
Assessment of Rib Fracture in Acute Trauma Using Automatic Rib Segmentation and a Curved, Unfolded View of the Ribs: Is There a Saving of Time?

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
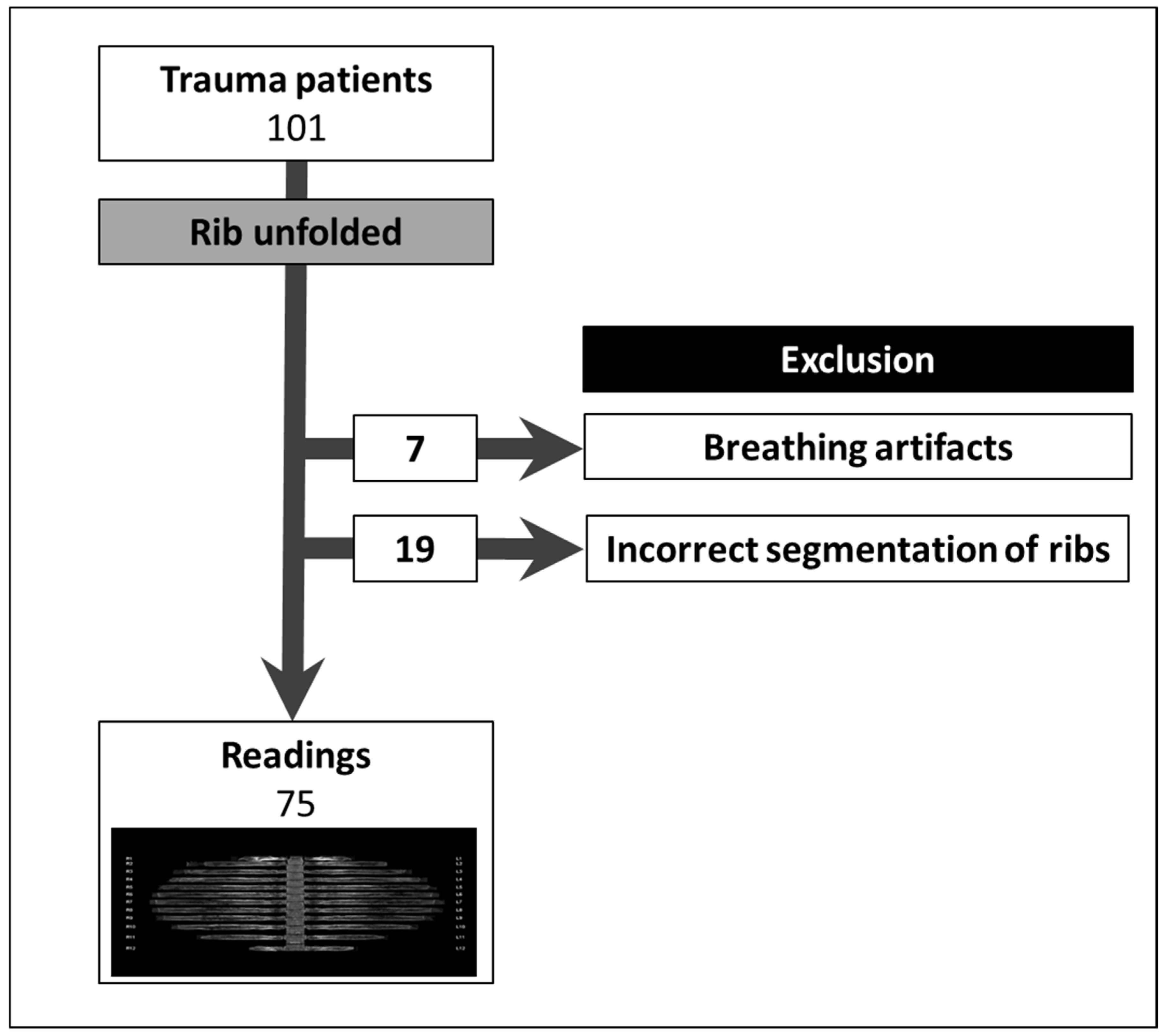
2.1. Study Design and Patient Selection
2.2. CT Acquisition and Post-Processing
2.3. Image Analysis
2.4. Statistical Analysis
3. Results
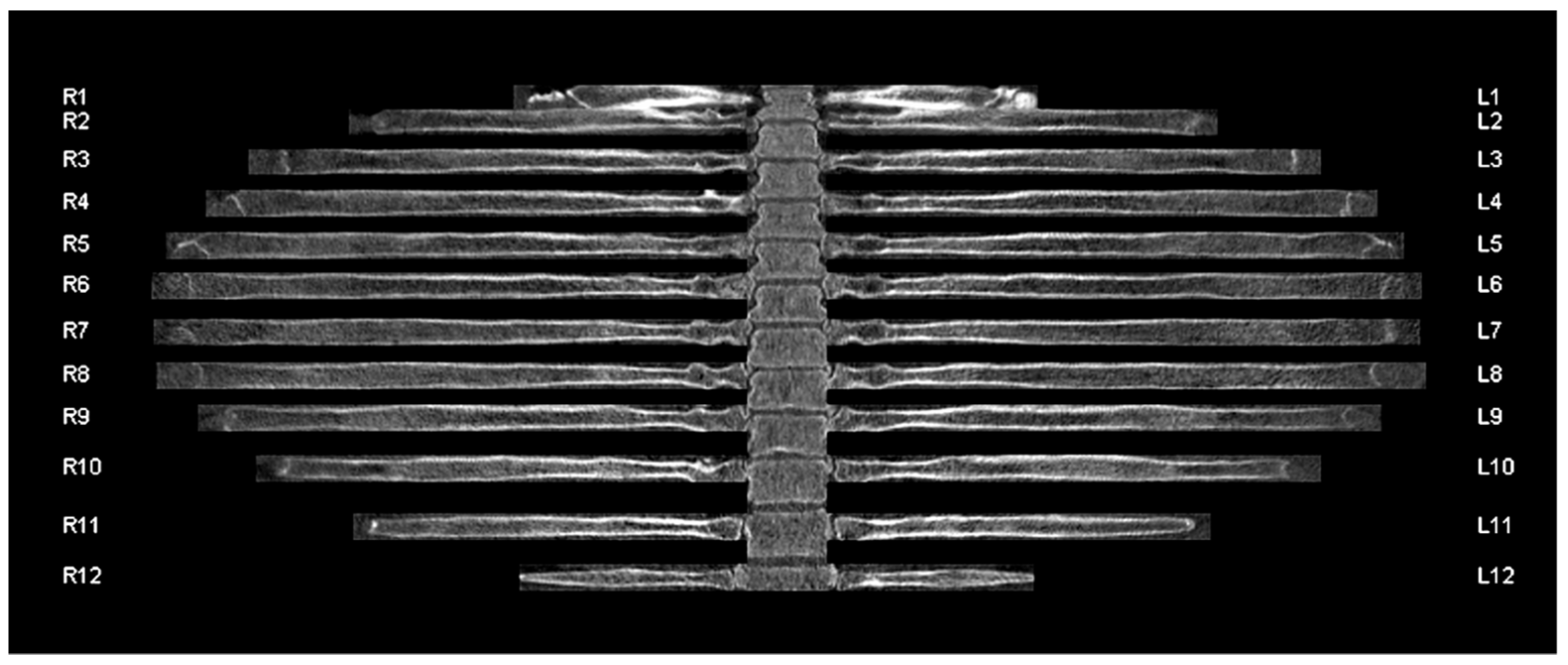
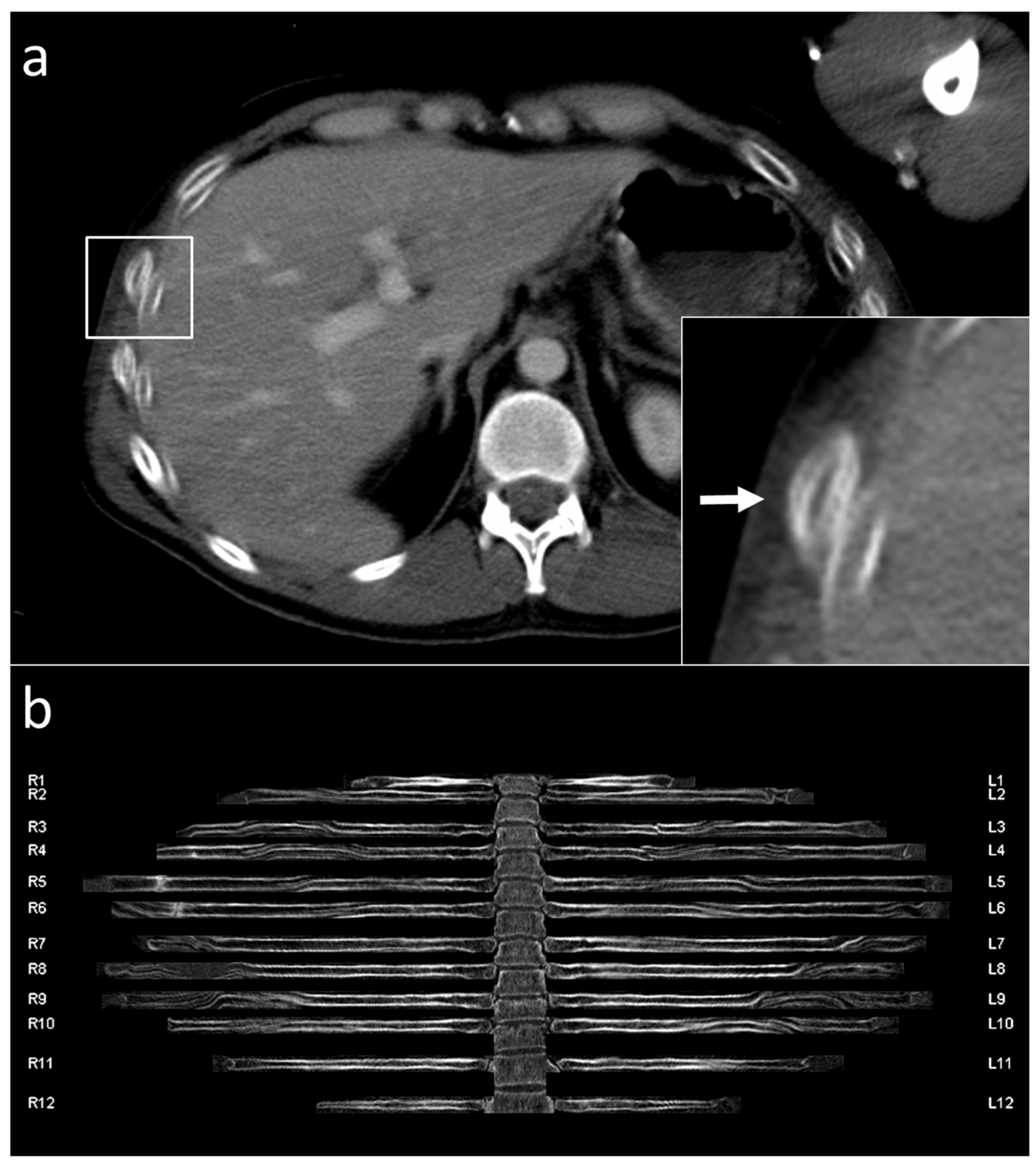
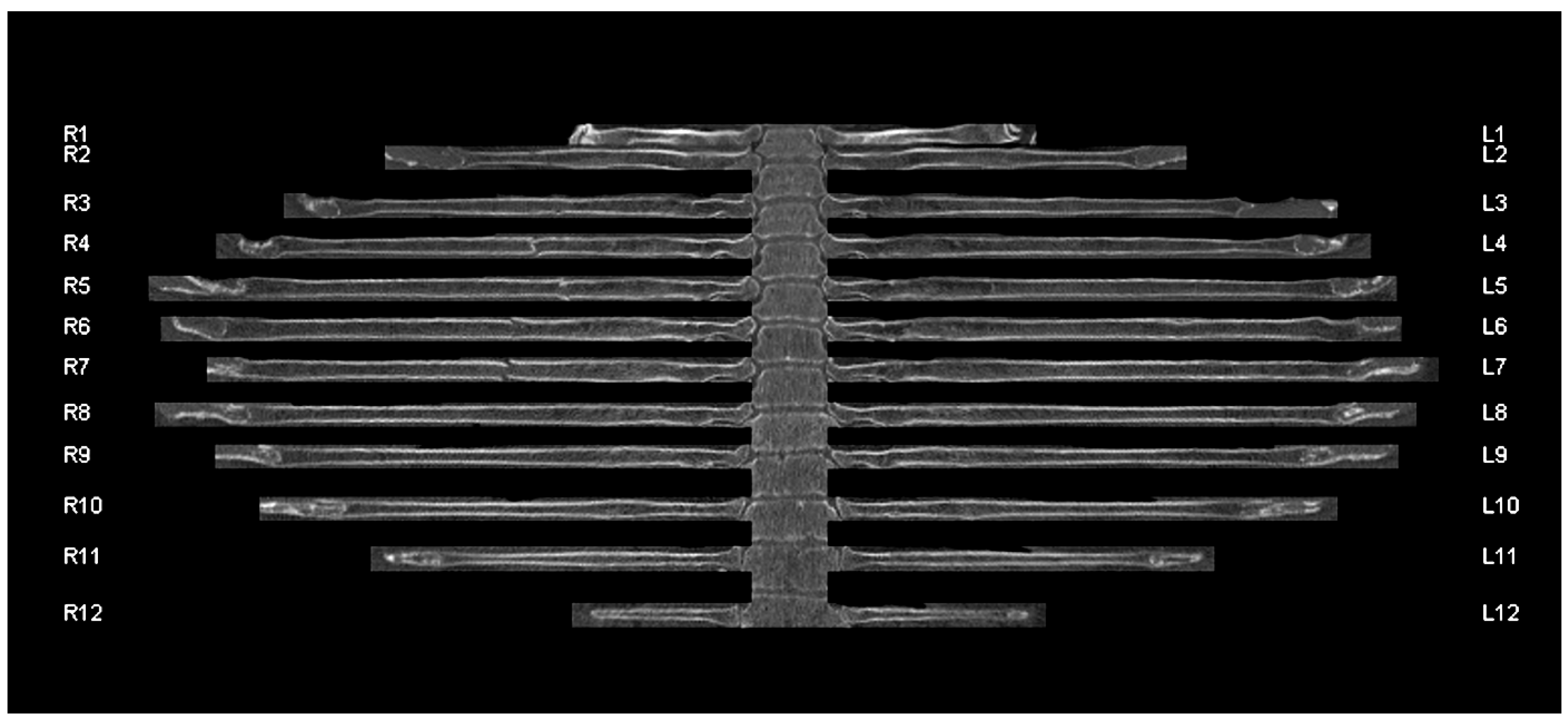
3.1. Segmentation and Labelling
3.2. Patient Characteristics
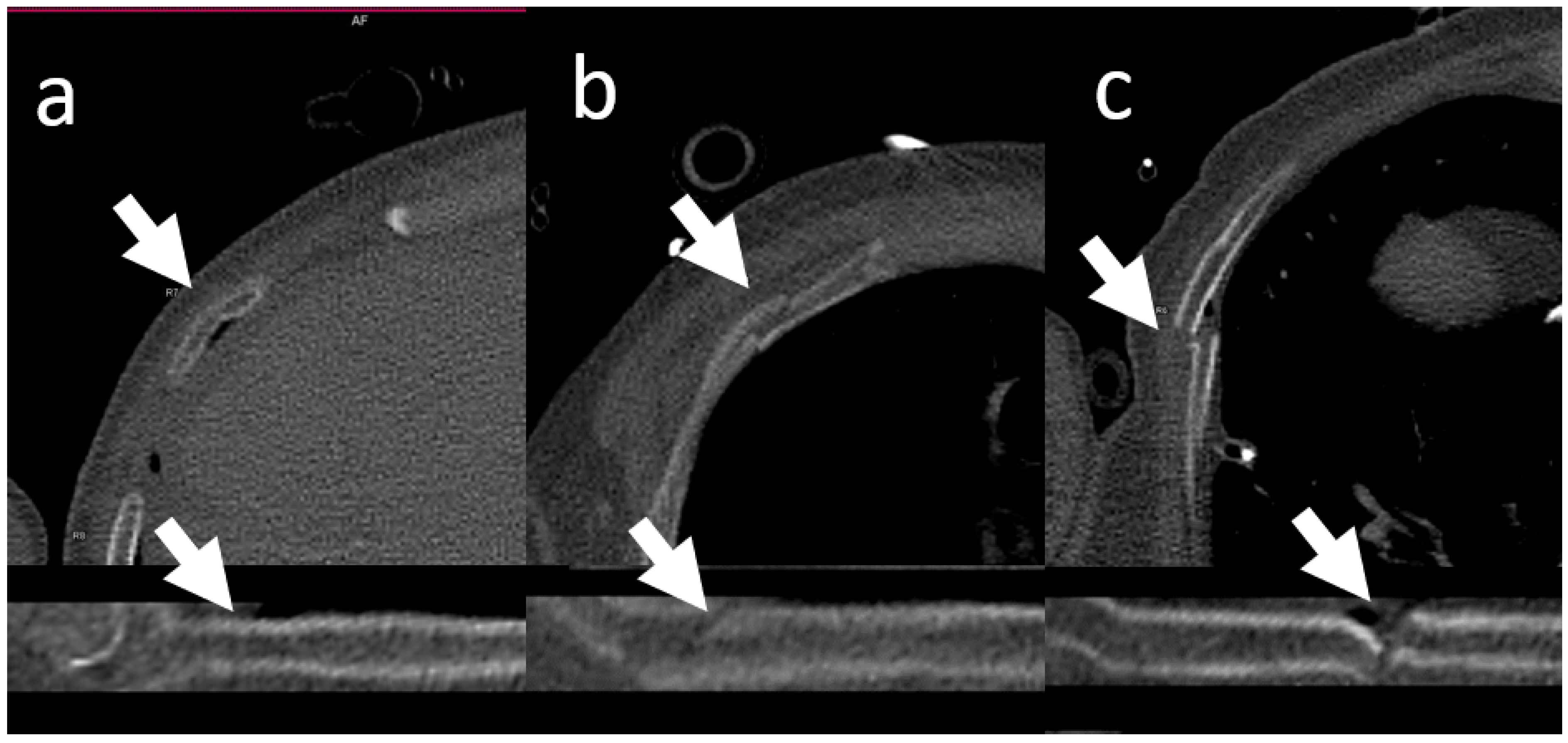
3.3. Rib Fractures
3.4. Diagnostic Accuracy
3.5. Investigation Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Battle, C.E.; Hutchings, H.; Evans, P.A. Risk factors that predict mortality in patients with blunt chest wall trauma: A systematic review and meta-analysis. Injury 2012, 43, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Livingston, D.H.; Shogan, B.; John, P.; Lavery, R.F. CT diagnosis of Rib fractures and the prediction of acute respiratory failure. J. Trauma 2008, 64, 905–911. [Google Scholar] [CrossRef] [PubMed]
- Sirmali, M.; Türüt, H.; Topcu, S.; Gülhan, E.; Yazici, Ü.; Kaya, S.; Taştepe, I. A comprehensive analysis of traumatic rib fractures: Morbidity, mortality and management. Eur. J. Cardio Thorac. Surg. 2003, 24, 133–138. [Google Scholar] [CrossRef]
- Marasco, S.; Lee, G.; Summerhayes, R.; Fitzgerald, M.; Bailey, M. Quality of life after major trauma with multiple rib fractures. Injury 2015, 46, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Gordy, S.; Fabricant, L.; Ham, B.; Mullins, R.; Mayberry, J. The contribution of rib fractures to chronic pain and disability. Am. J. Surg. 2014, 207, 659–662. [Google Scholar] [CrossRef] [PubMed]
- Gunn, M.L.; Kool, D.R.; Lehnert, B.E. Improving outcomes in the patient with polytrauma: A review of the role of whole-body computed tomography. Radiol. Clin. N. Am. 2015, 53, 639–656. [Google Scholar] [CrossRef] [PubMed]
- Huber-Wagner, S.; Lefering, R.; Qvick, L.-M.; Körner, M.; Kay, M.V.; Pfeifer, K.-J.; Reiser, M.; Mutschler, W.; Kanz, K.-G. Effect of whole-body CT during trauma resuscitation on survival: A retrospective, multicentre study. Lancet 2009, 373, 1455–1461. [Google Scholar] [CrossRef]
- Jiang, L.; Ma, Y.; Jiang, S.; Ye, L.; Zheng, Z.; Xu, Y.; Zhang, M. Comparison of whole-body computed tomography vs selective radiological imaging on outcomes in major trauma patients: A meta-analysis. Scand. J. Trauma Resusc. Emerg. Med. 2014, 22, 54. [Google Scholar] [CrossRef] [PubMed]
- Sokolovskaya, E.; Shinde, T.; Ruchman, R.B.; Kwak, A.J.; Lu, S.; Shariff, Y.K.; Wiggins, E.F.; Talangbayan, L. The effect of faster reporting speed for imaging studies on the number of misses and interpretation errors: A pilot study. J. Am. Coll. Radiol. 2015, 12, 683–688. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Song, H.H.; Han, J.H.; Park, J.M.; Lee, E.J.; Kang, K.J.; Lee, J.H.; Hwang, S.S.; Rho, S.C.; Jeong, S.O.; et al. Effect of noise on the detection of rib fractures by residents. Investig. Radiol. 1994, 29, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Mang, T.; Kolligs, F.T.; Schaefer, C.; Reiser, M.F.; Graser, A. Comparison of diagnostic accuracy and interpretation times for a standard and an advanced 3D visualisation technique in CT colonography. Eur. Radiol. 2010, 21, 653–662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ringl, H.; Schernthaner, R.; Philipp, M.O.; Metz-Schimmerl, S.; Czerny, C.; Weber, M.; Gäbler, C.; Steiner-Ringl, A.; Peloschek, P.; Herold, C.J.; et al. Three-dimensional fracture visualisation of multidetector CT of the skull base in trauma patients: Comparison of three reconstruction algorithms. Eur. Radiol. 2009, 19, 2416–2424. [Google Scholar] [CrossRef] [PubMed]
- Ringl, H.; Schernthaner, R.; Schueller, G.; Balassy, C.; Kienzl, D.; Botosaneanu, A.; Weber, M.; Czerny, C.; Hajdu, S.; Mang, T.; et al. The skull unfolded: A cranial CT visualization algorithm for fast and easy detection of skull fractures. Radiology 2010, 255, 553–562. [Google Scholar] [CrossRef] [PubMed]
- Ringl, H.; Lazar, M.; Töpker, M.; Woitek, R.; Prosch, H.; Asenbaum, U.; Balassy, C.; Toth, D.; Weber, M.; Hajdu, S.; et al. The ribs unfolded—A CT visualization algorithm for fast detection of rib fractures: Effect on sensitivity and specificity in trauma patients. Eur. Radiol. 2015, 25, 1865–1874. [Google Scholar] [CrossRef] [PubMed]
- Bier, G.; Schabel, C.; Othman, A.; Bongers, M.N.; Schmehl, J.; Ditt, H.; Nikolaou, K.; Bamberg, F.; Notohamiprodjo, M. Enhanced reading time efficiency by use of automatically unfolded CT rib reformations in acute trauma. Eur. J. Radiol. 2015, 84, 2173–2180. [Google Scholar] [CrossRef] [PubMed]
- Pepe, M.S. The Statistical Evaluation of Medical Tests for Classification and Prediction, 2nd ed.; Oxford University Press: Oxford, UK, 2003. [Google Scholar]
- Cochran, W.G. Sampling Techniques, 3rd ed.; John Wiley and Sons: New York, NY, USA, 1977. [Google Scholar]
- Cohen, J. A coefficient of agreement for nominal scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Pulley, B.R.; Taylor, B.C.; Fowler, T.T.; Dominguez, N.; Trinh, T.Q. Utility of three-dimensional computed tomography for the surgical management of rib fractures. J. Trauma Acute Care Surg. 2015, 78, 530–534. [Google Scholar] [CrossRef] [PubMed]
- Khung, S.; Masset, P.; Duhamel, A.; Faivre, J.-B.; Flohr, T.; Remy, J.; Remy-Jardin, M. Automated 3D rendering of ribs in 110 polytrauma patients: Strengths and limitations. Acad. Radiol. 2016, 24, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Chai, Z.; Qian, G.; Lin, H.; Wang, Q.; Wang, L.; Chen, H. Development and evaluation of a deep learning algorithm for rib segmentation and fracture detection from multicenter chest CT images. Radiol. Artif. Intell. 2021, 3, e200248. [Google Scholar] [CrossRef] [PubMed]
- Jin, L.; Yang, J.; Kuang, K.; Ni, B.; Gao, Y.; Sun, Y.; Gao, P.; Ma, W.; Tan, M.; Kang, H.; et al. Deep-learning-assisted detection and segmentation of rib fractures from CT scans: Development and validation of FracNet. EBioMedicine 2020, 62, 103106. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics (n = 75) | |
| Age—years | 45 ± 19 |
| Male sex | 57 (76%) |
| Trauma mechanism | |
| Traffic accident | 45 (60%) |
| Fall from great height | 24 (32%) |
| Other | 6 (8%) |
| Injured regions | |
| Head | 17 (22.7%) |
| Chest | 35 (46.7%) |
| Abdomen | 23 (30.7%) |
| Limbs | 10 (13.3%) |
| Sensitivity | Specificity | |||
|---|---|---|---|---|
| Axial | Unfolded | Axial | Unfolded | |
| Per-patient analysis | ||||
| Reader 1 | 92% (23/25) | 84% (21/25) | 100% (50/50) | 98% (49/50) |
| Reader 2 | 56% (14/25) | 84% (21/25) | 94% (47/50) | 96% (48/50) |
| Per-rib analysis | ||||
| Reader 1 | 93% (99/107) | 76% (82/107) | 100% (1689/1693) | 100% (1687/1693) |
| Reader 2 | 42% (45/107) | 67% (72/107) | 99% (1677/1693) | 100% (1690/1693) |
| Axial View | Unfolded View | p-Value | |
|---|---|---|---|
| Sensitivity | |||
| Reader 1 | 94% [90%, 99%] | 81% [62%, 100%] | 0.002 |
| Reader 2 | 63% [46%, 81%] | 71% [54%, 88%] | <0.001 |
| Specificity | |||
| Reader 1 | 100% [100%, 100%] | 100% [100%, 100%] | 0.754 |
| Reader 2 | 99% [99%, 99%] | 100% [100%, 100%] | 0.002 |
| Fracture Type | Buckled | Undislocated | Dislocated |
|---|---|---|---|
| Fractured ribs—no. | 13 | 63 | 31 |
| Reader 1 | 4/13 (31%) | 49/63 (78%) | 29/31 (94%) |
| Reader 2 | 5/13 (38%) | 39/63 (62%) | 28/31 (90%) |
| Axial View | Unfolded View | p-Value | |
|---|---|---|---|
| Reader 1 | 68.6 ± 32.4 (25–157) | 19.5 ± 9.4 (8–58) | <0.001 |
| Reader 2 | 40.2 ± 12.7 (23–101) | 24.1 ± 9.5 (10–57) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pregler, B.; Beyer, L.P.; Platz Batista da Silva, N.; Steer, S.; Zeman, F.; Popp, D.; Stroszczynski, C.; Müller-Wille, R. Assessment of Rib Fracture in Acute Trauma Using Automatic Rib Segmentation and a Curved, Unfolded View of the Ribs: Is There a Saving of Time? J. Clin. Med. 2022, 11, 2502. https://doi.org/10.3390/jcm11092502
Pregler B, Beyer LP, Platz Batista da Silva N, Steer S, Zeman F, Popp D, Stroszczynski C, Müller-Wille R. Assessment of Rib Fracture in Acute Trauma Using Automatic Rib Segmentation and a Curved, Unfolded View of the Ribs: Is There a Saving of Time? Journal of Clinical Medicine. 2022; 11(9):2502. https://doi.org/10.3390/jcm11092502
Chicago/Turabian StylePregler, Benedikt, Lukas Philipp Beyer, Natascha Platz Batista da Silva, Sebastian Steer, Florian Zeman, Daniel Popp, Christian Stroszczynski, and René Müller-Wille. 2022. "Assessment of Rib Fracture in Acute Trauma Using Automatic Rib Segmentation and a Curved, Unfolded View of the Ribs: Is There a Saving of Time?" Journal of Clinical Medicine 11, no. 9: 2502. https://doi.org/10.3390/jcm11092502
APA StylePregler, B., Beyer, L. P., Platz Batista da Silva, N., Steer, S., Zeman, F., Popp, D., Stroszczynski, C., & Müller-Wille, R. (2022). Assessment of Rib Fracture in Acute Trauma Using Automatic Rib Segmentation and a Curved, Unfolded View of the Ribs: Is There a Saving of Time? Journal of Clinical Medicine, 11(9), 2502. https://doi.org/10.3390/jcm11092502