
The Interplay of Perceived Risks and Benefits in Deciding to Become Vaccinated against COVID-19 While Pregnant or Breastfeeding: A Cross-Sectional Study in Italy
 , , ,
, , ,  ,
,  ,
,  , ,
, ,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Statistical Analyses
2.3.1. Descriptive Analysis
2.3.2. Dimensionality Reduction—Factor Analyses
2.3.3. Logistic and Beta Regressions
3. Results
3.1. Demographic
3.2. Logistic Regression Model
3.3. Beta Regression Models
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Luxi, N.; Giovanazzi, A.; Capuano, A.; Crisafulli, S.; Cutroneo, P.M.; Fantini, M.P.; Trifirò, G. COVID-19 vaccination in pregnancy, paediatrics, immunocompromised patients, and persons with history of allergy or prior SARS-CoV-2 infection: Overview of current recommendations and pre-and post-marketing evidence for vaccine efficacy and safety. Drug Saf. 2021, 44, 1247–1269. [Google Scholar] [CrossRef] [PubMed]
- Brewer, N.T.; Chapman, G.B.; Gibbons, F.X.; Gerrard, M.; McCaul, K.D.; Weinstein, N.D. Meta-analysis of the relationship between risk perception and health behavior: The example of vaccination. Health Psychol. 2007, 26, 136. [Google Scholar] [CrossRef] [PubMed]
- Slovic, P.; Finucane, M.L.; Peters, E.; MacGregor, D.G. The affect heuristic. Eur. J. Oper. Res. 2007, 177, 1333–1352. [Google Scholar] [CrossRef]
- Meharry, P.M.; Colson, E.R.; Grizas, A.P.; Stiller, R.; Vázquez, M. Reasons why women accept or reject the trivalent inactivated influenza vaccine (TIV) during pregnancy. Matern. Child Health J. 2013, 17, 156–164. [Google Scholar] [CrossRef]
- Song, Y.; Zhang, T.; Chen, L.; Yi, B.; Hao, X.; Zhou, S.; Greene, C. Increasing seasonal influenza vaccination among high risk groups in China: Do community healthcare workers have a role to play? Vaccine 2017, 35, 4060–4063. [Google Scholar] [CrossRef] [PubMed]
- Yun, X.; Xu, J. Survey of attitude toward immunization of H1N1 influenza A vaccine of pregnant women in Guangzhou. J. Trop. Med. 2010, 10, 1136–1140. [Google Scholar]
- McCarthy, E.A.; Pollock, W.E.; Tapper, L.; Sommerville, M.; McDonald, S. Increasing uptake of influenza vaccine by pregnant women post H1N1 pandemic: A longitudinal study in Melbourne, Australia, 2010 to 2014. BMC Pregnancy Childbirth 2015, 15, 1–7. [Google Scholar] [CrossRef]
- Goldfarb, I.; Panda, B.; Wylie, B.; Riley, L. Uptake of influenza vaccine in pregnant women during the 2009 H1N1 influenza pandemic. Am. J. Obstet. Gynecol. 2011, 204, S112–S115. [Google Scholar] [CrossRef]
- Campbell, H.; Van Hoek, A.J.; Bedford, H.; Craig, L.; Yeowell, A.L.; Green, D.; Amirthalingam, G. Attitudes to immunisation in pregnancy among women in the UK targeted by such programmes. Br. J. Midwifery 2015, 23, 566–573. [Google Scholar] [CrossRef]
- Kilich, E.; Dada, S.; Francis, M.R.; Tazare, J.; Chico, R.M.; Paterson, P.; Larson, H.J. Factors that influence vaccination decision-making among pregnant women: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0234827. [Google Scholar] [CrossRef]
- Bhattacharya, O.; Siddiquea, B.N.; Shetty, A.; Afroz, A.; Billah, B. COVID-19 vaccine hesitancy among pregnant women: A systematic review and meta-analysis. BMJ Open 2022, 12, e061477. [Google Scholar] [CrossRef]
- Bianchi, F.P.; Stefanizzi, P.; Di Gioia, M.C.; Brescia, N.; Lattanzio, S.; Tafuri, S. COVID-19 vaccination hesitancy in pregnant and breastfeeding women and strategies to increase vaccination compliance: A systematic review and meta-analysis. Expert Rev. Vaccines 2022, 21, 1443–1454. [Google Scholar] [CrossRef]
- Januszek, S.M.; Faryniak-Zuzak, A.; Barnaś, E.; Łoziński, T.; Góra, T.; Siwiec, N.; Kluz, T. The approach of pregnant women to vaccination based on a COVID-19 systematic review. Medicina 2021, 57, 977. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Effraimidou, E.; Cassimos, D.C.; Medic, S.; Topalidou, M.; Konstantinidis, T.; Rodolakis, A. Vaccination programs for pregnant women in Europe, 2021. Vaccine 2021, 39, 6137–6143. [Google Scholar] [CrossRef]
- Goncu Ayhan, S.; Oluklu, D.; Atalay, A.; Menekse Beser, D.; Tanacan, A.; Moraloglu Tekin, O.; Sahin, D. COVID-19 vaccine acceptance in pregnant women. Int. J. Gynecol. Obstet. 2021, 154, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Mohan, S.; Reagu, S.; Lindow, S.; Alabdulla, M. COVID-19 vaccine hesitancy in perinatal women: A cross sectional survey. J. Perinat. Med. 2021, 49, 678–685. [Google Scholar] [CrossRef] [PubMed]
- Jayagobi, P.A.; Ong, C.; Thai, Y.K.; Lim, C.C.; Jiun, S.M.; Koon, K.L.; Chien, C.M. Perceptions and acceptance of COVID-19 vaccine among pregnant and lactating women in Singapore: A cross-sectional study. MedRxiv 2021, 2021, 6. [Google Scholar] [CrossRef] [PubMed]
- Ceulemans, M.; Foulon, V.; Panchaud, A.; Winterfeld, U.; Pomar, L.; Lambelet, V.; Nordeng, H. Vaccine willingness and impact of the COVID-19 pandemic on women’s perinatal experiences and practices—A multinational, cross-sectional study covering the first wave of the pandemic. Int. J. Environ. Res. Public Health 2021, 18, 3367. [Google Scholar] [CrossRef]
- Skjefte, M.; Ngirbabul, M.; Akeju, O.; Escudero, D.; Hernandez-Diaz, S.; Wyszynski, D.F.; Wu, J.W. COVID-19 vaccine acceptance among pregnant women and mothers of young children: Results of a survey in 16 countries. Eur. J. Epidemiol. 2021, 36, 197–211. [Google Scholar] [CrossRef]
- Caserotti, M.; Girardi, P.; Rubaltelli, E.; Tasso, A.; Lotto, L.; Gavaruzzi, T. Associations of COVID-19 risk perception with vaccine hesitancy over time for Italian residents. Soc. Sci. Med. 2021, 272, 113688. [Google Scholar] [CrossRef]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; Hyland, P. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 29. [Google Scholar] [CrossRef] [PubMed]
- Khubchandani, J.; Sharma, S.; Price, J.H.; Wiblishauser, M.J.; Sharma, M.; Webb, F.J. COVID-19 vaccination hesitancy in the United States: A rapid national assessment. J. Community Health 2021, 46, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Caserotti, M.; Girardi, P.; Tasso, A.; Rubaltelli, E.; Lotto, L.; Gavaruzzi, T. Joint analysis of the intention to vaccinate and to use contact tracing app during the COVID-19 pandemic. Sci. Rep. 2022, 12, 793. [Google Scholar] [CrossRef] [PubMed]
- Lilleholt, L.; Zettler, I.; Betsch, C.; Böhm, R. Pandemic fatigue: Measurement, correlates, and consequences. PsyArXiv 2020, preprint. [Google Scholar] [CrossRef]
- Caserotti, M.; Gavaruzzi, T.; Girardi, P.; Sellaro, R.; Rubaltelli, E.; Tasso, A.; Lotto, L. People’s perspectives about COVID-19 vaccination certificate: Findings from a representative Italian sample. Vaccine 2022, 40, 7406–7414. [Google Scholar] [CrossRef] [PubMed]
- Boccalini, S.; Vannacci, A.; Crescioli, G.; Lombardi, N.; Del Riccio, M.; Albora, G.; Bechini, A. Knowledge of university students in health care settings on vaccines and vaccinations strategies: Impact evaluation of a specific educational training course during the COVID-19 pandemic period in Italy. Vaccines 2022, 10, 1085. [Google Scholar] [CrossRef]
- Smithson, M.; Verkuilen, J. A better lemon squeezer? Maximum-likelihood regression with beta-distributed dependent variables. Psychol. Methods 2006, 11, 54. [Google Scholar] [CrossRef]
- Danchin, M.H.; Costa-Pinto, J.; Attwell, K.; Willaby, H.; Wiley, K.; Hoq, M.; Marshall, H. Vaccine decision-making begins in pregnancy: Correlation between vaccine concerns, intentions and maternal vaccination with subsequent childhood vaccine uptake. Vaccine 2018, 36, 6473–6479. [Google Scholar] [CrossRef]
- Thorpe, A.; Fagerlin, A.; Drews, F.A.; Shoemaker, H.; Scherer, L.D. Self-reported health behaviors and risk perceptions following the COVID-19 vaccination rollout in the US: An online survey study. Public Health 2022, 208, 68–71. [Google Scholar] [CrossRef]
- Attwell, K.; Leask, J.; Meyer, S.B.; Rokkas, P.; Ward, P. Vaccine rejecting parents’ engagement with expert systems that inform vaccination programs. J. Bioethical Inq. 2017, 14, 65–76. [Google Scholar] [CrossRef]
- Geiger, M.; Rees, F.; Lilleholt, L.; Santana, A.P.; Zettler, I.; Wilhelm, O.; Betsch, C.; Böhm, R. Measuring the 7Cs of vaccination readiness. Eur. J. Psychol. Assess. 2022, 38, 261–269. [Google Scholar] [CrossRef]
- Allington, D.; McAndrew, S.; Moxham-Hall, V.; Duffy, B. Coronavirus conspiracy suspicions, general vaccine attitudes, trust and coronavirus information source as predictors of vaccine hesitancy among UK residents during the COVID-19 pandemic. Psychol. Med. 2021, 53, 236–247. [Google Scholar] [CrossRef] [PubMed]
- Zarbo, C.; Candini, V.; Ferrari, C.; d’Addazio, M.; Calamandrei, G.; Starace, F.; De Girolamo, G. COVID-19 Vaccine Hesitancy in Italy: Predictors of Acceptance, Fence Sitting and Refusal of the COVID-19 Vaccination. Front. Public Health 2022, 10, 873098. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.E.; Sivertsen, N.; Lines, L.; De Bellis, A. Decision making in vaccine hesitant parents and pregnant women–An integrative review. Int. J. Nurs. Stud. Adv. 2022, 4, 100062. [Google Scholar] [CrossRef]
- Caserotti, M.; Gavaruzzi, T.; Girardi, P.; Tasso, A.; Buizza, C.; Candini, V.; Lotto, L. Who is likely to vacillate in their COVID-19 vaccination decision? Free-riding intention and post-positive reluctance. Prev. Med. 2022, 154, 106885. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Overall, N = 1104 1 | C19 Vaccine Status | p-Value 2 | |
|---|---|---|---|---|
| Not Vaccinated, N = 592 1 | Vaccinated, N = 512 1 | |||
| Age (years) | 34.0 (31.0, 37.0) | 34.0 (31.0, 37.0) | 35.0 (32.0, 37.0) | 0.012 |
| Education | <0.001 | |||
| Middle school | 25 (2.3%) | 15 (2.5%) | 10 (2.0%) | |
| High school | 318 (29%) | 212 (36%) | 106 (21%) | |
| University degree | 581 (53%) | 289 (49%) | 292 (57%) | |
| Higher level degree | 180 (16%) | 76 (13%) | 104 (20%) | |
| Employment | 0.516 | |||
| Private or public employee | 735 (67%) | 392 (66%) | 343 (67%) | |
| Unemployed or Other | 182 (16%) | 104 (18%) | 78 (15%) | |
| Self-employed | 187 (17%) | 96 (16%) | 91 (18%) | |
| Other Children | 0.238 | |||
| No | 476 (43%) | 266 (45%) | 210 (41%) | |
| 1 | 481 (44%) | 244 (41%) | 237 (46%) | |
| 2+ | 147 (13%) | 82 (14%) | 65 (13%) | |
| Mother Status | <0.001 | |||
| Breastfeeding | 572 (52%) | 188 (32%) | 384 (75%) | |
| Pregnacy | 532 (48%) | 404 (68%) | 128 (25%) | |
| C19 Risk Perception | 0.19 (−0.58, 0.70) | −0.19 (−1.09, 0.58) | 0.41 (−0.02, 0.77) | <0.001 |
| Pandemic Fatigue | 0.04 (−0.62, 0.64) | 0.21 (−0.50 0.79) | −0.18 (−0.68, 0.39) | <0.001 |
| Pro-vax Attitude | 0.17 (−0.57, 0.74) | −0.25 (−0.96, 0.47) | 0.48 (0.01, 0.99) | <0.001 |
| C19 Conspiracy score | −0.30 (−0.79, 0.66) | 0.51 (−0.36, 1.26) | −0.70 (−0.96, −0.32) | <0.001 |
| C19 Vaccine Perception of | Overall, N = 1104 1 | C19 Vaccine Status | p-Value 2 | |
|---|---|---|---|---|
| Not Vaccinated, N = 592 | Vaccinated, N = 512 1 | |||
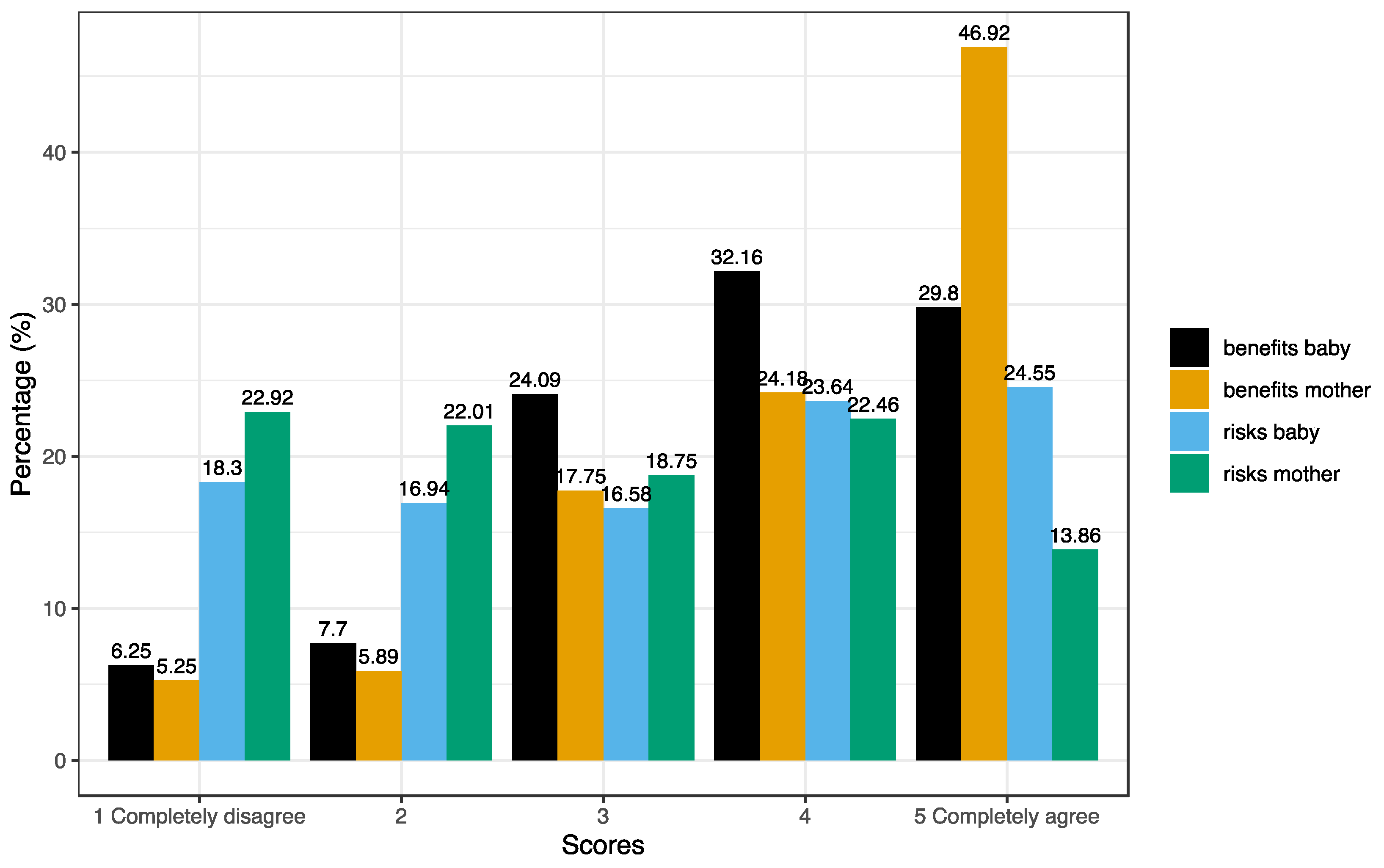
| Risks for baby | 3 (2, 4) | 4 (4, 5) | 2 (1, 3) | <0.001 |
| Risks for mother | 3 (2, 4) | 4 (2, 4) | 2 (1, 3) | <0.001 |
| Benefits for baby | 4 (3, 5) | 3 (3, 4) | 5 (4, 5) | <0.001 |
| Benefits for mother | 4 (3, 5) | 4 (3, 4) | 5 (5, 5) | <0.001 |
| C19 Vax | Mother Status | C19 Vaccine Status | |||||
|---|---|---|---|---|---|---|---|
| Overall, N = 1104 1 | Breasfeeding, N = 572 1 | Pregnancy, N = 532 1 | p-Value 2 | Not Vaccinated, N = 592 1 | Vaccinated, N = 512 1 | p-Value 2 | |
| Risks/benefits ratio | 0.75 (0.44, 1.17) | 0.62 (0.40, 1.00) | 0.89 (0.56, 1.33) | <0.001 | 1.14 (0.80, 1.60) | 0.44 (0.30, 0.67) | <0.001 |
| Baby/mother ratio | 1.00 (1.00, 2.00) | 1.00 (0.83, 1.67) | 1.25 (1.00, 2.00) | <0.001 | 1.25 (1.00, 2.02) | 1.00 (0.83, 1.33) | <0.001 |
| Predictors | OR | 95%CI | p-Values |
|---|---|---|---|
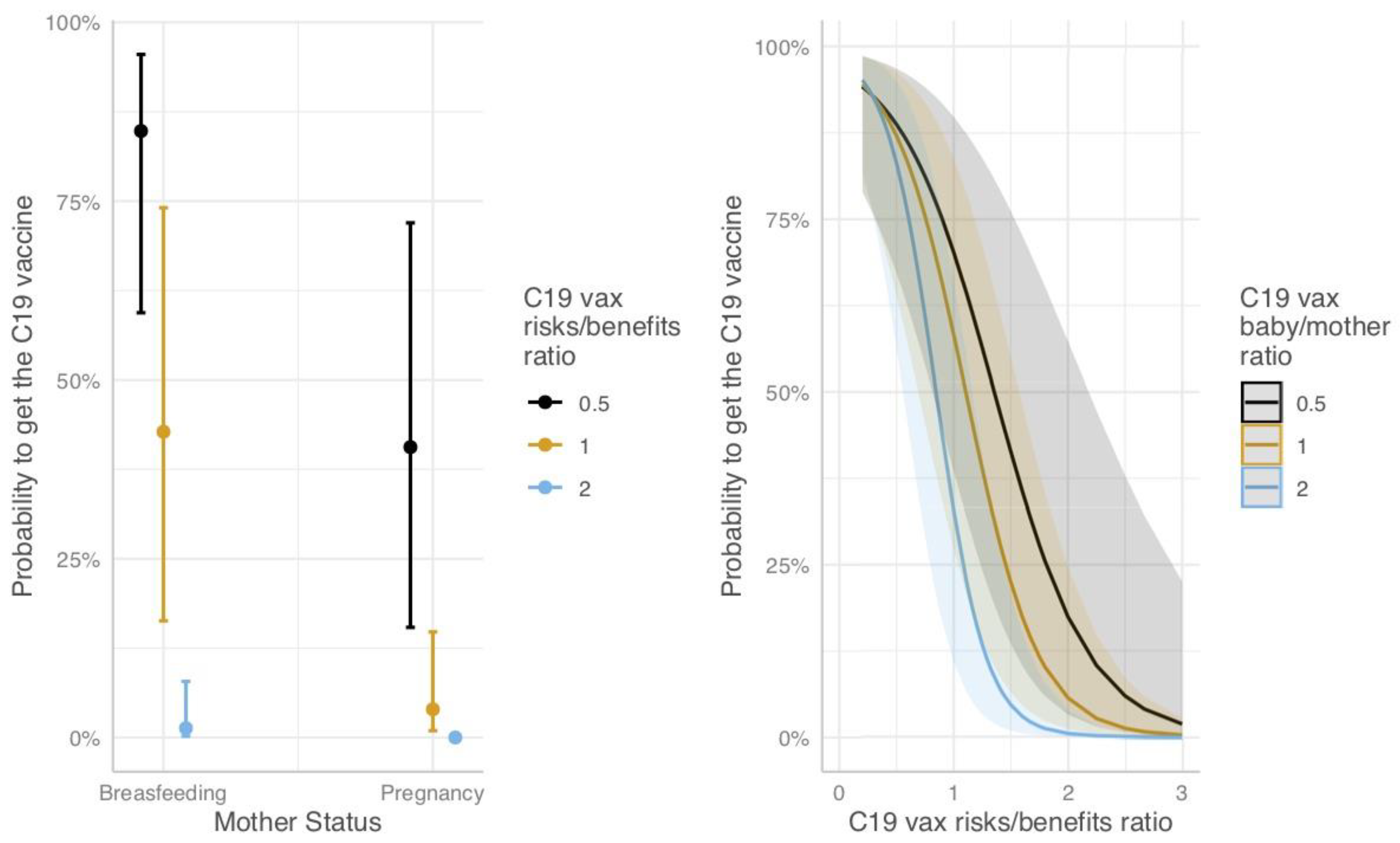
| COVID-19 vax risks/benefits overall ratio | 0.19 | 0.04–0.74 | 0.021 |
| COVID-19 vax baby/mother risks/benefits ratio | 1.52 | 0.81–2.90 | 0.193 |
| Mother Status [Pregnancy] | 0.27 | 0.10–0.76 | 0.012 |
| Age (+1 years) | 1.04 | 0.98–1.09 | 0.175 |
| Education [High school] | 0.89 | 0.23–3.15 | 0.858 |
| Education [University Degree] | 1.04 | 0.27–3.63 | 0.955 |
| Education [High level degree] | 1.10 | 0.27–4.21 | 0.891 |
| Employment [Unemployed or Other] | 1.14 | 0.64–2.03 | 0.666 |
| Employment [Self-employed] | 1.21 | 0.69–2.14 | 0.512 |
| Other Children [1] | 1.03 | 0.66–1.59 | 0.905 |
| Other Children [2+] | 0.81 | 0.42–1.55 | 0.513 |
| COVID-19 Conspiracy score 2 | 0.36 | 0.24–0.54 | <0.001 |
| Pandemic Fatigue 2 | 1.44 | 1.13–1.83 | 0.003 |
| COVID-19 vax risks/benefits ratio×Mother Status [Pregnancy] | 0.20 | 0.05–0.82 | 0.029 |
| COVID-19 vax risks/benefits ratio×COVID-19 vax baby/mother ratio | 0.23 | 0.08–0.60 | 0.003 |
| Observations | 1104 | ||
| R2 Tjur | 0.636 | ||
| Predictors | WTV in Current Status | WTV if Not Preg./Breast. | ||||
|---|---|---|---|---|---|---|
| OR | 95%CI | p-Values | OR | 95%CI | p-Values | |
| COVID-19 vax risks/benefits ratio | 0.83 | 0.73–0.94 | 0.003 | 0.79 | 0.69–0.90 | <0.001 |
| COVID-19 vax baby/mother ratio | 0.87 | 0.83–0.92 | <0.001 | 1.05 | 1.00–1.11 | 0.045 |
| Mother Status [Pregnancy] | 0.61 | 0.49–0.76 | <0.001 | NS | - | - |
| Age (+1 years) | 0.99 | 0.96–1.01 | 0.234 | 0.98 | 0.95–1.00 | 0.075 |
| Education [High school] | 0.68 | 0.36–1.30 | 0.246 | 0.97 | 0.51–1.84 | 0.924 |
| Education [University Degree] | 0.74 | 0.39–1.41 | 0.362 | 0.86 | 0.45–1.64 | 0.643 |
| Education [High level degree] | 0.78 | 0.39–1.57 | 0.487 | 0.96 | 0.48–1.91 | 0.898 |
| Employment [Unemployed or Other] | 0.98 | 0.74–1.29 | 0.882 | 0.90 | 0.69–1.18 | 0.460 |
| Employment [Self-employed] | 0.84 | 0.63–1.11 | 0.223 | 0.89 | 0.67–1.17 | 0.401 |
| Other Children [1] | 1.03 | 0.82–1.29 | 0.804 | 0.94 | 0.75–1.16 | 0.548 |
| Other Children [2+] | 1.11 | 0.81–1.53 | 0.517 | 0.83 | 0.61–1.14 | 0.247 |
| COVID-19 Risk Perception 2 | 1.24 | 1.10–1.39 | <0.001 | 1.43 | 1.27–1.61 | <0.001 |
| COVID-19 Conspiracy score 2 | 0.57 | 0.49–0.67 | <0.001 | 0.59 | 0.49–0.71 | <0.001 |
| Pro-vax Attitude 2 | NS | - | - | 1.18 | 1.02–1.36 | 0.026 |
| Observations | 592 | 592 | ||||
| R2 | 0.406 | 0.611 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gavaruzzi, T.; Caserotti, M.; Bonaiuti, R.; Bonanni, P.; Crescioli, G.; Di Tommaso, M.; Lombardi, N.; Lotto, L.; Ravaldi, C.; Rubaltelli, E.; et al. The Interplay of Perceived Risks and Benefits in Deciding to Become Vaccinated against COVID-19 While Pregnant or Breastfeeding: A Cross-Sectional Study in Italy. J. Clin. Med. 2023, 12, 3469. https://doi.org/10.3390/jcm12103469
Gavaruzzi T, Caserotti M, Bonaiuti R, Bonanni P, Crescioli G, Di Tommaso M, Lombardi N, Lotto L, Ravaldi C, Rubaltelli E, et al. The Interplay of Perceived Risks and Benefits in Deciding to Become Vaccinated against COVID-19 While Pregnant or Breastfeeding: A Cross-Sectional Study in Italy. Journal of Clinical Medicine. 2023; 12(10):3469. https://doi.org/10.3390/jcm12103469
Chicago/Turabian StyleGavaruzzi, Teresa, Marta Caserotti, Roberto Bonaiuti, Paolo Bonanni, Giada Crescioli, Mariarosaria Di Tommaso, Niccolò Lombardi, Lorella Lotto, Claudia Ravaldi, Enrico Rubaltelli, and et al. 2023. "The Interplay of Perceived Risks and Benefits in Deciding to Become Vaccinated against COVID-19 While Pregnant or Breastfeeding: A Cross-Sectional Study in Italy" Journal of Clinical Medicine 12, no. 10: 3469. https://doi.org/10.3390/jcm12103469
APA StyleGavaruzzi, T., Caserotti, M., Bonaiuti, R., Bonanni, P., Crescioli, G., Di Tommaso, M., Lombardi, N., Lotto, L., Ravaldi, C., Rubaltelli, E., Tasso, A., Vannacci, A., & Girardi, P. (2023). The Interplay of Perceived Risks and Benefits in Deciding to Become Vaccinated against COVID-19 While Pregnant or Breastfeeding: A Cross-Sectional Study in Italy. Journal of Clinical Medicine, 12(10), 3469. https://doi.org/10.3390/jcm12103469