
Effects of Severe Varus Deformity on Soft Tissue Balancing in Total Knee Arthroplasty



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
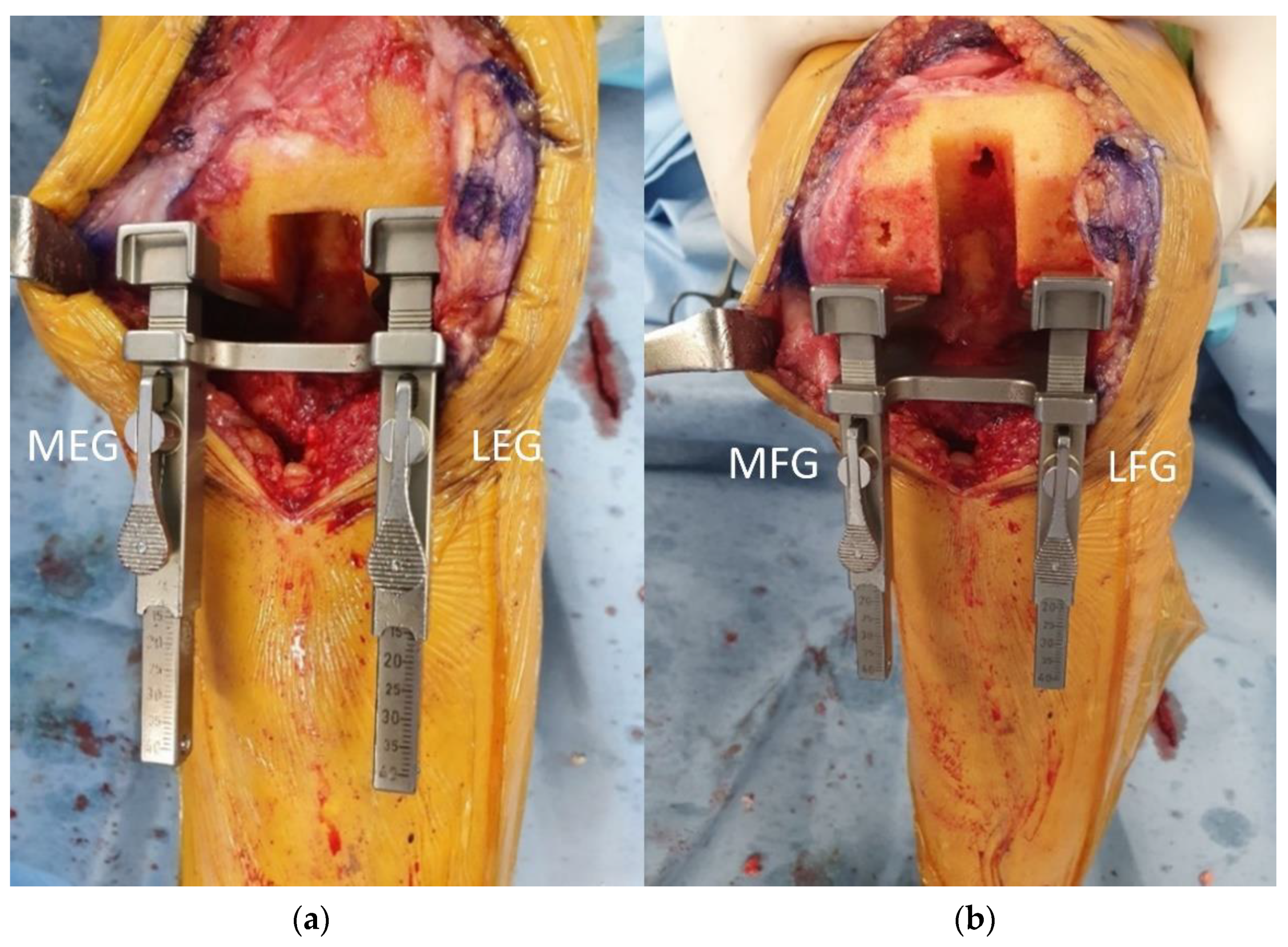
2.2. Surgical Technique and Gap Measurement
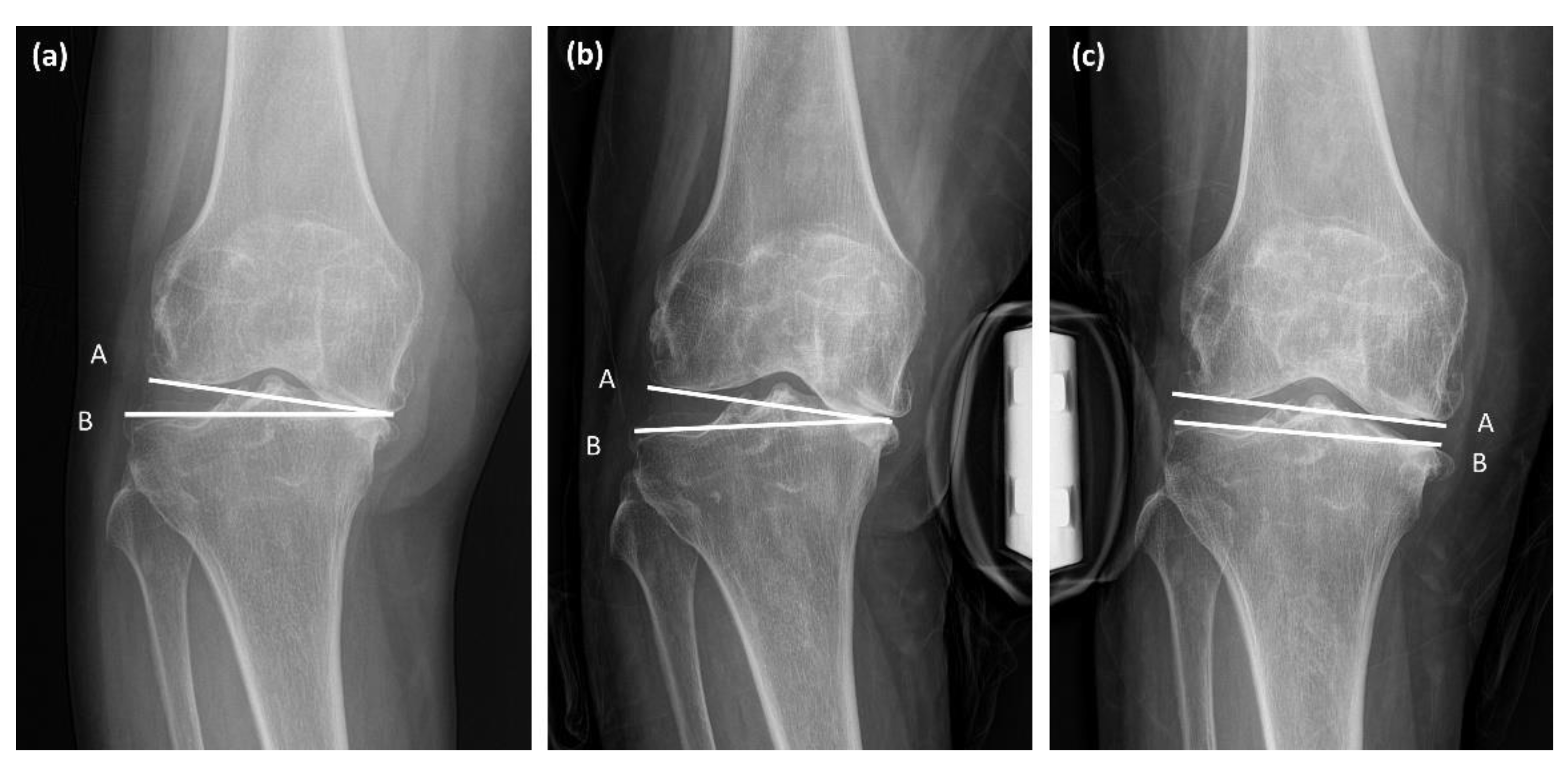
2.3. Clinical and Radiologic Assessments
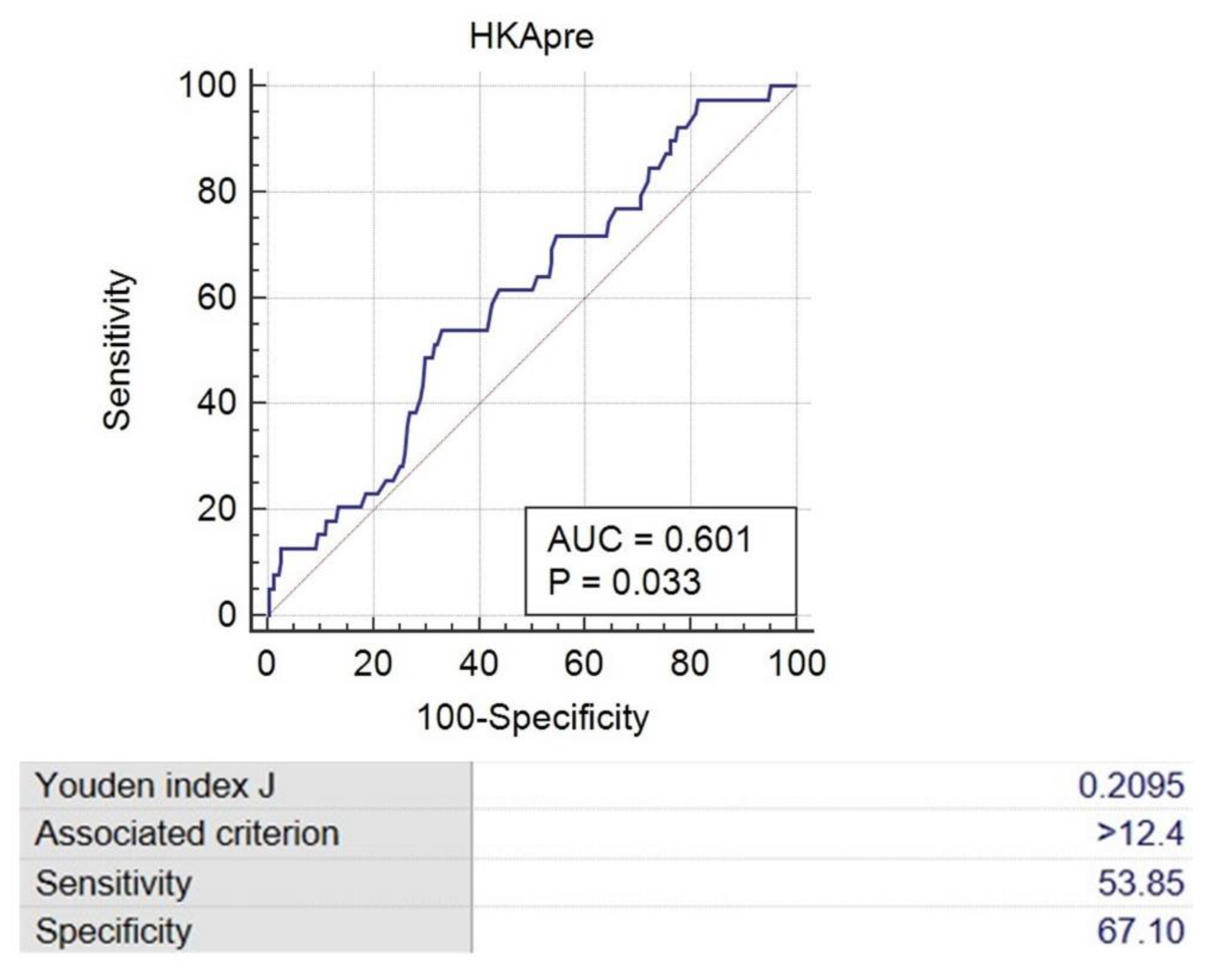
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Singh, D.; Patel, K.C.; Singh, R.D. Achieving coronal plane alignment in total knee arthroplasty through modified preoperative planning based on long-leg radiographs: A prospective study. J. Exp. Orthop. 2021, 8, 100. [Google Scholar] [CrossRef] [PubMed]
- Roof, M.A.; Kreinces, J.B.; Schwarzkopf, R.; Rozell, J.C.; Aggarwal, V.K. Are there avoidable causes of early revision total knee arthroplasty? Knee Surg. Relat. Res. 2022, 34, 29. [Google Scholar] [CrossRef] [PubMed]
- Yagishita, K.; Muneta, T.; Ikeda, H. Step-by-step measurements of soft tissue balancing during total knee arthroplasty for patients with varus knees. J. Arthroplast. 2003, 18, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Insall, J.N.; Binazzi, R.; Soudry, M.; Mestriner, L.A. Total knee arthroplasty. Clin. Orthop. Relat. Res. 1985, 192, 13–22. [Google Scholar] [CrossRef]
- Insall, J.; Scott, W.N.; Ranawat, C.S. The total condylar knee prosthesis. A report of two hundred and twenty cases. J. Bone Joint. Surg. Am. 1979, 61, 173–180. [Google Scholar] [CrossRef]
- Sugama, R.; Kadoya, Y.; Kobayashi, A.; Takaoka, K. Preparation of the flexion gap affects the extension gap in total knee arthroplasty. J. Arthroplast. 2005, 20, 602–607. [Google Scholar] [CrossRef]
- Mihalko, W.M.; Saleh, K.J.; Krackow, K.A.; Whiteside, L.A. Soft-tissue balancing during total knee arthroplasty in the varus knee. J. Am. Acad. Orthop. Surg. 2009, 17, 766–774. [Google Scholar] [CrossRef]
- Lee, O.S.; Elazab, A.; Lee, Y.S. Preoperative Varus-Valgus Stress Angle Difference Is Valuable for Predicting the Extent of Medial Release in Varus Deformity during Total Knee Arthroplasty. Knee Surg. Relat. Res. 2019, 31, 12–18. [Google Scholar] [CrossRef]
- Moon, Y.W.; Kim, J.G.; Han, J.H.; Do, K.H.; Seo, J.G.; Lim, H.C. Factors correlated with the reducibility of varus deformity in knee osteoarthritis: An analysis using navigation guided TKA. Clin. Orthop. Surg. 2013, 5, 36–43. [Google Scholar] [CrossRef]
- Mullaji, A.B.; Padmanabhan, V.; Jindal, G. Total knee arthroplasty for profound varus deformity: Technique and radiological results in 173 knees with varus of more than 20 degrees. J. Arthroplast. 2005, 20, 550–561. [Google Scholar] [CrossRef]
- De Muylder, J.; Victor, J.; Cornu, O.; Kaminski, L.; Thienpont, E. Total knee arthroplasty in patients with substantial deformities using primary knee components. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 3653–3659. [Google Scholar] [CrossRef] [PubMed]
- Thienpont, E.; Parvizi, J. A New Classification for the Varus Knee. J. Arthroplast. 2016, 31, 2156–2160. [Google Scholar] [CrossRef] [PubMed]
- Tian, F.; Zang, X.H.; Sun, Y.S. Impact of knee varus and valgus deformity on alignment in lower extremities after total knee arthroplasty (TKA). Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 83–89. [Google Scholar] [CrossRef]
- Sekiya, H.; Takatoku, K.; Takada, H.; Sasanuma, H.; Sugimoto, N. Postoperative lateral ligamentous laxity diminishes with time after TKA in the varus knee. Clin. Orthop. Relat. Res. 2009, 467, 1582–1586. [Google Scholar] [CrossRef] [PubMed]
- Ishibashi, K.; Sasaki, E.; Sasaki, S.; Kimura, Y.; Yamamoto, Y.; Ishibashi, Y. Medial stabilizing technique preserves anatomical joint line and increases range of motion compared with the gap-balancing technique in navigated total knee arthroplasty. Knee 2020, 27, 558–564. [Google Scholar] [CrossRef]
- Tanaka, K.; Muratsu, H.; Mizuno, K.; Kuroda, R.; Yoshiya, S.; Kurosaka, M. Soft tissue balance measurement in anterior cruciate ligament-resected knee joint: Cadaveric study as a model for cruciate-retaining total knee arthroplasty. J. Orthop. Sci. 2007, 12, 149–153. [Google Scholar] [CrossRef]
- Lee, D.H.; Padhy, D.; Park, J.H.; Jeong, W.K.; Han, S.B. The impact of a rectangular or trapezoidal flexion gap on the femoral component rotation in TKA. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 1141–1147. [Google Scholar] [CrossRef]
- Lee, D.H.; Park, J.H.; Song, D.I.; Padhy, D.; Jeong, W.K.; Han, S.B. Accuracy of soft tissue balancing in TKA: Comparison between navigation-assisted gap balancing and conventional measured resection. Knee Surg. Sports Traumatol. Arthrosc. 2010, 18, 381–387. [Google Scholar] [CrossRef]
- Lee, D.H.; Park, S.C.; Park, H.J.; Han, S.B. Effect of soft tissue laxity of the knee joint on limb alignment correction in open-wedge high tibial osteotomy. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 3704–3712. [Google Scholar] [CrossRef]
- Lee, D.H.; Shin, Y.S.; Jeon, J.H.; Suh, D.W.; Han, S.B. Flexion and extension gaps created by the navigation-assisted gap technique show small acceptable mismatches and close mutual correlations. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 1793–1798. [Google Scholar] [CrossRef]
- Shon, O.J.; Kim, G.B. Does the degree of intraoperatively identified cartilage loss affect the outcomes of primary total knee arthroplasty without patella resurfacing? A prospective comparative cohort study. Knee Surg. Relat. Res. 2022, 34, 36. [Google Scholar] [CrossRef] [PubMed]
- Piovan, G.; Farinelli, L.; Screpis, D.; Iacono, V.; Povegliano, L.; Bonomo, M.; Auregli, L.; Zorzi, C. Distal femoral osteotomy versus lateral unicompartmental arthroplasty for isolated lateral tibiofemoral osteoarthritis with intra-articular and extra-articular deformity: A propensity score-matched analysis. Knee Surg. Relat. Res. 2022, 34, 34. [Google Scholar] [CrossRef] [PubMed]
- Moon, Y.W.; Park, J.H.; Lee, S.S.; Kang, J.W.; Lee, D.H. Distal femoral phenotypes in Asian varus osteoarthritic knees. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 456–463. [Google Scholar] [CrossRef]
- Lee, H.J.; Kim, S.H.; Park, Y.B. Selective medial release using multiple needle puncturing with a spacer block in situ for correcting severe varus deformity during total knee arthroplasty. Arch. Orthop. Trauma Surg. 2020, 140, 1523–1531. [Google Scholar] [CrossRef] [PubMed]
- Herschmiller, T.; Grosso, M.J.; Cunn, G.J.; Murtaugh, T.S.; Gardner, T.R.; Geller, J.A. Step-wise medial collateral ligament needle puncturing in extension leads to a safe and predictable reduction in medial compartment pressure during TKA. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 1759–1766. [Google Scholar] [CrossRef] [PubMed]
- Azukizawa, M.; Kuriyama, S.; Nakamura, S.; Nishitani, K.; Lyman, S.; Morita, Y.; Furu, M.; Ito, H.; Matsuda, S. Intraoperative medial joint laxity in flexion decreases patient satisfaction after total knee arthroplasty. Arch. Orthop. Trauma Surg. 2018, 138, 1143–1150. [Google Scholar] [CrossRef] [PubMed]
- Ramappa, M. Midflexion instability in primary total knee replacement: A review. SICOT J. 2015, 1, 24. [Google Scholar] [CrossRef]
- Tsukiyama, H.; Kuriyama, S.; Kobayashi, M.; Nakamura, S.; Furu, M.; Ito, H.; Matsuda, S. Medial rather than lateral knee instability correlates with inferior patient satisfaction and knee function after total knee arthroplasty. Knee 2017, 24, 1478–1484. [Google Scholar] [CrossRef]
- Jawhar, A.; Shah, V.; Sohoni, S.; Scharf, H.P. Joint line changes after primary total knee arthroplasty: Navigated versus non-navigated. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 2355–2362. [Google Scholar] [CrossRef]
- Okazaki, K.; Miura, H.; Matsuda, S.; Takeuchi, N.; Mawatari, T.; Hashizume, M.; Iwamoto, Y. Asymmetry of mediolateral laxity of the normal knee. J. Orthop. Sci. 2006, 11, 264–266. [Google Scholar] [CrossRef]
- Lee, Y.S.; Howell, S.M.; Won, Y.Y.; Lee, O.S.; Lee, S.H.; Vahedi, H.; Teo, S.H. Kinematic alignment is a possible alternative to mechanical alignment in total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 3467–3479. [Google Scholar] [CrossRef] [PubMed]
- Slevin, O.; Hirschmann, A.; Schiapparelli, F.F.; Amsler, F.; Huegli, R.W.; Hirschmann, M.T. Neutral alignment leads to higher knee society scores after total knee arthroplasty in preoperatively non-varus patients: A prospective clinical study using 3D-CT. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 1602–1609. [Google Scholar] [CrossRef] [PubMed]
- An, V.V.G.; Twiggs, J.; Leie, M.; Fritsch, B.A. Kinematic alignment is bone and soft tissue preserving compared to mechanical alignment in total knee arthroplasty. Knee 2019, 26, 466–476. [Google Scholar] [CrossRef] [PubMed]
- Daines, B.K.; Dennis, D.A. Gap balancing vs. measured resection technique in total knee arthroplasty. Clin. Orthop. Surg. 2014, 6, 1050221. [Google Scholar] [CrossRef]
- Schwarzkopf, R.; Meftah, M.; Marwin, S.E.; Zabat, M.A.; Muir, J.M.; Lamb, I.R. The use of imageless navigation to quantify cutting error in total knee arthroplasty. Knee Surg. Relat. Res. 2021, 33, 43. [Google Scholar] [CrossRef]
- Meftah, M.; Blum, Y.C.; Raja, D.; Ranawat, A.S.; Ranawat, C.S. Correcting fixed varus deformity with flexion contracture during total knee arthroplasty: The ”inside-out” technique: AAOS exhibit selection. J. Bone Jt. Surg. Am. 2012, 94, e66. [Google Scholar] [CrossRef]
- Okamoto, S.; Okazaki, K.; Mitsuyasu, H.; Matsuda, S.; Iwamoto, Y. Lateral soft tissue laxity increases but medial laxity does not contract with varus deformity in total knee arthroplasty. Clin. Orthop. Relat. Res. 2013, 471, 1334–1342. [Google Scholar] [CrossRef]
- Matsumoto, T.; Muratsu, H.; Kubo, S.; Matsushita, T.; Kurosaka, M.; Kuroda, R. The influence of preoperative deformity on intraoperative soft tissue balance in posterior-stabilized total knee arthroplasty. J. Arthroplast. 2011, 26, 1291–1298. [Google Scholar] [CrossRef]
- Kuroyanagi, Y.; Nagura, T.; Kiriyama, Y.; Matsumoto, H.; Otani, T.; Toyama, Y.; Suda, Y. A quantitative assessment of varus thrust in patients with medial knee osteoarthritis. Knee 2012, 19, 130–134. [Google Scholar] [CrossRef]
- Song, S.J.; Park, C.H.; Bae, D.K. What to Know for Selecting Cruciate-Retaining or Posterior-Stabilized Total Knee Arthroplasty. Clin. Orthop. Surg. 2019, 11, 142–150. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall | Varus < 10° | Varus ≥ 10° | p-Value | |
|---|---|---|---|---|
| Sample size (number) | 270 | 116 | 154 | |
| Sex (male/female) | 52/218 | 18/98 | 34/120 | 0.176 |
| Age (years) | 72.3 ± 6.1 | 71.4 ± 6.0 | 72.9 ± 6.2 | 0.41 |
| Height (cm) | 154.3 ± 7.3 | 155.5 ± 7.4 | 153.4 ± 7.2 | 0.553 |
| Weight (kg) | 65.0 ± 11.7 | 66.9 ± 12.4 | 63.5 ± 10.9 | 0.067 |
| Body mass index (kg/m2) | 27.2 ± 3.8 | 27.6 ± 4.0 | 26.8 ± 3.7 | 0.135 |
| Preoperative ROM | 110.4 ± 15.6 | 112.6 ± 15.8 | 108.7 ± 15.3 | 0.438 |
| Preoperative HSS | 23.3 ± 12.6 | 24.6 ± 13.0 | 21.9 ± 11.6 | 0.603 |
| Overall | Varus < 10° | Varus ≥ 10° | p-Value | |
|---|---|---|---|---|
| (N = 270) | (N = 116) | (N = 154) | ||
| MFG (mm) | 19.20 ± 1.99 | 18.72 ± 1.68 | 19.57 ± 2.13 | <0.001 |
| LFG (mm) | 20.47 ± 2.13 | 19.76 ± 1.84 | 20.99 ± 2.19 | <0.001 |
| MEG (mm) | 19.11 ± 2.05 | 18.67 ± 1.78 | 19.44 ± 2.18 | 0.002 |
| LEG (mm) | 20.35 ± 2.28 | 19.64 ± 1.98 | 20.89 ± 2.35 | <0.001 |
| FGD(LFG-MFG) (mm) | 1.26 ± 1.28 | 1.05 ± 1.16 | 1.42 ± 1.35 | 0.019 |
| EGD(LEG-MEG) (mm) | 1.24 ± 1.43 | 0.97 ± 1.53 | 1.45 ± 1.32 | 0.006 |
| Overall | Varus < 10° | Varus ≥ 10° | p-Value | |
|---|---|---|---|---|
| (N = 270) | (N = 116) | (N = 154) | ||
| HKA varus angle (°) | 11.07 ± 4.91 | 6.73 ± 2.27 | 14.33 ± 3.66 | <0.001 |
| mLDFA (°) | 89.81 ± 2.41 | 89.03 ± 2.33 | 90.77 ± 5.06 | 0.001 |
| MPTA (°) | 84.31 ± 3.02 | 85.86 ± 2.40 | 83.14 ± 2.92 | <0.001 |
| JLCA (°) | 5.35 ± 2.48 | 4.16 ± 1.99 | 6.24 ± 2.44 | <0.001 |
| JLCA under varus stress (°) | 7.32 ± 2.80 | 6.88 ± 2.13 | 8.01 ± 3.03 | 0.001 |
| JLCA under valgus stress (°) | 2.28 ± 1.79 | −0.12 ± 2.31 | −0.05 ± 2.30 | 0.805 |
| FGD | EGD | |
|---|---|---|
| HKA varus angle (°) | 0.264 (<0.001) | 0.319 (<0.001) |
| mLDFA (°) | 0.123 (0.043) | 0.089 (0.146) |
| MPTA (°) | −0.192 (0.002) | −0.323 (<0.001) |
| JLCA (°) | 0.105 (0.085) | 0.140 (0.021) |
| JLCA under varus stress (°) | 0.153 (0.021) | 0.177 (0.004) |
| JLCA under valgus stress (°) | −0.097 (0.113) | 0.014 (0.814) |
| Dependent Variables | Independent Variables | Non-Standardized Coefficients | Standardized Coefficients | ||
|---|---|---|---|---|---|
| B | SE | β | p-Value | ||
| FGD | HKA varus angle | 0.06 | 0.029 | 0.232 | 0.04 |
| MPTA | −0.046 | 0.038 | −0.11 | 0.239 | |
| mLDFA | 0 | 0.042 | 0.153 | 0.639 | |
| JLCA under varus stress | 0.072 | 0.028 | 0 | 0.012 | |
| JLCA under valgus stress | −0.102 | 0.092 | −0.103 | 0.092 | |
| EGD | HKA varus angle | 0.066 | 0.031 | 0.229 | 0.037 |
| MPTA | −0.114 | 0.041 | −0.244 | 0.006 | |
| mLDFA | −0.025 | 0.045 | −0.042 | 0.58 | |
| JLCA under varus stress | 0.093 | 0.031 | 0.177 | 0.004 | |
| JLCA under valgus stress | −0.005 | 0.04 | −0.008 | 0.894 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwak, I.-H.; Lee, S.-S.; Lee, J.; Lee, D.-H. Effects of Severe Varus Deformity on Soft Tissue Balancing in Total Knee Arthroplasty. J. Clin. Med. 2023, 12, 263. https://doi.org/10.3390/jcm12010263
Kwak I-H, Lee S-S, Lee J, Lee D-H. Effects of Severe Varus Deformity on Soft Tissue Balancing in Total Knee Arthroplasty. Journal of Clinical Medicine. 2023; 12(1):263. https://doi.org/10.3390/jcm12010263
Chicago/Turabian StyleKwak, Il-Hoon, Sung-Sahn Lee, Jeounghun Lee, and Dae-Hee Lee. 2023. "Effects of Severe Varus Deformity on Soft Tissue Balancing in Total Knee Arthroplasty" Journal of Clinical Medicine 12, no. 1: 263. https://doi.org/10.3390/jcm12010263
APA StyleKwak, I.-H., Lee, S.-S., Lee, J., & Lee, D.-H. (2023). Effects of Severe Varus Deformity on Soft Tissue Balancing in Total Knee Arthroplasty. Journal of Clinical Medicine, 12(1), 263. https://doi.org/10.3390/jcm12010263