
The Neutrophil-to-Lymphocyte Ratio and Preoperative Pulmonary Function Test Results as Predictors of In-Hospital Postoperative Complications after Hip Fracture Surgery in Older Adults †


Abstract
1. Introduction
2. Materials and Methods
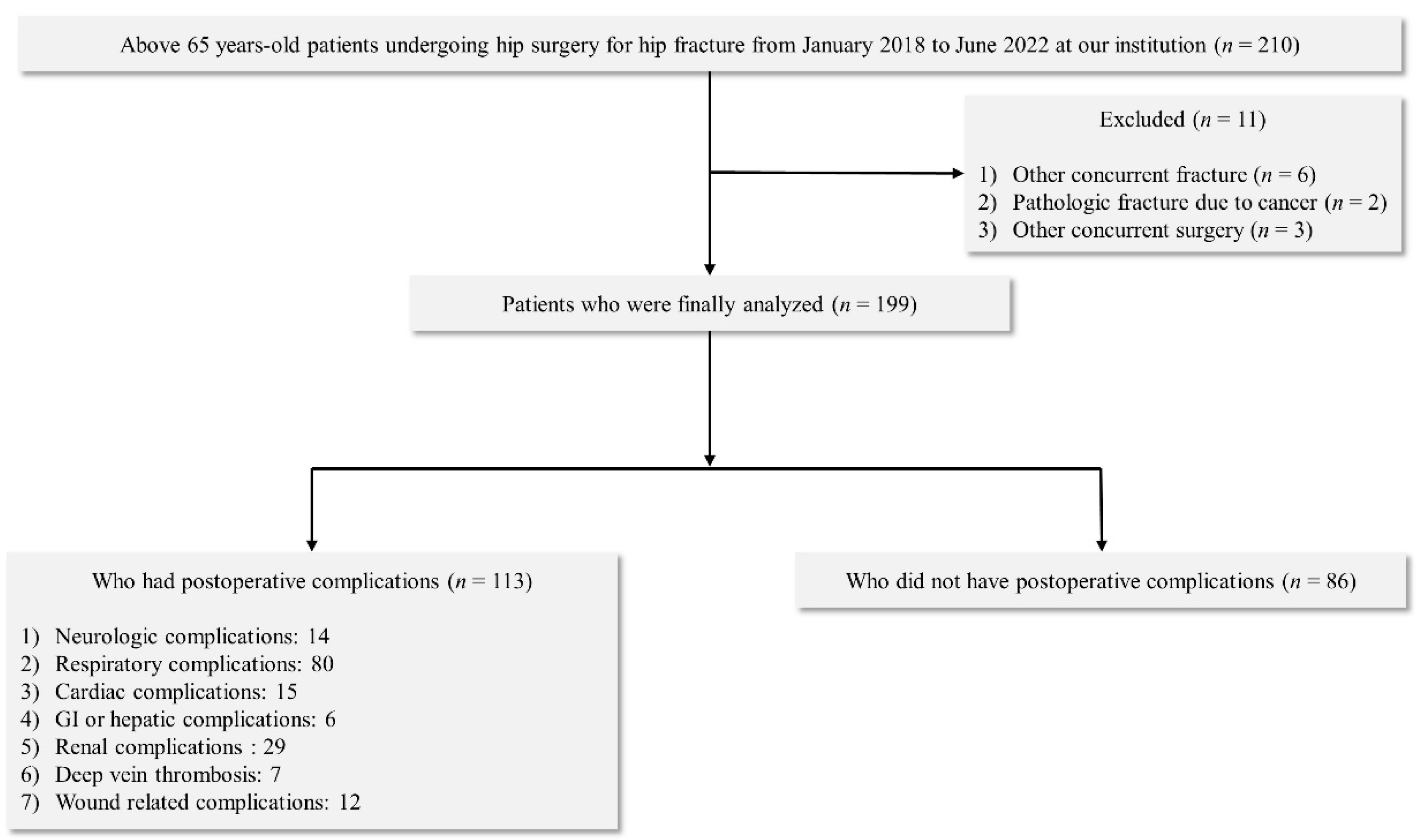
2.1. Study Population
2.2. NLR
2.3. PNI
2.4. Preoperative PFT
2.5. Anaesthesia Technique and Intra- and Postoperative Management
2.6. In-Hospital Postoperative Complications
2.7. Statistical Analyses
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kang, H.Y.; Yang, K.H.; Kim, Y.N.; Moon, S.H.; Choi, W.J.; Kang, D.R.; Park, S.E. Incidence and mortality of hip fracture among the elderly population in South Korea: A population-based study using the national health insurance claims data. BMC Public Health 2010, 10, 230. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.H.; Chou, C.H.; Su, H.H.; Tsai, Y.T.; Chiang, M.H.; Kuo, Y.J.; Chen, Y.P. Correlation between neutrophil-to-lymphocyte ratio and postoperative mortality in elderly patients with hip fracture: A meta-analysis. J. Orthop. Surg. Res. 2021, 16, 681. [Google Scholar] [CrossRef] [PubMed]
- Forget, P.; Dillien, P.; Engel, H.; Cornu, O.; De Kock, M.; Yombi, J.C. Use of the neutrophil-to-lymphocyte ratio as a component of a score to predict postoperative mortality after surgery for hip fracture in elderly subjects. BMC Res. Notes 2016, 9, 284. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Gao, C.; Xin, H.; Li, J.; Li, B.; Wei, Z.; Yue, Y. The application of “upper-body yoga” in elderly patients with acute hip fracture: A prospective, randomized, and single-blind study. J. Orthop. Surg. Res. 2019, 14, 250. [Google Scholar] [CrossRef]
- Zahorec, R. Neutrophil-to-lymphocyte ratio, past, present and future perspectives. Bratisl. Lek. Listy 2021, 122, 474–488. [Google Scholar] [CrossRef]
- Onodera, T.; Goseki, N.; Kosaki, G. Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients. Nihon Geka Gakkai Zasshi 1984, 85, 1001–1005. [Google Scholar]
- Zahorec, R. Ratio of neutrophil to lymphocyte counts--rapid and simple parameter of systemic inflammation and stress in critically ill. Bratisl. Lek. Listy 2001, 102, 5–14. [Google Scholar]
- Plas, M.; Rutgers, A.; van der Wal-Huisman, H.; de Haan, J.J.; Absalom, A.R.; de Bock, G.H.; van Leeuwen, B.L. The association between the inflammatory response to surgery and postoperative complications in older patients with cancer; a prospective prognostic factor study. J. Geriatr. Oncol. 2020, 11, 873–879. [Google Scholar] [CrossRef]
- Alazawi, W.; Pirmadjid, N.; Lahiri, R.; Bhattacharya, S. Inflammatory and Immune Responses to Surgery and Their Clinical Impact. Ann. Surg. 2016, 264, 73–80. [Google Scholar] [CrossRef]
- Kaufmann, K.B.; Heinrich, S.; Staehle, H.F.; Bogatyreva, L.; Buerkle, H.; Goebel, U. Perioperative cytokine profile during lung surgery predicts patients at risk for postoperative complications-A prospective, clinical study. PLoS One 2018, 13, e0199807. [Google Scholar] [CrossRef]
- Chen, X.X.; Wang, T.; Li, J.; Kang, H. Relationship between Inflammatory Response and Estimated Complication Rate after Total Hip Arthroplasty. Chin. Med. J. 2016, 129, 2546–2551. [Google Scholar] [CrossRef] [PubMed]
- Buzby, G.P.; Mullen, J.L.; Matthews, D.C.; Hobbs, C.L.; Rosato, E.F. Prognostic nutritional index in gastrointestinal surgery. Am. J. Surg. 1980, 139, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.; Cao, S.; Geng, J.; Wang, C.; Meng, Q.; Yu, Y. High prognostic nutritional index (PNI) as a positive prognostic indicator for non-small cell lung cancer patients with bone metastasis. Clin. Respir. J. 2021, 15, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Lv, X.; Zhang, Z.; Yuan, W. Pretreatment Prognostic Nutritional Index (PNI) as a Prognostic Factor in Patients with Biliary Tract Cancer: A Meta-Analysis. Nutr. Cancer 2021, 73, 1872–1881. [Google Scholar] [CrossRef]
- Li, B.; Lu, Z.; Wang, S.; Hou, J.; Xia, G.; Li, H.; Yin, B.; Lu, W. Pretreatment elevated prognostic nutritional index predicts a favorable prognosis in patients with prostate cancer. BMC Cancer 2020, 20, 361. [Google Scholar] [CrossRef]
- Ren, H.; Wu, L.; Hu, W.; Ye, X.; Yu, B. Prognostic value of the c-reactive protein/prognostic nutritional index ratio after hip fracture surgery in the elderly population. Oncotarget 2017, 8, 61365–61372. [Google Scholar] [CrossRef]
- Feng, L.; Chen, W.; Ping, P.; Ma, T.; Li, Y.; Xu, L.; Feng, Z.; Zhao, Y.; Fu, S. Preoperative malnutrition as an independent risk factor for the postoperative mortality in elderly Chinese individuals undergoing hip surgery: A single-center observational study. Ther. Adv. Chronic Dis. 2022, 13, 20406223221102739. [Google Scholar] [CrossRef]
- Goisser, S.; Schrader, E.; Singler, K.; Bertsch, T.; Gefeller, O.; Biber, R.; Bail, H.J.; Sieber, C.C.; Volkert, D. Malnutrition According to Mini Nutritional Assessment Is Associated With Severe Functional Impairment in Geriatric Patients Before and up to 6 Months After Hip Fracture. J. Am. Med. Dir. Assoc. 2015, 16, 661–667. [Google Scholar] [CrossRef]
- Miyanishi, K.; Jingushi, S.; Torisu, T. Mortality after hip fracture in Japan: The role of nutritional status. J. Orthop. Surg. 2010, 18, 265–270. [Google Scholar] [CrossRef]
- Malafarina, V.; Reginster, J.Y.; Cabrerizo, S.; Bruyere, O.; Kanis, J.A.; Martinez, J.A.; Zulet, M.A. Nutritional Status and Nutritional Treatment Are Related to Outcomes and Mortality in Older Adults with Hip Fracture. Nutrients 2018, 10, 555. [Google Scholar] [CrossRef]
- Moradian, S.T.; Najafloo, M.; Mahmoudi, H.; Ghiasi, M.S. Early mobilization reduces the atelectasis and pleural effusion in patients undergoing coronary artery bypass graft surgery: A randomized clinical trial. J. Vasc. Nurs. 2017, 35, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Wang, X.; Qian, H.; Ye, J.; Qian, J.; Hua, J. Correlation between common postoperative complications of prolonged bed rest and quality of life in hospitalized elderly hip fracture patients. Ann. Palliat. Med. 2020, 9, 1125–1133. [Google Scholar] [CrossRef] [PubMed]
- Yagi, T.; Oshita, Y.; Okano, I.; Kuroda, T.; Ishikawa, K.; Nagai, T.; Inagaki, K. Controlling nutritional status score predicts postoperative complications after hip fracture surgery. BMC Geriatr. 2020, 20, 243. [Google Scholar] [CrossRef] [PubMed]
- Dong, C.H.; Wang, Z.M.; Zhao, X.L.; Wang, A.M. The use of damage control orthopaedics to minimize negative sequelae of surgery delay in elderly comorbid patients with hip fracture. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 2505–2514. [Google Scholar]
- De Cassai, A.; Boscolo, A.; Tonetti, T.; Ban, I.; Ori, C. Assignment of ASA-physical status relates to anesthesiologists’ experience: A survey-based national-study. Korean J. Anesthesiol. 2019, 72, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Kim, J.W.; Nam, K.H.; Han, S.H.; Kim, J.W.; Ahn, S.H.; Park, D.J.; Lee, K.W.; Lee, H.S.; Kim, H.H. Systemic inflammation is associated with the density of immune cells in the tumor microenvironment of gastric cancer. Gastric Cancer 2017, 20, 602–611. [Google Scholar] [CrossRef]
- Nerpin, E.; Jacinto, T.; Fonseca, J.A.; Alving, K.; Janson, C.; Malinovschi, A. Systemic inflammatory markers in relation to lung function in NHANES. 2007-2010. Respir. Med. 2018, 142, 94–100. [Google Scholar] [CrossRef]
- Suarez-Cuenca, J.A.; Ruiz-Hernandez, A.S.; Mendoza-Castaneda, A.A.; Dominguez-Perez, G.A.; Hernandez-Patricio, A.; Vera-Gomez, E.; De la Pena-Sosa, G.; Banderas-Lares, D.Z.; Montoya-Ramirez, J.; Blas-Azotla, R.; et al. Neutrophil-to-lymphocyte ratio and its relation with pro-inflammatory mediators, visceral adiposity and carotid intima-media thickness in population with obesity. Eur. J. Clin. Investig. 2019, 49, e13085. [Google Scholar] [CrossRef]
- Chen, Z.Y.; Raghav, K.; Lieu, C.H.; Jiang, Z.Q.; Eng, C.; Vauthey, J.N.; Chang, G.J.; Qiao, W.; Morris, J.; Hong, D.; et al. Cytokine profile and prognostic significance of high neutrophil-lymphocyte ratio in colorectal cancer. Br. J. Cancer 2015, 112, 1088–1097. [Google Scholar] [CrossRef]
- Park, J.W.; Chang, H.J.; Yeo, H.Y.; Han, N.; Kim, B.C.; Kong, S.Y.; Kim, J.; Oh, J.H. The relationships between systemic cytokine profiles and inflammatory markers in colorectal cancer and the prognostic significance of these parameters. Br. J. Cancer 2020, 123, 610–618. [Google Scholar] [CrossRef]
- Mantovani, A.; Cassatella, M.A.; Costantini, C.; Jaillon, S. Neutrophils in the activation and regulation of innate and adaptive immunity. Nat. Rev. Immunol. 2011, 11, 519–531. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S.D.; DeLeo, F.R. Role of neutrophils in innate immunity: A systems biology-level approach. Wiley Interdiscip. Rev. Syst. Biol. Med. 2009, 1, 309–333. [Google Scholar] [CrossRef] [PubMed]
- Vats, R.; Kaminski, T.W.; Brzoska, T.; Leech, J.A.; Tutuncuoglu, E.; Katoch, O.; Jonassaint, J.; Tejero, J.; Novelli, E.M.; Pradhan-Sundd, T.; et al. Liver-to-lung microembolic NETs promote gasdermin D-dependent inflammatory lung injury in sickle cell disease. Blood 2022, 140, 1020–1037. [Google Scholar] [CrossRef] [PubMed]
- Scozzi, D.; Liao, F.; Krupnick, A.S.; Kreisel, D.; Gelman, A.E. The role of neutrophil extracellular traps in acute lung injury. Front. Immunol. 2022, 13, 953195. [Google Scholar] [CrossRef] [PubMed]
- Muller-Redetzky, H. Targeting neutrophil extracellular traps in acute lung injury: A novel therapeutic approach in acute respiratory distress syndrome? Anesthesiology 2015, 122, 725–727. [Google Scholar] [CrossRef]
- Basilico, M.; Vitiello, R.; Oliva, M.S.; Covino, M.; Greco, T.; Cianni, L.; Dughiero, G.; Ziranu, A.; Perisano, C.; Maccauro, G. Predictable risk factors for infections in proximal femur fractures. J. Biol. Regul. Homeost Agents 2020, 34, 77–81, Advances in Musculoskeletal Diseases and Infections—SOTIMI 2019. [Google Scholar]
- Vitiello, R.; Perisano, C.; Covino, M.; Perna, A.; Bianchi, A.; Oliva, M.S.; Greco, T.; Sirgiovanni, M.; Maccauro, G. Euthyroid sick syndrome in hip fractures: Valuation of vitamin D and parathyroid hormone axis. Injury 2020, 51 (Suppl. 3), S13–S16. [Google Scholar] [CrossRef]
- Cauteruccio, M.; Vitiello, R.; Perisano, C.; Covino, M.; Sircana, G.; Piccirillo, N.; Pesare, E.; Antonio, Z.; Maccauro, G. Euthyroid sick syndrome in hip fractures: Evaluation of postoperative anemia. Injury 2020, 51 (Suppl. 3), S9–S12. [Google Scholar] [CrossRef]
- Baines, K.J.; Backer, V.; Gibson, P.G.; Powel, H.; Porsbjerg, C.M. Impaired lung function is associated with systemic inflammation and macrophage activation. Eur. Respir. J. 2015, 45, 557–559. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Complications | Number of Patients | |
|---|---|---|
| Neurologic | ||
| Delirium | 13 | |
| Cerebral infarction | 1 | |
| Respiratory | ||
| Atelectasis | 21 | |
| Pneumonia | 17 | |
| Pleural effusion | 32 | |
| Pulmonary thromboembolism | 10 | |
| Cardiac | ||
| Hemodynamic instability | 3 | |
| Arrythmia | 12 | |
| GI or hepatic | ||
| Hepatic enzyme elevation | 6 | |
| Renal | ||
| Acute kidney injury | 12 | |
| Urinary tract infection | 17 | |
| Deep vein thrombosis | 7 | |
| Wound related | 12 |
| With Cxs (n = 113) | Without Cxs (n = 86) | p-Value | ||
|---|---|---|---|---|
| Gender (M/F) | 39/74 | 30/56 | 0.772 | |
| Age (years) | 82.3 ± 7.9 | 79.4 ± 7.2 | 0.020 | |
| Height (cm) | 156.1 ± 6.4 | 156.9 ± 7.3 | 0.193 | |
| Weight (kg) | 54.2 ± 11.9 | 56.2 ± 10.4 | 0.161 | |
| Underlying dz | ||||
| HTN | 89 | 70 | 0.646 | |
| DM | 41 | 32 | 0.893 | |
| CVA history | 31 | 27 | 0.632 | |
| Pulmonary dz | 43 | 29 | 0.193 | |
| Cardiovascular dz | 37 | 33 | 0.584 | |
| Renal dz | 16 | 12 | 0.581 | |
| Medication | ||||
| ACEi or ARB | 56 | 34 | 0.159 | |
| β-blocker | 15 | 7 | 0.252 | |
| CCB | 49 | 34 | 0.466 | |
| Diuretics | 18 | 8 | 0.169 | |
| Hypoglycemic | 33 | 27 | 0.611 | |
| Antiplatelet | 40 | 27 | 0.544 | |
| ASA PS | 0.027 | |||
| I | 0 | 0 | ||
| II | 54 | 48 | ||
| III | 59 | 38 | ||
| Hospital stay (days) | 37.3 ± 26.2 | 15.1 ± 3.4 | <0.001 |
| With Cxs (n = 113) | Without Cxs (n = 86) | p-Value | ||
|---|---|---|---|---|
| Laboratory findings | ||||
| NLR | 8.01 ± 4.70 | 5.12 ± 4.34 | <0.001 | |
| PNI | 38.33 ± 6.8 | 42.67 ± 6.47 | <0.001 | |
| PFT | ||||
| FVC (L) | 2.04 ± 0.76 | 2.45 ± 0.71 | <0.001 | |
| FEV1 (L) | 1.43 ± 0.53 | 1.78 ± 0.58 | <0.001 | |
| FEV1/FVC | 70.43 ± 11.76 | 72.03 ± 8.69 | 0.290 |
| Variables | Univariate | Multivariable | |||
|---|---|---|---|---|---|
| Odd Ratio (95% CI) | p-Value | Odd Ratio (95% CI) | p-Value | ||
| Gender (M/F) | 1.092 (0.602–1.979) | 0.773 | |||
| Age (years) | 1.046 (1.007–1.088) | 0.022 | |||
| Height (cm) | 0.963 (0.915–1.016) | 0.186 | |||
| Weight (kg) | 1.019 (0.993–1.047) | 0.156 | |||
| Underlying dz | |||||
| HTN | 0.848 (0.418–1.717) | 0.646 | |||
| DM | 0.961 (0.537–1.779) | 0.893 | |||
| CVA history | 1.170 (0.615–2.225) | 0.632 | |||
| Pulmonary dz | 0.642 (0.392–1.134) | 0.164 | |||
| Cardiovascular dz | 0.649 (0.427–1.184) | 0.187 | |||
| Renal disease | 0.802 (0.366–1.758) | 0.582 | |||
| Medication | |||||
| ACEi or ARB | 0.665 (0.377–1.173) | 0.624 | |||
| β-blocker | 0.548 (0.233–1.314) | 0.243 | |||
| CCB | 0.599 (0.254–1.547) | 0.221 | |||
| Diuretic | 0.574 (0.232–1.394) | 0.433 | |||
| Hypoglycemic agent | 1.089 (0.718–2.264) | 0.731 | |||
| Antiplatelet agents | 0.541 (0.232–1.243) | 0.304 | |||
| ASA PS | 2.113 (1.093–3.957) | 0.025 | |||
| Laboratory findings | |||||
| NLR | 1.159 (1.073–1.252) | <0.001 | 1.142 (1.060–1.230) | <0.001 | |
| PNI | 0.947 (0.906–0.990) | 0.001 | |||
| PFT | |||||
| FVC (L) | 0.476 (0.320–0.707) | <0.001 | |||
| FEV1 (L) | 0.328 (0.190–0.566) | <0.001 | 0.340 (0.191–0.603) | <0.001 | |
| FEV1/FVC | 0.985 (0.958–1.013) | 0.292 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hong, S.-W.; Jeong, H.-C.; Kim, S.-H. The Neutrophil-to-Lymphocyte Ratio and Preoperative Pulmonary Function Test Results as Predictors of In-Hospital Postoperative Complications after Hip Fracture Surgery in Older Adults. J. Clin. Med. 2023, 12, 108. https://doi.org/10.3390/jcm12010108
Hong S-W, Jeong H-C, Kim S-H. The Neutrophil-to-Lymphocyte Ratio and Preoperative Pulmonary Function Test Results as Predictors of In-Hospital Postoperative Complications after Hip Fracture Surgery in Older Adults. Journal of Clinical Medicine. 2023; 12(1):108. https://doi.org/10.3390/jcm12010108
Chicago/Turabian StyleHong, Seung-Wan, Hae-Chang Jeong, and Seong-Hyop Kim. 2023. "The Neutrophil-to-Lymphocyte Ratio and Preoperative Pulmonary Function Test Results as Predictors of In-Hospital Postoperative Complications after Hip Fracture Surgery in Older Adults" Journal of Clinical Medicine 12, no. 1: 108. https://doi.org/10.3390/jcm12010108
APA StyleHong, S.-W., Jeong, H.-C., & Kim, S.-H. (2023). The Neutrophil-to-Lymphocyte Ratio and Preoperative Pulmonary Function Test Results as Predictors of In-Hospital Postoperative Complications after Hip Fracture Surgery in Older Adults. Journal of Clinical Medicine, 12(1), 108. https://doi.org/10.3390/jcm12010108