
Non-Achievement of Alanine Aminotransferase Normalization Associated with the Risk of Hepatocellular Carcinoma during Nucleos(t)ide Analogue Therapies: A Multicenter Retrospective Study

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Assays of Serological Tests and HBV Genotypes
2.4. HCC Surveillance
2.5. Statistical Analysis
3. Results
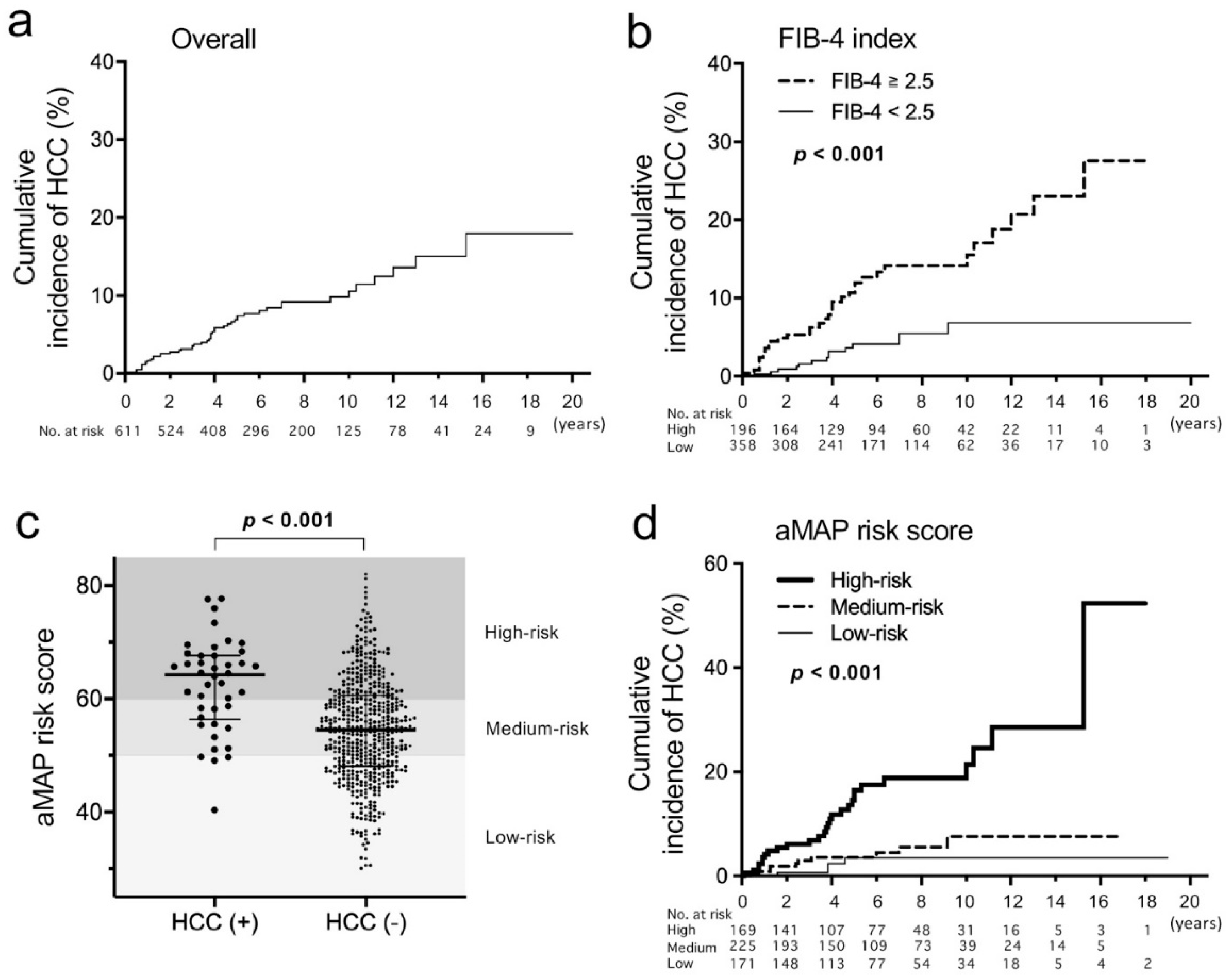
3.1. Patient Characteristics and Validation of the aMAP Risk Score
3.2. Factors Associated with HCC Incidence
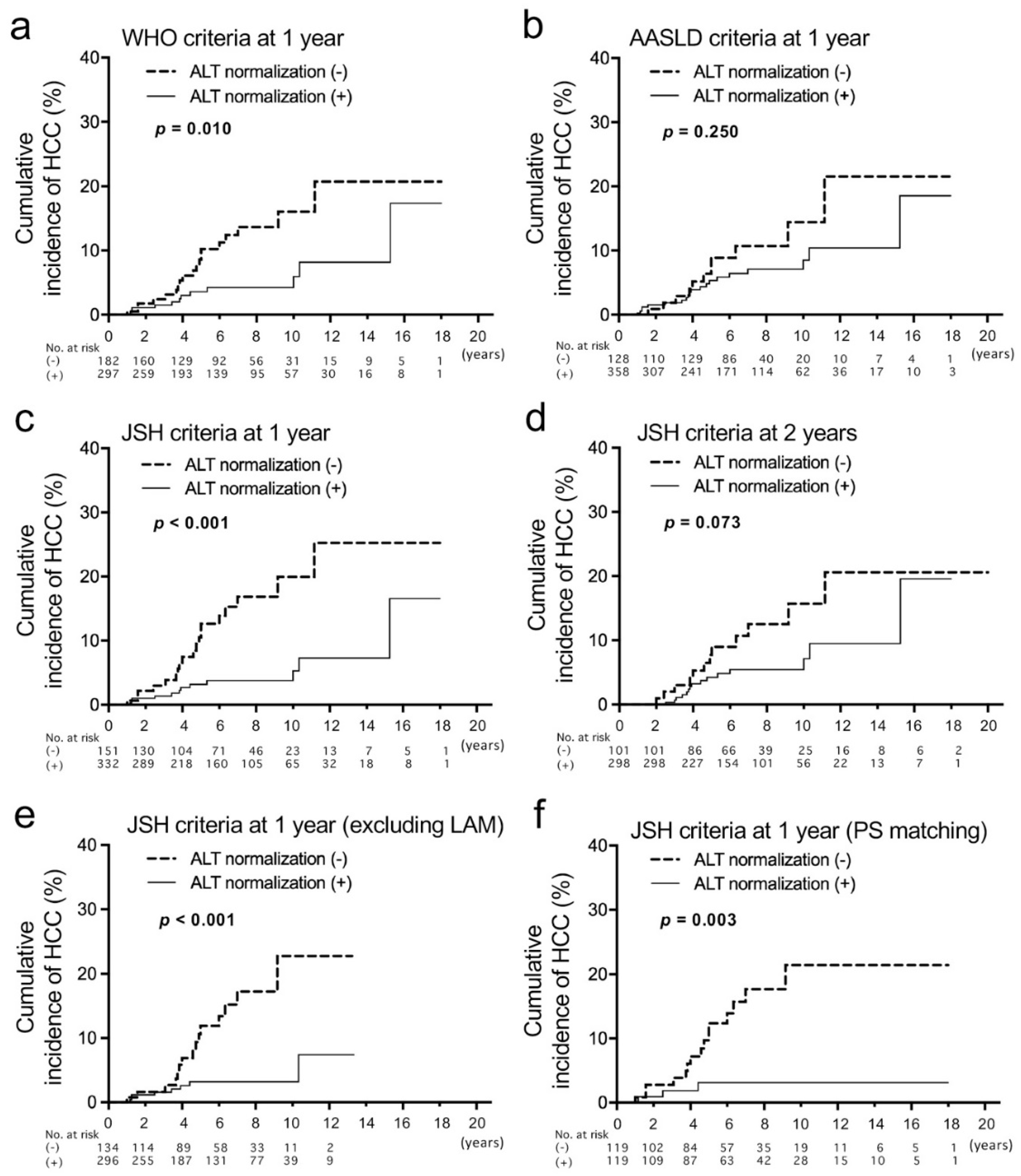
3.3. Evaluation of ALT Normalization after NAs
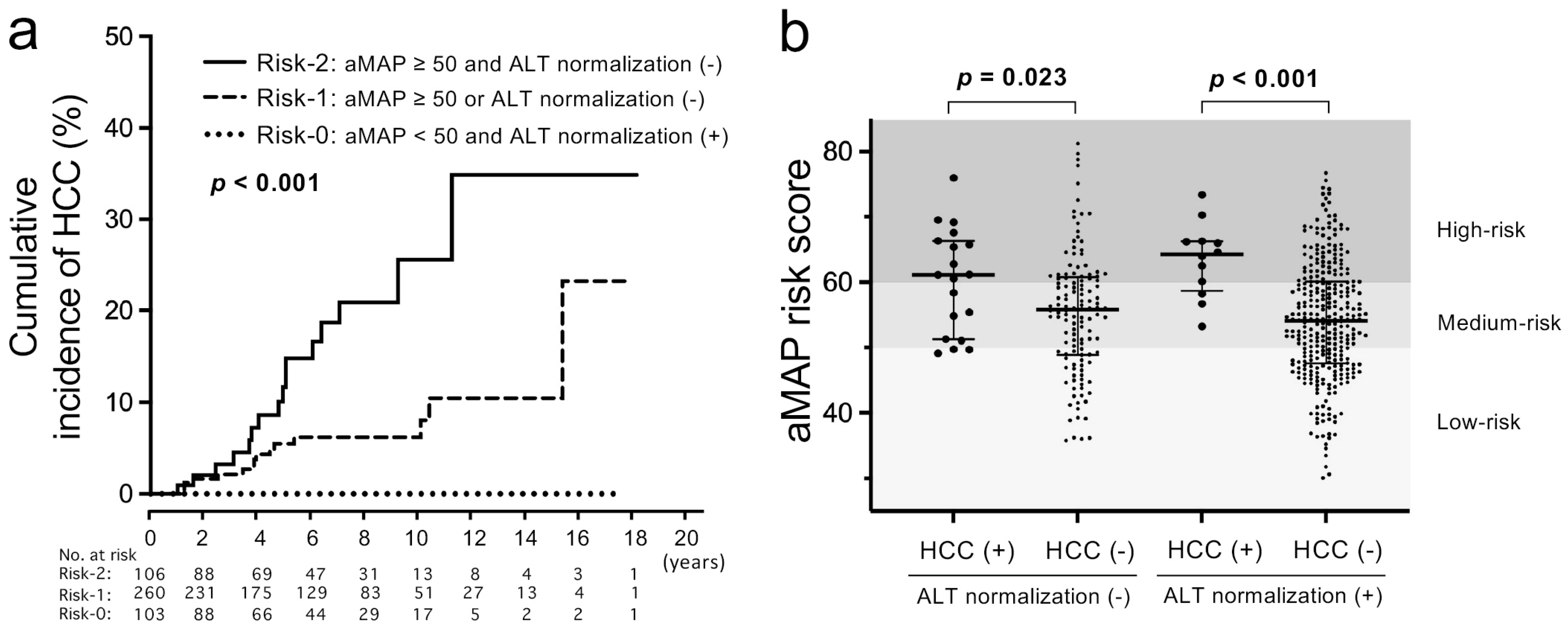
3.4. Combination of aMAP Risk Score and ALT Normalization
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Hepatitis B. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-b (accessed on 12 March 2022).
- Hosaka, T.; Suzuki, F.; Kobayashi, M.; Seko, Y.; Kawamura, Y.; Sezaki, H.; Akuta, N.; Suzuki, Y.; Saitoh, S.; Arase, Y.; et al. Long-term entecavir treatment reduces hepatocellular carcinoma incidence in patients with hepatitis B virus infection. Hepatology 2013, 58, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Su, T.H.; Hu, T.H.; Chen, C.Y.; Huang, Y.H.; Chuang, W.L.; Lin, C.C.; Wang, C.C.; Su, W.W.; Chen, M.Y.; Peng, C.Y.; et al. Four-year entecavir therapy reduces hepatocellular carcinoma, cirrhotic events and mortality in chronic hepatitis B patients. Liver Int. 2016, 36, 1755–1764. [Google Scholar] [CrossRef] [PubMed]
- Yip, T.C.; Lai, J.C.; Wong, G.L. Secondary prevention for hepatocellular carcinoma in patients with chronic hepatitis B: Are all the nucleos(t)ide analogues the same? J. Gastroenterol. 2020, 55, 1023–1036. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.S.J.; Tonthat, A.; Janssen, H.L.A.; Terrault, N.A. Aiming for Functional Cure with Established and Novel Therapies for Chronic Hepatitis B. Hepatol. Commun. 2021. [Google Scholar] [CrossRef]
- Inoue, J.; Akahane, T.; Kobayashi, T.; Obara, N.; Umetsu, T.; Kakazu, E.; Ninomiya, M.; Iwata, T.; Sano, A.; Tsuruoka, M.; et al. Switching to tenofovir disoproxil fumarate in entecavir-treated chronic hepatitis B patients: A pilot randomized controlled study. Biomed. Rep. 2021, 14, 20. [Google Scholar] [CrossRef]
- Kao, J.H.; Jeng, W.J.; Ning, Q.; Su, T.H.; Tseng, T.C.; Ueno, Y.; Yuen, M.F. APASL guidance on stopping nucleos(t)ide analogues in chronic hepatitis B patients. Hepatol. Int. 2021, 15, 833–851. [Google Scholar] [CrossRef]
- Inoue, J.; Ninomiya, M.; Shimosegawa, T.; McNiven, M.A. Cellular membrane trafficking machineries used by the hepatitis viruses. Hepatology 2018, 68, 751–762. [Google Scholar] [CrossRef]
- Martinez, M.G.; Testoni, B.; Zoulim, F. Biological basis for functional cure of chronic hepatitis B. J. Viral Hepat. 2019, 26, 786–794. [Google Scholar] [CrossRef]
- Vittal, A.; Sharma, D.; Hu, A.; Majeed, N.A.; Terry, N.; Auh, S.; Ghany, M.G. Systematic review with meta-analysis: The impact of functional cure on clinical outcomes in patients with chronic hepatitis B. Aliment. Pharmacol. Ther. 2022, 55, 8–25. [Google Scholar] [CrossRef]
- Inoue, J.; Akahane, T.; Nakayama, H.; Kimura, O.; Kobayashi, T.; Kisara, N.; Sato, T.; Morosawa, T.; Izuma, M.; Kakazu, E.; et al. Comparison of hepatitis B virus genotypes B and C among chronically hepatitis B virus-infected patients who received nucleos(t)ide analogs: A multicenter retrospective study. Hepatol. Res. 2019, 49, 1263–1274. [Google Scholar] [CrossRef]
- Orito, E.; Hasebe, C.; Kurosaki, M.; Osaki, Y.; Joko, K.; Watanabe, H.; Kimura, H.; Nishijima, N.; Kusakabe, A.; Izumi, N.; et al. Risk of hepatocellular carcinoma in cirrhotic hepatitis B virus patients during nucleoside/nucleotide analog therapy. Hepatol. Res. 2015, 45, 872–879. [Google Scholar] [CrossRef] [PubMed]
- Pandyarajan, V.; Govalan, R.; Yang, J.D. Risk Factors and Biomarkers for Chronic Hepatitis B Associated Hepatocellular Carcinoma. Int. J. Mol. Sci. 2021, 22, 479. [Google Scholar] [CrossRef] [PubMed]
- Wong, V.W.; Janssen, H.L. Can we use HCC risk scores to individualize surveillance in chronic hepatitis B infection? J. Hepatol. 2015, 63, 722–732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.H.; Kim, Y.D.; Lee, M.; Jun, B.G.; Kim, T.S.; Suk, K.T.; Kang, S.H.; Kim, M.Y.; Cheon, G.J.; Kim, D.J.; et al. Modified PAGE-B score predicts the risk of hepatocellular carcinoma in Asians with chronic hepatitis B on antiviral therapy. J. Hepatol. 2018, 69, 1066–1073. [Google Scholar] [CrossRef]
- Fan, R.; Papatheodoridis, G.; Sun, J.; Innes, H.; Toyoda, H.; Xie, Q.; Mo, S.; Sypsa, V.; Guha, I.N.; Kumada, T.; et al. aMAP risk score predicts hepatocellular carcinoma development in patients with chronic hepatitis. J. Hepatol. 2020, 73, 1368–1378. [Google Scholar] [CrossRef]
- Yotsuyanagi, H.; Takano, T.; Tanaka, M.; Amano, K.; Imamura, M.; Ogawa, K.; Yasunaka, T.; Yasui, Y.; Hayashi, K.; Tanaka, Y.; et al. Hepatitis B virus-related hepatocellular carcinoma in young adults: Efficacy of nationwide selective vaccination. Hepatol. Res. 2020, 50, 182–189. [Google Scholar] [CrossRef]
- Kawai-Kitahata, F.; Asahina, Y.; Tanaka, S.; Kakinuma, S.; Murakawa, M.; Nitta, S.; Watanabe, T.; Otani, S.; Taniguchi, M.; Goto, F.; et al. Comprehensive analyses of mutations and hepatitis B virus integration in hepatocellular carcinoma with clinicopathological features. J. Gastroenterol. 2016, 51, 473–486. [Google Scholar] [CrossRef]
- Inoue, J.; Sato, K.; Ninomiya, M.; Masamune, A. Envelope Proteins of Hepatitis B Virus: Molecular Biology and Involvement in Carcinogenesis. Viruses 2021, 13, 1124. [Google Scholar] [CrossRef]
- Wong, G.L.; Chan, H.L.; Tse, Y.K.; Yip, T.C.; Lam, K.L.; Lui, G.C.; Wong, V.W. Normal on-treatment ALT during antiviral treatment is associated with a lower risk of hepatic events in patients with chronic hepatitis B. J. Hepatol. 2018, 69, 793–802. [Google Scholar] [CrossRef]
- Choi, J.; Kim, G.A.; Han, S.; Lim, Y.S. Earlier Alanine Aminotransferase Normalization During Antiviral Treatment Is Independently Associated With Lower Risk of Hepatocellular Carcinoma in Chronic Hepatitis B. Am. J. Gastroenterol. 2020, 115, 406–414. [Google Scholar] [CrossRef]
- Kim, S.; Lee, Y.; Bang, S.M.; Bak, H.; Yim, S.Y.; Lee, Y.S.; Yoo, Y.J.; Jung, Y.K.; Kim, J.H.; Seo, Y.S.; et al. Early Normalization of Alanine Aminotransferase during Antiviral Therapy Reduces Risk of Hepatocellular Carcinoma in HBV Patients. J. Clin. Med. 2021, 10, 1840. [Google Scholar] [CrossRef] [PubMed]
- Vallet-Pichard, A.; Mallet, V.; Nalpas, B.; Verkarre, V.; Nalpas, A.; Dhalluin-Venier, V.; Fontaine, H.; Pol, S. FIB-4: An inexpensive and accurate marker of fibrosis in HCV infection. comparison with liver biopsy and fibrotest. Hepatology 2007, 46, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.Q.; Hoang, J.K.; Leong, J.; Riveiro-Barciela, M.; Maeda, M.; Yang, J.D.; Accarino, E.V.; Thin, K.; Trinh, L.; Cheung, R.C.; et al. Differential characteristics and outcomes of Asian and non-Asian patients with HBV-related hepatocellular carcinoma. Liver Int. 2021, 41, 1922–1932. [Google Scholar] [CrossRef] [PubMed]
- Prati, D.; Taioli, E.; Zanella, A.; Della Torre, E.; Butelli, S.; Del Vecchio, E.; Vianello, L.; Zanuso, F.; Mozzi, F.; Milani, S.; et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann. Intern. Med. 2002, 137, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Wong, G.L.; Chan, H.L.; Yu, Z.; Chan, A.W.; Choi, P.C.; Chim, A.M.; Chan, H.Y.; Tse, C.H.; Wong, V.W. Coincidental metabolic syndrome increases the risk of liver fibrosis progression in patients with chronic hepatitis B--a prospective cohort study with paired transient elastography examinations. Aliment. Pharmacol. Ther. 2014, 39, 883–893. [Google Scholar] [CrossRef]
- Van Kleef, L.A.; Ayada, I.; Alferink, L.J.M.; Pan, Q.; de Knegt, R.J. Metabolic dysfunction-associated fatty liver disease improves detection of high liver stiffness: The Rotterdam Study. Hepatology 2022, 75, 419–429. [Google Scholar] [CrossRef]
- Van Kleef, L.A.; Choi, H.S.J.; Brouwer, W.P.; Hansen, B.E.; Patel, K.; de Man, R.A.; Janssen, H.L.A.; de Knegt, R.J.; Sonneveld, M.J. Metabolic dysfunction-associated fatty liver disease increases risk of adverse outcomes in patients with chronic hepatitis B. JHEP Rep. 2021, 3, 100350. [Google Scholar] [CrossRef]
- Li, J.; Yang, H.I.; Yeh, M.L.; Le, M.H.; Le, A.K.; Yeo, Y.H.; Dai, C.Y.; Barnett, S.; Zhang, J.Q.; Huang, J.F.; et al. Association Between Fatty Liver and Cirrhosis, Hepatocellular Carcinoma, and Hepatitis B Surface Antigen Seroclearance in Chronic Hepatitis B. J. Infect. Dis. 2021, 224, 294–302. [Google Scholar] [CrossRef]
- Mak, L.Y.; Hui, R.W.; Fung, J.; Liu, F.; Wong, D.K.; Cheung, K.S.; Yuen, M.F.; Seto, W.K. Diverse effects of hepatic steatosis on fibrosis progression and functional cure in virologically quiescent chronic hepatitis B. J. Hepatol. 2020, 73, 800–806. [Google Scholar] [CrossRef]
- Liang, Y.J.; Teng, W.; Chen, C.L.; Sun, C.P.; Teng, R.D.; Huang, Y.H.; Liang, K.H.; Chen, Y.W.; Lin, C.C.; Su, C.W.; et al. Clinical Implications of HBV PreS/S Mutations and the Effects of PreS2 Deletion on Mitochondria, Liver Fibrosis, and Cancer Development. Hepatology 2021, 74, 641–655. [Google Scholar] [CrossRef]
- Lin, Y.T.; Jeng, L.B.; Chan, W.L.; Su, I.J.; Teng, C.F. Hepatitis B Virus Pre-S Gene Deletions and Pre-S Deleted Proteins: Clinical and Molecular Implications in Hepatocellular Carcinoma. Viruses 2021, 13, 862. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.F.; Jang, T.Y.; Jun, D.W.; Ahn, S.B.; An, J.; Enomoto, M.; Takahashi, H.; Ogawa, E.; Yoon, E.; Jeong, S.W.; et al. On-treatment gamma-glutamyl transferase predicts the development of hepatocellular carcinoma in chronic hepatitis B patients. Liver Int. 2022, 42, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Corti, A.; Belcastro, E.; Dominici, S.; Maellaro, E.; Pompella, A. The dark side of gamma-glutamyltransferase (GGT): Pathogenic effects of an ‘antioxidant’ enzyme. Free Radic. Biol. Med. 2020, 160, 807–819. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.L.; Wang, Y.J.; Kao, W.Y.; Chen, P.H.; Huo, T.I.; Huang, Y.H.; Lan, K.H.; Su, C.W.; Chan, W.L.; Lin, H.C.; et al. Inverse association between hepatitis B virus infection and fatty liver disease: A large-scale study in populations seeking for check-up. PLoS ONE 2013, 8, e72049. [Google Scholar] [CrossRef]
- Joo, E.J.; Chang, Y.; Yeom, J.S.; Ryu, S. Hepatitis B virus infection and decreased risk of nonalcoholic fatty liver disease: A cohort study. Hepatology 2017, 65, 828–835. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Pan, Q.; Duan, X.Y.; Liu, Q.; Mo, G.Y.; Rao, G.R.; Fan, J.G. Fatty liver reduces hepatitis B virus replication in a genotype B hepatitis B virus transgenic mice model. J. Gastroenterol. Hepatol. 2012, 27, 1858–1864. [Google Scholar] [CrossRef]
- Ito, K.; Yotsuyanagi, H.; Sugiyama, M.; Yatsuhashi, H.; Karino, Y.; Takikawa, Y.; Saito, T.; Arase, Y.; Imazeki, F.; Kurosaki, M.; et al. Geographic distribution and characteristics of genotype A hepatitis B virus infection in acute and chronic hepatitis B patients in Japan. J. Gastroenterol. Hepatol. 2016, 31, 180–189. [Google Scholar] [CrossRef]
- Moini, M.; Fung, S. HBsAg Loss as a Treatment Endpoint for Chronic HBV Infection: HBV Cure. Viruses 2022, 14, 657. [Google Scholar] [CrossRef]
- Liang, L.Y.; Wong, V.W.; Toyoda, H.; Tse, Y.K.; Yip, T.C.; Yuen, B.W.; Tada, T.; Kumada, T.; Lee, H.W.; Lui, G.C.; et al. Serum hepatitis B core-related antigen predicts hepatocellular carcinoma in hepatitis B e antigen-negative patients. J. Gastroenterol. 2020, 55, 899–908. [Google Scholar] [CrossRef]
- Kaneko, S.; Kurosaki, M.; Inada, K.; Kirino, S.; Hayakawa, Y.; Yamashita, K.; Osawa, L.; Sekiguchi, S.; Higuchi, M.; Takaura, K.; et al. Hepatitis B core-related antigen predicts disease progression and hepatocellular carcinoma in hepatitis B e antigen-negative chronic hepatitis B patients. J. Gastroenterol. Hepatol. 2021, 36, 2943–2951. [Google Scholar] [CrossRef]
- Hosaka, T.; Suzuki, F.; Kobayashi, M.; Fujiyama, S.; Kawamura, Y.; Sezaki, H.; Akuta, N.; Kobayashi, M.; Suzuki, Y.; Saitoh, S.; et al. Ultrasensitive Assay for Hepatitis B Core-Related Antigen Predicts Hepatocellular Carcinoma Incidences during Entecavir. Hepatol. Commun. 2022, 6, 36–49. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, F.; Hosaka, T.; Imaizumi, M.; Kobayashi, M.; Ohue, C.; Suzuki, Y.; Fujiyama, S.; Kawamura, Y.; Sezaki, H.; Akuta, N.; et al. Potential of ultra-highly sensitive immunoassays for hepatitis B surface and core-related antigens in patients with or without development of hepatocellular carcinoma after hepatitis B surface antigen seroclearance. Hepatol. Res. 2021, 51, 426–435. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Parameter | Total (n = 611) | HCC (−) (n = 563) | HCC (+) (n = 48) | p-Value * |
|---|---|---|---|---|
| Age (years) | 53 (42–62) | 51 (42–61) | 58 (52–64) | 0.001 |
| Sex (male/female) | 390/221 | 349/214 | 41/7 | <0.001 |
| Previous IFN (+/−) | 84/527 | 76/487 | 8/40 | 0.551 |
| DM (+/−) | 35/576 | 29/534 | 6/42 | 0.035 |
| T-Bil (mg/dL) | 0.8 (0.1–1.1) | 0.8 (0.6–1.1) | 0.8 (0.7–1.4) | 0.008 |
| AST (U/L) | 49 (34–91) | 47 (33–90) | 57 (41–131) | 0.107 |
| ALT (U/L) | 63 (39–129) | 64 (39–130) | 53 (38–114) | 0.764 |
| Alb (g/dL) | 4.2 (3.9–4.4) | 4.2 (3.9–4.5) | 3.9 (3.4–4.2) | <0.001 |
| Cr (mg/dL) | 0.72 (0.65–0.84) | 0.72 (0.64–0.84) | 0.78 (0.70–0.86) | 0.145 |
| PLT (×104/μL) | 17.3 (13.4–21.9) | 17.8 (14.0–22.1) | 12.3 (9.4–16.2) | <0.001 |
| AFP (ng/mL) | 4.5 (3.0–9.3) | 4.1 (3.0–8.2) | 13.5 (6.3–32.6) | <0.001 |
| HBV DNA (log IU/mL) | 5.7 (4.6–7.0) | 5.7 (4.6–7.0) | 6.1 (5.1–7.1) | 0.368 |
| HBsAg (IU/mL) | 940 (162–2875) | 840 (148–2910) | 1372 (570–1881) | 0.542 |
| HBeAg (+/−) † | 202/331 | 191/302 | 11/29 | 0.159 |
| HBcrAg (log U/mL) | 4.3 (3.0–6.5) | 4.4 (3.0–6.6) | 3.0 (3.0–5.2) | 0.175 |
| FIB-4 index | 2.00 (1.25–3.13) | 1.89 (1.21–2.94) | 3.07 (2.11–5.63) | <0.001 |
| aMAP risk (low/medium/high) † | 171/225/169 | 167/215/141 | 4/10/28 | <0.001 |
| HBV genotype (A/B/C/D) † | 5/187/334/2 | 5/176/305/2 | 0/11/29/0 | 0.477 |
| Initial NA (LAM/ETV/TDF/TAF) | 95/434/47/35 | 80/403/46/34 | 15/31/1/1 | 0.010 |
| Observation period (months) | 72 (36–110) | 72 (36–108) | 100 (64–141) | <0.001 |
| Factor | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| p-Value * | HR (95% CI) | p-Value * | HR (95% CI) | |
| Male | 0.003 | 3.32 (1.49–7.40) | 0.009 | 6.91 (1.63–29.23) |
| Age ≥ 48 | <0.001 | 5.04 (1.99–12.87) | 0.014 | 3.99 (1.33–11.94) |
| DM | 0.067 | 2.23 (0.95–5.27) | ||
| Alb < 4.0 | 0.001 | 2.76 (1.48–5.15) | 0.116 | 1.98 (0.85–4.62) |
| PLT < 15.0 | <0.001 | 4.59 (2.49–8.46) | 0.015 | 3.03 (1.24–7.43) |
| AFP ≥ 5.5 | <0.001 | 6.28 (2.42–16.26) | 0.013 | 4.40 (1.36–14.20) |
| HBeAg (+) | 0.156 | 1.65 (0.83–3.31) | ||
| FIB-4 ≥ 2.5 | <0.001 | 3.64 (1.91–6.91) | N/A | N/A |
| aMAP medium or high | 0.007 | 4.12 (1.47–11.54) | N/A | N/A |
| HBV genotype C | 0.527 | 1.25 (0.62–2.52) | ||
| HBV DNA (+) at 1 year | 0.824 | 1.09 (0.51–2.30) | ||
| Abnormal ALT at 1 year | ||||
| WHO criteria | 0.007 | 2.45 (1.28–4.69) | N/A | N/A |
| AASLD criteria | 0.283 | 1.44 (0.74–2.82) | ||
| JSH criteria | <0.001 | 3.39 (1.77–6.50) | 0.007 | 2.89 (1.33–6.26) |
| Parameter | ALT ≤ 30 at 1 Year (n = 337) | ALT > 30 at 1 Year (n = 156) | p-Value * |
|---|---|---|---|
| Age (years) | 54 (43–63) | 51 (41–61) | 0.132 |
| Sex (male/female) | 197/140 | 121/35 | <0.001 |
| Previous IFN (+/−) | 37/300 | 16/140 | 0.801 |
| DM (+/−) | 14/323 | 12/144 | 0.102 |
| T-Bil (mg/dL) | 0.8 (0.6–1.0) | 0.8 (0.6–1.1) | 0.088 |
| AST (U/L) | 50 (33–98) | 45 (33–70) | 0.288 |
| ALT (U/L) | 69 (36–140) | 57 (42–96) | 0.236 |
| Alb (g/dL) | 4.2 (3.9–4.4) | 4.2 (3.9–4.5) | 0.330 |
| Cr (mg/dL) | 0.70 (0.60–0.82) | 0.79 (0.70–0.87) | 0.002 |
| PLT (×104/μL) | 18.4 (14.5–22.4) | 16.2 (12.4–21.8) | 0.023 |
| AFP (ng/mL) | 4.3 (3.0–8.5) | 5.5 (3.1–11.1) | 0.346 |
| HBV DNA (log IU/mL) | 5.8 (4.6–7.1) | 5.4 (4.0–6.5) | 0.044 |
| HBsAg (IU/mL) | 978 (198–2851) | 928 (145–3262) | 0.833 |
| HBeAg (+/−) † | 104/182 | 49/87 | 0.989 |
| HBcrAg (log U/mL) | 4.3 (3.0–6.6) | 4.3 (3.0–6.0) | 0.564 |
| FIB-4 index | 1.97 (1.25–3.21) | 2.05 (1.29–2.98) | 0.981 |
| aMAP risk (low/medium/high) † | 104/131/92 | 42/60/50 | 0.499 |
| HBV genotype (A/B/C/D) † | 3/115/171/0 | 2/45/96/2 | 0.063 |
| Initial NA (LAM/ETV/TDF/TAF) | 36/255/23/23 | 17/116/13/10 | 0.944 |
| Observation period (months) | 63 (36–108) | 72 (36–108) | 0.332 |
| Factor | Category | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|---|
| p-Value * | OR (95% CI) | p-Value * | OR (95% CI) | ||
| Sex | Male | <0.001 | 2.46 (1.59–3.79) | <0.001 | 2.36 (1.45–3.84) |
| DM | Presence | 0.112 | 1.92 (0.87–4.26) | ||
| T-bil | By 1.0 mg/dL up | 0.440 | 1.10 (0.87–1.40) | ||
| Cr | By 1.0 mg/dL up | 0.487 | 0.91 (0.67–1.22) | ||
| PLT | By 1.0×104/μL up | 0.048 | 0.97 (0.94–1.00) | 0.180 | 0.98 (0.95–1.01) |
| HBV DNA | By 1.0 log IU/mL up | 0.031 | 0.87 (0.78–0.99) | 0.016 | 0.86 (0.76–0.97) |
| HBV genotype | C | 0.153 | 1.35 (0.89–2.05) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inoue, J.; Kobayashi, T.; Akahane, T.; Kimura, O.; Sato, K.; Ninomiya, M.; Iwata, T.; Takai, S.; Kisara, N.; Sato, T.; et al. Non-Achievement of Alanine Aminotransferase Normalization Associated with the Risk of Hepatocellular Carcinoma during Nucleos(t)ide Analogue Therapies: A Multicenter Retrospective Study. J. Clin. Med. 2022, 11, 2354. https://doi.org/10.3390/jcm11092354
Inoue J, Kobayashi T, Akahane T, Kimura O, Sato K, Ninomiya M, Iwata T, Takai S, Kisara N, Sato T, et al. Non-Achievement of Alanine Aminotransferase Normalization Associated with the Risk of Hepatocellular Carcinoma during Nucleos(t)ide Analogue Therapies: A Multicenter Retrospective Study. Journal of Clinical Medicine. 2022; 11(9):2354. https://doi.org/10.3390/jcm11092354
Chicago/Turabian StyleInoue, Jun, Tomoo Kobayashi, Takehiro Akahane, Osamu Kimura, Kosuke Sato, Masashi Ninomiya, Tomoaki Iwata, Satoshi Takai, Norihiro Kisara, Toshihiro Sato, and et al. 2022. "Non-Achievement of Alanine Aminotransferase Normalization Associated with the Risk of Hepatocellular Carcinoma during Nucleos(t)ide Analogue Therapies: A Multicenter Retrospective Study" Journal of Clinical Medicine 11, no. 9: 2354. https://doi.org/10.3390/jcm11092354
APA StyleInoue, J., Kobayashi, T., Akahane, T., Kimura, O., Sato, K., Ninomiya, M., Iwata, T., Takai, S., Kisara, N., Sato, T., Nagasaki, F., Miura, M., Nakamura, T., Umetsu, T., Sano, A., Tsuruoka, M., Onuki, M., Niitsuma, H., Masamune, A., & THERME Study Group. (2022). Non-Achievement of Alanine Aminotransferase Normalization Associated with the Risk of Hepatocellular Carcinoma during Nucleos(t)ide Analogue Therapies: A Multicenter Retrospective Study. Journal of Clinical Medicine, 11(9), 2354. https://doi.org/10.3390/jcm11092354