
Exposures and Suspected Intoxications to Pharmacological and Non-Pharmacological Agents in Children Aged 0–14 Years: Real-World Data from an Italian Reference Poison Control Centre †


 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Toce, M.S.; Burns, M.M. The Poisoned Pediatric Patient. Pediatr. Rev. 2017, 38, 207–220. [Google Scholar] [CrossRef] [PubMed]
- Mintegi, S.; Azkunaga, B.; Prego, J.; Qureshi, N.; Dalziel, S.R.; Arana-Arri, E.; Acedo, Y.; Martinez-Indart, L.; Urkaregi, A.; Salmon, N.; et al. International Epidemiological Differences in Acute Poisonings in Pediatric Emergency Departments. Pediatr. Emerg. Care 2019, 35, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Gummin, D.D.; Mowry, J.B.; Beuhler, M.C.; Spyker, D.A.; Bronstein, A.C.; Rivers, L.J.; Pham, N.P.T.; Weber, J. 2020 Annual Report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 38th Annual Report. Clin. Toxicol. (Phila.) 2021, 59, 1282–1501. [Google Scholar] [CrossRef] [PubMed]
- Berta, G.N.; Di Scipio, F.; Bosetti, F.M.; Mognetti, B.; Romano, F.; Carere, M.E.; Del Giudice, A.C.; Castagno, E.; Bondone, C.; Urbino, A.F. Childhood acute poisoning in the Italian North-West area: A six-year retrospective study. Ital. J. Pediatr. 2020, 46, 83. [Google Scholar] [CrossRef] [PubMed]
- Marano, M.; Rossi, F.; Ravà, L.; Ramla, M.K.; Pisani, M.; Bottari, G.; Genuini, L.; Zampini, G.; Nunziata, J.; Reale, A.; et al. Acute toxic exposures in children: Analysis of a three year registry managed by a Pediatric poison control Center in Italy. Ital. J. Pediatr. 2021, 47, 125. [Google Scholar] [CrossRef] [PubMed]
- Persson, H.E.; Sjöberg, G.K.; Haines, J.A.; Pronczuk de Garbino, J. Poisoning severity score. Grading of acute poisoning. J. Toxicol. Clin. Toxicol. 1998, 36, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Crescioli, G.; Lanzi, C.; Gambassi, F.; Ieri, A.; Ercolini, A.; Borgioli, G.; Bettiol, A.; Vannacci, A.; Mannaioni, G.; Lombardi, N. Exposures and suspected intoxications during SARS-CoV-2 pandemic: Preliminary results from an Italian poison control centre. Intern. Emerg. Med. 2021, 17, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Soave, P.M.; Curatola, A.; Ferretti, S.; Raitano, V.; Conti, G.; Gatto, A.; Chiaretti, A. Acute poisoning in children admitted to pediatric emergency department: A five-years retrospective analysis. Acta Biomed. 2022, 93, 2022004. [Google Scholar] [CrossRef]
- Desai, N.M.; Mistry, R.D.; Brou, L.; Boehnke, M.E.; Lee, J.S.; Wang, G.S. Pediatric Exposures Reported to the Toxicology Investigators Consortium, 2010-2015. Pediatr. Emerg. Care 2021, 37, e1039–e1043. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.-W.; Kernic, M.A.; Mueller, B.A.; Simon, G.E.; Chan, K.C.G.; Stoep, A.V. Association of Parental Mental Illness With Child Injury Occurrence, Hospitalization, and Death During Early Childhood. JAMA Pediatr. 2020, 174, e201749. [Google Scholar] [CrossRef] [PubMed]
- Baker, R.; Kendrick, D.; Tata, L.J.; Orton, E. Association between maternal depression and anxiety episodes and rates of childhood injuries: A cohort study from England. Inj. Prev. 2017, 23, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Orton, E.; Kendrick, D.; West, J.; Tata, L.J. Independent Risk Factors for Injury in Pre-School Children: Three Population-Based Nested Case-Control Studies Using Routine Primary Care Data. PLoS ONE 2012, 7, e35193. [Google Scholar] [CrossRef] [PubMed]
- Crescioli, G.; Lanzi, C.; Mannaioni, G.; Vannacci, A.; Lombardi, N. Adverse drug reactions in SARS-CoV-2 hospitalised patients: A case-series with a focus on drug-drug interactions-reply. Intern. Emerg. Med. 2021, 16, 799–800. [Google Scholar] [CrossRef] [PubMed]
- Missanelli, A.; Lombardi, N.; Bettiol, A.; Lanzi, C.; Rossi, F.; Pacileo, I.; Donvito, L.; Garofalo, V.; Ravaldi, C.; Vannacci, A.; et al. Birth outcomes in women exposed to diagnostic radiology procedures during first trimester of pregnancy: A prospective cohort study. Clin. Toxicol. 2022, 60, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Sartori, S.; Crescioli, G.; Brilli, V.; Traversoni, S.; Lanzi, C.; Vannacci, A.; Mannaioni, G.; Lombardi, N. Phenobarbital use in benzodiazepine and z-drug detoxification: A single-centre 15-year observational retrospective study in clinical practice. Intern. Emerg. Med. 2022, 17, 1631–1640. [Google Scholar] [CrossRef] [PubMed]
- Crescioli, G.; Bonaiuti, R.; Corradetti, R.; Mannaioni, G.; Vannacci, A.; Lombardi, N. Clinical Medicine Pharmacovigilance and Pharmacoepidemiology as a Guarantee of Patient Safety: The Role of the Clinical Pharmacologist. J. Clin. Med. 2022, 11, 3552. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Demographic and Clinical Characteristics | 0–11 Months N = 1220 (%) | 1–5 Years N = 8854 (%) | 6–11 Years N = 1451 (%) | >12 Years N = 471 (%) | p-Value |
|---|---|---|---|---|---|
| Sex | |||||
| Male | 633 (51.89) | 4779 (53.98) | 855 (58.92) | 222 (47.13) | <0.001 |
| Female | 587 (48.11) | 4075 (46.02) | 596 (41.08) | 249 (52.87) | |
| Route of exposure | |||||
| Oral | 1133 (92.87) | 8279 (93.51) | 1263 (87.04) | 408 (86.62) | <0.001 |
| Skin | 15 (1.23) | 220 (2.48) | 64 (4.41) | 24 (5.10) | |
| Ocular | 16 (1.31) | 215 (2.43) | 33 (2.27) | 10 (2.12) | |
| Inhalation | 35 (2.87) | 108 (1.22) | 77 (5.31) | 27 (5.73) | |
| Other route of exposure | 21 (1.72) | 32 (0.36) | 14 (0.96) | 2 (0.42) | |
| Qualification | |||||
| Caregiver | 768 (62.95) | 5050 (57.04) | 745 (51.34) | 140 (29.72) | <0.001 |
| Healthcare professional | 452 (37.05) | 3804 (42.96) | 706 (48.66) | 331 (70.28) | |
| Location of exposure | |||||
| Home | 1189 (97.46) | 8656 (97.76) | 1343 (92.56) | 418 (88.75) | <0.001 |
| Others | 31 (2.54) | 198 (2.24) | 108 (7.44) | 53 (11.25) | |
| Circumstances | |||||
| Involuntary intoxication | 1220 (100) | 8854 (100) | 1445 (99.59) | 362 (76.86) | <0.001 |
| Domestic exposure | 980 | 8333 | 1198 | 287 | |
| Therapeutic error | 231 | 511 | 242 | 74 | |
| Adverse reactions | 9 | 10 | 5 | 1 | |
| Voluntary intoxications | - | - | 6 (0.41) | 109 (23.14) | |
| Suicide attempt | - | - | 6 | 94 | |
| Substance abuse | - | - | - | 15 | |
| Time from exposure | |||||
| Mean ± SD (hours) | 5.75 ± 40.66 | 2.76 ± 17.68 | 5.20 ± 19.58 | 6.13 ± 30.09 | 0.997 |
| <30 min | 621 (50.90) | 4388 (49.56) | 563 (38.80) | 134 (28.45) | <0.001 |
| 30–60 min | 204 (16.72) | 1776 (20.06) | 247 (17.02) | 79 (16.77) | |
| 60 min–24 h | 341 (27.95) | 2447 (17.02) | 555 (38.25) | 232 (49.26) | |
| ≥24 h | 54 (4.43) | 243 (2.74) | 86 (5.93) | 26 (5.52) | |
| Symptoms | |||||
| Absent | 1067 (87.46) | 7494 (84.64) | 1054 (72.64) | 271 (57.54) | <0.001 |
| Gastrointestinal | 77 (6.31) | 755 (8.53) | 190 (13.90) | 78 (16.56) | |
| Neurologic | 35 (2.87) | 140 (1.58) | 72 (4.96) | 70 (14.86) | |
| Cutaneous | 12 (0.98) | 159 (1.80) | 67 (4.62) | 24 (5.10) | |
| Ocular | 6 (0.49) | 174 (1.97) | 23 (1.59) | 9 (1.91) | |
| Respiratory | 10 (0.82) | 92 (1.04) | 31 (2.14) | 13 (2.76) | |
| Cardiac | 4 (0.33) | 13 (0.15) | 9 (0.62) | 5 (1.06) | |
| Other | 9 (0.74) | 27 (0.30) | 5 (0.34) | 1 (0.21) | |
| Toxicologist advices | |||||
| Observation at home | 908 (74.43) | 6165 (69.63) | 967 (66.64) | 188 (39.92) | <0.001 |
| ED visit for outpatients | 89 (7.30) | 795 (8.98) | 118 (8.13) | 55 (11.68) | |
| ED observation for inpatients | 146 (11.97) | 1318 (14.89) | 224 (15.44) | 117 (24.84) | |
| Hospitalisation | 77 (6.31) | 576 (6.51) | 142 (9.79) | 111 (23.57) | |
| Prescribed therapies | |||||
| No | 989 (81.07) | 6433 (72.66) | 997 (68.71) | 219 (46.50) | <0.001 |
| Yes | 231 (18.93) | 2421 (27.34) | 454 (31.29) | 252 (53.50) | |
| Symptomatic therapies | 190 | 1933 | 358 | 170 | |
| Decontamination | 31 | 444 | 69 | 63 | |
| Antidotal therapies | 10 | 44 | 27 | 19 |
| 0–11 Months N = 1220 (%) | 1–5 Years N = 8854 (%) | 6–11 Years N = 1451 (%) | >12 Years N = 471 (%) | |
|---|---|---|---|---|
| Number of toxic agents | ||||
| One | 1211 (99.26) | 8754 (98.87) | 1434 (98.83) | 434 (92.14) |
| More than one | 9 (0.74) | 100 (1.13) | 17 (1.17) | 37 (7.86) |
| Toxic agents | ||||
| Non-pharmacological agents | 854 (70.00) | 6144 (69.39) | 952 (65.61) | 256 (54.35) |
| Cleaners | 160 | 1947 | 171 | 55 |
| Other household products | 126 | 951 | 190 | 41 |
| Toys | 105 | 844 | 145 | 18 |
| Cosmetics | 90 | 817 | 52 | 19 |
| Plant poisons | 164 | 589 | 95 | 14 |
| Pesticides | 120 | 449 | 66 | 8 |
| Foods | 32 | 193 | 85 | 23 |
| Caustics | 12 | 219 | 49 | 16 |
| Animal poisons | 12 | 80 | 59 | 24 |
| Substances of abuse | 16 | 44 | 9 | 28 |
| Carbon monoxide or other gasses | 17 | 33 | 34 | 12 |
| Pharmacological agents § | 366 (30.00) | 2707 (30.57) | 499 (34.39) | 213 (45.22) |
| Analgesics (ATC N02) | 63 | 269 | 43 | 32 |
| Antibacterials for systemic use (ATC J01) | 30 | 182 | 49 | 15 |
| NSAIDs and antirheumatic products (ATC M01) | 8 | 209 | 38 | 22 |
| Psycholeptics (ATC N05) | 11 | 118 | 51 | 63 |
| Thyroid therapy (ATC H03) | 7 | 170 | 16 | 3 |
| Psychoanaleptics (ATC N06) | 9 | 98 | 37 | 24 |
| Drugs for obstructive airway diseases (ATC R03) | 13 | 120 | 17 | 0 |
| Sex hormones and modulators of the genital system (ATC G03) | 0 | 116 | 11 | 1 |
| Antihistamines for systemic use (ATC R06) | 9 | 81 | 19 | 5 |
| Agents acting on the renin–angiotensin system (ATC C09) | 5 | 98 | 6 | 7 |
| Antiepileptics (ATC N03) | 4 | 59 | 29 | 23 |
| Nasal preparations (ATC R01) | 19 | 66 | 9 | 2 |
| Mineral supplements (ATC A12) | 27 | 52 | 9 | 0 |
| Cough and cold preparations (ATC R05) | 4 | 61 | 11 | 4 |
| Beta blocking agents (ATC C07) | 2 | 57 | 5 | 6 |
| Complementary and alternative medicine | 36 (2.95) | 238 (2.68) | 44 (3.03) | 8 (1.69) |
| Dietary supplements | 25 | 144 | 32 | 2 |
| Phytotherapy | 9 | 56 | 7 | 4 |
| Homeopathy | 2 | 38 | 5 | 2 |
| Crude Odds Ratio (95% Confidence Interval) | Adjusted Odds Ratio (95% Confidence Interval) | |
|---|---|---|
| Sex | ||
| Male | 1 | 1 |
| Female | 0.92 (0.86–1.00) | 0.88 (0.81–0.95) |
| Age | ||
| 0–11 months | 1 | 1 |
| 1–5 years | 1.27 (1.11–1.45) | 1.27 (1.10–1.45) |
| 6–11 years | 1.46 (1.23–1.72) | 1.35 (1.14–1.60) |
| >12 years | 4.38 (3.50–5.48) | 2.52 (1.97–3.22) |
| Number of toxic agents | ||
| One | 1 | 1 |
| More than one | 5.53 (3.93–7.78) | 3.79 (2.65–5.42) |
| Circumstances | ||
| Involuntary intoxication | 1 | 1 |
| Voluntary intoxications | 51.31 (20.94–125.74) | 29.18 (11.76–72.38) |
| Toxic agents | ||
| Non-pharmacological agents | 1 | 1 |
| Pharmacological agents | 1.40 (1.29–1.52) | 1.34 (1.23–1.46) |
| Pharmacological and non-pharmacological agents | 9.76 (1.09–87.39) | 2.03 (0.20–20.13) |
| Route of exposure | ||
| Other route of exposure | 1 | 1 |
| Oral | 0.53 (0.33–0.86) | 0.57 (0.35–0.93) |
| Skin | 0.60 (0.35–1.01) | 0.68 (0.40–1.16) |
| Ocular | 0.91 (0.54–1.55) | 1.07 (0.63–1.84) |
| Inhalation | 1.74 (1.02–2.98) | 1.87 (1.09–3.23) |
| Crude Odds Ratio (95% Confidence Interval) | Adjusted Odds Ratio (95% Confidence Interval) | |
|---|---|---|
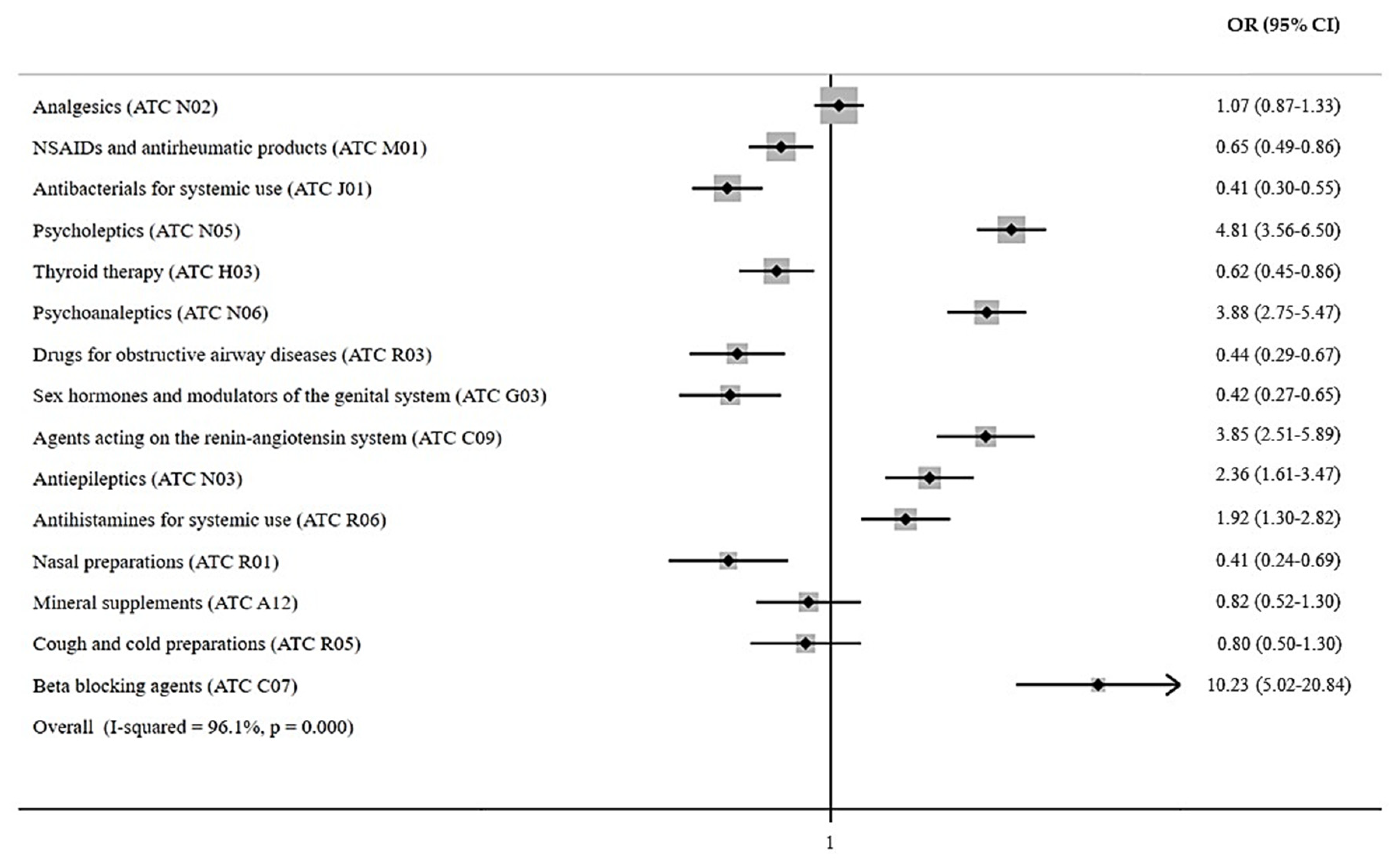
| Analgesics (ATC N02) | 1.07 (0.87–1.33) | 1.05 (0.84–1.30) |
| NSAIDs and antirheumatics (ATC M01) | 0.65 (0.49–0.86) | 0.65 (0.49–0.86) |
| Antibacterials for systemic use (ATC J01) | 0.41 (0.30–0.55) | 0.37 (0.27–0.50) |
| Psycholeptics (ATC N05) | 4.81 (3.56–6.50) | 4.25 (3.13–5.78) |
| Thyroid therapy (ATC H03) | 0.62 (0.45–0.86) | 0.67 (0.48–0.93) |
| Psychoanaleptics (ATC N06) | 3.88 (2.75–5.47) | 3.68 (2.60–5.20) |
| Drugs for obstructive airway diseases (ATC R03) | 0.44 (0.29–0.67) | 0.46 (0.30–0.69) |
| Sex hormones (ATC G03) | 0.42 (0.27–0.65) | 0.45 (0.29–0.71) |
| Agents acting on the renin–angiotensin system (ATC C09) | 3.85 (2.51–5.89) | 4.13 (2.69–6.34) |
| Antiepileptics (ATC N03) | 2.36 (1.61–3.47) | 2.08 (1.40–3.07) |
| Antihistamines for systemic use (ATC R06) | 1.92 (1.30–2.82) | 1.92 (1.30–2.84) |
| Nasal preparations (ATC R01) | 0.41 (0.24–0.69) | 0.42 (0.25–0.71) |
| Mineral supplements (ATC A12) | 0.82 (0.52–1.30) | 0.89 (0.56–1.40) |
| Cough and cold preparations (ATC R05) | 0.80 (0.50–1.30) | 0.80 (0.49–1.29) |
| Beta blocking agents (ATC C07) | 10.23 (5.02–20.84) | 10.99 (5.38–22.44) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brilli, V.; Crescioli, G.; Missanelli, A.; Lanzi, C.; Trombini, M.; Ieri, A.; Gambassi, F.; Vannacci, A.; Mannaioni, G.; Lombardi, N. Exposures and Suspected Intoxications to Pharmacological and Non-Pharmacological Agents in Children Aged 0–14 Years: Real-World Data from an Italian Reference Poison Control Centre. J. Clin. Med. 2023, 12, 352. https://doi.org/10.3390/jcm12010352
Brilli V, Crescioli G, Missanelli A, Lanzi C, Trombini M, Ieri A, Gambassi F, Vannacci A, Mannaioni G, Lombardi N. Exposures and Suspected Intoxications to Pharmacological and Non-Pharmacological Agents in Children Aged 0–14 Years: Real-World Data from an Italian Reference Poison Control Centre. Journal of Clinical Medicine. 2023; 12(1):352. https://doi.org/10.3390/jcm12010352
Chicago/Turabian StyleBrilli, Valentina, Giada Crescioli, Andrea Missanelli, Cecilia Lanzi, Massimo Trombini, Alessandra Ieri, Francesco Gambassi, Alfredo Vannacci, Guido Mannaioni, and Niccolò Lombardi. 2023. "Exposures and Suspected Intoxications to Pharmacological and Non-Pharmacological Agents in Children Aged 0–14 Years: Real-World Data from an Italian Reference Poison Control Centre" Journal of Clinical Medicine 12, no. 1: 352. https://doi.org/10.3390/jcm12010352
APA StyleBrilli, V., Crescioli, G., Missanelli, A., Lanzi, C., Trombini, M., Ieri, A., Gambassi, F., Vannacci, A., Mannaioni, G., & Lombardi, N. (2023). Exposures and Suspected Intoxications to Pharmacological and Non-Pharmacological Agents in Children Aged 0–14 Years: Real-World Data from an Italian Reference Poison Control Centre. Journal of Clinical Medicine, 12(1), 352. https://doi.org/10.3390/jcm12010352