
Medium- to Long-Term Outcomes after Reverse Total Shoulder Arthroplasty with a Standard Long Stem


 and
and
Abstract
:1. Introduction
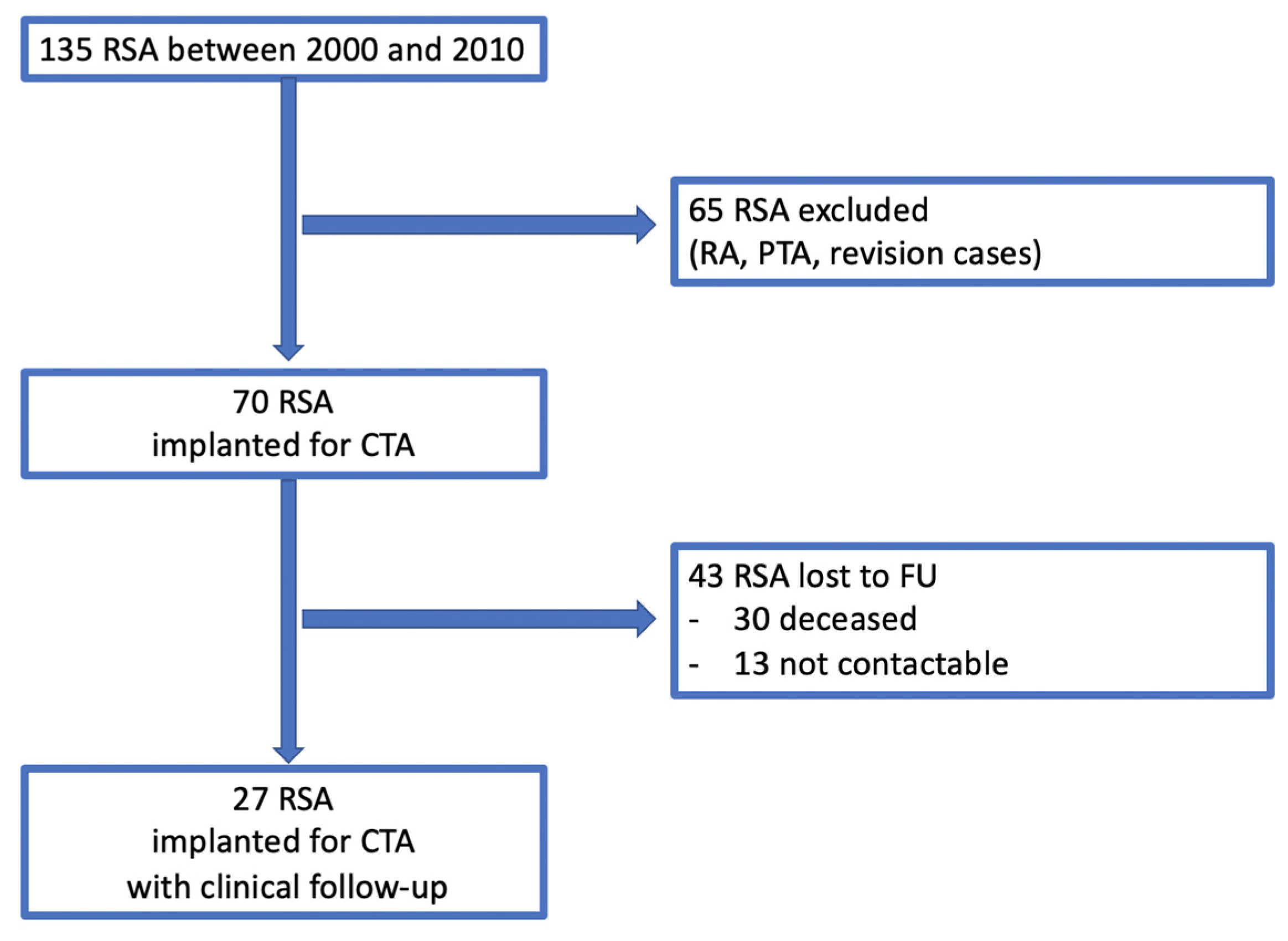
2. Materials and Methods
3. Surgical Technique
4. Clinical Analysis
5. Radiographic Analysis
6. Statistics
7. Results
7.1. Clinical Results
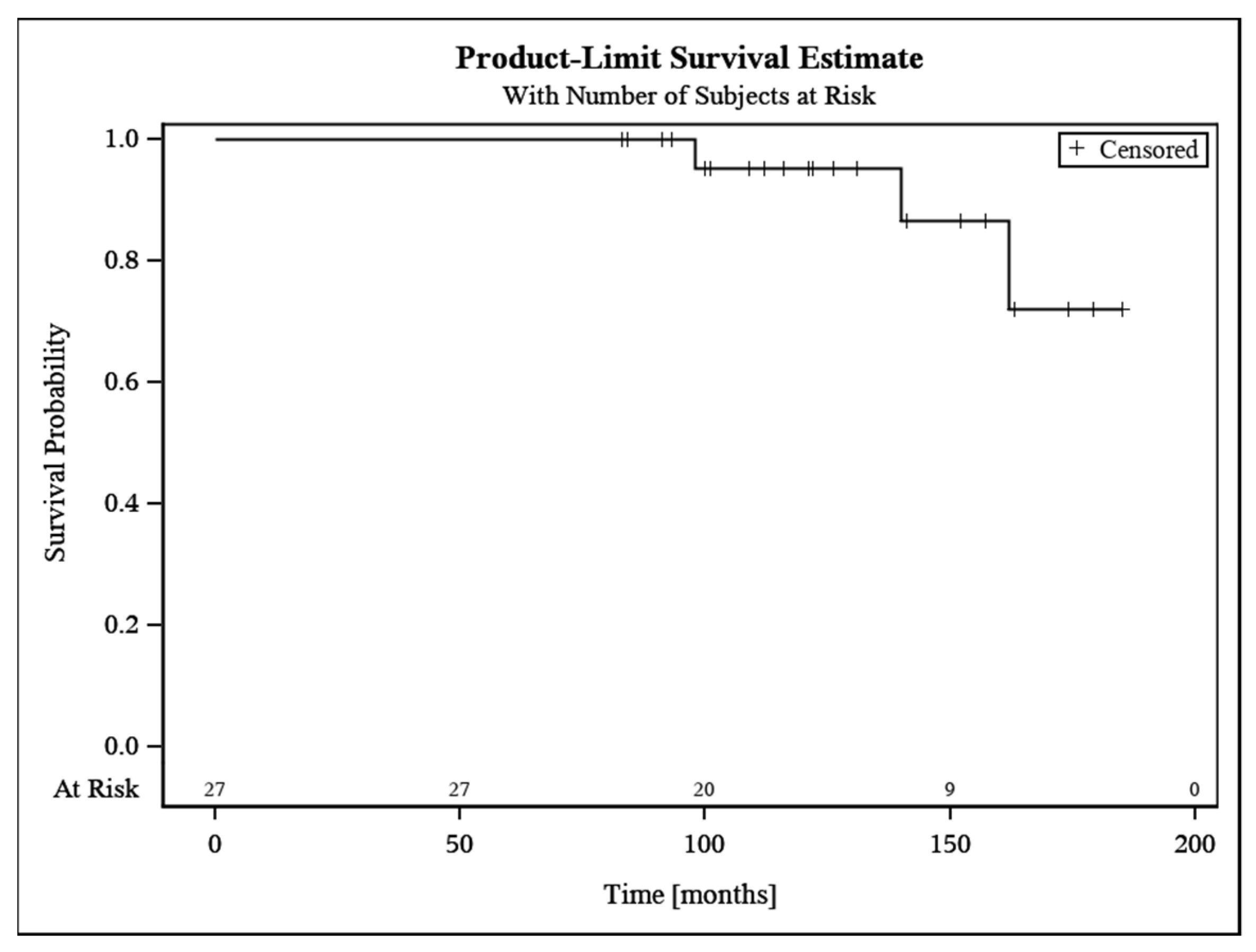
7.2. Revisions
7.3. Radiographic Outcome
8. Discussion
9. Limitations
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Gerber, C.; Pennington, S.D.; Nyffeler, R.W. Reverse total shoulder arthroplasty. J. Am. Acad. Orthop. Surg. 2009, 17, 284–295. [Google Scholar] [CrossRef] [PubMed]
- Streit, M.R.; Lehner, B.; Peitgen, D.S.; Innmann, M.M.; Omlor, G.W.; Walker, T.; Merle, C.; Moradi, B. What Is the Long-term (27- to 32-year) Survivorship of an Uncemented Tapered Titanium Femoral Component and Survival in Patients Younger than 50 Years? Clin. Orthop. Relat. Res. 2020, 478, 1283–1291. [Google Scholar] [CrossRef] [PubMed]
- Westermann, R.W.; Pugely, A.J.; Martin, C.T.; Gao, Y.; Wolf, B.R.; Hettrich, C.M. Reverse Shoulder Arthroplasty in the United States: A Comparison of National Volume, Patient Demographics, Complications, and Surgical Indications. Iowa Orthop. J. 2015, 35, 1–7. [Google Scholar]
- Grammont, P.M.; Baulot, E. The Classic: Delta Shoulder Prosthesis for Rotator Cuff Rupture. Clin. Orthop. Relat. Res. 2011, 469, 2424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rolf, O.G.F. Inverse Prothese. In AE-Manual der Endoprothetik; Loew, M., Ed.; Springer: Berlin/Heidelberg, Germany, 2010; Volume 1, pp. 117–130. [Google Scholar]
- Thompson, T.; Greenspoon, J.; Hanypsiak, B.; Lederman, E. Reverse total shoulder arthroplasty: A comprehensive review of biomechanics, surgical technique, and potential complications. Curr. Orthop. Pract. 2014, 25, 580–588. [Google Scholar] [CrossRef]
- Rittmeister, M.; Kerschbaumer, F. Grammont reverse total shoulder arthroplasty in patients with rheumatoid arthritis and nonreconstructible rotator cuff lesions. J. Shoulder Elb. Surg. 2001, 10, 17–22. [Google Scholar] [CrossRef]
- Wall, B.; Nové-Josserand, L.; O’Connor, D.P.; Edwards, T.B.; Walch, G. Reverse total shoulder arthroplasty: A review of results according to etiology. J. Bone Jt. Surg. Am. 2007, 89, 1476–1485. [Google Scholar] [CrossRef]
- Australian Orthopaedic Association National Joint Replacement Registry. Annual Reports 2020. Available online: https://aoanjrr.sahmri.com/annual-reports-2020 (accessed on 8 April 2022).
- Sirveaux, F.; Favard, L.; Oudet, D.; Huquet, D.; Walch, G.; Molé, D. Grammont inverted total shoulder arthroplasty in the treatment of glenohumeral osteoarthritis with massive rupture of the cuff. Results of a multicentre study of 80 shoulders. J. Bone Jt. Surg. Br. 2004, 86, 388–395. [Google Scholar] [CrossRef]
- Werner, C.M.; Steinmann, P.A.; Gilbart, M.; Gerber, C. Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the Delta III reverse-ball-and-socket total shoulder prosthesis. J. Bone Jt. Surg. Am. 2005, 87, 1476–1486. [Google Scholar] [CrossRef]
- Favard, L.; Levigne, C.; Nerot, C.; Gerber, C.; De Wilde, L.; Mole, D. Reverse prostheses in arthropathies with cuff tear: Are survivorship and function maintained over time? Clin. Orthop. Relat. Res. 2011, 469, 2469–2475. [Google Scholar] [CrossRef] [Green Version]
- Fevang, B.T.; Lie, S.A.; Havelin, L.I.; Skredderstuen, A.; Furnes, O. Risk factors for revision after shoulder arthroplasty: 1825 shoulder arthroplasties from the Norwegian Arthroplasty Register. Acta Orthop. 2009, 80, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, R.; Debeer, P.; De Smet, L. Treatment of rotator cuff arthropathy with a reversed Delta shoulder prosthesis. Acta Orthop. Belg. 2001, 67, 344–347. [Google Scholar] [PubMed]
- Boileau, P.; Watkinson, D.J.; Hatzidakis, A.M.; Balg, F. Grammont reverse prosthesis: Design, rationale, and biomechanics. J. Shoulder Elb. Surg. 2005, 14, 147s–161s. [Google Scholar] [CrossRef] [PubMed]
- Melis, B.; DeFranco, M.; Lädermann, A.; Molé, D.; Favard, L.; Nérot, C.; Maynou, C.; Walch, G. An evaluation of the radiological changes around the Grammont reverse geometry shoulder arthroplasty after eight to 12 years. J. Bone Jt. Surg. Br. Vol. 2011, 93, 1240–1246. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, G.P.; Strauss, E.J.; Sherman, S.L. Scapular notching: Recognition and strategies to minimize clinical impact. Clin. Orthop. Relat. Res. 2011, 469, 2521–2530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simovitch, R.W.; Zumstein, M.A.; Lohri, E.; Helmy, N.; Gerber, C. Predictors of scapular notching in patients managed with the Delta III reverse total shoulder replacement. J. Bone Jt. Surg. Am. 2007, 89, 588–600. [Google Scholar] [CrossRef]
- Lévigne, C.; Boileau, P.; Favard, L.; Garaud, P.; Molé, D.; Sirveaux, F.; Walch, G. Scapular notching in reverse shoulder arthroplasty. J. Shoulder Elb. Surg. 2008, 17, 925–935. [Google Scholar] [CrossRef]
- Seebauer, L. Total reverse shoulder arthroplasty: European lessons and future trends. Am. J. Orthop. 2007, 36, 22–28. [Google Scholar]
- Tross, A.K.; Lädermann, A.; Wittmann, T.; Schnetzke, M.; Nolte, P.C.; Collin, P.; Raiss, P. Subsidence of Uncemented Short Stems in Reverse Shoulder Arthroplasty-A Multicenter Study. J. Clin. Med. 2020, 9, 3362. [Google Scholar] [CrossRef]
- Constant, C.R.; Murley, A.H. A clinical method of functional assessment of the shoulder. Clin. Orthop. Relat. Res. 1987, 214, 160–164. [Google Scholar] [CrossRef]
- Constant, C.R.; Gerber, C.; Emery, R.J.H.; Søjbjerg, J.O.; Gohlke, F.; Boileau, P. A review of the Constant score: Modifications and guidelines for its use. J. Shoulder Elb. Surg. 2008, 17, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Boehm, D.; Wollmerstedt, N.; Doesch, M.; Handwerker, M.; Mehling, E.; Gohlke, F. Entwicklung eines Fragebogens basierend auf dem Constant-Murely-Score zur Selbstevaluation der Schulterfunktion durch den Patienten. Der Unf. 2004, 107, 397–402. [Google Scholar] [CrossRef] [PubMed]
- Ek, E.T.; Neukom, L.; Catanzaro, S.; Gerber, C. Reverse total shoulder arthroplasty for massive irreparable rotator cuff tears in patients younger than 65 years old: Results after five to fifteen years. J. Shoulder Elb. Surg. 2013, 22, 1199–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boileau, P.; Gonzalez, J.F.; Chuinard, C.; Bicknell, R.; Walch, G. Reverse total shoulder arthroplasty after failed rotator cuff surgery. J. Shoulder Elb. Surg. 2009, 18, 600–606. [Google Scholar] [CrossRef] [PubMed]
- Raiss, P.; Zeifang, F.; Pons-Villanueva, J.; Smithers, C.J.; Loew, M.; Walch, G. Reverse arthroplasty for osteoarthritis and rotator cuff deficiency after previous surgery for recurrent anterior shoulder instability. Int. Orthop. 2014, 38, 1407–1413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Hadithy, N.; Domos, P.; Sewell, M.D.; Pandit, R. Reverse shoulder arthroplasty in 41 patients with cuff tear arthropathy with a mean follow-up period of 5 years. J. Shoulder Elb. Surg. 2014, 23, 1662–1668. [Google Scholar] [CrossRef] [PubMed]
- Gruber, S.; Schoch, C.; Geyer, M. The reverse shoulder arthroplasty Delta Xtend: Mid-term results. Orthopade 2017, 46, 222–226. [Google Scholar] [CrossRef]
- Boileau, P.; Morin-Salvo, N.; Bessière, C.; Chelli, M.; Gauci, M.O.; Lemmex, D.B. Bony increased-offset-reverse shoulder arthroplasty: 5 to 10 years’ follow-up. J. Shoulder Elb. Surg. 2020, 29, 2111–2122. [Google Scholar] [CrossRef]
- Mizuno, N.; Denard, P.J.; Raiss, P.; Walch, G. Reverse total shoulder arthroplasty for primary glenohumeral osteoarthritis in patients with a biconcave glenoid. J. Bone Jt. Surg. Am. 2013, 95, 1297–1304. [Google Scholar] [CrossRef]
- Vanhove, B.; Beugnies, A. Grammont’s reverse shoulder prosthesis for rotator cuff arthropathy. A retrospective study of 32 cases. Acta Orthop. Belg. 2004, 70, 219–225. [Google Scholar]
- Seebauer, L.; Walter, W.; Keyl, W. Reverse total shoulder arthroplasty for the treatment of defect arthropathy. Oper. Orthop. Traumatol. 2005, 17, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Berhouet, J.; Garaud, P.; Favard, L. Influence of glenoid component design and humeral component retroversion on internal and external rotation in reverse shoulder arthroplasty: A cadaver study. Orthop. Traumatol. Surg. Res. 2013, 99, 887–894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Callegari, J.; Haidamous, G.; Lädermann, A.; Phillips, C.; Tracy, S.; Denard, P. Factors Influencing Appropriate Implant Selection and Position in Reverse Total Shoulder Arthroplasty. Orthop. Clin. N. Am. 2021, 52, 157–166. [Google Scholar] [CrossRef]
- Mollon, B.; Mahure, S.A.; Roche, C.P.; Zuckerman, J.D. Impact of scapular notching on clinical outcomes after reverse total shoulder arthroplasty: An analysis of 476 shoulders. J. Shoulder Elb. Surg. 2017, 26, 1253–1261. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, P.N.; Boileau, P.; Romeo, A.A.; Tashjian, R.Z. Revision Reverse Shoulder Arthroplasty. J. Am. Acad. Orthop. Surg. 2019, 27, 426–436. [Google Scholar] [CrossRef] [PubMed]
- Boileau, P.; Watkinson, D.; Hatzidakis, A.M.; Hovorka, I. Neer Award 2005: The Grammont reverse shoulder prosthesis: Results in cuff tear arthritis, fracture sequelae, and revision arthroplasty. J. Shoulder Elb. Surg. 2006, 15, 527–540. [Google Scholar] [CrossRef]
- Goldenberg, B.T.; Samuelsen, B.T.; Spratt, J.D.; Dornan, G.J.; Millett, P.J. Complications and implant survivorship following primary reverse total shoulder arthroplasty in patients younger than 65 years: A systematic review. J. Shoulder Elb. Surg. 2020, 29, 1703–1711. [Google Scholar] [CrossRef]
- Schnetzke, M.; Preis, A.; Coda, S.; Raiss, P.; Loew, M. Anatomical and reverse shoulder replacement with a convertible, uncemented short-stem shoulder prosthesis: First clinical and radiological results. Arch. Orthop. Trauma Surg. 2017, 137, 679–684. [Google Scholar] [CrossRef]
- Tross, A.K.; Woolson, T.E.; Nolte, P.C.; Schnetzke, M.; Loew, M.; Millett, P.J. Primary reverse shoulder replacement with a short stem: A systematic literature review. JSES Rev. Rep. Tech. 2021, 1, 7–16. [Google Scholar] [CrossRef]
- Raiss, P.; Schnetzke, M.; Wittmann, T.; Kilian, C.M.; Edwards, T.B.; Denard, P.J.; Neyton, L.; Godeneche, A.; Walch, G. Postoperative radiographic findings of an uncemented convertible short stem for anatomic and reverse shoulder arthroplasty. J. Shoulder Elb. Surg. 2019, 28, 715–723. [Google Scholar] [CrossRef]
- Merolla, G.; Walch, G.; Ascione, F.; Paladini, P.; Fabbri, E.; Padolino, A.; Porcellini, G. Grammont humeral design versus onlay curved-stem reverse shoulder arthroplasty: Comparison of clinical and radiographic outcomes with minimum 2-year follow-up. J. Shoulder Elb. Surg. 2018, 27, 701–710. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Demographic Variable | Value (n = 27) |
|---|---|
| Age *, years, mean (SD; range) | 72.6 (5.4; 61–84) |
| Gender, female/male; n (%) | 23 (85)/4 (15) |
| Primary osteoarthritis, n (%) | 2 (7.4) |
| Cuff tear arthropathy, n (%) | 25 (92.6) |
| Clinical FU, months, mean (SD; range) | 127.6 (33.7; 83–185) |
| Radiographic FU, months, mean (SD; range) | 126.4 (34.3; 83–185) |
| Operation time, minutes, mean (SD; range) | 98 (31.1; 59–210) |
| Variable | Preoperative | Follow-Up | p-Value |
|---|---|---|---|
| CS, median (range) | 20.0 (0–41) | 62.0 (21–98) | p < 0.001 |
| aCS, median (range) | 30.0 (10–59) | 95.0 (33–141) | p < 0.001 |
| Activity, median (range) | 8.0 (3–14) | 18.0 (6–20) | p < 0.001 |
| Mobility, median (range) | 8.0 (0–30) | 24.0 (2–38) | p < 0.001 |
| Strength, median (range) | 0 (0–8) | 5.0 (0–12) | p < 0.001 |
| Pain, median (range) | 4.5 (0–15) | 15.0 (5–15) | p < 0.001 |
| Forward elevation, degree, median (range) | 60.0 (0–150) | 120 (30–160) | p < 0.001 |
| External rotation, degree, median (range) | 0 (−20–45) | 10.0 (0–50) | p = 0.104 |
| Abduction, degree, median (range) | 60.0 (20–140) | 110.0 (0–160) | p < 0.001 |
| Symptoms and Pathology | Time until Revision | Revision Surgery |
|---|---|---|
| Instability; polyethylene wear | 13 years | Exchange of liner |
| Pain; polyethylene wear | 9 years | Exchange of liner |
| Pain; polyethylene wear | 7 years | Exchange of liner |
| Radiographic Observation | Absolute Numbers and Percentage |
|---|---|
| Stem loosening, n (%) | 3 (13.6) |
| Glenoid loosening, n (%) | 2 (9.1) |
| Polyethylene wear, n (%) | 4 (18.2) |
| Scapular notching, n (%) | |
| Grade 1 | 3 (20%) |
| Grade 2 | 7 (46.7%) |
| Grade 3 | 5 (33.3%) |
| Author and Year of Publication | N | Indication | Mean FU (Months) | CS Pre/Post | aCS Pre/Post | Forward Elevation Pre/Post | Glenoid Loosening Rate (%) | Stem Loosening Rate (%) | Revision Rate (%) | Scapular Notching Rate (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| Jacobs et al., 2001 [14] | 7 | CTA | 16 | 18/57 | NA | NA | 0 | NA | NA | NA |
| Sirveaux et al., 2003 [10] | 80 | CTA | 44 | 23/66 | NA | 73/138 | 6 | NA | 5 | 63.6 |
| Vanhove et al., 2004 [32] | 14 | CTA | 31 | NA/60 | NA | NA | NA | NA | NA | 50 |
| Seebauer et al., 2005 [33] | 57 | CTA, RCD | 18 | NA/67 | NA/94 | NA/145 | 0 | NA | NA | 24 |
| Boileau et al., 2009 [26] | 46 | RCD | 50 | 25/56 | 36/79 | 82/123 | 0 | 2.2 | 4.3 | 67 |
| Favard et al., 2011 [12] | 148 | CTA, OA, RCD | 90 | 24/62 | 33/85 | 69/129 | NA | NA | NA | 35 (grade 3 and 4) |
| Mizuno et al., 2013 [31] | 27 | OA | 54 | 31/76 | NA | 89/152 | 3.7 | 0 | 3.7 | 37 |
| Ek et al., 2013 [25] | 40 | RCD | 93 | 34/74 | 72/119 | 7.5 | 0 | 27.5 | 56 | |
| Raiss et al., 2014 [27] | 13 | CTA | 42 | 26/67 | NA | 70/130 | 0 | 0 | 8 | 38 |
| Al-Hadithy et al., 2014 [28] | 41 | RCD | 60 | 24/60 | 34/71 | 55/108 | 0 | 0 | 2.4 | 68 |
| Gruber et al., 2017 [29] | 39 | CTA, RCD, OA | 68 | NA | 39/71 | NA/39 | NA | NA | 7.7 | 64 |
| Boileau et al., 2020 [30] | 143 | RCD | 75 | 40/93 | NA | 84/137 | 0 | 0 | 4 | 56 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bülhoff, M.; Zeifang, F.; Welters, C.; Renkawitz, T.; Schiltenwolf, M.; Tross, A.-K. Medium- to Long-Term Outcomes after Reverse Total Shoulder Arthroplasty with a Standard Long Stem. J. Clin. Med. 2022, 11, 2274. https://doi.org/10.3390/jcm11092274
Bülhoff M, Zeifang F, Welters C, Renkawitz T, Schiltenwolf M, Tross A-K. Medium- to Long-Term Outcomes after Reverse Total Shoulder Arthroplasty with a Standard Long Stem. Journal of Clinical Medicine. 2022; 11(9):2274. https://doi.org/10.3390/jcm11092274
Chicago/Turabian StyleBülhoff, Matthias, Felix Zeifang, Caroline Welters, Tobias Renkawitz, Marcus Schiltenwolf, and Anna-K. Tross. 2022. "Medium- to Long-Term Outcomes after Reverse Total Shoulder Arthroplasty with a Standard Long Stem" Journal of Clinical Medicine 11, no. 9: 2274. https://doi.org/10.3390/jcm11092274
APA StyleBülhoff, M., Zeifang, F., Welters, C., Renkawitz, T., Schiltenwolf, M., & Tross, A.-K. (2022). Medium- to Long-Term Outcomes after Reverse Total Shoulder Arthroplasty with a Standard Long Stem. Journal of Clinical Medicine, 11(9), 2274. https://doi.org/10.3390/jcm11092274