
The Relationship between Cognitive Functions and Psychopathological Symptoms in First Episode Psychosis and Chronic Schizophrenia

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Clinical Measures
2.3. Neurocognitive Assessment
2.4. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Differences in Cognitive Functions
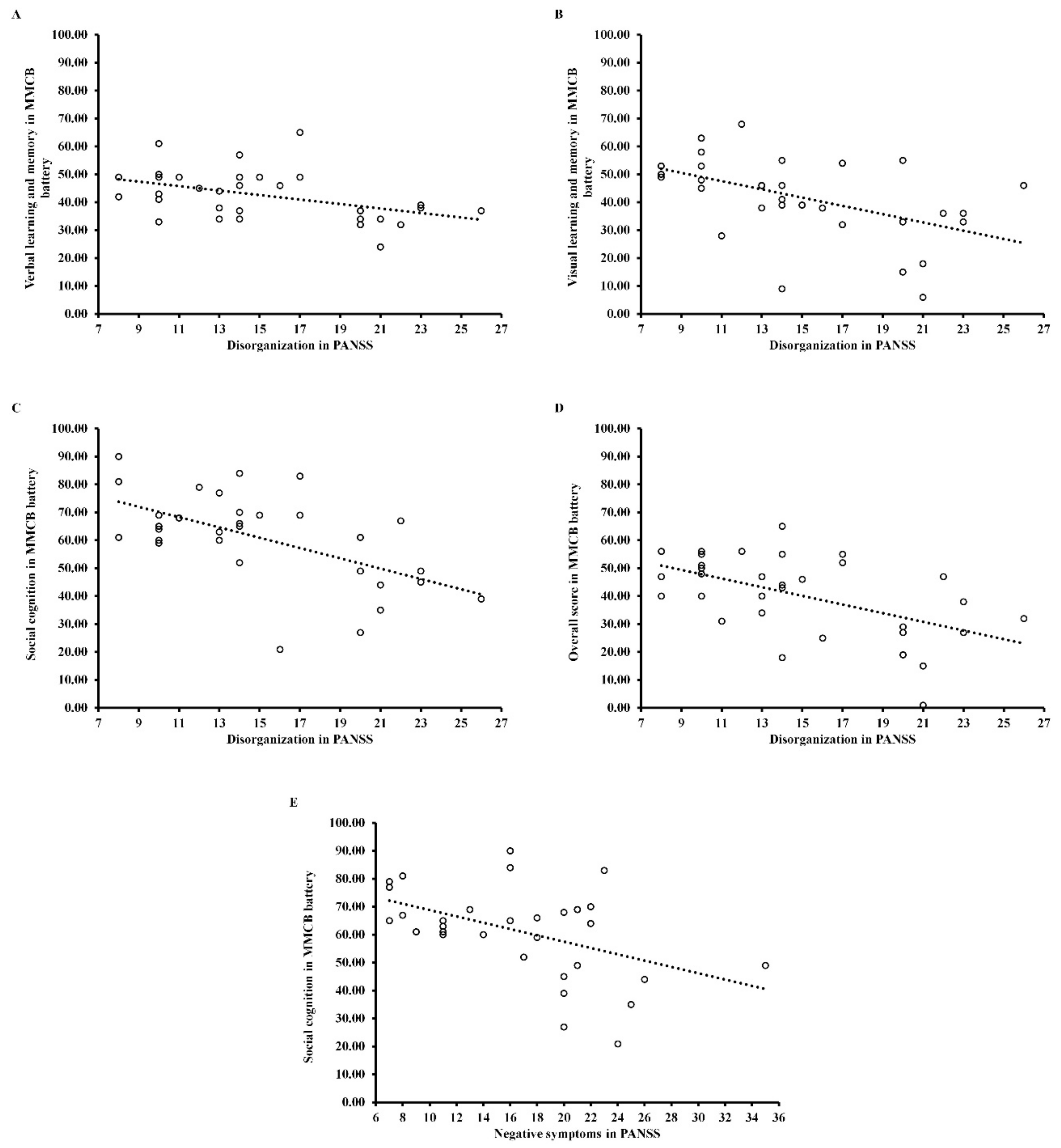
3.3. Relationship between Psychopathological Dimensions and Cognitive Functions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bora, E.; Murray, R.M. Meta-analysis of cognitive deficits in ultra-high risk to psychosis and first-episode psychosis: Do the cognitive deficits progress over, or after, the onset of psychosis? Schizophr. Bull. 2014, 40, 744–755. [Google Scholar] [CrossRef] [PubMed]
- Fioravanti, M.; Bianchi, V.; Cinti, M.E. Cognitive deficits in schizophrenia: An updated metanalysis of the scientific evidence. BMC Psychiatry 2012, 12, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, G.; Jin, H.; Lyu, H.; Liu, Y.; Guo, W.; Shi, C.; Meyers, J.; Wang, J.; Zhao, J.; et al. Cognitive deficits in subjects at risk for psychosis, first-episode and chronic schizophrenia patients. Psychiatry Res. 2019, 274, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Sponheim, S.R.; Jung, R.E.; Seidman, L.J.; Mesholam-Gately, R.I.; Manoach, D.S.; O’Leary, D.S.; Ho, B.C.; Andreasen, N.C.; Lauriello, J.; Schulz, S.C. Cognitive deficits in recent-onset and chronic schizophrenia. J. Psychiatry Res. 2010, 44, 421–428. [Google Scholar] [CrossRef]
- Wu, J.Q.; Tan, Y.L.; Xiu, M.H.; De Yang, F.; Soares, J.C.; Zhang, X.Y. Cognitive impairments in first-episode drug-naive and chronic medicated schizophrenia: MATRICS consensus cognitive battery in a Chinese Han population. Psychiatry Res. 2016, 238, 196–202. [Google Scholar] [CrossRef]
- Aas, M.; Dazzan, P.; Mondelli, V.; Melle, I.; Murray, R.M.; Pariante, C.M. A systematic review of cognitive function in first-episode psychosis, including a discussion on childhood trauma, stress, and inflammation. Front. Psychiatry 2014, 4, 182. [Google Scholar] [CrossRef]
- Keefe, R.S. The longitudinal course of cognitive impairment in schizophrenia: An examination of data from premorbid through posttreatment phases of illness. J. Clin. Psychiatry 2014, 75, 8–13. [Google Scholar] [CrossRef]
- Xiong, Y.B.; Bo, Q.J.; Wang, C.M.; Tian, Q.; Liu, Y.; Wang, C.Y. Differential of frequency and duration mismatch negativity and theta power deficits in first-episode and chronic schizophrenia. Front. Behav. Neurosci. 2019, 13, 37. [Google Scholar] [CrossRef]
- Bowie, C.R.; Harvey, P.D. Cognitive deficits and functional outcome in schizophrenia. Neuropsychiatr. Dis. Treat. 2006, 2, 531. [Google Scholar] [CrossRef]
- Minatogawa-Chang, T.M.; Schaufelberger, M.S.; Ayres, A.M.; Duran, F.L.; Gutt, E.K.; Murray, R.M.; Rushe, T.M.; McGuire, P.K.; Menazes, P.R.; Scazufca, M.; et al. Cognitive performance is related to cortical grey matter volumes in early stages of schizophrenia: A population-based study of first-episode psychosis. Schizophr. Res. 2009, 113, 200–209. [Google Scholar] [CrossRef]
- Tyburski, E.; Mak, M.; Samochowiec, A.; Plichta, P.; Bielecki, M.; Rek-Owodzin, K.; Podwalski, P.; Rutkowski, K.; Waszczuk, K.; Pełka- Wysiecka, J.; et al. The relationship between cingulum bundle integrity and different aspects of executive functions in chronic schizophrenia. Prog. Neuropsychopharmacol. Biol. Psychiatry 2020, 102, 109955. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, S.; Rosenheck, R.; Swartz, M.; Stroup, S.; Lieberman, J.A.; Keefe, R.S. Relationship of cognition and psychopathology to functional impairment in schizophrenia. Am. J. Psychiatry 2008, 165, 978–987. [Google Scholar] [CrossRef]
- Bozikas, V.P.; Kosmidis, M.H.; Kioperlidou, K.; Karavatos, A. Relationship between psychopathology and cognitive functioning in schizophrenia. Compr. Psychiatry 2004, 45, 392–400. [Google Scholar] [CrossRef] [PubMed]
- De Gracia Dominguez, M.; Viechtbauer, W.; Simons, C.J.; van Os, J.; Krabbendam, L. Are psychotic psychopathology and neurocognition orthogonal? A systematic review of their associations. Psychol. Bull. 2009, 135, 157. [Google Scholar] [CrossRef] [PubMed]
- Green, M.F.; Nuechterlein, K.H.; Gold, J.M.; Barch, D.M.; Cohen, J.; Essock, S.; Fenton, W.S.; Frese, F.; Goldberg, T.E.; Heaton, R.K.; et al. Approaching a consensus cognitive battery for clinical trials in schizophrenia: The NIMH-MATRICS conference to select cognitive domains and test criteria. Biol. Psychiatry 2004, 56, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Kay, S.R.; Fiszbein, A.; Opler, L.A. The Positive and Negative Syndrome Scale (PANSS) for Schizophrenia. Schizophr. Bull. 1987, 13, 261–276. [Google Scholar] [CrossRef]
- Nuechterlein, K.H.; Green, M.F.; Kern, R.S.; Baade, L.E.; Barch, D.M.; Cohen, J.D.; Essock, S.; Fenton, S.W.; Frese, F.J.; Gold, J.M. The MATRICS Consensus Cognitive Battery, part 1: Test selection, reliability, and validity. Am. J. Psychiatry 2008, 165, 203–213. [Google Scholar] [CrossRef] [PubMed]
- Myers, N.L. Udpate: Schizophrenia Across Cultures. Curr. Psychiatry Rep. 2011, 13, 305–3011. [Google Scholar] [CrossRef]
- Yang, Y.; Liu, Y.; Wang, G.; Hei, G.; Wang, X.; Li, R.; Wu, R.; Zhao, J. Brain-derived neurotrophic factor is associated with cognitive impairments in first-episode and chronic schizophrenia. Psychiatry Res. 2019, 273, 528–536. [Google Scholar] [CrossRef]
- Shafer, A.; Dazzi, F. Meta-analysis of the positive and Negative Syndrome Scale (PANSS) factor structure. J. Psychiatry Res. 2019, 115, 113–120. [Google Scholar] [CrossRef]
- World Health Organization (WHO). The ICD-10 Classification of Mental and Behavioural Disorders; World Health Organization: Geneva, Switzerland, 1993. [Google Scholar]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59, 22–33. [Google Scholar] [PubMed]
- Hall, R.C. Global assessment of functioning: A modified scale. Psychosomatics 1995, 36, 267–275. [Google Scholar] [CrossRef]
- Jędrasik-Styła, M.; Ciołkiewicz, A.; Styła, R.; Linke, M.; Parnowska, D.; Gruszka, A.; Denisiuk, M.; Jarema, M.; Green, M.F.; Wichniak, A. The Polish Academic Version of the MATRICS Consensus Cognitive Battery (MCCB): Evaluation of Psychometric Properties. Psychiatr. Q. 2015, 86, 435–447. [Google Scholar] [CrossRef] [PubMed]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R. Multivariate Data Analysis: A Global Perspective, 7th ed.; Pearson Educational International: Upper Saddle River, NJ, USA, 2010. [Google Scholar]
- Cohen, J. A Power Primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Wendt, H.W. Dealing with a Common Problem in Social Science: A Simplified Rank-Biserial Coefficient of Correlation Based on the U Statistic. Eur. J. Soc. Psychol. 1972, 2, 463–465. [Google Scholar] [CrossRef]
- Gray, C.D.; Kinnear, P.R. IBM SPSS Statistics 19 Made Simple; Psychology Press: New York, NY, USA, 2012. [Google Scholar]
- Corigliano, V.; De Carolis, A.; Trovini, G.; Dehning, J.; Di Pietro, S.; Curto, M.; Donato, N.; De Pisa, E.; Girardi, P.; Comparelli, A. Neurocognition in schizophrenia: From prodrome to multi-episode illness. Psychiatry Res. 2014, 220, 129–134. [Google Scholar] [CrossRef]
- McCleery, A.; Ventura, J.; Kern, R.S.; Subotnik, K.L.; Gretchen-Doorly, D.; Green, M.F.; Hellemann, G.S.; Nuechterlein, K.H. Cognitive functioning in first-episode schizophrenia: MATRICS Consensus Cognitive Battery (MCCB) Profile of Impairment. Schizophr. Res. 2014, 157, 33–39. [Google Scholar] [CrossRef]
- Rodriguez-Jimenez, R.; Santos, J.L.; Dompablo, M.; Santabárbara, J.; Aparicio, A.I.; Torioa, I.; Moreno-Ortegaab, M.; Lopez-Antonbf, R.; Lobobg, A.; Kernhi, R.S.; et al. MCCB cognitive profile in Spanish first episode schizophrenia patients. Schizophr. Res. 2019, 211, 88–92. [Google Scholar] [CrossRef]
- Bagney, A.; Dompablo, M.; Santabárbara, J.; Moreno-Ortega, M.; Lobo, A.; Jimenez-Arriero, M.A.; Palomo, T.; Rodriguez-Jimenez, R. Are negative symptoms really related to cognition in schizophrenia? Psychiatry Res. 2015, 230, 377–382. [Google Scholar] [CrossRef]
- Klingberg, S.; Wittorf, A.; Wiedemann, G. Disorganization and cognitive impairment in schizophrenia: Independent symptom dimensions? Eur. Arch. Psychiatry Clin. Neurosci. 2006, 256, 532–540. [Google Scholar] [CrossRef]
- Ventura, J.; Thames, A.D.; Wood, R.C.; Guzik, L.H.; Hellemann, G.S. Disorganization and reality distortion in schizophrenia: A meta-analysis of the relationship between positive symptoms and neurocognitive deficits. Schizophr. Res. 2010, 121, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Minor, K.S.; Lysaker, P.H. Necessary, but not sufficient: Links between neurocognition, social cognition, and metacognition in schizophrenia are moderated by disorganized symptoms. Schizophr. Res. 2014, 159, 198–204. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Cognitive Domain | Cognitive Tests |
|---|---|
| Attention/vigilance | Continuous Performance Test—Identical Pairs (CPT-IP) |
| Reasoning and problem solving | Neuropsychological Assessment Battery (NAB): Mazes |
| Social cognition | Mayer–Salovey–Caruso Emotional Intelligence Test (MSCEIT): Managing Emotions |
| Speed of processing | Trail Making Test (TMT): Part A |
| Brief assessment of Cognition in Schizophrenia (BACS) | |
| Category Fluency: Animal Fluency | |
| Working memory | Wechsler Memory Scale (WMS®-III): Spatial Span forward and backward (WMS-SS) |
| Letter number span (LNS) | |
| Verbal learning and memory | Hopkins Verbal Learning Test—Revised (HVLTR) |
| Visual learning and memory | Brief Visuospatial Memory Test—Revised (BVMT-R) |
| First-Episode Psychosis Patients (FEP) (n = 32) | Chronic Schizophrenia Patients (CS) (n = 70) | Healthy Control (HC) (n = 39) | F/χ2/t/Z | η2/d/rU | |
|---|---|---|---|---|---|
| Age: M (SD) | 28.09 (6.32) e***, g*** | 39.10 (6.85) | 37.08 (7.94) | 27.29 a*** | 0.28 h |
| Years of education: M (SD) | 12.81 (3.52) | 13.20 (2.93) f* | 14.59 (2.62) | 3.77 a* | 0.05 h |
| Sex: female/male | 18/14 | 30/40 | 23/16 | 3.18 b | - |
| Antipsychotic medications: | |||||
| Atypical: n (%) | 28 (87.50) | 46 (65.71) | - | 6.91 b | - |
| Atypical and typical: n (%) | 2 (6.25) | 20 (28.57) | - | ||
| Typical: n (%) | 1 (3.125) | 3 (4.29) | - | ||
| No medications: n (%) | 1 (3.125) | 1 (1.43) | - | ||
| Chlorpromazine equivalent (mg): M (SD) | 478.69 (299.48) | 671.69 (290.30) | - | −3.08 c** | 0.62 i |
| Duration of illness in years: M (SD) | 0.71 (1.27) | 14.97 (5.49) | - | −8.13 d*** | 1.00 j |
| Exacerbation: M (SD) | 1.06 (0.25) | 6.19 (4.30) | - | −8.06 d*** | 0.98 j |
| Global functioning in GAF: M (SD) | 57.61 (17.04) | 55.51 (14.91) | - | 0.62 c | - |
| Psychopathological dimensions in PANSS: | |||||
| Positive symptoms: M (SD) | 12.03 (4.80) | 7.71 (3.77) | - | −4.48 d*** | 0.55 j |
| Negative symptoms: M (SD) | 16.81 (6.69) | 16.77 (6.45) | - | −0.10 d | - |
| Disorganization: M (SD) | 14.91 (5.06) | 11.81 (3.81) | - | −3.02 d* | 0.37 j |
| Affect: M (SD) | 10.19 (3.88) | 8.79 (3.38) | - | −1.78 d | - |
| Resistance: M (SD) | 5.38 (1.91) | 4.66 (1.99) | - | −2.43 d* | 0.25 j |
| First-Episode Psychosis Patients (FEP) (n = 32) | Chronic Schizophrenia Patients (CS) (n = 70) | Healthy Control (HC) (n = 39) | F | η2 | |
|---|---|---|---|---|---|
| Speed of processing | 37.66 (13.35) a*** | 31.90 (12.27) b*** | 53.15 (9.66) | 39.86 *** | 0.37 |
| Attention/vigilance | 35.97 (10.80) a*** | 28.04 (10.24) b*** | 42.90 (11.55) | 23.53 *** | 0.26 |
| Working memory | 46.59 (15.07) a*,c** | 36.54 (11.83) b*** | 54.51 (9.57) | 24.98 *** | 0.27 |
| Verbal learning and memory | 42.69 (9.04) a** | 38.16 (9.92) b*** | 48.95 (7.50) | 15.31 *** | 0.18 |
| Visual learning and memory | 41.84 (15.06) a** | 37.07 (14.20) b*** | 56.90 (8.21) | 26.38 *** | 0.28 |
| Reasoning and problem solving | 44.75 (10.98) a** | 40.37 (10.08) b*** | 54.44 (9.20) | 21.28 *** | 0.24 |
| Social cognition | 61.13 (16.18) a* | 55.40 (13.56) b*** | 67.87 (9.33) | 8.15 *** | 0.11 |
| Overall score | 40.28 (14.64) a***, c* | 30.26 (12.68) b*** | 56.69 (9.13) | 50.57 *** | 0.43 |
| Speed of Processing | Attention/Vigilance | Working Memory | Verbal Learning and Memory | Visual Learning and Memory | Reasoning and Problem Solving | Social Cognition | Overall Score | |
|---|---|---|---|---|---|---|---|---|
| First-Episode Psychosis Patients (FEP) | ||||||||
| r | r | r | r | r | r | r | r | |
| Positive symptoms | −0.18 | −0.05 | −0.18 | −0.27 | −0.23 | −0.16 | −0.23 | −0.28 |
| Negative symptoms | −0.26 | −0.05 | −0.01 | −0.05 | −0.39 | −0.26 | −0.47 * | −0.35 |
| Disorganization | −0.29 | −0.31 | −0.06 | −0.45 * | −0.50 * | −0.32 | −0.58 *** | −0.54 * |
| Affect | −0.10 | 0.40 | 0.02 | 0.20 | 0.07 | 0.15 | −0.08 | 0.11 |
| Resistance | −0.06 | 0.07 | 0.00 | −0.22 | −0.12 | 0.37 | 0.10 | 0.03 |
| Chronic Schizophrenia Patients (CS) | ||||||||
| rho | rho | rho | rho | rho | rho | rho | rho | |
| Positive symptoms | −0.11 | −0.07 | −0.11 | −0.01 | −0.21 | −0.34 * | −0.11 | −0.22 |
| Negative symptoms | −0.30 * | −0.20 | −0.28 | −0.14 | −0.39 * | −0.16 | −0.14 | −0.39 *** |
| Disorganization | −0.32 * | −0.05 | −0.20 | 0.01 | −0.25 | −0.36 * | −0.13 | −0.34 * |
| Affect | 0.02 | −0.19 | −0.01 | 0.12 | −0.04 | 0.00 | 0.05 | −0.01 |
| Resistance | −0.25 | 0.10 | 0.06 | 0.03 | −0.08 | −0.26 | 0.00 | −0.11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rek-Owodziń, K.; Tyburski, E.; Plichta, P.; Waszczuk, K.; Bielecki, M.; Wietrzyński, K.; Podwalski, P.; Rudkowski, K.; Michalczyk, A.; Grąźlewski, T.; et al. The Relationship between Cognitive Functions and Psychopathological Symptoms in First Episode Psychosis and Chronic Schizophrenia. J. Clin. Med. 2022, 11, 2619. https://doi.org/10.3390/jcm11092619
Rek-Owodziń K, Tyburski E, Plichta P, Waszczuk K, Bielecki M, Wietrzyński K, Podwalski P, Rudkowski K, Michalczyk A, Grąźlewski T, et al. The Relationship between Cognitive Functions and Psychopathological Symptoms in First Episode Psychosis and Chronic Schizophrenia. Journal of Clinical Medicine. 2022; 11(9):2619. https://doi.org/10.3390/jcm11092619
Chicago/Turabian StyleRek-Owodziń, Katarzyna, Ernest Tyburski, Piotr Plichta, Katarzyna Waszczuk, Maksymilian Bielecki, Krzysztof Wietrzyński, Piotr Podwalski, Krzysztof Rudkowski, Anna Michalczyk, Tomasz Grąźlewski, and et al. 2022. "The Relationship between Cognitive Functions and Psychopathological Symptoms in First Episode Psychosis and Chronic Schizophrenia" Journal of Clinical Medicine 11, no. 9: 2619. https://doi.org/10.3390/jcm11092619
APA StyleRek-Owodziń, K., Tyburski, E., Plichta, P., Waszczuk, K., Bielecki, M., Wietrzyński, K., Podwalski, P., Rudkowski, K., Michalczyk, A., Grąźlewski, T., Sagan, L., Kucharska-Mazur, J., Samochowiec, J., & Mak, M. (2022). The Relationship between Cognitive Functions and Psychopathological Symptoms in First Episode Psychosis and Chronic Schizophrenia. Journal of Clinical Medicine, 11(9), 2619. https://doi.org/10.3390/jcm11092619