
The Accuracy of Jaws Repositioning in Bimaxillary Orthognathic Surgery in Patients with Cleft Lip and Palate Compared to Non-Syndromic Skeletal Class III Patients



 and
and 
Abstract
:1. Introduction
2. Materials and Method
- Group A included 16 adult patients with cleft lip and palate (12 males, 4 females, mean age 20.4 years, SD 2.6);
- Group B consisted of 16 patients with a non-syndromic skeletal class III (4 males, 12 females, mean age 24.6 years, SD 5.14).
- Skeletal class III (with ANB ≤ 0 and/or Wits appraisal ≤ −2 mm);
- Unilateral or bilateral cleft lip and palate (only for group A);
- Absence of congenital craniofacial anomalies or syndromes (only for group B);
- Orthodontic-surgical treatment with bimaxillary orthognathic surgery;
- Absence of previous facial traumas;
- No previous orthognathic surgery;
- Availability of adequate radiographic documentation, photographs, dental casts, pre/post cephalometric analysis, 2D pre-surgical Visual Treatment Objectives (VTO).
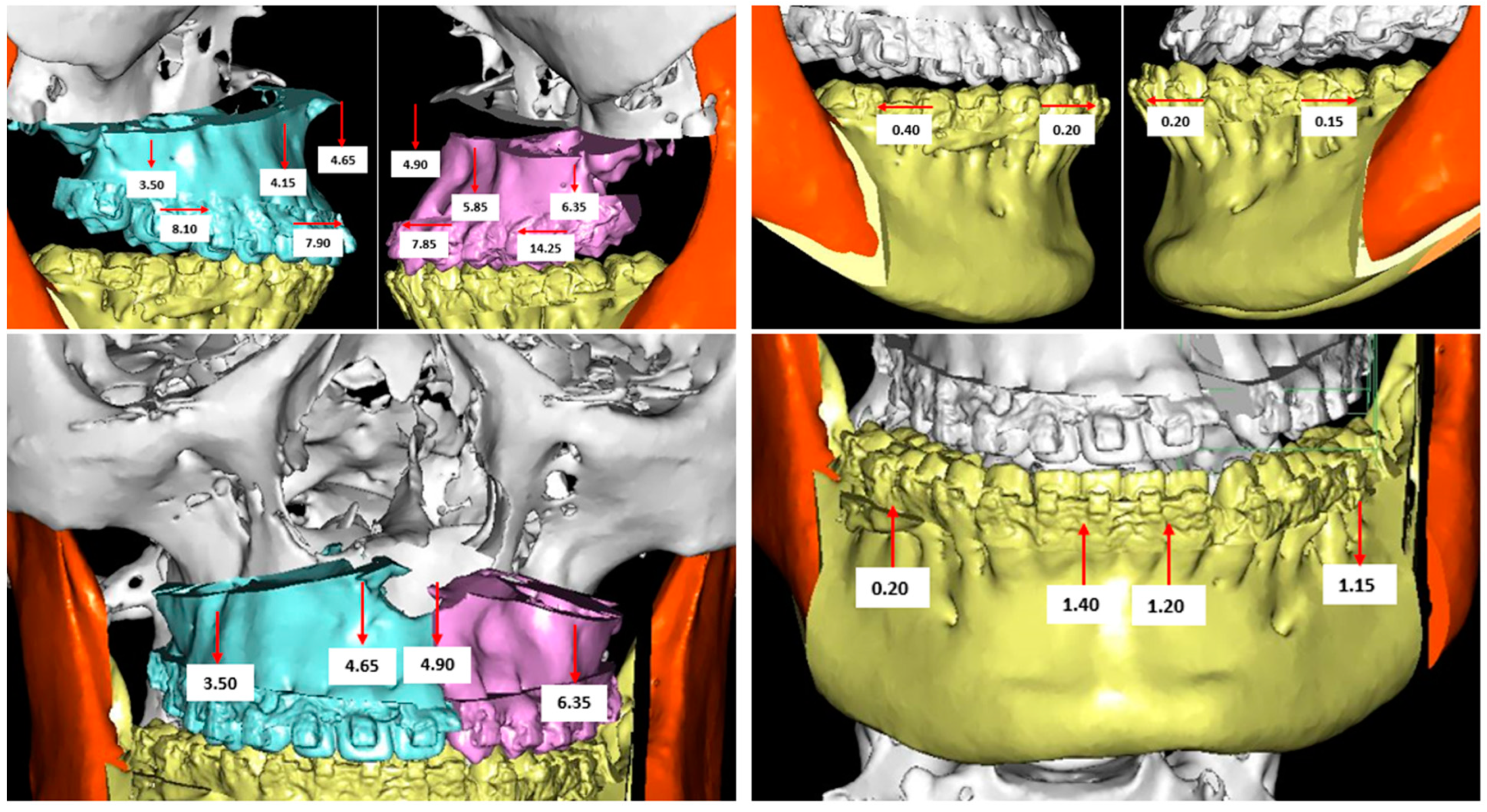
2.1. Digital Surgical Planning
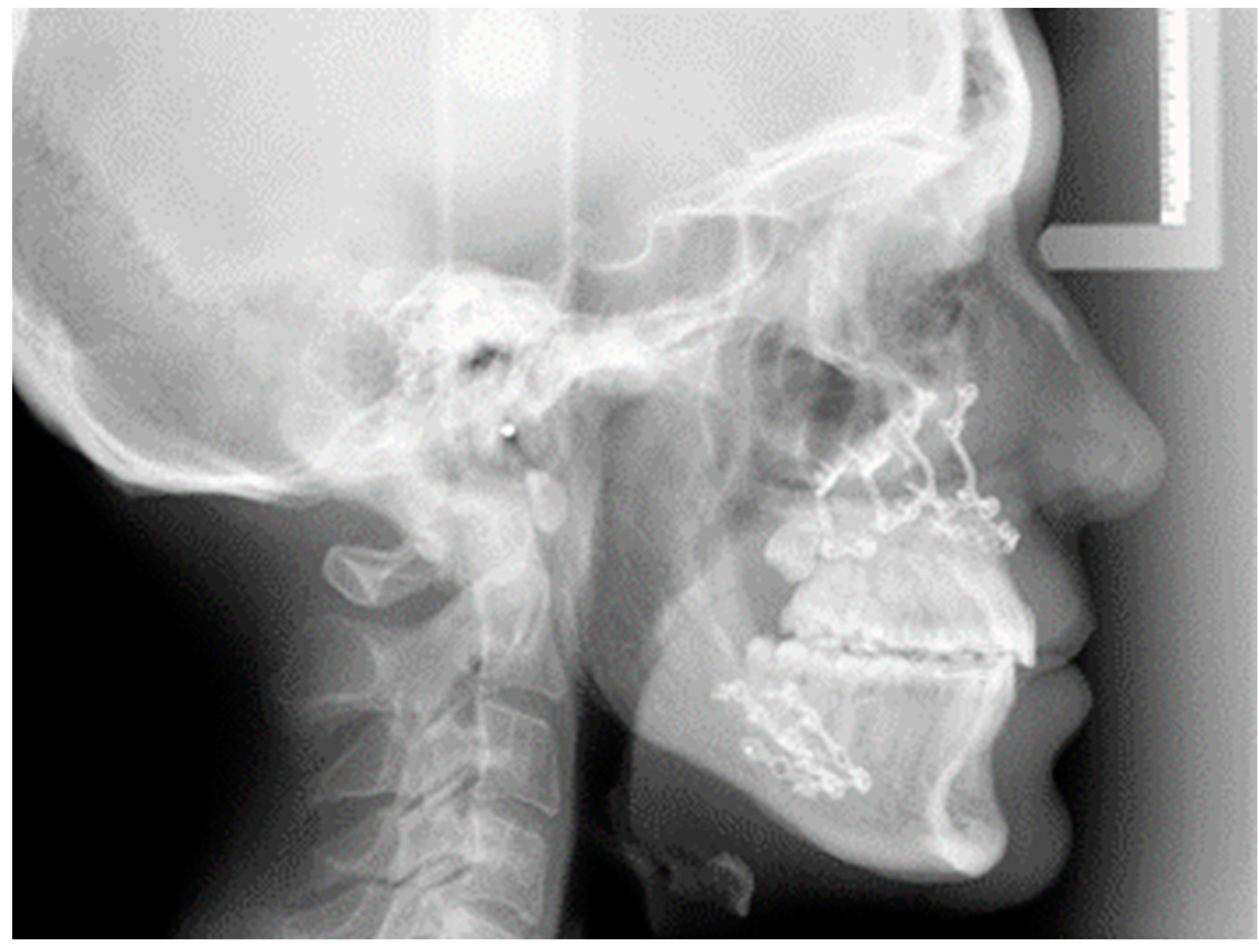
2.2. Evaluation of the Surgical Accuracy
- ANB angle to evaluate the skeletal class;
- SNA and SNB angles for the evaluation of the anterior-posterior position of the mandible and maxilla, respectively, relative to the upper and lower jaw;
- Gonial and Articular angles to evaluate verticality.
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lin, Y.; Fu, Z.; Ma, L.; Li, W. Cone-beam computed tomography-synthesized cephalometric study of operated unilateral cleft lip and palate and noncleft children with Class III skeletal relationship. Am. J. Orthod. Dentofac. Orthop. 2016, 150, 802–810. [Google Scholar] [CrossRef] [PubMed]
- Salari, N.; Darvishi, N.; Heydari, M.; Bokaee, S.; Darvishi, F.; Mohammadi, M. Global prevalence of cleft palate, cleft lip and cleft palate and lip: A comprehensive systematic review and meta-analysis. J. Stomatol. Oral Maxillofac. Surg. 2021, 123, 110–120. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, I.M.; Sakuda, K.; Takimoto, T. Miyazaki Craniofacial growth in complete unilateral cleft lip and palate: A roentgeno-cephalometric study. Cleft Palate J. 1976, 13, 215–237. [Google Scholar] [PubMed]
- Wlodarczyk, J.R.; Munabi, N.C.O.; Wolfswinkel, E.; Nagengast, E.; Higuchi, E.C.; Turk, M.; Urata, M.M.; Hammoudeh, J.A.; Yao, C.; Magee, W., 3rd. Midface Growth Potential in Unoperated Clefts: A Systematic Review and Meta-Analysis. J. Craniofacial Surg. 2021. [Google Scholar] [CrossRef] [PubMed]
- McCance, A.M.; Roberts-Harry, D.; Sherriff, M.; Mars, M.; Houston, W.J. A study model analysis of adult unoperated Sri Lankans with unilateral cleft lip and palate. Cleft Palate J. 1990, 27, 146–154. [Google Scholar]
- Wu, T.T.; Ko, E.W.; Chen, P.K.; Huang, C.S. Craniofacial characteristics in unilateral complete cleft lip and palate patients with congenitally missing teeth. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 381–390. [Google Scholar] [CrossRef]
- Astani, S.A.; Yilmaz, H.N.; Nevzatoglu, S.; Demirkaya, A.A.; Acar, Z.A. Evaluation of airway volume in cleft lip and palate following nasoalveolar molding. J. Craniofacial Surg. 2018, 29, 2143–2147. [Google Scholar] [CrossRef]
- Phillips, J.H.; Nish, I.; Daskalogiannakis, J. Orthognathic surgery in cleft patients. Plast. Reconstr. Surg. 2012, 129, 535e–548e. [Google Scholar] [CrossRef]
- McIntyre, J.K.; Sethi, H.; Schönbrunner, A.; Proudfoot, J.; Jones, M.; Gosman, A. Number of Surgical Procedures for Patients With Cleft lip and Palate From Birth to 21 Years Old at a Single Children’s Hospital. Ann. Plast. Surg. 2016, 76 (Suppl. S3), S205–S208. [Google Scholar] [CrossRef]
- Roy, A.A.; Rtshiladze, M.A.; Stevens, K.; Phillips, J. Orthognathic Surgery for Patients with Cleft Lip and Palate. Clin. Plast. Surg. 2019, 46, 157–171. [Google Scholar] [CrossRef]
- Good, P.M.; Mulliken, J.B.; Padwa, B.L. Frequency of Le Fort I osteotomy after repaired cleft lip and palate or cleft palate. Cleft Palate Craniofacial J. 2007, 44, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.J.; Wlodarczyk, J.R.; Nagengast, E.S.; Wolfswinkel, E.; Munabi, N.C.O.; Yao, C.; Magee, W.P., 3rd. The Likelihood of Orthognathic Surgery after Orofacial Cleft Repair. J. Craniofacial Surg. 2021, 32, 902–906. [Google Scholar] [CrossRef] [PubMed]
- Khechoyan, D.Y. Orthognathic surgery: General considerations. Semin. Plast. Surg. 2013, 27, 133–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaroni, F.M.; Cavalcante, R.C.; João da Costa, D.; Kluppel, L.E.; Scariot, R.; Rebellato, N.L.B. Complications associated with orthognathic surgery: A retrospective study of 485 cases. J. Cranio-Maxillofac. Surg. 2019, 47, 1855–1860. [Google Scholar] [CrossRef] [PubMed]
- Bell, W.H.; Jacobs, J.D. Surgical-orthodontic correction of maxillary retrusion by Le Fort I osteotomy and proplast. J. Maxillofac. Surg. 1980, 8, 84–94. [Google Scholar] [CrossRef]
- Berkowitz, S. Cleft Lip and Palate, 2nd ed.; Springer: Berlin, Heidelberg, 2006. [Google Scholar]
- Chen, Z.; Mo, S.; Fan, X.; You, Y.; Ye, G.; Zhou, N. A Meta-analysis and Systematic Review Comparing the Effectiveness of Traditional and Virtual Surgical Planning for Orthognathic Surgery: Based on Randomized Clinical Trials. J. Oral Maxillofac. Surg. 2021, 79, 471.e1–471.e19. [Google Scholar] [CrossRef]
- Barone, M.; De Stefani, A.; Baciliero, U.; Bruno, G.; Gracco, A. The Accuracy of Jaws Repositioning in Bimaxillary Orthognathic Surgery with Traditional Surgical Planning Compared to Digital Surgical Planning in Skeletal Class III Patients: A Retrospective Observational Study. J. Clin. Med. 2020, 9, 1840. [Google Scholar] [CrossRef]
- Yen, S.; Hammoudeh, J.; Edwards, S.P.; Urata, M. Orthodontic Considerations for Cleft Orthognathic Surgery. Oral Maxillofac. Surg. Clin. N. Am. 2020, 32, 249–267. [Google Scholar] [CrossRef]
- Proffit, W.R.; Fields HWJr Moray, L.J. Prevalence of malocclusion and orthodontic treatment need in the United States: Estimates from the NHANES III survey. Int. J. Adult Orthod. Orthognath. Surg. 1998, 13, 97–106. [Google Scholar]
- Altobelli, D.E.; Kikinis, R.; Mulliken, J.B.; Cline, H.; Lorensen, W.; Jolesz, F. Computer-assisted three-dimensional planning in craniofacial surgery. Plast. Reconstr. Surg. 1993, 92, 576–585. [Google Scholar] [CrossRef]
- Haas, O.L., Jr.; Becker, O.E.; de Oliveira, R.B. Computer-aided planning in orthognathic surgery-systematic review. Int. J. Oral Maxillofac. Surg. 2015, 44, 329–342. [Google Scholar] [CrossRef] [PubMed]
- Xia, J.J.; Gateno, J.; Teichgraeber, J.F.; Christensen, A.M.; Lasky, R.E.; Lemoine, J.J.; Liebschner, M.A.K. Accuracy of the computer-aided surgical simulation (CASS) system in the treatment of patients with complex craniomaxillofacial deformity: A pilot study. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 2007, 65, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Aboul-Hosn Centenero, S.; Hernandez-Alfaro, F. 3D planning in orthognathic surgery: CAD/CAM surgical splints and prediction of the soft and hard tissues results—Our experience in 16 cases. J. Cranio-Maxillo-Facial Surg. Off. Publ. Eur. Assoc. Cranio-Maxillo-Facial Surg. 2012, 40, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.H.; Lo, L.J. Three-dimensional computer-assisted surgical simulation and intraoperative navigation in orthognathic surgery: A literature review. J. Formos. Med. Assoc. Taiwan Yi Zhi 2015, 114, 300–307. [Google Scholar] [CrossRef] [Green Version]
- De Riu, G.; Meloni, S.M.; Baj, A.; Corda, A.; Soma, D.; Tullio, A. Computer-assisted orthognathic surgery for correction of facial asymmetry: Results of a randomised controlled clinical trial. Br. J. Oral Maxillofac. Surg. 2014, 52, 251–257. [Google Scholar] [CrossRef]
- Mossey, P.A. Epidemiology of oral clefts: An international perspective. In Cleft Lip and Palate: From Origins to Treatment; Mossey, P.A., Little, J., Wyszynski, D.F., Eds.; Oxford University Press: New York, NY, USA, 2002; pp. 127–158. [Google Scholar]
- Baek, S.-H.; Lee, J.-K.; Lee, J.-H.; Kim, M.-J.; Kim, J.-R. Comparison of treatment outcome and stability between distraction osteogenesis and LeFort I osteotomy in cleft patients with maxillary hypoplasia. J. Craniofacial Surg. 2007, 18, 1209–1215. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Group A: Average (SD) or n (%) | Group B: Average (SD) or n (%) | p-Value | |
|---|---|---|---|
| n | 16 | 16 | - |
| Males | 12 (75%) | 4 (25%) | 0.01 |
| Age at the time of surgery | 20 (3) | 25 (5) | 0.008 |
| Wits appraisal, mm | −6.9 (4.9) | −9.3 (4.8) | 0.19 |
| ANB, ° | −4.2 (2.7) | −3.3 (4.5) | 0.51 |
| DIFFERENCE (IN ABSOLUTE VALUE) BETWEEN THE OBTAINED AND PLANNED RESULT, AVERAGE (SD) | CASES WITH ABSOLUTE DIFFERENCE > 2°, N (%) | EQUIVALENCE TEST: 90% CI (p-VALUE) | |
|---|---|---|---|
| ANB, ° | 1.20 (1.01) | 2 (12%) | 0.76 to 1.64 (p = 0.003) |
| SNA, ° | 0.90 (0.95) | 0 (0%) | 0.48 to 1.31 (p = 0.0009) |
| SNB, ° | 0.66 (0.49) | 0 (0%) | 0.44 to 0.87 (p < 0.0001) |
| AR-GO-ME, ° | 1.09 (1.32) | 2 (12%) | 0.51 to 1.67 (p = 0.007) |
| S-AR-GO, ° | 0.83 (0.97) | 1 (6%) | 0.40 to 1.25 (p = 0.001) |
| DIFFERENCE (IN ABSOLUTE VALUE) BETWEEN THE OBTAINED AND PLANNED RESULT, AVERAGE (SD) | CASES WITH ABSOLUTE DIFFERENCE > 2°, N (%) | EQUIVALENCE TEST: 90% CI (p-VALUE) | |
|---|---|---|---|
| ANB, ° | 0.54 (0.50) | 0 (0%) | 0.32 to 0.76 (p = 0.0003) |
| SNA, ° | 0.70 (0.59) | 1 (6%) | 0.44 to 0.96 (p = 0.0001) |
| SNB, ° | 0.81 (0.78) | 1 (6%) | 0.47 to 1.15 (p = 0.0004) |
| Ar-Go-Me, ° | 1.43 (0.98) | 3 (18%) | 1.00 to 1.85 (p = 0.02) |
| S-Ar-Go, ° | 0.49 (0.44) | 0 (0%) | 0.30 to 0.68 (p = 0.0002) |
| DIFFERENCE (IN ABSOLUTE VALUE) BETWEEN THE OBTAINED AND PLANNED RESULT, AVERAGE (SD) | - | |||
|---|---|---|---|---|
| Group A | Group B | Mean Difference (95% CI) | p-Value | |
| ANB, ° | 1.20 (1.01) | 0.54 (0.50) | 0.66 (0.08 to 1.25) | 0.03 |
| SNA, ° | 0.90 (0.95) | 0.70 (0.59) | 0.20 (−0.40 to 0.80) | 0.50 |
| SNB, ° | 0.66 (0.49) | 0.81 (0.78) | −0.15 (−0.62 to 0.33) | 0.54 |
| Ar-Go-Me, ° | 1.09 (1.32) | 1.43 (0.98) | −0.34 (−1.19 to 0.50) | 0.41 |
| S-Ar-Go, ° | 0.83 (0.97) | 0.49 (0.44) | 0.34 (−0.22 to 0.89) | 0.22 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bollato, B.; Barone, M.; Gracco, A.; Baciliero, U.; Crivellin, G.; Bruno, G.; De Stefani, A. The Accuracy of Jaws Repositioning in Bimaxillary Orthognathic Surgery in Patients with Cleft Lip and Palate Compared to Non-Syndromic Skeletal Class III Patients. J. Clin. Med. 2022, 11, 2675. https://doi.org/10.3390/jcm11092675
Bollato B, Barone M, Gracco A, Baciliero U, Crivellin G, Bruno G, De Stefani A. The Accuracy of Jaws Repositioning in Bimaxillary Orthognathic Surgery in Patients with Cleft Lip and Palate Compared to Non-Syndromic Skeletal Class III Patients. Journal of Clinical Medicine. 2022; 11(9):2675. https://doi.org/10.3390/jcm11092675
Chicago/Turabian StyleBollato, Benedetta, Martina Barone, Antonio Gracco, Ugo Baciliero, Giorgia Crivellin, Giovanni Bruno, and Alberto De Stefani. 2022. "The Accuracy of Jaws Repositioning in Bimaxillary Orthognathic Surgery in Patients with Cleft Lip and Palate Compared to Non-Syndromic Skeletal Class III Patients" Journal of Clinical Medicine 11, no. 9: 2675. https://doi.org/10.3390/jcm11092675
APA StyleBollato, B., Barone, M., Gracco, A., Baciliero, U., Crivellin, G., Bruno, G., & De Stefani, A. (2022). The Accuracy of Jaws Repositioning in Bimaxillary Orthognathic Surgery in Patients with Cleft Lip and Palate Compared to Non-Syndromic Skeletal Class III Patients. Journal of Clinical Medicine, 11(9), 2675. https://doi.org/10.3390/jcm11092675