; Franchi, E.; Assanta, N.; Valverde, I.; Simpson, J.; Kutty, S. Echocardiographic examination of mitral valve abnormalities in the paediatric population: Current practices. Cardiol. Young 2020, 30, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Zoghbi, W.A.; Adams, D.; Bonow, R.O.; Enriquez-Sarano, M.; Foster, E.; Grayburn, P.A.; Hahn, R.T.; Han, Y.; Hung, J.; Lang, R.M.; et al. Recommendations for noninvasive evaluation of native valvular regurgitation: A report from the american society of echocardiography developed in collaboration with the society for cardiovascular magnetic resonance. J. Indian Acad. Echocardiogr. Cardiovasc. Imaging 2020, 4, 58. [Google Scholar] [CrossRef]
- Hirono, K.; Origasa, H.; Tsuboi, K.; Takarada, S.; Oguri, M.; Okabe, M.; Miyao, N.; Nakaoka, H.; Ibuki, K.; Ozawa, S.; et al. Clinical Status and Outcome of Isolated Right Ventricular Hypoplasia: A Systematic Review and Pooled Analysis of Case Reports. Front. Pediatr. 2022, 10, 794053. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Population | End Point | Echo Predictors | |
|---|---|---|---|
| Cho MJ 2013 South Corea [4] | 9 PA IVS, 13 CPS Undergoing PBPV −10 need aPBF Age 4.89 ± 2.47 days Weight 2.98 ± 0.6 kg −10 do not need aPBF Age 10.10 ± 10.63 days Weight 3.3 ± 0.3 kg | Need of PDA stenting or shunt | TV z-score ≤ −0.74 (AUC 0.8; specificity 90%, sensitivity 77.8%, p = 0.0189) TV/MV ≤ 0.9, (AUC 0.939; specificity 90%, sensitivity 88.89%; p < 0.0001) z-score IVSD ≥ 2.37 (AUC 0.804; specificity 75%, sensitivity 85.71%; p = 0.0222) |
| Chen RHS 2018 Hong Kong [5] | 36 PA IVS Undergoing PBPV −26 BVR Age 5 (1–83) days Weight 3.21 ± 0.55 kg −5 no BVR Age 4 (2–51) days Weight 2.8 ± 0.31 | Good BVR outcome | TV/MV > 0.79 AUC 0.858 specificity 100%, sensitivity 70%, PPV 100%, NPV 50%) |
| Yucel IK, 2016 Turkey [6] | 56 CPS Undergoing PBPV Age 7 (2–28) days. Weight 3.1 (1.6–4.5) kg NR 34 do not need aPBF Weight 3.07 ± 0.4 kg NR 21 need aPBF Weight 3.17 ± 0.4 kg | Need of PDA stenting or shunt Need of re-intervention |
TV Z score < −1.93 (AUC = 0.696, specificity 84.4%, sensitivity 63.2%, p = 0.022) PV Z score < −1.69 (AUC = 0.72, specificity 64.7%, sensitivity 74%, p = 0.008) Bipartite RV (odds ratio 9.6). |
| Alwi M 2005 Malaysia [8] | 53 PA IVS Undergoing PBPV −10 need aPBF Age 8 days (3 days–7 months) Weight 3.1 (2.4–6.8) kg −37 do not need aPBF Age 7 days (1 day–8 years) Weight 3.3 (2–18) kg | Need of PDA stenting or shunt | Lower TV z score TV Z-score −1.1 ± 1.47 Need of aPBF TV Z-score −0.58 ± 1.18 No need of aPBF |
| Drighil A, 2009, USA [9] | 26 PA IVS Undergoing PBPV Age 6 (1–49) days −13 successful BVR Age 14.5 ± 9.0 days Weight 3.3 ± 0.6 kg −13 unsuccessful BVR Age 17.6 ± 15.3 days Weight 3.1 ± 0.6 kg | PBPV success |
|
| Schwartz MC, 2006, USA [10] | 23 PA IVS undergoing RFV Age 2 (−16) days Weight 3.1 (2.1–4.1) kg | Need of re-intervention | Lower post-procedural PV PG (p = 0.05) TV z-score < −0.7 (p = 0.08) |
| Cleuziou J, 2010, Germany [11] | 86 PA IVS 55 underwent PVVP (16 plus shunt) 26 underwent shunt. BVR in 56 Age 2.2 ± 4.8 years Shunt palliation in 13 UV in 17 | Predictors of BVR Predictors of mortality | RV decompression ± shunt (p < 0.001), Tripartite RV (p < 0.001) No coronary fistulae (p < 0.001). At univariate analysis TV z score < 5, unipartite RV, coronary fistula, Ebstein’s, RV dependent coronary circulation, connection of the fistula with LCA and RCA |
| Maskatia SA, 2018, USA [1] | 81 PA IVS Undergoing PBPV Age 3 (2–4) days | BVR, RV growth |
Baseline RV area ≥ 0.6 cm2/m2 (Sensitivity 93%, specificity 80%, AUC 0.88, odds ratio 50.4) Follow-up RV area ≥ 0.8 cm2/m2 sensitivity 100% specificity 100%, AUC 0.96, odds ratio 67) More than moderate TR |
| Minich LL,2000, USA [13] |
23 successful surgical BVR ° Age 11–20 days Weight 3.5 ± 0.6 kg 13 unsuccessful BVR Weight 2.9 ± 0.5 kg | BVR |
Greater pre-op weight TV z score > −3, TV/MV > 0.5 |
| Petit CJ, 2017, USA [2] | 99 PA IVS undergoing PBPV Age 3 (2–5) days Weight 3.3 (2.7–3.7) kg | Primary: Reintervention post-RV decompression. Secondary: BVR | Virtual atresia (HR, 0.51; 95% CI, 0.28–091; p = 0.027), Smaller RV length (HR, 0.94; 95% CI, 0.89–0.99; p = 0.027), ≤Mild TR (HR, 3.58; 95% CI, 2.04–6.30; p < 0.001). ≤Mild TR (OR, 18.6; 95% CI, 5.3–5.2; p < 0.001) Lower RV area (OR, 0.81; 95% CI, 0.72–0.91; p < 0.001). |
| Giordano M, 2022, Italy [3] | 55 PA IVS or CPS Age NR Weight 2.9 ± 5 kg 27 need aPBF Weight 3.0 ± 0.4 kg 28 do not need aPBF Weight 2.9 ± 0.6 KG | Need of PDA stenting or shunt | Composite score including TV < 8.8 mm, TV z-score ← 2.12, TV/MV <0.78, PV < 6.7 mm, PV z-score ←1.17, RVED area < 1.35 cm2, RA area > 2.45 cm2, % of PFO right-to-left shunt > 69.5%, moderate/severe TR, RV systolic pressure > 42.5 mmHg, tricuspid E/E′ ratio > 6.6 A score ≥ 4 sensitivity 100% and specificity 86% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cantinotti, M.; McMahon, C.J.; Marchese, P.; Köstenberger, M.; Scalese, M.; Franchi, E.; Santoro, G.; Assanta, N.; Jacquemyn, X.; Kutty, S.; et al. Echocardiographic Parameters for Risk Prediction in Borderline Right Ventricle: Review with Special Emphasis on Pulmonary Atresia with Intact Ventricular Septum and Critical Pulmonary Stenosis. J. Clin. Med. 2023, 12, 4599. https://doi.org/10.3390/jcm12144599
Cantinotti M, McMahon CJ, Marchese P, Köstenberger M, Scalese M, Franchi E, Santoro G, Assanta N, Jacquemyn X, Kutty S, et al. Echocardiographic Parameters for Risk Prediction in Borderline Right Ventricle: Review with Special Emphasis on Pulmonary Atresia with Intact Ventricular Septum and Critical Pulmonary Stenosis. Journal of Clinical Medicine. 2023; 12(14):4599. https://doi.org/10.3390/jcm12144599
Chicago/Turabian StyleCantinotti, Massimiliano, Colin Joseph McMahon, Pietro Marchese, Martin Köstenberger, Marco Scalese, Eliana Franchi, Giuseppe Santoro, Nadia Assanta, Xander Jacquemyn, Shelby Kutty, and et al. 2023. "Echocardiographic Parameters for Risk Prediction in Borderline Right Ventricle: Review with Special Emphasis on Pulmonary Atresia with Intact Ventricular Septum and Critical Pulmonary Stenosis" Journal of Clinical Medicine 12, no. 14: 4599. https://doi.org/10.3390/jcm12144599
APA StyleCantinotti, M., McMahon, C. J., Marchese, P., Köstenberger, M., Scalese, M., Franchi, E., Santoro, G., Assanta, N., Jacquemyn, X., Kutty, S., & Giordano, R. (2023). Echocardiographic Parameters for Risk Prediction in Borderline Right Ventricle: Review with Special Emphasis on Pulmonary Atresia with Intact Ventricular Septum and Critical Pulmonary Stenosis. Journal of Clinical Medicine, 12(14), 4599. https://doi.org/10.3390/jcm12144599