
The Moderating Effects of Physical Activity on the Relationships between Child Maltreatment and Health Outcomes among Korean Adolescents: A Secondary Analysis of the 2020 Korean Children and Youth Rights Survey


Abstract
1. Introduction
2. Materials and Methods
2.1. Data and Participants
2.2. Measures
2.2.1. Predictor: Child Maltreatment
2.2.2. Outcome Variables
2.2.3. Moderator: Physical Activity
2.2.4. Covariates
2.3. Data Analysis
3. Results
3.1. Descriptive Statistics and Correlation Analysis
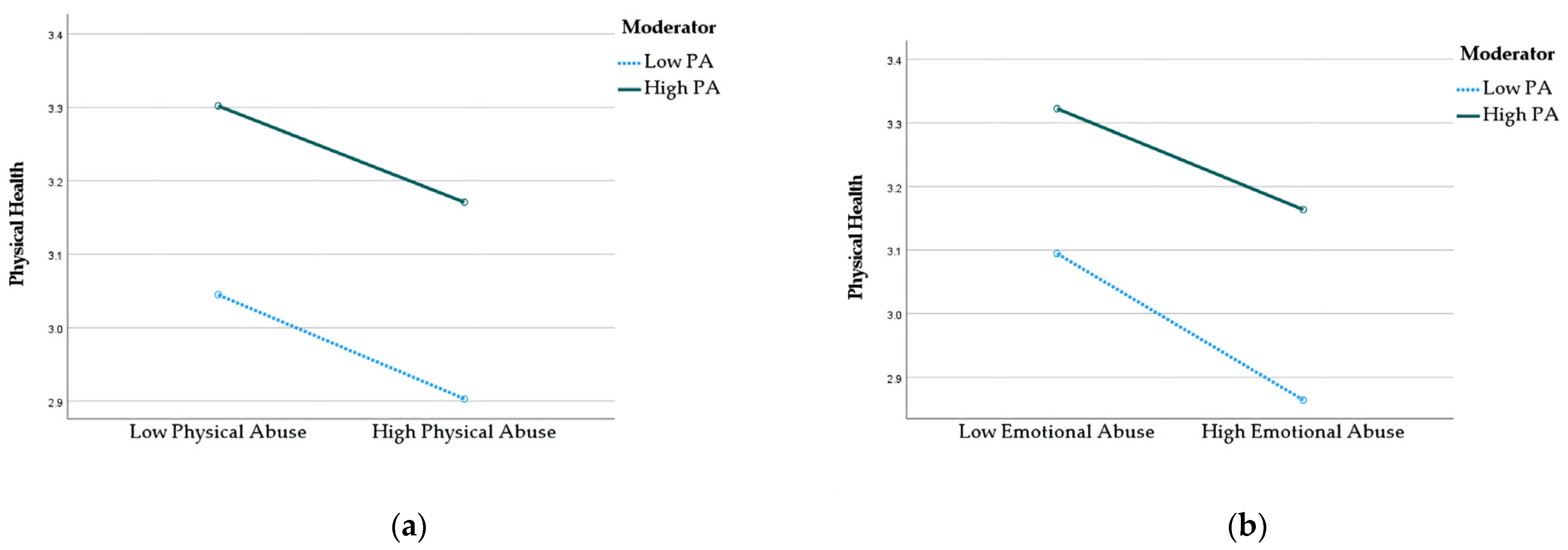
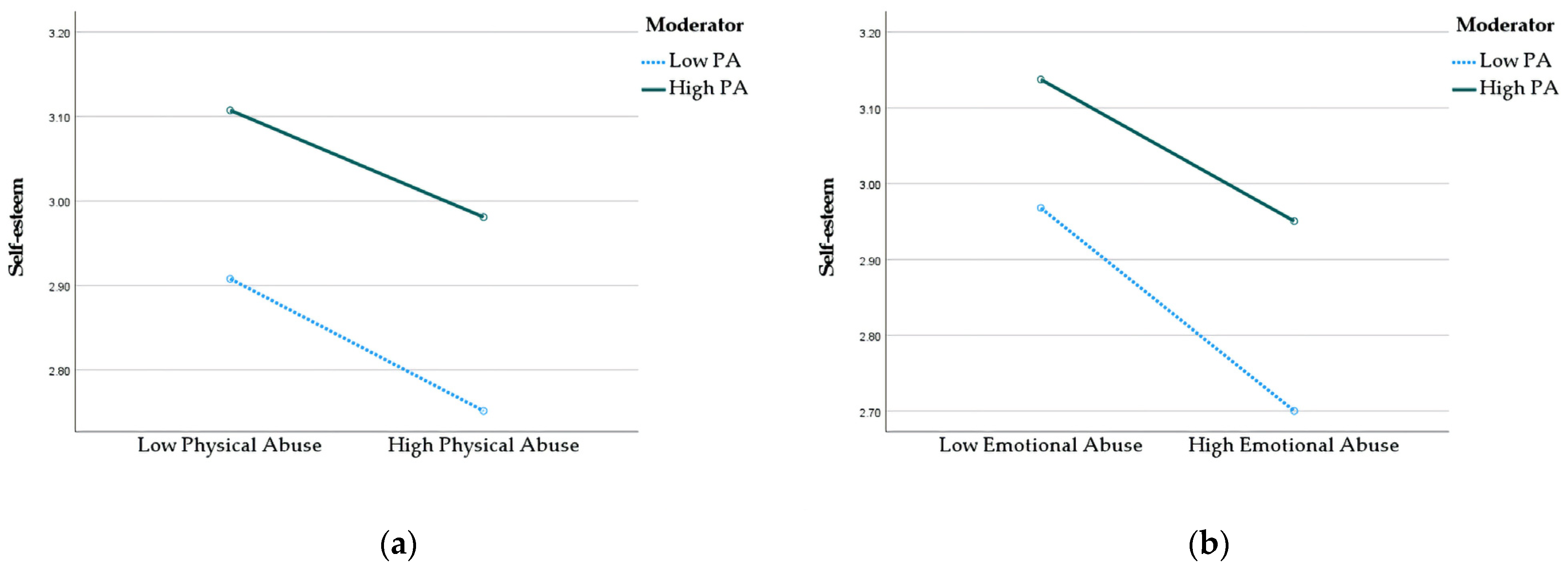
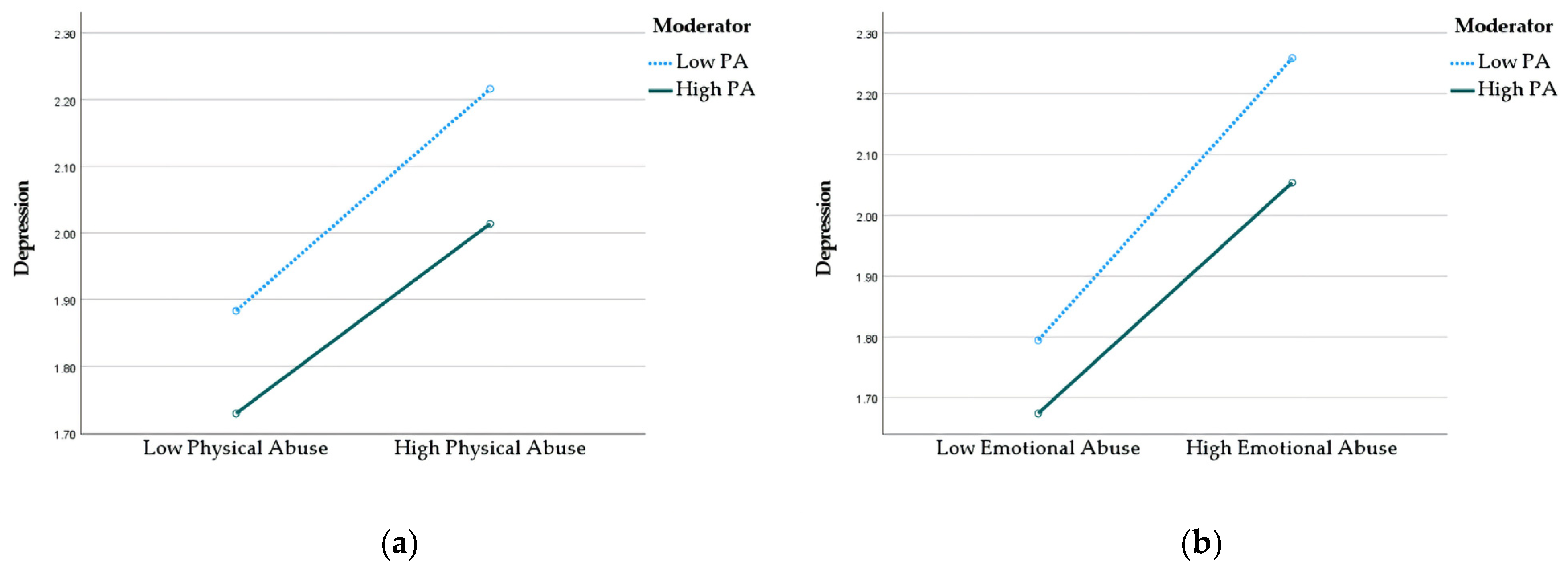
3.2. Moderation Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Centers for Disease Control and Prevention. Preventing Adverse Childhood Experiences: Leveraging the Best Available Evidence; National Center for Injury Prevention and Control, Centers for Disease Control and Prevention: Atlanta, GA, USA, 2019.
- Merrick, M.T.; Ford, D.C.; Ports, K.A.; Guinn, A.S. Prevalence of Adverse Childhood Experiences from the 2011–2014 Behavioral Risk Factor Surveillance System in 23 States. JAMA Pediatr. 2018, 172, 1038–1044. [Google Scholar] [CrossRef]
- Ministry of Health and Welfare. Key Statistics on Child Abuse in 2021; Division of Child Abuse Response: Sejong, Republic of Korea, 2022.
- Monnat, S.M.; Chandler, R.F. Long-Term Physical Health Consequences of Adverse Childhood Experiences. Sociol. Q. 2015, 56, 723–752. [Google Scholar] [CrossRef]
- Johnson, W.F.; Huelsnitz, C.O.; Carlson, E.A.; Roisman, G.I.; Englund, M.M.; Miller, G.E.; Simpson, J.A. Childhood abuse and neglect and physical health at midlife: Prospective, longitudinal evidence. Dev. Psychopathol. 2017, 29, 1935–1946. [Google Scholar] [CrossRef] [PubMed]
- Hughes, K.; Lowey, H.; Quigg, Z.; Bellis, M.A. Relationships between adverse childhood experiences and adult mental well-being: Results from an English national household survey. BMC Public Health 2016, 16, 222. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.W.; Anda, R.F.; Tiemeier, H.; Felitti, V.J.; Edwards, V.J.; Croft, J.B.; Giles, W.H. Adverse Childhood Experiences and the Risk of Premature Mortality. Am. J. Prev. Med. 2009, 37, 389–396. [Google Scholar] [CrossRef]
- Lu, W.; Mueser, K.T.; Rosenberg, S.D.; Jankowski, M.K. Correlates of Adverse Childhood Experiences Among Adults with Severe Mood Disorders. Psychiatr. Serv. 2008, 59, 1018–1026. [Google Scholar] [CrossRef] [PubMed]
- Norman, R.E.; Byambaa, M.; De, R.; Butchart, A.; Scott, J.; Vos, T. The Long-Term Health Consequences of Child Physical Abuse, Emotional Abuse, and Neglect: A Systematic Review and Meta-Analysis. PLoS Med. 2012, 9, e1001349. [Google Scholar] [CrossRef]
- Salinas-Miranda, A.A.; Salemi, J.L.; King, L.M.; Baldwin, J.A.; Berry, E.; Austin, D.A.; Scarborough, K.; Spooner, K.K.; Zoorob, R.J.; Salihu, H.M. Adverse childhood experiences and health-related quality of life in adulthood: Revelations from a community needs assessment. Health Qual. Life Outcomes 2015, 13, 123. [Google Scholar] [CrossRef]
- Corso, P.S.; Edwards, V.J.; Fang, X.; Mercy, J.A. Health-Related Quality of Life Among Adults Who Experienced Maltreatment During Childhood. Am. J. Public Health 2008, 98, 1094–1100. [Google Scholar] [CrossRef]
- Moon, I.; Han, J. Moderating Effects of Physical Activity on the Relationship between Adverse Childhood Experiences and Health-Related Quality of Life. Int. J. Environ. Res. Public Health 2022, 19, 668. [Google Scholar] [CrossRef]
- Sedlak, A.J.; Mettenburg, J.; Basena, M.; Petta, I.; McPherson, K.; Greene, A.; Li, S. Fourth National Incidence Study of Child Abuse and Neglect (NIS-4); US Department of Health and Human Services: Washington, DC, USA, 2010.
- Korean National Youth Policy Institute. A Study on the Implementation of the UN Convention on the Rights of the Child: 2020 Review of Korean Children’s and Youth Rights; National Youth Policy Institute: Sejong, Republic of Korea, 2020. [Google Scholar]
- Font, S.A.; Maguire-Jack, K. Pathways from childhood abuse and other adversities to adult health risks: The role of adult socioeconomic conditions. Child Abus. Negl. 2016, 51, 390–399. [Google Scholar] [CrossRef]
- Ryu, S.; Lee, J.E.; Zeng, N.; Stodden, D.; McDonough, D.J.; Liu, W.; Gao, Z. Bidirectional relationships among children’s perceived competence, motor skill competence, physical activity, and cardiorespiratory fitness across one school year. Biomed. Res. Int. 2021. [Google Scholar] [CrossRef] [PubMed]
- Levine, G.N.; Cohen, B.E.; Commodore-Mensah, Y.; Fleury, J.; Huffman, J.C.; Khalid, U.; Labarthe, D.R.; Lavretsky, H.; Michos, E.D.; Spatz, E.S.; et al. Psychological Health, Well-Being, and the Mind-Heart-Body Connection: A Scientific Statement from the American Heart Association. Circulation 2021, 143, e763–e783. [Google Scholar] [CrossRef] [PubMed]
- Hong, X.; Li, J.; Xu, F.; Tse, L.A.; Liang, Y.; Wang, Z.; Yu, I.T.-S.; Griffiths, S. Physical activity inversely associated with the presence of depression among urban adolescents in regional China. BMC Public Health 2009, 9, 148. [Google Scholar] [CrossRef] [PubMed]
- Long, S.; Rogers, M.L.; Gjelsvik, A. The influence of depression status on weekly exercise in children ages 6 to 17 years. Prev. Med. Rep. 2019, 13, 199–204. [Google Scholar] [CrossRef]
- Shen, L.; Gu, X.; Zhang, T.; Lee, J. Adolescents’ Physical Activity and Depressive Symptoms: A Psychosocial Mechanism. Int. J. Environ. Res. Public Health 2022, 19, 1276. [Google Scholar] [CrossRef] [PubMed]
- Naderi, S.; Naderi, S.; Delavar, A.; Dortaj, F. The effect of physical exercise on anxiety among the victims of child abuse. Sport Sci. Health 2019, 15, 519–525. [Google Scholar] [CrossRef]
- Boisgontier, M.P.; Orsholits, D.; von Arx, M.; Sieber, S.; Miller, M.W.; Courvoisier, D.; Iversen, M.D.; Cullati, S.; Cheval, B. Adverse Childhood Experiences, Depressive Symptoms, Functional Dependence, and Physical Activity: A Moderated Mediation Model. J. Phys. Act. Health 2020, 17, 790–799. [Google Scholar] [CrossRef]
- Easterlin, M.C.; Chung, P.J.; Leng, M.; Dudovitz, R. Association of Team Sports Participation with Long-term Mental Health Outcomes Among Individuals Exposed to Adverse Childhood Experiences. JAMA Pediatr. 2019, 173, 681–688. [Google Scholar] [CrossRef]
- World Health Organization. Global Accelerated Action for the Health of Adolescents (AA-HA!): Guidance to Support Country Implementation; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Beets, M.W.; Pitetti, K.H. Contribution of Physical Education and Sport to Health-Related Fitness in High School Students. J. Sch. Health 2005, 75, 25–30. [Google Scholar] [CrossRef]
- Korean Educational Development Institute. Statistics of Education. Korean Statistical Information Service. Available online: https://kosis.kr/index/index.do (accessed on 31 March 2023).
- Korea Statistics. Dropout Rate. Kindicator. Updated 5 September 2022. Available online: https://www.index.go.kr/unify/idx-info.do?idxCd=5072 (accessed on 31 March 2023).
- Bae, S.M. Long-Term Effect of Adverse Childhood Experiences, School Disengagement, and Reasons for Leaving School on Delinquency in Adolescents Who Dropout. Front. Psychol. 2020, 11, 2096. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, M. The Measurement of Self-Esteem, Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 1965; pp. 16–36. [Google Scholar]
- 2018 Physical Activity Guidelines Advisory Committee. 2018 Physical Activity Guidelines Advisory Committee Scientific Report; U.S. Department of Health and Human Services: Washington, DC, USA, 2018.
- Fasciano, L.C.; Dale, L.P.; Shaikh, S.K.; Hodge, A.L.L.; Gracia, B.; Majdick, J.M.; Holder, A.Y.; Ford, J.D. Relationship of childhood maltreatment, exercise, and emotion regulation to self-esteem, PTSD, and depression symptoms among college students. J. Am. Coll. Health 2021, 69, 653–659. [Google Scholar] [CrossRef]
- Gunnell, K.E.; Flament, M.F.; Buchholz, A.; Henderson, K.A.; Obeid, N.; Schubert, N.; Goldfield, G.S. Examining the bidirectional relationship between physical activity, screen time, and symptoms of anxiety and depression over time during adolescence. Prev. Med. 2016, 88, 147–152. [Google Scholar] [CrossRef]
- Mazereel, V.; Vansteelandt, K.; Menne-Lothmann, C.; Decoster, J.; Derom, C.; Thiery, E.; Rutten, B.P.; Jacobs, N.; van Os, J.; Wichers, M.; et al. The complex and dynamic interplay between self-esteem, belongingness and physical activity in daily life: An experience sampling study in adolescence and young adulthood. Ment. Health Phys. Act. 2021, 21, 100413. [Google Scholar] [CrossRef]
- Afifi, T.O.; Mota, N.P.; Dasiewicz, P.; MacMillan, H.L.; Sareen, J. Physical Punishment and Mental Disorders: Results from a Nationally Representative US Sample. Pediatrics 2012, 130, 184–192. [Google Scholar] [CrossRef]
- Herzog, J.I.; Schmahl, C. Adverse Childhood Experiences and the Consequences on Neurobiological, Psychosocial, and Somatic Conditions Across the Lifespan. Front. Psychiatry 2018, 9, 420. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Physical Activity. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 1 July 2023).
- Tapia-Serrano, M.A.; Sevil-Serrano, J.; Sánchez-Miguel, P.A.; López-Gil, J.F.; Tremblay, M.S.; García-Hermoso, A. Prevalence of meeting 24-Hour Movement Guidelines from pre-school to adolescence: A systematic review and meta-analysis including 387,437 participants and 23 countries. J. Sport Health Sci. 2022, 11, 427–437. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Descriptive | |
|---|---|---|
| Gender | Boy | 1350 (51.7) |
| Girl | 1290 (48.3) | |
| Education level | Grade 7 | 929 (33.1) |
| Grade 8 | 850 (32.2) | |
| Grade 9 | 861 (34.8) | |
| Family structure | Nuclear | 2388 (90.7) |
| Single parent | 191 (6.9) | |
| Grandparent | 23 (0.9) | |
| Other | 38 (1.5) | |
| Economic status | High | 1507 (56.8) |
| Moderate | 963 (36.9) | |
| Low | 170 (6.3) | |
| Academic achievement | High | 839 (31.3) |
| Moderate | 1162 (44.3) | |
| Low | 639 (24.5) | |
| PA | 2.58 ± 1.12 | |
| Physical abuse | 1.33 ± 0.72 | |
| Emotional abuse | 1.65 ± 1.11 | |
| Physical health | 3.15 ± 0.64 | |
| Self-esteem | 2.98 ± 0.70 | |
| Depression | 1.88 ± 0.86 |
| Variables | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| 1. PA | 1 | |||||
| 2. Physical abuse | −0.04 * | 1 | ||||
| 3. Emotional abuse | −0.05 ** | 0.60 ** | 1 | |||
| 4. Physical health | 0.25 ** | −0.08 ** | −0.15 ** | 1 | ||
| 5. Self-esteem | 0.19 ** | −0.10 ** | −0.16 ** | 0.32 ** | 1 | |
| 6. Depression | −0.12 ** | 0.14 ** | 0.24 ** | −0.28 ** | −0.36 ** | 1 |
| B | S.E. | t | p | 95% CI | |
| Constant | 3.64 | 0.09 | 39.50 | <0.01 | 3.46, 3.82 |
| Physical abuse | 0.01 | 0.02 | 0.32 | 0.75 | −0.03, 0.05 |
| PA | 0.14 ** | 0.01 | 12.43 | <0.01 | 0.12, 0.16 |
| Physical abuse × PA | 0.00 | 0.02 | 0.18 | 0.86 | −0.03, 0.03 |
| F = 37.112, R2 = 0.11, adj R2 = 0.00 | |||||
| B | S.E. | t | p | 95% CI | |
| Constant | 3.51 | 0.10 | 36.51 | <0.01 | 3.32, 3.70 |
| Emotional abuse | −0.07 ** | 0.01 | −5.14 | <0.01 | −0.09, 0.04 |
| PA | 0.14 ** | 0.01 | 12.45 | <0.01 | 0.12, 0.16 |
| Emotional abuse × PA | 0.02 * | 0.01 | 2.14 | <0.05 | 0.00, 0.04 |
| F = 37.69, R2 = 0.11, adj R2 > 0.00 | |||||
| B | S.E. | t | p | 95% CI | |
| Constant | 4.10 | 0.10 | 42.03 | <0.01 | 3.91, 4.30 |
| Physical abuse | −0.01 | 0.02 | −0.61 | 0.54 | −0.06, 0.03 |
| PA | 0.09 | 0.01 | 7.71 | <0.01 | 0.07, 0.11 |
| Physical abuse × PA | 0.00 | 0.02 | 0.30 | 0.76 | −0.03, 0.04 |
| F = 58.02, R2 = 0.17, adj R2 = 0.00 | |||||
| B | S.E. | t | p | 95% CI | |
| Constant | 3.99 | 0.10 | 39.09 | <0.01 | 3.79, 4.19 |
| Emotional abuse | −0.08 | 0.01 | −5.64 | <0.01 | −0.11, −0.01 |
| PA | 0.09 | 0.01 | 7.71 | <0.01 | 0.07, 0.11 |
| Emotional abuse × PA | 0.02 | 0.01 | 1.98 | <0.05 | 0.00, 0.04 |
| F = 58.53, R2 = 0.17, adj R2 > 0.00 | |||||
| B | S.E. | t | p | 95% CI | |
| Constant | 0.31 | 0.12 | 2.56 | <0.05 | 0.07, 0.55 |
| Physical abuse | 0.01 | 0.03 | 0.33 | 0.74 | −0.04, 0.06 |
| PA | −0.01 | 0.01 | −0.88 | 0.38 | −0.04, 0.02 |
| Physical abuse × PA | 0.04 | 0.02 | 1.80 | 0.07 | −0.00, 0.08 |
| F = 55.63, R2 = 0.16, adj R2 > 0.00 | |||||
| B | S.E. | t | p | 95% CI | |
| Constant | 0.59 | 0.13 | 4.64 | <0.01 | 0.34, 0.83 |
| Emotional abuse | 0.17 | 0.02 | 9.76 | <0.01 | 0.14, 0.20 |
| PA | −0.01 | 0.01 | −0.96 | 0.34 | −0.04, 0.01 |
| Emotional abuse × PA | −0.00 | 0.01 | −0.27 | 0.79 | −0.03, 0.02 |
| F = 55.21, R2 = 0.16, adj R2 = 0.00 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ryu, S.; Gao, Z. The Moderating Effects of Physical Activity on the Relationships between Child Maltreatment and Health Outcomes among Korean Adolescents: A Secondary Analysis of the 2020 Korean Children and Youth Rights Survey. J. Clin. Med. 2023, 12, 4574. https://doi.org/10.3390/jcm12144574
Ryu S, Gao Z. The Moderating Effects of Physical Activity on the Relationships between Child Maltreatment and Health Outcomes among Korean Adolescents: A Secondary Analysis of the 2020 Korean Children and Youth Rights Survey. Journal of Clinical Medicine. 2023; 12(14):4574. https://doi.org/10.3390/jcm12144574
Chicago/Turabian StyleRyu, Suryeon, and Zan Gao. 2023. "The Moderating Effects of Physical Activity on the Relationships between Child Maltreatment and Health Outcomes among Korean Adolescents: A Secondary Analysis of the 2020 Korean Children and Youth Rights Survey" Journal of Clinical Medicine 12, no. 14: 4574. https://doi.org/10.3390/jcm12144574
APA StyleRyu, S., & Gao, Z. (2023). The Moderating Effects of Physical Activity on the Relationships between Child Maltreatment and Health Outcomes among Korean Adolescents: A Secondary Analysis of the 2020 Korean Children and Youth Rights Survey. Journal of Clinical Medicine, 12(14), 4574. https://doi.org/10.3390/jcm12144574