
Albumin as a Prognostic Marker for Atrial Fibrillation Recurrence following Cryoballoon Ablation of Pulmonary Venous
 , , , , , ,
, , , , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Ablation
2.2. Study Groups
2.3. Follow Up and Outcomes
2.4. Statistical Analysis
3. Results
3.1. Comparison across SA Tertiles
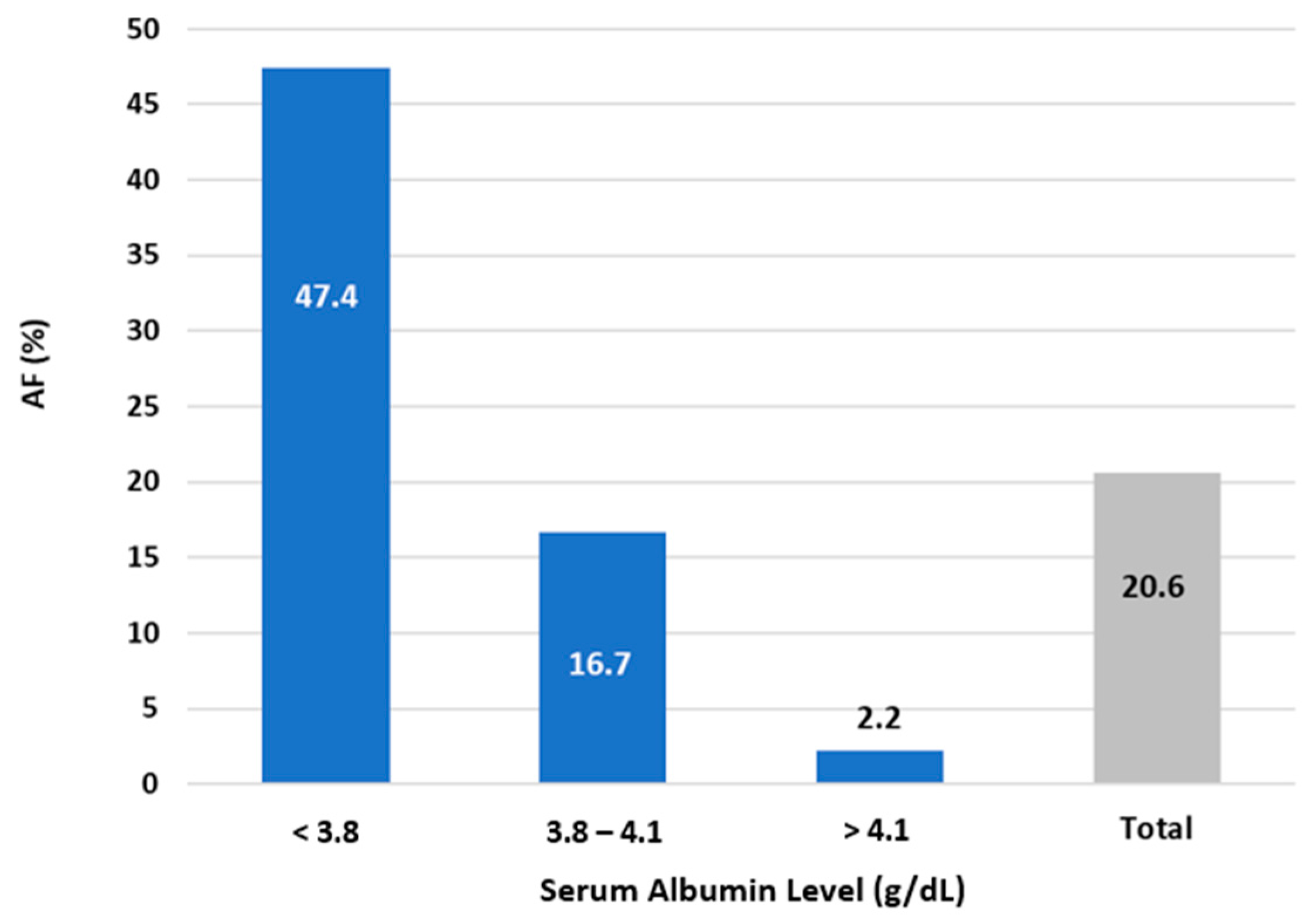
3.2. Follow up and Outcome
3.3. Association between SA Level and Recurrent AF
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart disease and stroke statistics—2019 update: A report from the American heart association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Kirchhof, P.; Camm, A.J.; Goette, A.; Brandes, A.; Eckardt, L.; Elvan, A.; Fetsch, T.; van Gelder, I.C.; Haase, D.; Haegeli, L.M.; et al. Early Rhythm-Control Therapy in Patients with Atrial Fibrillation. N. Engl. J. Med. 2020, 383, 1305–1316. [Google Scholar] [CrossRef] [PubMed]
- Pappone, C.; Augello, G.; Sala, S.; Gugliotta, F.; Vicedomini, G.; Gulletta, S.; Paglino, G.; Mazzone, P.; Sora, N.; Greiss, I.; et al. A Randomized Trial of Circumferential Pulmonary Vein Ablation Versus Antiarrhythmic Drug Therapy in Paroxysmal Atrial Fibrillation: The APAF Study. J. Am. Coll. Cardiol. 2006, 48, 2340–2347. [Google Scholar] [CrossRef] [PubMed]
- Nyong, J.; Amit, G.; Adler, A.J.; Owolabi, O.O.; Perel, P.; Prieto-Merino, D.; Lambiase, P.; Casas, J.P.; Morillo, C.A. Efficacy and safety of ablation for people with non-paroxysmal atrial fibrillation. Cochrane Database Syst. Rev. 2011, 2016, CD012088. [Google Scholar] [CrossRef] [PubMed]
- Andrade, J.G.; Wells, G.A.; Deyell, M.W.; Bennett, M.; Essebag, V.; Champagne, J.; Roux, J.-F.; Yung, D.; Skanes, A.; Khaykin, Y.; et al. Cryoablation or Drug Therapy for Initial Treatment of Atrial Fibrillation. N. Engl. J. Med. 2021, 384, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Kuck, K.-H.; Brugada, J.; Fürnkranz, A.; Metzner, A.; Ouyang, F.; Chun, K.J.; Elvan, A.; Arentz, T.; Bestehorn, K.; Pocock, S.J.; et al. Cryoballoon or Radiofrequency Ablation for Paroxysmal Atrial Fibrillation. N. Engl. J. Med. 2016, 374, 2235–2245. [Google Scholar] [CrossRef] [PubMed]
- January, C.T.; Wann, L.S.; Alpert, J.S.; Calkins, F.H.; Cigarroa, J.E.; Cleveland, J.C.; Conti, J.B.; Ellinor, P.; Ezekowitz, M.D.; Field, M.E.; et al. 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation 2014, 130, e199–e267. [Google Scholar] [CrossRef]
- Calkins, H.; Hindricks, G.; Cappato, R.; Kim, Y.-H.; Saad, E.B.; Aguinaga, L.; Akar, J.G.; Badhwar, V.; Brugada, J.; Camm, J.; et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Heart Rhythm. 2017, 14, e275–e444. [Google Scholar] [CrossRef]
- Wazni, O.M.; Dandamudi, G.; Sood, N.; Hoyt, R.; Tyler, J.; Durrani, S.; Niebauer, M.; Makati, K.; Halperin, B.; Gauri, A.; et al. Cryoballoon Ablation as Initial Therapy for Atrial Fibrillation. N. Engl. J. Med. 2021, 384, 316–324. [Google Scholar] [CrossRef]
- Su, W.; Aryana, A.; Passman, R.; Singh, G.; Hokanson, R.; Kowalski, M.; Andrade, J.; Wang, P. Cryoballoon Best Practices II: Practical guide to procedural monitoring and dosing during atrial fibrillation ablation from the perspective of experienced users. Heart Rhythm 2018, 15, 1348–1355. [Google Scholar] [CrossRef]
- Arques, S. Human serum albumin in cardiovascular diseases. Eur. J. Intern. Med. 2018, 52, 8–12. [Google Scholar] [CrossRef]
- van Beek, D.E.; Kuijpers, Y.A.; Königs, M.H.; van der Horst, I.C.; Scheeren, T.W. Low serum albumin levels and new-onset atrial fibrillation in the ICU: A prospective cohort study. J. Crit. Care 2020, 56, 26–30. [Google Scholar] [CrossRef]
- Liao, L.-Z.; Zhang, S.-Z.; Li, W.-D.; Liu, Y.; Li, J.-P.; Zhuang, X.-D.; Liao, X.-X. Serum albumin and atrial fibrillation: Insights from epidemiological and mendelian randomization studies. Eur. J. Epidemiol. 2020, 35, 113–122. [Google Scholar] [CrossRef]
- Roche, M.; Rondeau, P.; Singh, N.R.; Tarnus, E.; Bourdon, E. The antioxidant properties of serum albumin. FEBS Lett. 2008, 582, 1783–1787. [Google Scholar] [CrossRef]
- Paar, M.; Rossmann, C.; Nusshold, C.; Wagner, T.; Schlagenhauf, A.; Leschnik, B.; Oettl, K.; Koestenberger, M.; Cvirn, G.; Hallström, S. Anticoagulant action of low, physiologic, and high albumin levels in whole blood. PLoS ONE 2017, 12, e0182997. [Google Scholar] [CrossRef]
- Jiang, Z.; Dai, L.; Song, Z.; Li, H.; Shu, M. Association Between C-Reactive Protein and Atrial Fibrillation Recurrence After Catheter Ablation: A Meta-analysis. Clin. Cardiol. 2013, 36, 548–554. [Google Scholar] [CrossRef]
- Wu, N.; Xu, B.; Xiang, Y.; Wu, L.; Zhang, Y.; Ma, X.; Tong, S.; Shu, M.; Song, Z.; Li, Y.; et al. Association of inflammatory factors with occurrence and recurrence of atrial fibrillation: A meta-analysis. Int. J. Cardiol. 2013, 169, 62–72. [Google Scholar] [CrossRef]
- Harada, M.; Nattel, S. Implications of Inflammation and Fibrosis in Atrial Fibrillation Pathophysiology. Card. Electrophysiol. Clin. 2021, 13, 25–35. [Google Scholar] [CrossRef]
- Nicholson, J.; Wolmarans, M.; Park, G. The role of albumin in critical illness. Br. J. Anaesth. 2000, 85, 599–610. [Google Scholar] [CrossRef]
- Arques, S.; Ambrosi, P. Human Serum Albumin in the Clinical Syndrome of Heart Failure. J. Card. Fail. 2011, 17, 451–458. [Google Scholar] [CrossRef]
- Prenner, S.B.; Kumar, A.; Zhao, L.; Cvijic, M.E.; Basso, M.; Spires, T.; Li, Z.; Yarde, M.; Bhattacharya, P.; Zamani, P.; et al. Effect of Serum Albumin Levels in Patients with Heart Failure With Preserved Ejection Fraction (from the TOPCAT Trial). Am. J. Cardiol. 2020, 125, 575–582. [Google Scholar] [CrossRef]
- Kurtul, A.; Murat, S.N.; Yarlioglues, M.; Duran, M.; Ocek, A.H.; Koseoglu, C.; Celık, I.E.; Kilic, A.; Aksoy, O. Usefulness of Serum Albumin Concentration to Predict High Coronary SYNTAX Score and In-Hospital Mortality in Patients With Acute Coronary Syndrome. Angiology 2016, 67, 34–40. [Google Scholar] [CrossRef]
- Plakht, Y.; Gilutz, H.; Shiyovich, A. Decreased admission serum albumin level is an independent predictor of long-term mortality in hospital survivors of acute myocardial infarction. Soroka Acute Myocardial Infarction II (SAMI-II) project. Int. J. Cardiol. 2016, 219, 20–24. [Google Scholar] [CrossRef]
- Chen, L.Y.; Chung, M.K.; Allen, L.A.; Ezekowitz, M.; Furie, K.L.; McCabe, P.; Noseworthy, P.A.; Perez, M.V.; Turakhia, M.P.; American Heart Association Council on Clinical Cardiology; et al. Atrial Fibrillation Burden: Moving Beyond Atrial Fibrillation as a Binary Entity: A Scientific Statement From the American Heart Association. Circulation 2018, 137, e623–e644. [Google Scholar] [CrossRef]
- Njoku, A.; Kannabhiran, M.; Arora, R.; Reddy, P.; Gopinathannair, R.; Lakkireddy, D.; Dominic, P. Left atrial volume predicts atrial fibrillation recurrence after radiofrequency ablation: A meta-analysis. Europace 2018, 20, 33–42. [Google Scholar] [CrossRef]
- Marrouche, N.F.; Wilber, D.; Hindricks, G.; Jais, P.; Akoum, N.; Marchlinski, F.; Kholmovski, E.; Burgon, N.; Hu, N.; Mont, L.; et al. Association of Atrial Tissue Fibrosis Identified by Delayed Enhancement MRI and Atrial Fibrillation Catheter Ablation. JAMA 2014, 311, 498–506. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Values | Serum Albumin Level (g/dL) | p Value | |||
| <3.8 | 3.8–4.1 | ≥4.1 | Total | |||
| n | 38 | 42 | 46 | 126 | ||
| Demographics | ||||||
| Sex | Male | 21/38 (55.3%) | 29/42 (69.0%) | 34/44 (77.3%) | 84/124 (67.7%) | 0.102 |
| Age, years | n | 38 | 42 | 44 | 124 | |
| Mean (SD) | 60.92 (9.44) | 63.1 (8.90) | 61.43 (11.59) | 61.84 (10.05) | 0.597 | |
| Anthropometrics | ||||||
| Weight, kg | n | 38 | 42 | 46 | 126 | |
| Mean (SD) | 84.83 (17.81) | 84.88 (14.24) | 86.78 (13.81) | 85.56 (15.16) | 0.793 | |
| Height, cm | n | 38 | 42 | 46 | 126 | |
| Mean (SD) | 169.55 (9.21) | 173.55 (8.15) | 170.98 (7.40) | 171.4 (8.32) | 0.091 | |
| BMI, kg/m2 | n | 38 | 42 | 46 | 126 | |
| Mean (SD) | 29.25 (5.58) | 27.94 (3.34) | 29.37 (4.97) | 28.86 (4.71) | 0.304 | |
| Comorbidities | ||||||
| Hypertension | 25/38 (65.8%) | 23/42 (54.8%) | 24/42 (57.1%) | 72/122 (59%) | 0.578 | |
| Diabetes mellitus | 12/38 (31.6%) | 9/42 (21.4%) | 10/46 (21.7%) | 31/126 (24.6%) | 0.490 | |
| Dyslipidemia | 18/38 (47.4%) | 19/42 (45.2%) | 22/46 (47.8%) | 59/126 (46.8%) | 0.968 | |
| Smoker | 4/38 (10.5%) | 4/41 (9.8%) | 5/45 (11.1%) | 13/124 (10.5%) | 0.979 | |
| Coronary artery disease | 9/38 (23.7%) | 9/42 (21.4%) | 10/46 (21.7%) | 28/126 (22.2%) | 0.966 | |
| Variable | Values | Serum Albumin Level (g/dL) | p Value | |||
| <3.8 | 3.8–4.1 | ≥4.1 | Total | |||
| n | 38 | 42 | 46 | 126 | ||
| AF characteristics | ||||||
| AF duration, years | n | 34 | 34 | 35 | 103 | |
| Mean (SD) | 2.81 (1.99) | 7.34 (6.76) | 6.37 (6.72) | 5.52 (5.91) | 0.003 | |
| Type of AF | Paroxysmal | 29/38 (76.3%) | 28/42 (66.7%) | 30/46 (65.2%) | 87/126 (69.0%) | 0.196 |
| Persistent | 5/38 (15.8%) | 11/42 (26.2%) | 15/46 (32.6%) | 32/126 (25.4%) | ||
| Longstanding persistent | 4/38 (10.5%) | 3/42 (7.1%) | 1/46 (2.2%) | 8/126 (6.3%) | ||
| Number of previous cardioversions | Range | 0–8 | 0–5 | 0–4 | 0–8 | |
| Median (IQR) | 0 (0–2) | 1 (0–1) | 0 (0–0) | 0 (0–1) | 0.022 | |
| 0 | 19/35 (54.3%) | 16/35 (45.7%) | 28/35 (80%) | 63/105 (60%) | 0.002 | |
| 1 | 4/35 (11.4%) | 13/35 (37.1%) | 3/35 (8.6%) | 20/105 (19.0%) | ||
| ≥2 | 12/35 (34.3%) | 6/35 (17.1%) | 4/35 (11.4%) | 22/105 (21.0%) | ||
| NYHA | Range | 0–2 | 0–3 | 0–3 | 0–3 | |
| Median (IQR) | 1 (0–1) | 1 (0–1) | 1 (0.5–1) | 1 (0–1) | 0.576 | |
| 0 | 12/34 (35.3%) | 9/35 (25.7%) | 9/37 (24.3%) | 30/106 (28.3%) | 0.501 | |
| 1 | 18/34 (52.9%) | 21/35 (60.0%) | 23/37 (62.2%) | 62/106 (58.5%) | ||
| 2 | 4/34 (11.8%) | 4/35 (11.4%) | 2/37 (5.4%) | 10/106 (9.4%) | ||
| 3 | 0/34 (0%) | 1/35 (2.9%) | 3/37 (8.1%) | 4/106 (3.8%) | ||
| Canadian Cardiovascular Society (CCS) Severity of Atrial Fibrillation (SAF) scale | Range | 1–4 | 1–4 | 0–4 | 0–4 | |
| Median (IQR) | 3 (2–3) | 3 (2–3) | 2 (1–3) | 3 (2–3) | 0.061 | |
| 0 | 0/34 (0%) | 0/39 (0%) | 1/37 (2.2%) | 1/110 (0.8%) | 0.433 | |
| 1 | 2/34 (5.3%) | 6/39 (14.3%) | 9/37 (19.6%) | 17/110 (13.5%) | ||
| 2 | 11/34 (28.9%) | 13/39 (31%) | 12/37 (26.1%) | 36/110 (28.6%) | ||
| 3 | 18/34 (47.4%) | 18/39 (42.9%) | 14/37 (30.4%) | 50/110 (39.7%) | ||
| 4 | 3/34 (7.9%) | 2/39 (4.8%) | 1/37 (2.2%) | 6/110 (4.8%) | ||
| Previous atrial flutter | 7/38 (18.4%) | 8/42 (19.0%) | 17/46 (37.0%) | 32/126 (25.4%) | 0.078 | |
| Previous CTI ablations | 8/38 (21.1%) | 6/42 (14.3%) | 12/46 (26.1%) | 26/126 (20.6%) | 0.392 | |
| CHADS score | Range | 0–4 | 0–5 | 0–4 | 0–5 | |
| Median (IQR) | 1.5 (0–2) | 1 (0–2) | 1 (0 to –2) | 1 (0–2) | 0.458 | |
| 0 | 10/38 (26.3%) | 16/42 (38.1%) | 14/45 (31.1%) | 40/125 (32.0%) | 0.758 | |
| 1 | 9/38 (23.7%) | 11/42 (26.2%) | 14/45 (31.1%) | 34/125 (27.2%) | ||
| 2 | 14/38 (36.8%) | 10/42 (23.8%) | 13/45 (28.9%) | 37/125 (29.6%) | ||
| 3 | 4/38 (10.5%) | 2/42 (4.8%) | 3/45 (6.7%) | 9/125 (7.2%) | ||
| ≥4 | 1/38 (2.6%) | 3/42 (7.1%) | 1/45 (2.2%) | 5/125 (4.0%) | ||
| CHA₂DS₂-VASc Score | Range | 0–6 | 0–7 | 0–5 | 0–7 | |
| Median (IQR) | 2 (0.8–3.3) | 2 (0–3) | 2 (0.5–3) | 2 (0–3) | 0.965 | |
| 0 | 9/38 (23.7%) | 14/42 (33.3%) | 11/45 (24.4%) | 34/125 (27.2%) | 0.524 | |
| 1 | 7/38 (18.4%) | 4/42 (9.5%) | 10/45 (22.2%) | 21/125 (16.8%) | ||
| 2 | 9/38 (23.7%) | 7/42 (16.7%) | 6/45 (13.3%) | 22/125 (17.6%) | ||
| 3 | 4/38 (10.5%) | 10/42 (23.8%) | 10/45 (22.2%) | 24/125 (19.2%) | ||
| 4 | 6/38 (15.8%) | 2/42 (4.8%) | 5/45 (11.1%) | 13/125 (10.4%) | ||
| 5 | 2/38 (5.3%) | 3/42 (7.1%) | 3/45 (6.7%) | 8/125 (6.4%) | ||
| ≥6 | 1/38 (2.6%) | 2/42 (4.8%) | 0/45 (0%) | 3/125 (2.4%) | ||
| Variable | Values | Serum Albumin Level (g/dL) | p Value | |||
| <3.8 | 3.8–4.1 | ≥4.1 | Total | |||
| n | 38 | 42 | 46 | 126 | ||
| Treatment | ||||||
| Number of antiarrhythmic drugs | Range | 0–5 | 0–4 | 0–5 | 0–5 | |
| Median (IQR) | 1 (1–2) | 1 (1–2) | 1 (1–3) | 1 (1–2) | 0.414 | |
| 0 | 6/38 (15.8%) | 1/42 (2.4%) | 2/46 (4.3%) | 9/126 (7.1%) | 0.171 | |
| 1 | 17/38 (44.7%) | 23/42 (54.8%) | 23/46 (50.0%) | 63/126 (50.0%) | ||
| ≥2 | 15/38 (39.5%) | 18/42 (42.9%) | 21/46 (45.7%) | 54/126 (42.9%) | ||
| Amiodarone | 18/38 (47.4%) | 22/42 (52.4%) | 23/46 (50.0%) | 63/126 (50.0%) | 0.905 | |
| Propafenone | 17/38 (44.7%) | 22/42 (52.4%) | 26/46 (56.5%) | 65/126 (51.6%) | 0.556 | |
| Flecanide | 9/38 (23.7%) | 12/42 (28.6%) | 19/46 (41.3%) | 40/126 (31.7%) | 0.194 | |
| Dronaderone | 5/38 (13.2%) | 4/42 (9.5%) | 7/46 (15.2%) | 16/126 (12.7%) | 0.722 | |
| Sotalol | 11/38 (28.9%) | 10/42 (23.8%) | 7/46 (15.2%) | 28/126 (22.2%) | 0.307 | |
| Aspirin | 9/38 (23.7%) | 11/42 (26.2%) | 11/46 (23.9%) | 31/126 (24.6%) | 0.958 | |
| Warfarin | 11/38 (28.9%) | 8/42 (19%) | 15/46 (32.6%) | 34/126 (27.0%) | 0.340 | |
| Dabigatran | 4/38 (10.5%) | 9/42 (21.4%) | 3/46 (6.5%) | 16/126 (12.7%) | 0.099 | |
| Apixaban | 10/38 (26.3%) | 8/42 (19.0%) | 11/46 (23.9%) | 29/126 (23.0%) | 0.731 | |
| Xarelto | 11/38 (28.9%) | 14/42 (33.3%) | 9/46 (19.6%) | 34/126 (27.0%) | 0.330 | |
| ACE inhibitors | 19/38 (50.0%) | 10/42 (23.8%) | 17/46 (37%) | 46/126 (36.5%) | 0.052 | |
| ARBs | 6/38 (15.8%) | 9/42 (21.4%) | 3/46 (6.5%) | 18/126 (14.3%) | 0.130 | |
| Beta blockers | 30/38 (78.9%) | 30/42 (71.4%) | 39/46 (84.8%) | 99/126 (78.6%) | 0.312 | |
| Calcium Channel Blockers | 5/38 (13.2%) | 7/42 (16.7%) | 5/46 (10.9%) | 17/126 (13.5%) | 0.727 | |
| Digoxin | 2/38 (5.3%) | 1/42 (2.4%) | 4/46 (8.7%) | 7/126 (5.6%) | 0.432 | |
| Echocardiogram measurements | ||||||
| Left ventricular function | Good (>55%) | 24/35 (68.6%) | 21/35 (60.0%) | 20/34 (58.8%) | 65/104 (62.5%) | 0.922 |
| Preserved (50–55%) | 7/35 (20.0%) | 11/35 (31.4%) | 10/34 (29.4%) | 28/104 (26.9%) | ||
| Mild (41–49%) | 1/35 (2.9%) | 0/35 (0%) | 1/34 (2.9%) | 2/104 (1.9%) | ||
| Moderate (30–40%) | 2/35 (5.7%) | 1/35 (2.9%) | 2/34 (5.9%) | 5/104 (4.8%) | ||
| Severe (<30%) | 1/35 (2.9%) | 2/35 (5.7%) | 1/34 (2.9%) | 4/104 (3.8%) | ||
| Left atrial diameter (mm) | n | 29 | 30 | 28 | 87 | |
| Mean (SD) | 43.9 (5.79) | 40.6 (6.79) | 41.64 (3.66) | 42.03 (5.71) | 0.076 | |
| Left atrial area (cm2) | n | 29 | 28 | 31 | 88 | |
| Mean (SD) | 24.97 (4.84) | 22.79 (5.09) | 21.55 (4.46) | 23.07 (4.95) | 0.024 | |
| Systolic pulmonary artery pressure (mmHg) | n | 24 | 22 | 24 | 70 | |
| Mean (SD) | 27.96 (8.53) | 25.77 (10.05) | 28.13 (7.59) | 27.33 (8.68) | 0.602 | |
| Left atrial volume (mL/m2) | n | 33 | 34 | 35 | 102 | |
| Mean (SD) | 136.24 (42.56) | 119.76 (34.96) | 105.54 (27.73) | 120.22 (37.29) | 0.002 | |
| Variable | Values | Serum Albumin Level (g/dL) | p Value | |||
| <3.8 | 3.8–4.1 | ≥4.1 | Total | |||
| n | 38 | 42 | 46 | 126 | ||
| AF (during a 3-month window) | 9/37 (24.3%) | 5/41 (12.2%) | 2/42 (4.8%) | 16/120 (13.3%) | 0.037 | |
| Canadian Cardiovascular Society (CCS) Severity of Atrial Fibrillation (SAF) scale | Range | 0–3 | 0–3 | 0–2 | 0–3 | |
| Median (IQR) | 0 (0–1) | 0 (0–1) | 0 (0–1) | 1 (0–1) | 0.897 | |
| 0 | 21/34 (61.8%) | 21/40 (52.5%) | 21/41 (51.2%) | 63/115 (54.8%) | 0.317 | |
| 1 | 8/34 (23.5%) | 16/40 (40%) | 19/41 (46.3%) | 43/115 (37.4%) | ||
| 2 | 4/34 (11.8%) | 2/40 (5.0%) | 1/41 (2.4%) | 7/115 (6.1%) | ||
| 3 | 1/34 (2.9%) | 1/40 (2.5%) | 0/41 (0%) | 2/115 (1.7%) | ||
| 4 | 0/34 (0%) | 0/40 (0%) | 0/41 (0%) | 0/115 (0%) | ||
| Number of hospitalizations | Range | 0–6 | 0–2 | 0–7 | 0–7 | |
| Median (IQR) | 0 (0–1) | 0 (0–0) | 0 (0–0) | 0 (0–0) | 0.103 | |
| ≥1 | 10/29 (34.5%) | 5/38 (13.2%) | 8/39 (20.5%) | 23/106 (21.7%) | 0.108 | |
| NYHA | Range | 0–3 | 0–2 | 0–3 | 0–3 | |
| Median (IQR) | 1 (0–1) | 1 (0–1) | 1 (0–1) | 1 (0–1) | 0.625 | |
| 0 | 15/35 (42.9%) | 12/40 (30.0%) | 16/42 (38.1%) | 43/117 (36.8%) | 0.465 | |
| 1 | 18/35 (51.4%) | 26/40 (65.0%) | 23/42 (54.8%) | 67/117 (57.3%) | ||
| 2 | 0/35 (0%) | 2/40 (5.0%) | 2/42 (4.8%) | 4/117 (3.4%) | ||
| 3 | 2/35 (5.7%) | 0/40 (0%) | 1/42 (2.4%) | 3/117 (2.6%) | ||
| Treatment | ||||||
| Antiarrhythmic drug use | 17/30 (56.7%) | 19/35 (54.3%) | 22/37 (59.5%) | 58/102 (56.9%) | 0.906 | |
| Amiodarone | 8/38 (21.1%) | 6/42 (14.3%) | 8/46 (17.4%) | 22/126 (17.5%) | 0.728 | |
| Propafenone/flecainide | 6/38 (15.8%) | 5/42 (11.9%) | 9/46 (19.6%) | 20/126 (15.9%) | 0.617 | |
| Dronaderone | 0/38 (0%) | 0/42 (0%) | 1/46 (2.2%) | 1/126 (0.8%) | 0.416 | |
| Sotalol | 2/38 (5.3%) | 2/42 (4.8%) | 1/46 (2.2%) | 5/126 (4.0%) | 0.732 | |
| Hydroquinidine | 1/37 (2.7%) | 0/42 (0%) | 0/46 (0%) | 1/125 (0.8%) | 0.302 | |
| Parameter | Value | Univariate | Multivariate | ||||||
|---|---|---|---|---|---|---|---|---|---|
| B (SE) | OR | (95% CI) | p | B (SE) | AdjOR | (95% CI) | p | ||
| Serum albumin level (g/dL) | <3.8 vs. ≥3.8 | 2.197 (0.493) | 9.000 | (3.424; 23.653) | <0.001 | 1.960 (0.877) | 7.101 | (1.274; 39.575) | 0.025 |
| Left atrial diameter (mm) | 1 mm increase | 0.173 (0.053) | 1.189 | (1.071; 1.320) | 0.001 | 0.198 (0.081) | 1.219 | (1.041; 1.429) | 0.014 |
| Previous cardioversion | Yes vs. no | 0.678 (0.187) | 1.971 | (1.366; 2.843) | <0.001 | 0.774 (0.336) | 2.168 | (1.121; 4.191) | 0.021 |
| Type of baseline AF | Persistent/long persistent vs. paroxysmal | 1.046 (0.454) | 2.849 | (1.170; 6.944) | 0.021 | 1.181 (0.965) | 3.257 | (0.492; 21.739) | 0.221 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schamroth Pravda, N.; Golovchiner, G.; Goldenberg, G.; Plakht, Y.; Wiessman, M.; Tal, S.; Barsheshet, A.; Kadmon, E.; Erez, A.; Skalsky, K.; et al. Albumin as a Prognostic Marker for Atrial Fibrillation Recurrence following Cryoballoon Ablation of Pulmonary Venous. J. Clin. Med. 2023, 12, 264. https://doi.org/10.3390/jcm12010264
Schamroth Pravda N, Golovchiner G, Goldenberg G, Plakht Y, Wiessman M, Tal S, Barsheshet A, Kadmon E, Erez A, Skalsky K, et al. Albumin as a Prognostic Marker for Atrial Fibrillation Recurrence following Cryoballoon Ablation of Pulmonary Venous. Journal of Clinical Medicine. 2023; 12(1):264. https://doi.org/10.3390/jcm12010264
Chicago/Turabian StyleSchamroth Pravda, Nili, Gregory Golovchiner, Gustavo Goldenberg, Ygal Plakht, Maya Wiessman, Shir Tal, Alon Barsheshet, Ehud Kadmon, Aharon Erez, Keren Skalsky, and et al. 2023. "Albumin as a Prognostic Marker for Atrial Fibrillation Recurrence following Cryoballoon Ablation of Pulmonary Venous" Journal of Clinical Medicine 12, no. 1: 264. https://doi.org/10.3390/jcm12010264
APA StyleSchamroth Pravda, N., Golovchiner, G., Goldenberg, G., Plakht, Y., Wiessman, M., Tal, S., Barsheshet, A., Kadmon, E., Erez, A., Skalsky, K., Grinberg, T., Nardi Agmon, I., Aviv, Y., Kornowski, R., Shiyovich, A., & Hamdan, A. (2023). Albumin as a Prognostic Marker for Atrial Fibrillation Recurrence following Cryoballoon Ablation of Pulmonary Venous. Journal of Clinical Medicine, 12(1), 264. https://doi.org/10.3390/jcm12010264