
Early Virtual-Reality-Based Home Rehabilitation after Total Hip Arthroplasty: A Randomized Controlled Trial


 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
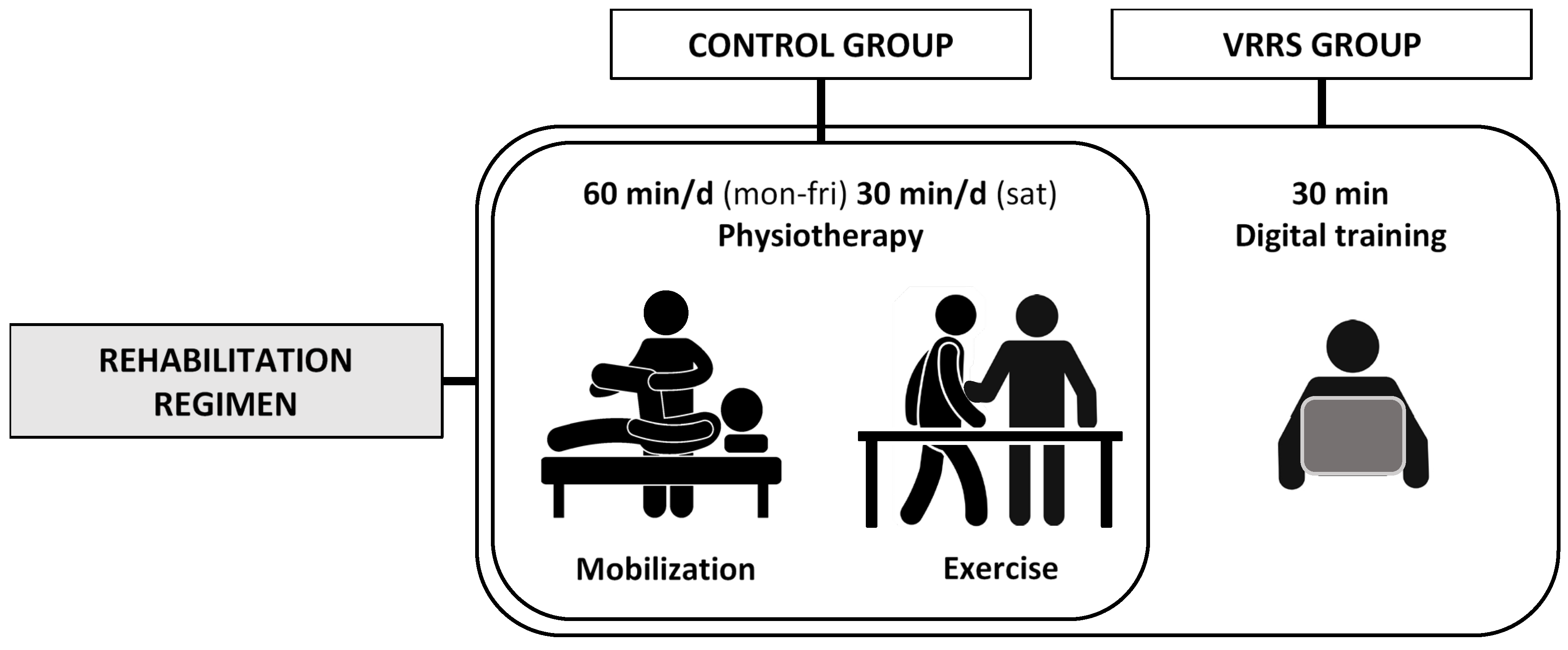
2.1. Study Design
2.2. Sample Size
2.3. Participants
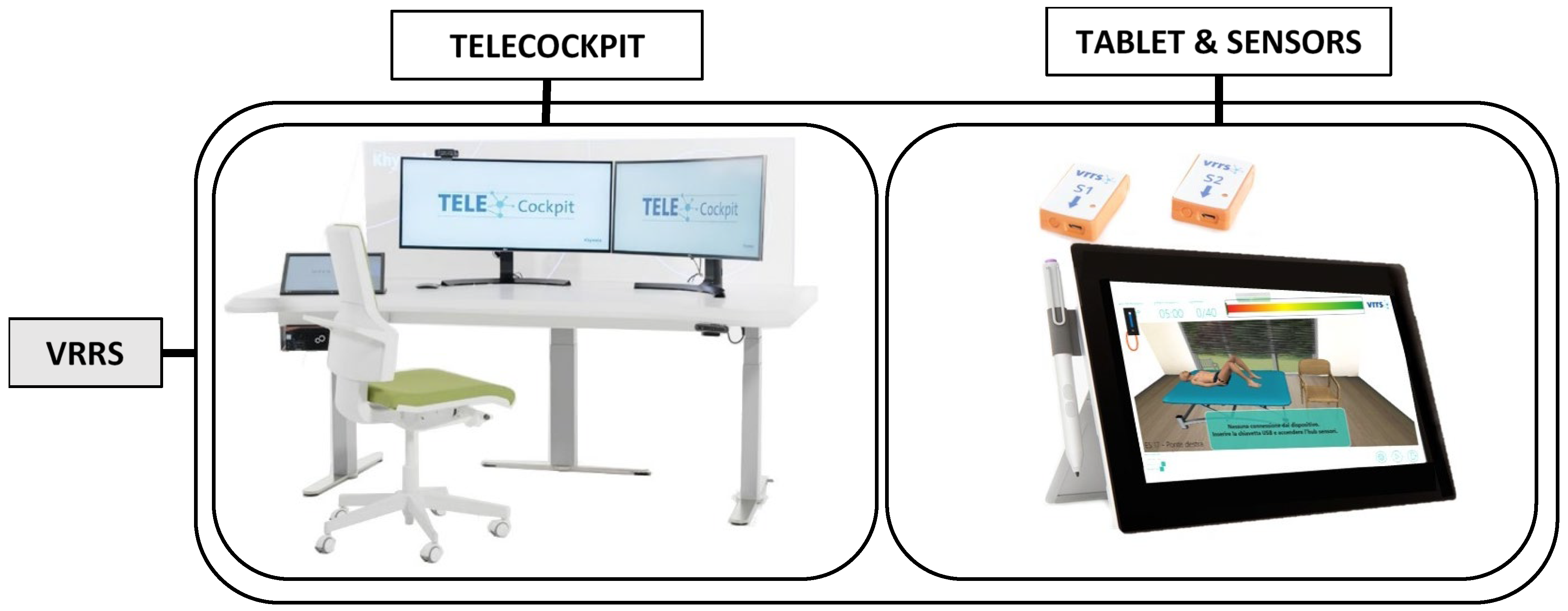
2.4. Virtual Reality Rehabilitation System (VRRS)
2.5. Exercise Program
2.6. Clinical Outcomes and Assessment
2.7. Statistical Analysis
3. Results
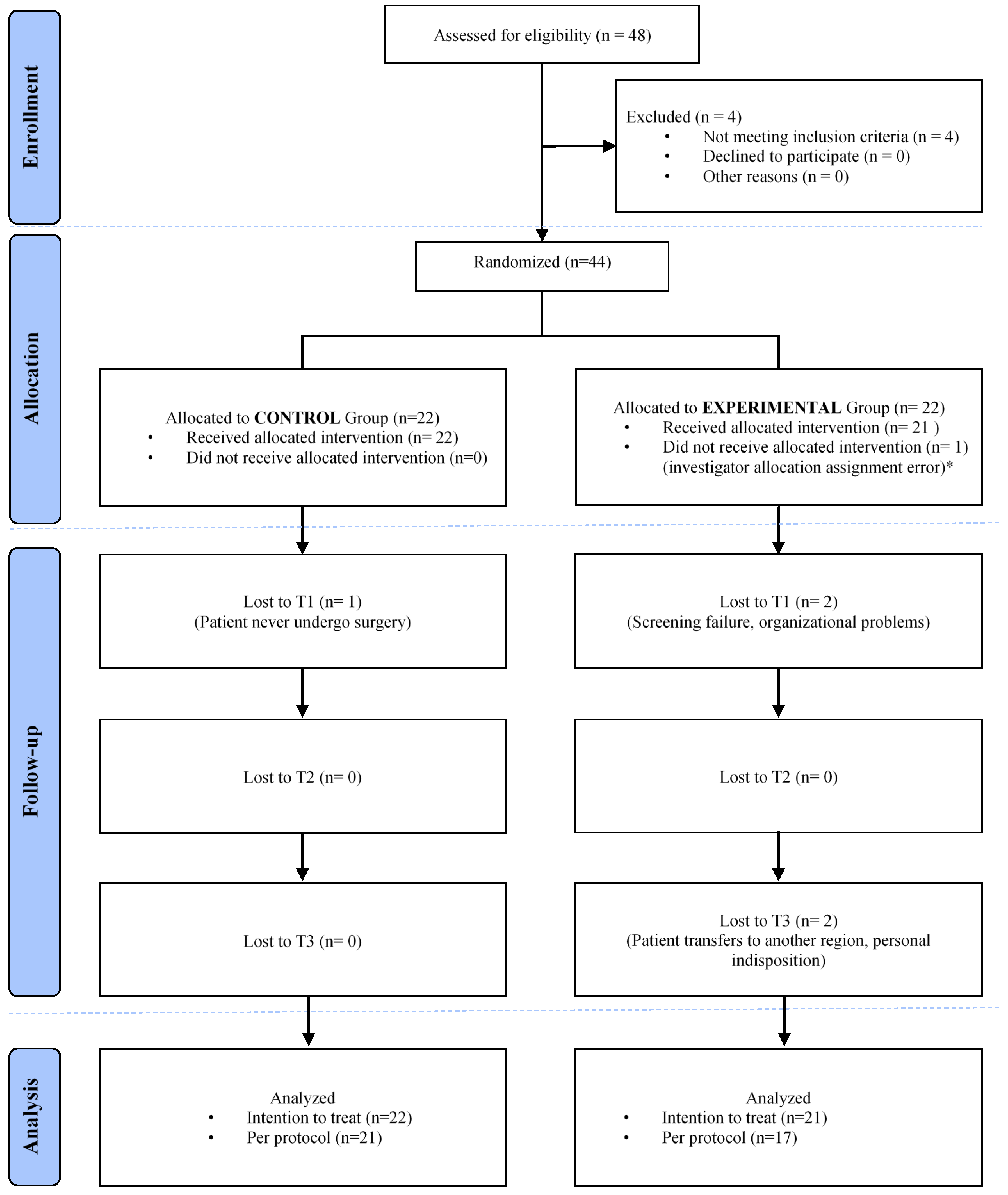
3.1. Participants
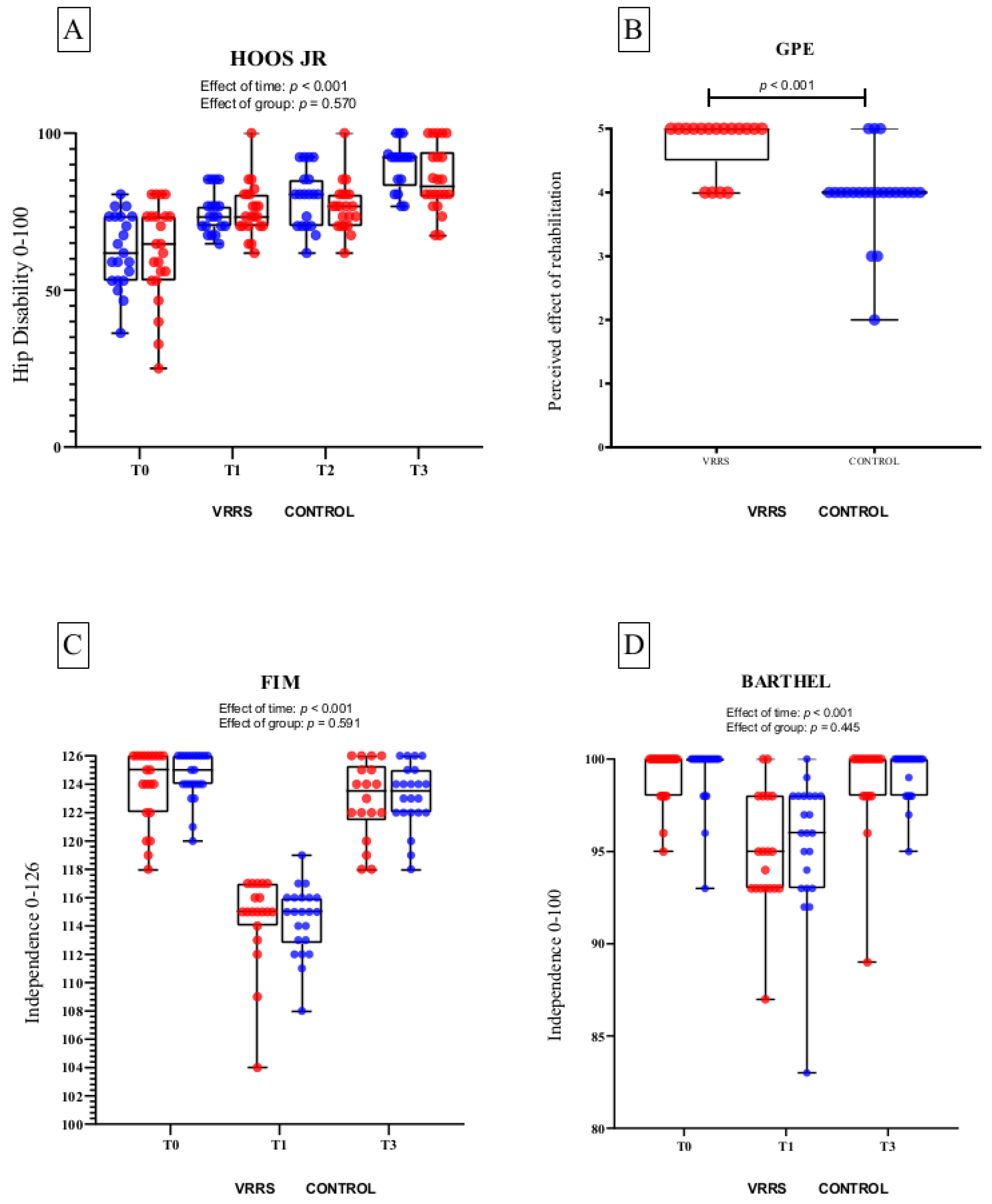
3.2. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Klussmann, A.; Gebhardt, H.; Nübling, M.; Liebers, F.; Perea, E.Q.; Cordier, W.; von Engelhardt, L.V.; Schubert, M.; Dávid, A.; Bouillon, B.; et al. Individual and occupational risk factors for knee osteoarthritis: Results of a case-control study in Germany. Arthritis Res. Ther. 2010, 12, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Vitale, J.A.; Banfi, G.; Tivolesi, V.; Pelosi, C.; Borghi, S.; Negrini, F. Rest-activity daily rhythm and physical activity levels after hip and knee joint replacement: The role of actigraphy in orthopedic clinical practice. Chronobiol. Int. 2021, 38, 1692–1701. [Google Scholar] [CrossRef]
- Winter, C.C.; Brandes, M.; Müller, C.; Schubert, T.; Ringling, M.; Hillmann, A.; Rosenbaum, D.; Schulte, T.L. Walking ability during daily life in patients with osteoarthritis of the knee or the hip and lumbar spinal stenosis: A cross sectional study. BMC Musculoskelet. Disord. 2010, 11, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ulivi, M.; Orlandini, L.; Vitale, J.A.; Meroni, V.; Prandoni, L.; Mangiavini, L.; Rossi, N.; Peretti, G.M. Direct superior approach versus posterolateral approach in total hip arthroplasty: A randomized controlled trial on early outcomes on gait, risk of fall, clinical and self-reported measurements. Acta Orthop. 2021, 92, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.A.; Vessely, M.B.; Harmsen, W.S.; Schleck, C.D.; Melton III, L.J.; Kurland, R.L.; Berry, D.J. A population-based study of trends in the use of total hip and total knee arthroplasty, 1969–2008. Mayo Clin. Proc. 2010, 85, 898–904. [Google Scholar] [CrossRef]
- Nelson, M.; Russell, T.; Crossley, K.; Bourke, M.; McPhail, S. Cost-effectiveness of telerehabilitation versus traditional care after total hip replacement: A trial-based economic evaluation. J. Telemed. Telecare 2021, 27, 359–366. [Google Scholar] [CrossRef]
- Conferenza Permanente per i Rapporti tra lo Stato, le Regioni e le Province Autonome di Trento e di Bolzano. 215/CSR. 2020. Available online: https://www.statoregioni.it/it/conferenza-stato-regioni/sedute-2020/seduta-del-17122020/atti/repertorio-atto-n-215csr/ (accessed on 20 October 2021).
- Senato della Repubblica. Piano Nazionale di Ripresa e Resilienza. XVIII Legislatura. Available online: https://www.senato.it/versionestampa/stampa.jsp?thispage (accessed on 27 October 2021).
- Russell, T. Physical rehabilitation using telemedicine. J. Telemed. Telecare 2007, 13, 217–220. [Google Scholar] [CrossRef]
- McKeon, J.F.; Alvarez, P.M.; Vajapey, A.S.; Sarac, N.; Spitzer, A.I.; Vajapey, S.P. Expanding Role of Technology in Rehabilitation After Lower-Extremity Joint Replacement: A Systematic Review. JBJS Rev. 2021, 9, e21. [Google Scholar] [CrossRef]
- Agostini, M.; Moja, L.; Banzi, R.; Pistotti, V.; Tonin, P.; Venneri, A.; Turolla, A. Telerehabilitation and recovery of motor function: A systematic review and meta-analysis. J. Telemed. Telecare 2015, 21, 202–213. [Google Scholar] [CrossRef]
- Cottrell, M.A.; Galea, O.A.; O’Leary, S.P.; Hill, A.J.; Russell, T.G. Real-time telerehabilitation for the treatment of musculoskeletal conditions is effective and comparable to standard practice: A systematic review and meta-analysis. Clin. Rehabil. 2017, 31, 625–638. [Google Scholar] [CrossRef]
- Shukla, H.; Nair, S.; Thakker, D. Role of telerehabilitation in patients following total knee arthroplasty: Evidence from a systematic literature review and meta-analysis. J. Telemed. Telecare 2017, 23, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Lee, R.L.; Hunter, S.; Chan, S.W. The effectiveness of internet-based telerehabilitation among patients after total joint arthroplasty: A systematic review and meta-analysis of randomised controlled trials. J. Telemed. Telecare 2021, 1357633X20980291. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.G.C.M.; Gupte, C.; Akhtar, K.; Smith, P.; Cobb, J. The Global Economic Cost of Osteoarthritis: How the UK Compares. Arthritis 2012, 2012, 698709. [Google Scholar] [CrossRef] [PubMed]
- Hunter, D.J.; Bierma-Zeinstra, S. Osteoarthritis. Lancet 2019, 393, 1745–1759. [Google Scholar] [CrossRef]
- Bandholm, T.; Kehlet, H. Physiotherapy exercise after fast-track total hip and knee arthroplasty: Time for reconsideration? Arch. Phys. Med. Rehabil. 2012, 93, 1292–1294. [Google Scholar] [CrossRef] [PubMed]
- Lyman, S.; Lee, Y.Y.; Franklin, P.D.; Li, W.; Mayman, D.J.; Padgett, D.E. Validation of the HOOS, JR: A Short-form Hip Replacement Survey. Clin. Orthop. Relat. Res. 2016, 474, 1472–1482. [Google Scholar] [CrossRef] [PubMed]
- Ottenbacher, K.J.; Hsu, Y.; Granger, C.V.; Fiedler, R.C. The Reliability of the Functional Independence Measure: A Quantitative Review. Arch. Phys. Med. Rehabil. 1996, 77, 1226–1232. [Google Scholar] [CrossRef]
- Taricco, M.; Andreoli, E.; Miccoli, B.; Foresti, A.; Monti, E.; Gazzotti, A.; Menarini, M.; Zardi, E.; Arcangeli, E.; Bianconcini, F.; et al. Caratteristiche e utilità clinica e gestionale della Barthel Index “Modificato” (BIM) come indicatore di disabilità nei reparti di riabilitazione: Esperienza di condivisione in team. Eur. Med. Phys. 2021, 45. [Google Scholar]
- Kamper, S.J.; Ostelo, R.W.; Knol, D.L.; Maher, C.G.; de Vet, H.C.; Hancock, M.J. Global perceived effect scales provided reliable assessments of health transition in people with musculoskeletal disorders, but ratings are strongly influenced by current status. J. Clin. Epidemiol. 2010, 63, 760–766.e1. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; White, I.R.; Carlin, J.B.; Spratt, M.; Royston, P.; Kenward, M.G.; Wood, A.M.; Carpenter, J.R. Multiple imputation for missing data in epidemiological and clinical research: Potential and pitfalls. BMJ 2009, 339, 157–160. [Google Scholar] [CrossRef]
- Maire, J.; Faillenet-Maire, A.F.; Grange, C.; Dugué, B.; Tordi, N.; Parratte, B.; Rouillon, J.D. A specific arm-interval exercise program could improve the health status and walking ability of elderly patients after total hip arthroplasty: A pilot study. J. Rehabil. Med. 2004, 36, 92–94. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Stergiou-Kita, M.; Grigorovich, A. Community reintegration following a total joint replacement: A pilot study. Musculoskelet. Care 2014, 12, 103–113. [Google Scholar] [CrossRef]
- Gianola, S.; Stucovitz, E.; Castellini, G.; Mascali, M.; Vanni, F.; Tramacere, I.; Banfi, G.; Tornese, D. Effects of early virtual reality-based rehabilitation in patients with total knee arthroplasty: A randomized controlled trial. Medicine 2020, 99, e19136. [Google Scholar] [CrossRef] [PubMed]
- Tousignant, M.; Moffet, H.; Boissy, P.; Corriveau, H.; Cabana, F.; Marquis, F. A randomized controlled trial of home telerehabilitation for post-knee arthroplasty. J. Telemed. Telecare 2011, 17, 195–198. [Google Scholar] [CrossRef] [PubMed]
- Russell, T.G.; Buttrum, P.; Wootton, R.; Jull, G.A. Rehabilitation after total knee replacement via low-bandwidth telemedicine: The patient and therapist experience. J. Telemed. Telecare 2004, 10 (Suppl. S1), 85–87. [Google Scholar] [CrossRef] [PubMed]
- Piqueras, M.; Marco, E.; Coll, M.; Escalada, F.; Ballester, A.; Cinca, C.; Belmonte, R.; Muniesa, J.M. Effectiveness of an interactive virtual telerehabilitation system in patients after total knee arthoplasty: A randomized controlled trial. J. Rehabil. Med. 2013, 45, 392–396. [Google Scholar] [CrossRef]
- Gosman-Hedström, G.; Svensson, E. Parallel reliability of the functional independence measure and the Barthel ADL index. Disabil. Rehabil. 2020, 22, 702–715. [Google Scholar] [CrossRef]
- Gunnes, M.; Indredavik, B.; Langhammer, B.; Lydersen, S.; Ihle-Hansen, H.; Dahl, A.E.; Askim, T. Associations between adherence to the physical activity and exercise program applied in the last study and functional recovery after stroke. Arch. Phys. Med. Rehabil. 2019, 100, 2251–2259. [Google Scholar] [CrossRef]
- Seo, N.J.; Crocher, V.; Spaho, E.; Ewert, C.R.; Fathi, M.F.; Hur, P.; Atkinson, S.J.; Humanitzki, E.M.; Lauer, A.W.; Ramakrishnan, V.; et al. Capturing upper limb gross motor categories using the Kinect® sensor. Am. J. Occup. Ther. 2019, 73, 7304205090p1–7304205090p10. [Google Scholar]
- Busso, C.; Castorina, G.; Di Monaco, M.; Rodriguez, D.; Mahdavi, H.; Balocco, S.; Trucco, M.; Conti, M.; Castagna, A.; Minetto, M.A. Effectiveness of a home-based telerehabilitation system in patients after total hip arthroplasty: Study protocol of a randomized controlled trial. Trials 2020, 21, 1–7. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Exercise | Area | Mode | Group | Regimen | Tools | |
|---|---|---|---|---|---|---|
| 1 | strengthening | Hip flexors | concentric | C | AMAYC | Illustrated exercise booklet |
| V | 40 rep/5 min (1st week a.s.), 80 rep/10 min (2nd week a.s.) | tablet and sensors, interactive VR exercise | ||||
| 2 | strengthening | Hip extensors | concentric | C | AMAYC | Illustrated exercise booklet |
| V | 40 rep/5 min (1st week a.s.), 80 rep/10 min (2nd week a.s.) | tablet and sensors, interactive VR exercise | ||||
| 3 | strengthening | Hip abductors | concentric | C | AMAYC | Illustrated exercise booklet |
| V | 40 rep/5 min (1st week a.s.), 80 rep/10 min (2nd week a.s.) | tablet and sensors, interactive VR exercise | ||||
| 4 | strengthening | Hip adductors | concentric | n/a | n/a | n/a |
| V | 40 rep/5 min (1st week a.s.), 80 rep/10 min (2nd week a.s.) | tablet and sensors, interactive VR exercise | ||||
| 5 | strengthening | Knee flexors | concentric | n/a | n/a | n/a |
| V | 40 rep/5 min (1st week a.s.), 80 rep/10 min (2nd week a.s.) | tablet and sensors, interactive VR exercise | ||||
| 6 | strengthening | Knee flexors | auxotonic | C | AMAYC | Illustrated exercise booklet |
| V | 40 rep/5 min (1st week a.s.), 80 rep/10 min (2nd week a.s.) | tablet and sensors, interactive VR exercise | ||||
| 7 | strengthening | Knee extensors | isometric | C | AMAYC | Illustrated exercise booklet |
| V | 40 rep/5 min (1st week a.s.), 80 rep/10 min (2nd week a.s.) | tablet and sensors, interactive VR exercise | ||||
| 8 | strengthening | Knee extensors | concentric | C | AMAYC | Illustrated exercise booklet |
| V | 40 rep/5 min (1st week a.s.), 80 rep/10 min (2nd week a.s.) | tablet and sensors, interactive VR exercise | ||||
| 9 | Load management | n/a | bipodalic | C | AMAYC | Illustrated exercise booklet |
| n/a | n/a | n/a | ||||
| 10 | Semi-quat | n/a | bipodalic | C | AMAYC | Illustrated exercise booklet |
| V | 40 rep/5 min (1st week a.s.), 80 rep/10 min (2nd week a.s.) | tablet and sensors, interactive VR exercise | ||||
| 11 | Calf raise | n/a | bipodalic | C | AMAYC | Illustrated exercise booklet |
| n/a | n/a | n/a | ||||
| 12 | Lower Limb Triple Flexion | n/a | operated limb | C | AMAYC | Illustrated exercise booklet |
| V | 40 rep/5 min (1st week a.s.), 80 rep/10 min (2nd week a.s.) | tablet and sensors, interactive VR exercise |
| Control Group (n = 23) | VRRS Group (n = 21) | p-Value * | |
|---|---|---|---|
| Men—n. (%) | 13 (56.5%) | 12 (57.1%) | 0.967 |
| Age (years) | 60.9 ± 7.52 | 61.5 ± 6.21 | 0.767 |
| BARTHEL (0–100) | 99.26 ± 1.71 | 99.19 ± 1.47 | 0.642 |
| FIM (18–126) | 124.57 ± 1.67 | 123.86 ± 2.63 | 0.612 |
| HOOS JR (0–100) | 62.23 ± 15.54 | 62.71 ± 11.74 | 0.909 |
| VRRS Group | Control Group | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T0 | T1 | T2 | T3 | T0 | T1 | T2 | T3 | Effect of Time | Contrast | Effect of Group | Interaction | |
| HOOS JR | 62.7 ± 11.7 | 74.6 ± 6.6 | 79.3 ± 9.3 | 89.7 ± 7.6 | 62.2 ± 15.5 | 75.5 ± 8.4 | 76.6 ± 7.9 | 85.4 ± 10.4 | <0.0001 | T1 vs. T2 (p > 0.05) a | 0.570 | 0.510 |
| FIM | 123.9 ± 2.6 | 114.4 ± 3.2 | n/a | 122.9 ± 2.7 | 124.6 ± 1.6 | 114.4 ± 2.4 | n/a | 123.2 ± 2.2 | <0.0001 | T0 vs. T3 (p > 0.05) a | 0.591 | 0.730 |
| BARTHEL | 99.2 ± 1.5 | 94.9 ± 3.1 | n/a | 98.6 ± 2.8 | 99.3 ± 1.7 | 95.4 ± 3.6 | n/a | 99.2 ± 1.3 | <0.0001 | T0 vs. T3 (p > 0.05) a | 0.445 | 0.835 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fascio, E.; Vitale, J.A.; Sirtori, P.; Peretti, G.; Banfi, G.; Mangiavini, L. Early Virtual-Reality-Based Home Rehabilitation after Total Hip Arthroplasty: A Randomized Controlled Trial. J. Clin. Med. 2022, 11, 1766. https://doi.org/10.3390/jcm11071766
Fascio E, Vitale JA, Sirtori P, Peretti G, Banfi G, Mangiavini L. Early Virtual-Reality-Based Home Rehabilitation after Total Hip Arthroplasty: A Randomized Controlled Trial. Journal of Clinical Medicine. 2022; 11(7):1766. https://doi.org/10.3390/jcm11071766
Chicago/Turabian StyleFascio, Edoardo, Jacopo Antonino Vitale, Paolo Sirtori, Giuseppe Peretti, Giuseppe Banfi, and Laura Mangiavini. 2022. "Early Virtual-Reality-Based Home Rehabilitation after Total Hip Arthroplasty: A Randomized Controlled Trial" Journal of Clinical Medicine 11, no. 7: 1766. https://doi.org/10.3390/jcm11071766
APA StyleFascio, E., Vitale, J. A., Sirtori, P., Peretti, G., Banfi, G., & Mangiavini, L. (2022). Early Virtual-Reality-Based Home Rehabilitation after Total Hip Arthroplasty: A Randomized Controlled Trial. Journal of Clinical Medicine, 11(7), 1766. https://doi.org/10.3390/jcm11071766