
Intraoperative Quantification of MDS-UPDRS Tremor Measurements Using 3D Accelerometry: A Pilot Study

 ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
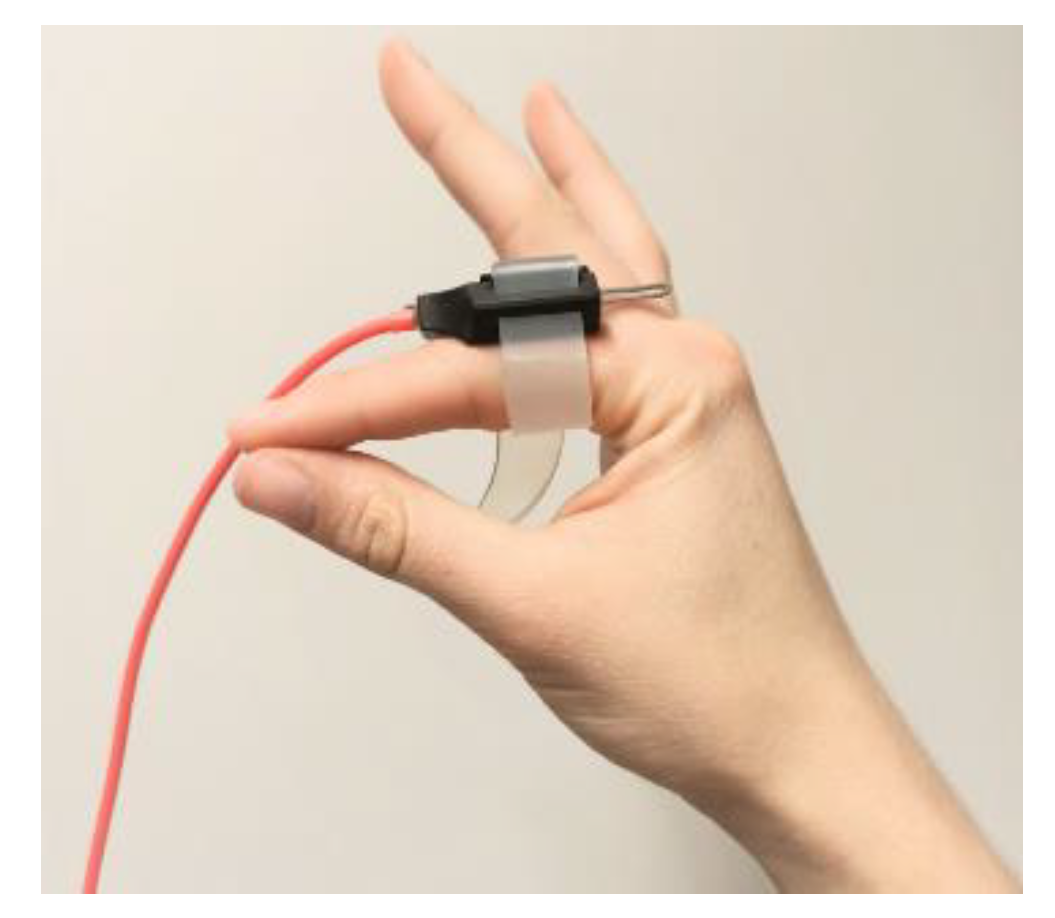
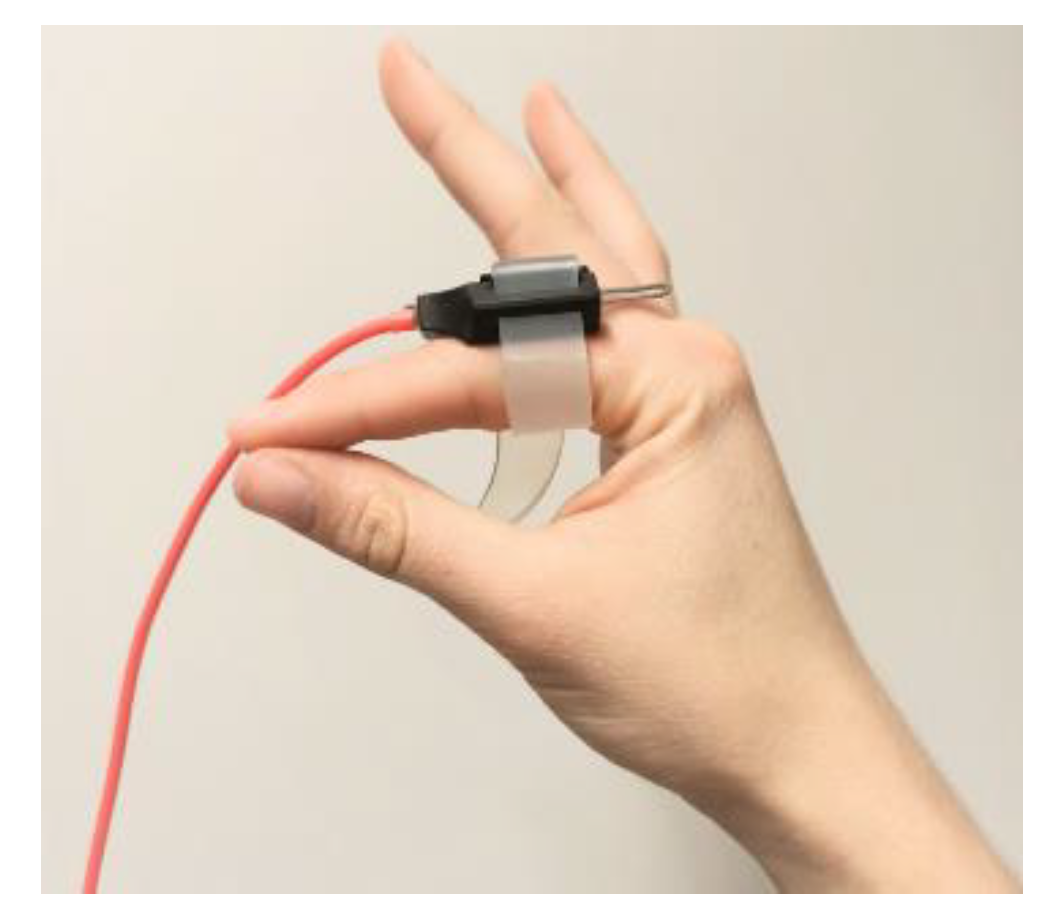
2.2. Materials
2.3. Measurements
2.4. Data Pre-Processing
2.5. Accelerometry Measures
2.6. Objective MDS-UPDRS Scores
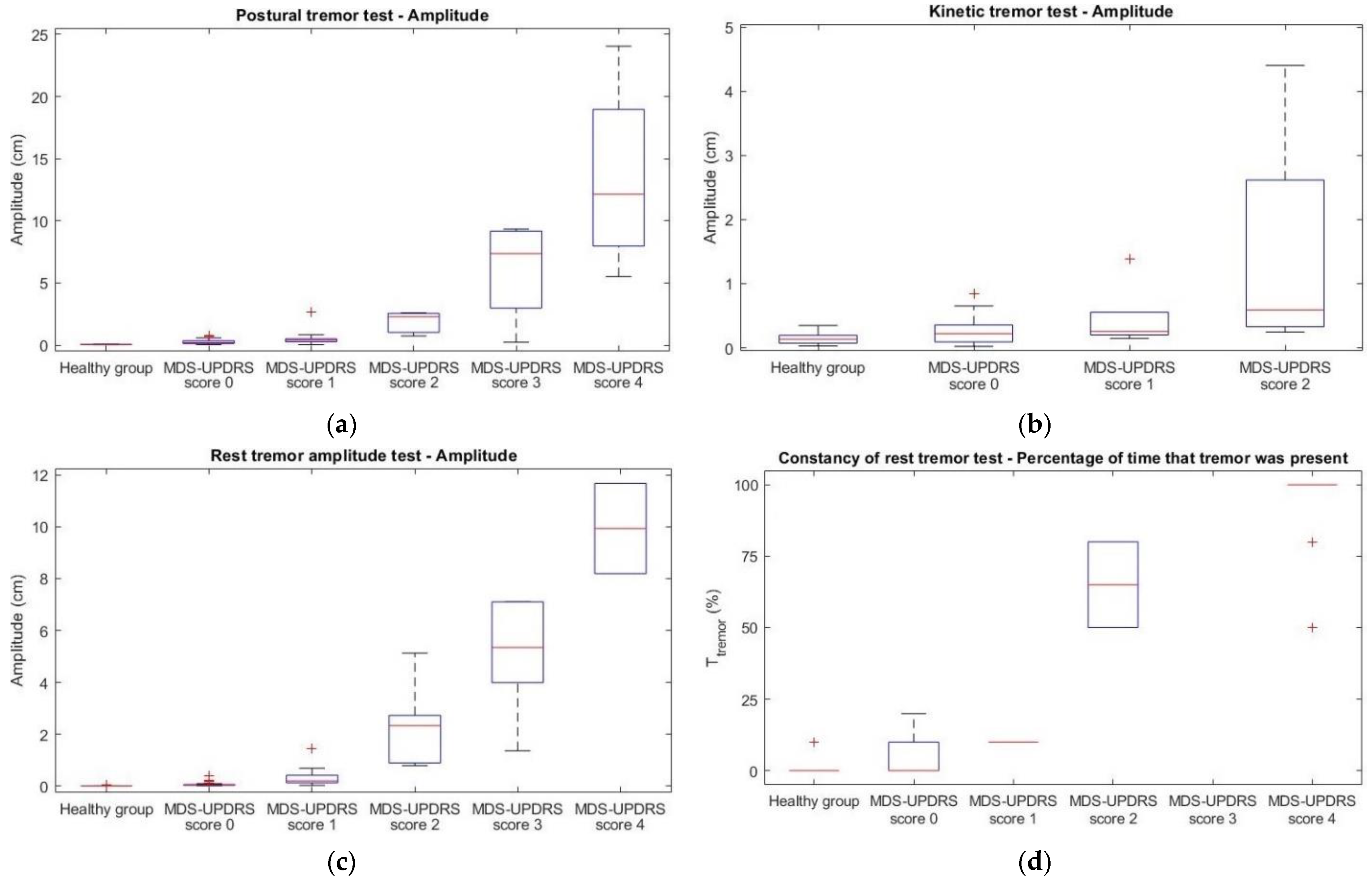
2.6.1. Postural, Kinetic and Rest Tremor Amplitude
2.6.2. Constancy of Rest Tremor
2.7. Statistical Analysis
3. Results
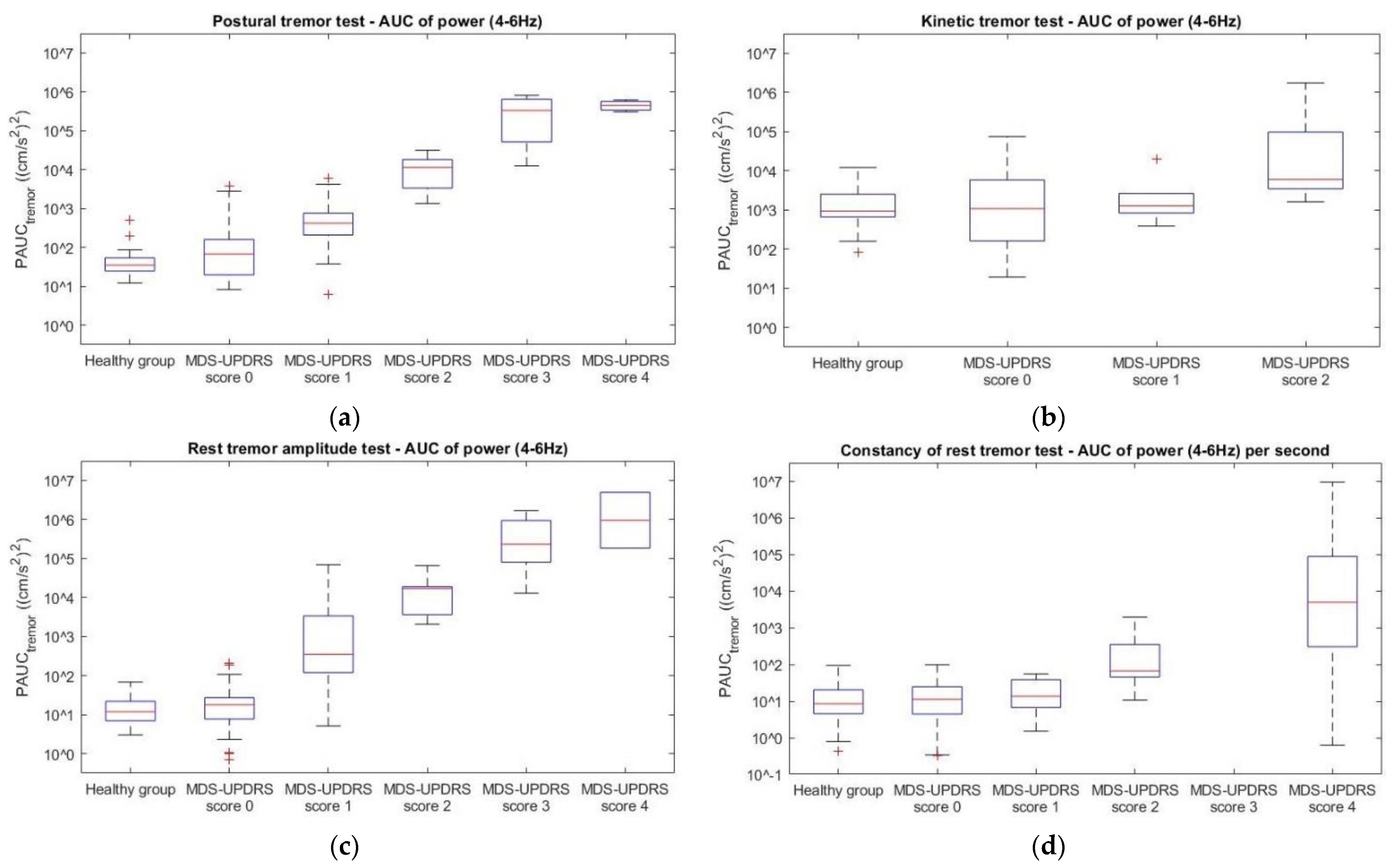
3.1. Accelerometry Measures
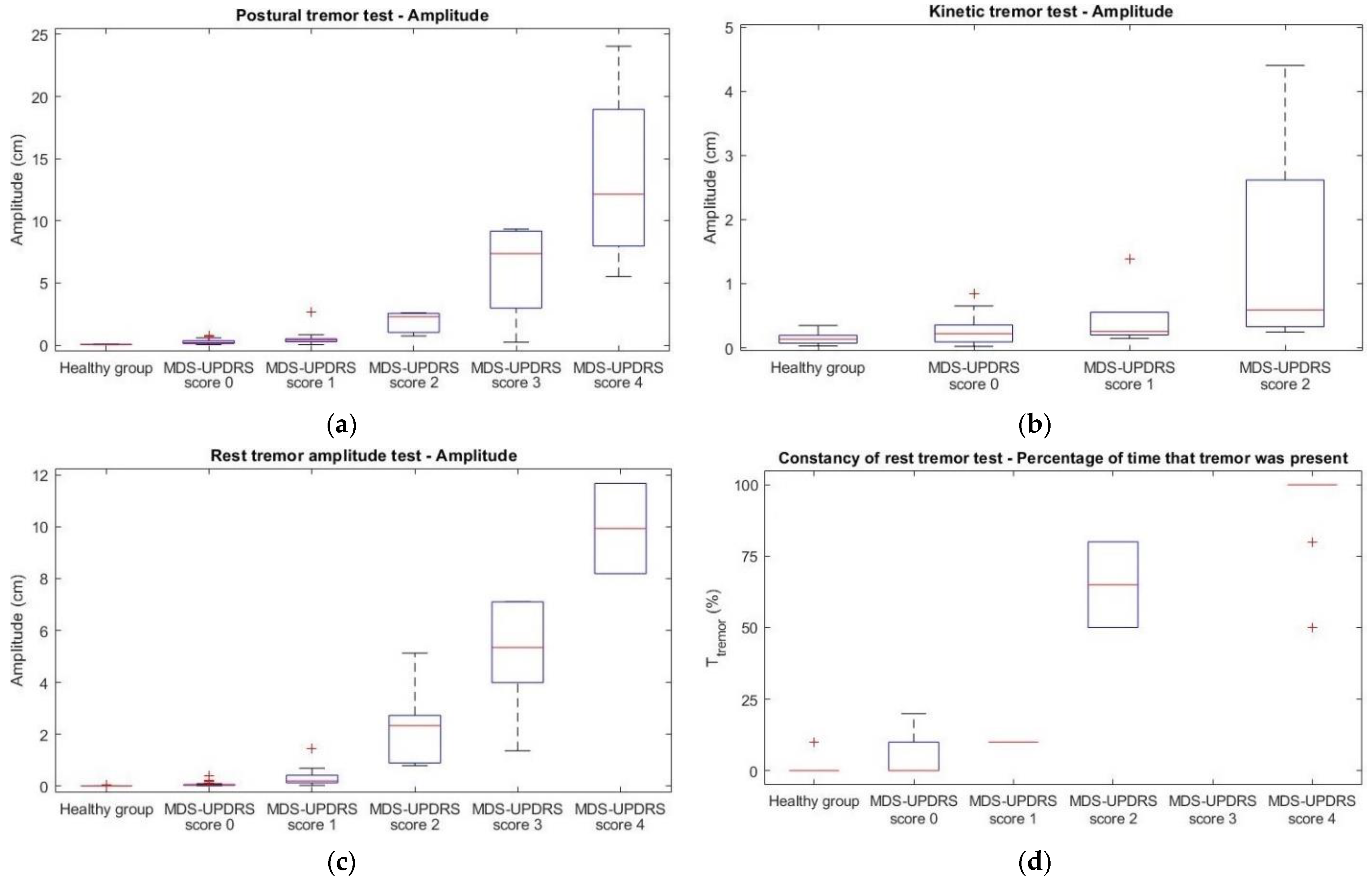
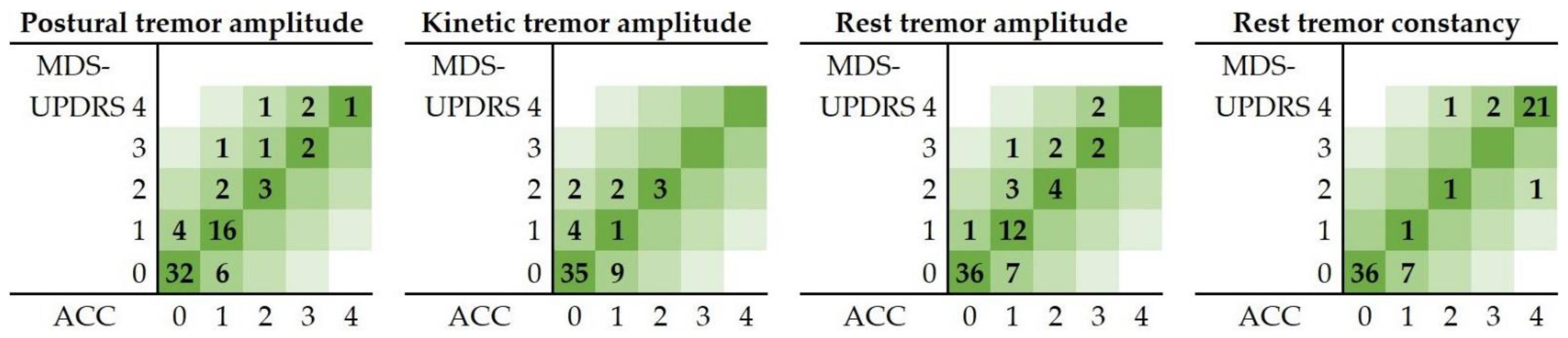
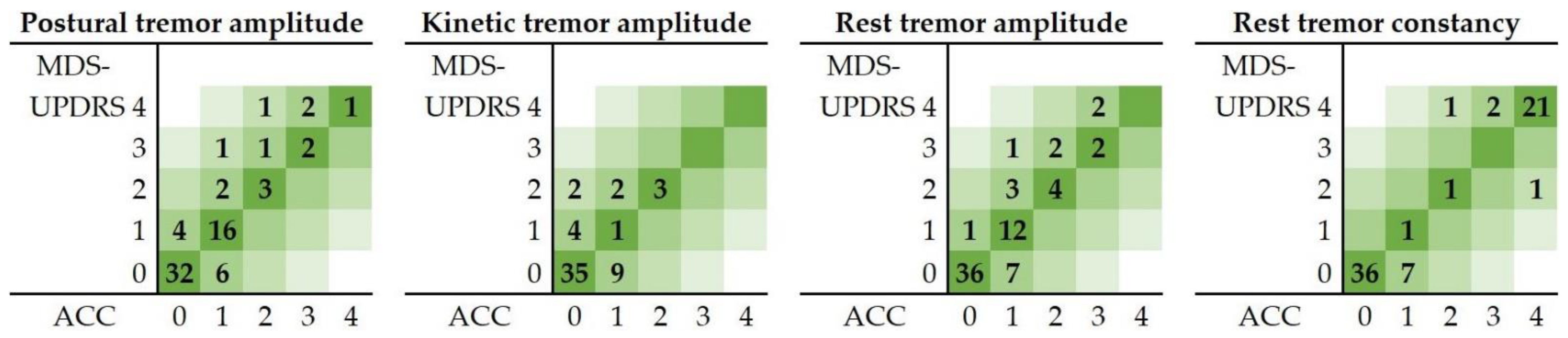
3.2. Objective MDS-UPDRS Scores
4. Discussion
4.1. Contributions
4.2. Accelerometry Measures
4.3. Objective MDS-UPDRS Scores
4.4. Inconsistencies
4.5. Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tysnes, O.B.; Storstein, A. Epidemiology of Parkinson’s Disease. J. Neural. Transm. 2017, 124, 901–905. [Google Scholar] [CrossRef]
- Galperin, I.; Hillel, I.; del Din, S.; Bekkers, E.M.J.; Nieuwboer, A.; Abbruzzese, G.; Avanzino, L.; Nieuwhof, F.; Bloem, B.R.; Rochester, L.; et al. Associations between Daily-Living Physical Activity and Laboratory-Based Assessments of Motor Severity in Patients with Falls and Parkinson’s Disease. Parkinsonism. Relat. Disord. 2019, 62, 85–90. [Google Scholar] [CrossRef]
- Dorsey, E.R.; Sherer, T.; Okun, M.S.; Bloem, B.R. The Emerging Evidence of the Parkinson Pandemic. J. Parkinsons. Dis. 2018, 8, S3–S8. [Google Scholar] [CrossRef] [Green Version]
- Jankovic, J. Parkinson’s Disease: Clinical Features and Diagnosis. J. Neurol. Neurosurg. Psychiatr. 2008, 79, 368–376. [Google Scholar] [CrossRef] [Green Version]
- Vaillancourt, D.E.; Newell, K.M. The Dynamics of Resting and Postural Tremor in Parkinson’s Disease. Clin. Neurophysiol. 2000, 111, 2046–2056. [Google Scholar] [CrossRef]
- Kalia, L.; Lang, A.E. Parkinson’s Disease. Lancet 2015, 386, 896–912. [Google Scholar] [CrossRef]
- Van der Stouwe, A.M.M.; Elting, J.W.; van der Hoeven, J.H.; van Laar, T.; Leenders, K.L.; Maurits, N.M.; Tijssen, M.A.J. How Typical Are ‘Typical’ Tremor Characteristics? Sensitivity and Specificity of Five Tremor Phenomena. Parkinsonism. Relat. Disord. 2016, 30, 23–28. [Google Scholar] [CrossRef]
- Erb, M.K.; Karlin, D.R.; Ho, B.K.; Thomas, K.C.; Parisi, F.; Vergara-Diaz, G.P.; Daneault, J.F.; Wacnik, P.W.; Zhang, H.; Kangarloo, T.; et al. MHealth and Wearable Technology Should Replace Motor Diaries to Track Motor Fluctuations in Parkinson’s Disease. NPJ Digit. Med. 2020, 3, 6. [Google Scholar] [CrossRef]
- Journee, H.L.; Postma, A.A.; Staal, M.J. Intraoperative Neurophysiological Assessment of Disabling Symptoms in DBS Surgery. Neurophysiol. Clin. 2007, 37, 467–475. [Google Scholar] [CrossRef]
- Shulman, L.M.; Gruber-Baldini, A.L.; Anderson, K.E.; Fishman, P.S.; Reich, S.G.; Weiner, W.J. The Clinically Important Difference on the Unified Parkinson’s Disease Rating Scale. Arch. Neurol. 2010, 67, 64–70. [Google Scholar] [CrossRef] [Green Version]
- Goetz, C.G.; Tilley, B.C.; Shaftman, S.R.; Stebbins, G.T.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stern, M.B.; Dodel, R.; et al. Movement Disorder Society-Sponsored Revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale Presentation and Clinimetric Testing Results. Mov. Disord. 2008, 23, 2129–2170. [Google Scholar] [CrossRef] [PubMed]
- Goetz, C.G.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stebbins, G.T.; Stern, M.B.; Tilley, B.C.; Dodel, R.; Dubois, B.; et al. Movement Disorders Society—Unified Parkinson Disease Rating Scale. Available online: https://www.movementdisorders.org/MDS/MDS-Rating-Scales/MDS-Unified-Parkinsons-Disease-Rating-Scale-MDS-UPDRS.htm (accessed on 1 February 2022).
- Maldonado-Naranjo, A.; Koop, M.M.; Hogue, O.; Alberts, J.; MacHado, A. Kinematic Metrics from a Wireless Stylus Quantify Tremor and Bradykinesia in Parkinson’s Disease. Parkinsons Dis. 2019, 2019, 6850478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, K.H.S.; Chen, R. Invasive and Noninvasive Brain Stimulation in Parkinson’s Disease: Clinical Effects and Future Perspectives. Clin. Pharmacol. Ther. 2019, 106, 763–775. [Google Scholar] [CrossRef] [PubMed]
- Hemm, S.; Wårdell, K. Stereotactic Implantation of Deep Brain Stimulation Electrodes: A Review of Technical Systems, Methods and Emerging Tools. Med. Biol. Eng. Comput. 2010, 48, 611–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruce, B.B.; Foote, K.D.; Rosenbek, J.; Sapienza, C.; Romrell, J.; Crucian, G.; Okun, M.S. Aphasia and Thalamotomy: Important Issues. Stereotact. Funct. Neurosurg. 2004, 82, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.; Coste, J.; Lemaire, J.J.; Taub, E.; Schüpbach, W.M.M.; Pollo, C.; Schkommodau, E.; Guzman, R.; Hemm-Ode, S. Intraoperative Acceleration Measurements to Quantify Improvement in Tremor during Deep Brain Stimulation Surgery. Med. Biol. Eng. Comput. 2017, 55, 845–858. [Google Scholar] [CrossRef] [Green Version]
- Lange, S.F.; Kremer, N.I.; van Laar, T.; Lange, F.; Steendam-Oldekamp, T.E.; Oterdoom, D.L.M.; Absalom, A.R.; van Dijk, J.M.C.; Drost, G. The Intraoperative Microlesion Effect Positively Correlates with the Short-Term Clinical Effect of Deep Brain Stimulation in Parkinson’s Disease. Neuromodulation 2021, in press. [Google Scholar] [CrossRef]
- Lukšys, D.; Jonaitis, G.; Griškevičius, J. Quantitative Analysis of Parkinsonian Tremor in a Clinical Setting Using Inertial Measurement Units. Parkinsons Dis. 2018, 2018, 1683831. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Molinero, A.; Samà, A.; Pérez-López, C.; Rodríguez-Martín, D.; Alcaine, S.; Mestre, B.; Quispe, P.; Giuliani, B.; Vainstein, G.; Browne, P.; et al. Analysis of Correlation between an Accelerometer-Based Algorithm for Detecting Parkinsonian Gait and UPDRS Subscales. Front. Neurol. 2017, 8, 431. [Google Scholar] [CrossRef] [Green Version]
- Post, B.; Merkus, M.P.; de Bie, R.M.A.; de Haan, R.J.; Speelman, J.D. Unified Parkinson’s Disease Rating Scale Motor Examination: Are Ratings of Nurses, Residents in Neurology, and Movement Disorders Specialists Interchangeable? Mov. Disord. 2005, 20, 1577–1584. [Google Scholar] [CrossRef]
- Evers, L.J.W.; Krijthe, J.H.; Meinders, M.J.; Bloem, B.R.; Heskes, T.M. Measuring Parkinson’s Disease over Time: The Real-World within-Subject Reliability of the MDS-UPDRS. Mov. Disord. 2019, 34, 1480–1487. [Google Scholar] [CrossRef] [Green Version]
- Espay, A.J.; Hausdorff, J.M.; Sánchez-Ferro, Á.; Klucken, J.; Merola, A.; Bonato, P.; Paul, S.S.; Horak, F.B.; Vizcarra, J.A.; Mestre, T.A.; et al. A Roadmap for Implementation of Patient-Centered Digital Outcome Measures in Parkinson’s Disease Obtained Using Mobile Health Technologies. Mov. Disord. 2019, 34, 657–663. [Google Scholar] [CrossRef]
- Farzanehfar, P.; Woodrow, H.; Braybrook, M.; McGregor, S.; Evans, A.; Nicklason, F.; Horne, M. Objective Measurement in Routine Care of People with Parkinson’s Disease Improves Outcomes. NPJ Parkinson’s Dis. 2018, 4, 10. [Google Scholar] [CrossRef] [PubMed]
- Hobert, M.A.; Maetzler, W.; Aminian, K.; Chiari, L. Technical and Clinical View on Ambulatory Assessment in Parkinson’s Disease. Acta Neurol. Scand. 2014, 130, 139–147. [Google Scholar] [CrossRef]
- Teshuva, I.; Hillel, I.; Gazit, E.; Giladi, N.; Mirelman, A.; Hausdorff, J.M. Using Wearables to Assess Bradykinesia and Rigidity in Patients with Parkinson’s Disease: A Focused, Narrative Review of the Literature. J. Neural Transm. 2019, 126, 699–710. [Google Scholar] [CrossRef] [PubMed]
- Oung, Q.W.; Muthusamy, H.; Lee, H.L.; Basah, S.N.; Yaacob, S.; Sarillee, M.; Lee, C.H. Technologies for Assessment of Motor Disorders in Parkinson’s Disease: A Review. Sensors 2015, 15, 21710–21745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ossig, C.; Antonini, A.; Buhmann, C.; Classen, J.; Csoti, I.; Falkenburger, B.; Schwarz, M.; Winkler, J.; Storch, A. Wearable Sensor-Based Objective Assessment of Motor Symptoms in Parkinson’s Disease. J. Neural Transm. 2016, 123, 57–64. [Google Scholar] [CrossRef]
- Salarian, A.; Russmann, H.; Wider, C.; Burkhard, P.R.; Vingerhoets, F.J.G.; Aminian, K. Quantification of Tremor and Bradykinesia in Parkinson’s Disease Using a Novel Ambulatory Monitoring System. IEEE Trans. Biomed. Eng. 2007, 54, 313–322. [Google Scholar] [CrossRef]
- Espay, A.J.; Bonato, P.; Nahab, F.B.; Maetzler, W.; Dean, J.M.; Klucken, J.; Eskofier, B.M.; Merola, A.; Horak, F.; Lang, A.E.; et al. Technology in Parkinson’s Disease: Challenges and Opportunities. Mov. Disord. 2016, 31, 1272–1282. [Google Scholar] [CrossRef] [Green Version]
- Jeon, H.; Lee, W.; Park, H.; Lee, H.J.; Kim, S.K.; Kim, H.B.; Jeon, B.; Park, K.S. High-Accuracy Automatic Classification of Parkinsonian Tremor Severity Using Machine Learning Method. Physiol. Meas. 2017, 38, 1980–1999. [Google Scholar] [CrossRef]
- Lieber, B.; Taylor, B.E.S.; Appelboom, G.; Mckhann, G.; Connolly, E.S. Motion Sensors to Assess and Monitor Medical and Surgical Management of Parkinson Disease. World Neurosurg. 2015, 84, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Rigas, G.; Tzallas, A.T.; Tsipouras, M.G.; Bougia, P.; Tripoliti, E.E.; Baga, D.; Fotiadis, D.I.; Tsouli, S.G.; Konitsiotis, S. Assessment of Tremor Activity in the Parkinson’s Disease Using a Set of Wearable Sensors. IEEE Trans. Inf. Technol. Biomed. 2012, 16, 478–487. [Google Scholar] [CrossRef] [PubMed]
- Burg, J.P. Maximum Entropy Spectral Analysis. Ph.D. Dissertation, Stanford University, Stanford, CA, USA, May 1975. [Google Scholar]
- Hughes, A.J.; Daniel, S.E.; Kilford, L.; Lees, A.J. Accuracy of Clinical Diagnosis of Idiopathic Parkinson’s Disease: A Clinico-Pathological Study of 100 Cases. J. Neurol. Neurosurg. Psychiatr. 1992, 55, 181–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elble, R.J.; Pullman, S.L.; Matsumoto, J.Y.; Raethjen, J.; Deuschl, G.; Tintner, R. Tremor Amplitude Is Logarithmically Related to 4- and 5-Point Tremor Rating Scales. Brain 2006, 129, 2660–2666. [Google Scholar] [CrossRef]
- McHugh, M. Interrater Reliability—The Kappa Statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Ranganathan, P.; Pramesh, C.; Aggarwal, R. Common Pitfalls in Statistical Analysis: Measures of Agreement. Perspect. Clin. Res. 2017, 8, 187–191. [Google Scholar] [CrossRef]
- Heldman, D.A.; Espay, A.J.; LeWitt, P.A.; Giuffrida, J.P. Clinician versus Machine: Reliability and Responsiveness of Motor Endpoints in Parkinson’s Disease. Parkinsonism. Relat. Disord. 2014, 20, 590–595. [Google Scholar] [CrossRef] [Green Version]
- Jeon, H.; Kim, S.K.; Jeon, B.; Park, K.S. Distance Estimation from Acceleration for Quantitative Evaluation of Parkinson Tremor. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, Boston, MA, USA, 30 August–3 September 2011; pp. 393–396. [Google Scholar]
- Mahadevan, N.; Demanuele, C.; Zhang, H.; Volfson, D.; Ho, B.; Erb, M.K.; Patel, S. Development of Digital Biomarkers for Resting Tremor and Bradykinesia Using a Wrist-Worn Wearable Device. NPJ Digit. Med. 2020, 3, 5. [Google Scholar] [CrossRef] [Green Version]
- Elble, R.J.; Ondo, W. Tremor rating scales and laboratory tools for assessing tremor. J. Neurol. Sci. 2022, 435, 120202. [Google Scholar] [CrossRef]
- Fahn, S.; Tolosa, E.; Marín, C. Clinical Rating Scale for Tremor. Parkinson’s Dis. Mov. Disord. 1993, 2, 271–280. [Google Scholar]
- Zajki-Zechmeister, T.; Kögl, M.; Kalsberger, K.; Franthal, S.; Homayoon, N.; Katschnig-Winter, P.; Wenzel, K.; Zajki-Zechmeister, L.; Schwingenschuh, P. Quantification of Tremor Severity with a Mobile Tremor Pen. Heliyon 2020, 6, e047. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.; Song, H.J.; Sharma, V.D.; Lyons, K.E.; Pahwa, R.; Akinwuntan, A.E.; Devos, H. Classification of Parkinson’s disease and essential tremor based on balance and gait characteristics from wearable motion sensors via machine learning techniques: A data-driven approach. J. Neuroeng. Rehabil. 2020, 17, 125. [Google Scholar] [CrossRef] [PubMed]
- Hssayeni, M.D.; Jimenez-Shahed, J.; Burack, M.A.; Ghoraani, B. Wearable Sensors for Estimation of Parkinsonian Tremor Severity during Free Body Movements. Sensors 2019, 19, 4215. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Score | Scoring Criteria MDS-UPDRS Items 3.15–3.17 | Score | Scoring Criteria MDS-UPDRS Item 3.18 |
|---|---|---|---|
| 0 | No tremor | 0 | No tremor |
| 1 | ≤1 cm in maximal amplitude | 1 | Tremor is present ≤25% of the time |
| 2 | >1 cm but <3 cm in maximal amplitude | 2 | Tremor is present 26–50% of the time |
| 3 | 3–10 cm in maximal amplitude | 3 | Tremor is present 51–75% of the time |
| 4 | >10 cm in maximal amplitude | 4 | Tremor is present >75% of the time |
| MDS-UPDRS Test | Outcome Measure | R | R2 * | Coefficient ** | 95%CI | p |
|---|---|---|---|---|---|---|
| 3.15 Postural tremor | Log(PAUCtremor) | 0.869 | 0.755 | 3.171 | 2.737, 3.605 | <0.001 |
| Log(Amplitude) | 0.805 | 0.648 | 1.312 | 1.079, 1.544 | <0.001 | |
| 3.16 Kinetic tremor | Log(PAUCtremor) | 0.379 | 0.144 | 1.749 | 0.584, 2.914 | 0.004 |
| Log(Amplitude) | 0.513 | 0.264 | 1.030 | 0.560, 1.499 | <0.001 | |
| 3.17 Rest tremor amplitude | Log(PAUCtremor) | 0.904 | 0.818 | 4.256 | 3.769, 3.769 | <0.001 |
| Log(Amplitude) | 0.912 | 0.832 | 2.032 | 1.811, 2.253 | <0.001 | |
| 3.18 Rest tremor constancy | Log(PAUCtremor/s) | 0.857 | 0.735 | 2.322 | 1.985, 2.660 | <0.001 |
| Ttremor | 0.974 | 0.949 | 7.180 | 6.779, 7.581 | <0.001 |
| MDS-UPDRS Test | Concordance | Cohen’s κ | 95%CI | RMSE | MAE |
|---|---|---|---|---|---|
| 3.15 Postural tremor | 76.1% | 0.614 | 0.563, 0.665 | 0.569 | 0.268 |
| 3.16 Kinetic tremor | 69.6% | 0.239 | 0.137, 0.341 | 0.641 | 0.339 |
| 3.17 Rest tremor amplitude | 77.1% | 0.620 | 0.597, 0.643 | 0.521 | 0.243 |
| 3.18 Rest tremor constancy | 84.3% | 0.726 | 0.628, 0.824 | 0.493 | 0.186 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smid, A.; Elting, J.W.J.; van Dijk, J.M.C.; Otten, B.; Oterdoom, D.L.M.; Tamasi, K.; Heida, T.; van Laar, T.; Drost, G. Intraoperative Quantification of MDS-UPDRS Tremor Measurements Using 3D Accelerometry: A Pilot Study. J. Clin. Med. 2022, 11, 2275. https://doi.org/10.3390/jcm11092275
Smid A, Elting JWJ, van Dijk JMC, Otten B, Oterdoom DLM, Tamasi K, Heida T, van Laar T, Drost G. Intraoperative Quantification of MDS-UPDRS Tremor Measurements Using 3D Accelerometry: A Pilot Study. Journal of Clinical Medicine. 2022; 11(9):2275. https://doi.org/10.3390/jcm11092275
Chicago/Turabian StyleSmid, Annemarie, Jan Willem J. Elting, J. Marc C. van Dijk, Bert Otten, D. L. Marinus Oterdoom, Katalin Tamasi, Tjitske Heida, Teus van Laar, and Gea Drost. 2022. "Intraoperative Quantification of MDS-UPDRS Tremor Measurements Using 3D Accelerometry: A Pilot Study" Journal of Clinical Medicine 11, no. 9: 2275. https://doi.org/10.3390/jcm11092275
APA StyleSmid, A., Elting, J. W. J., van Dijk, J. M. C., Otten, B., Oterdoom, D. L. M., Tamasi, K., Heida, T., van Laar, T., & Drost, G. (2022). Intraoperative Quantification of MDS-UPDRS Tremor Measurements Using 3D Accelerometry: A Pilot Study. Journal of Clinical Medicine, 11(9), 2275. https://doi.org/10.3390/jcm11092275