
Does Repeated Dosing of Intravenous Ferric Carboxymaltose Alleviate Symptoms of Restless Legs Syndrome?



Abstract
:1. Introduction
2. Materials and Methods
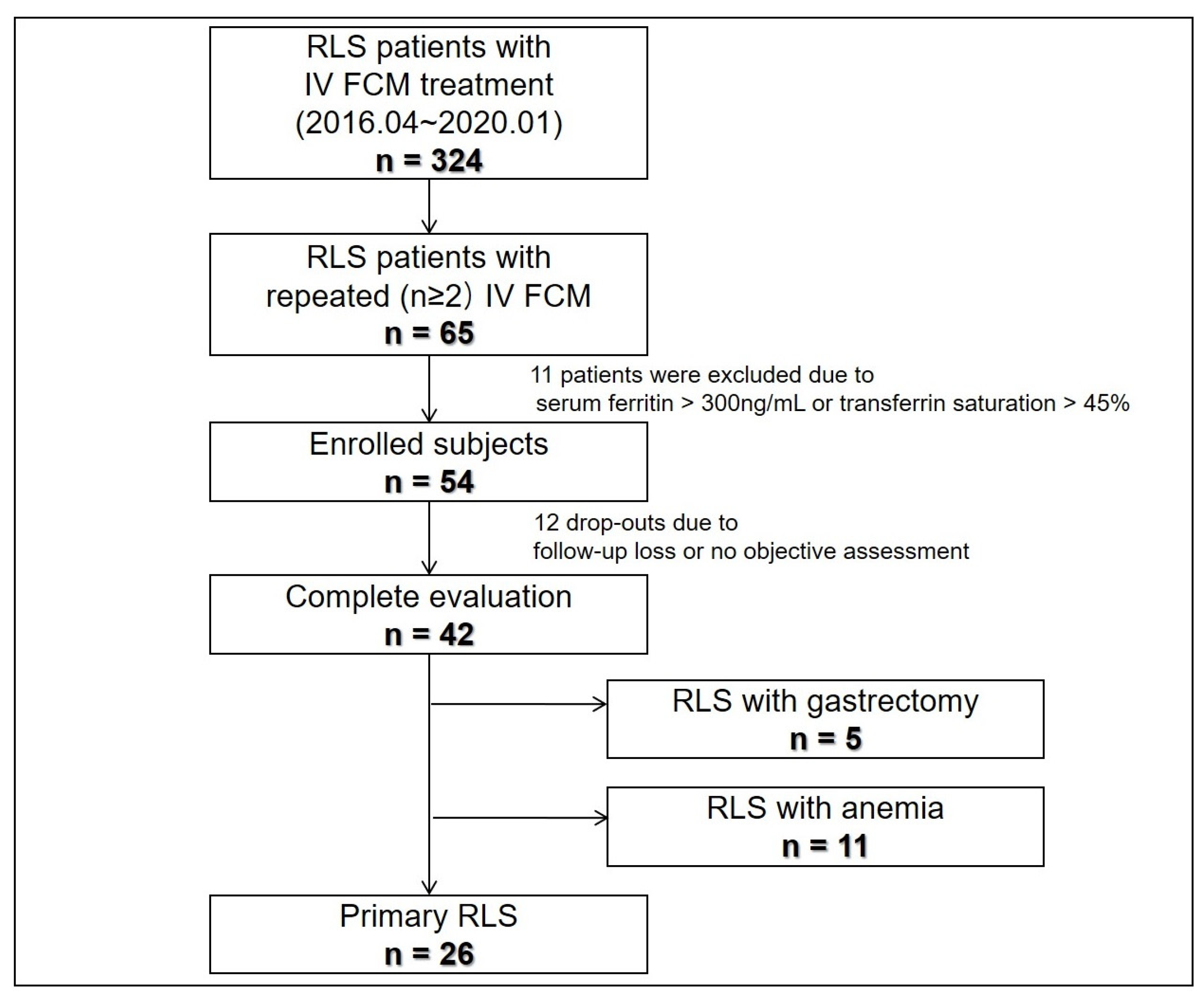
2.1. Subjects
2.2. Clinical Data and Blood Tests
2.3. Repeated FCM Treatment Protocol and Outcome Measures
2.4. Statistical Analysis
3. Results
3.1. Treatment Response to Repeated IV FCM in Patients with Primary and Secondary RLS
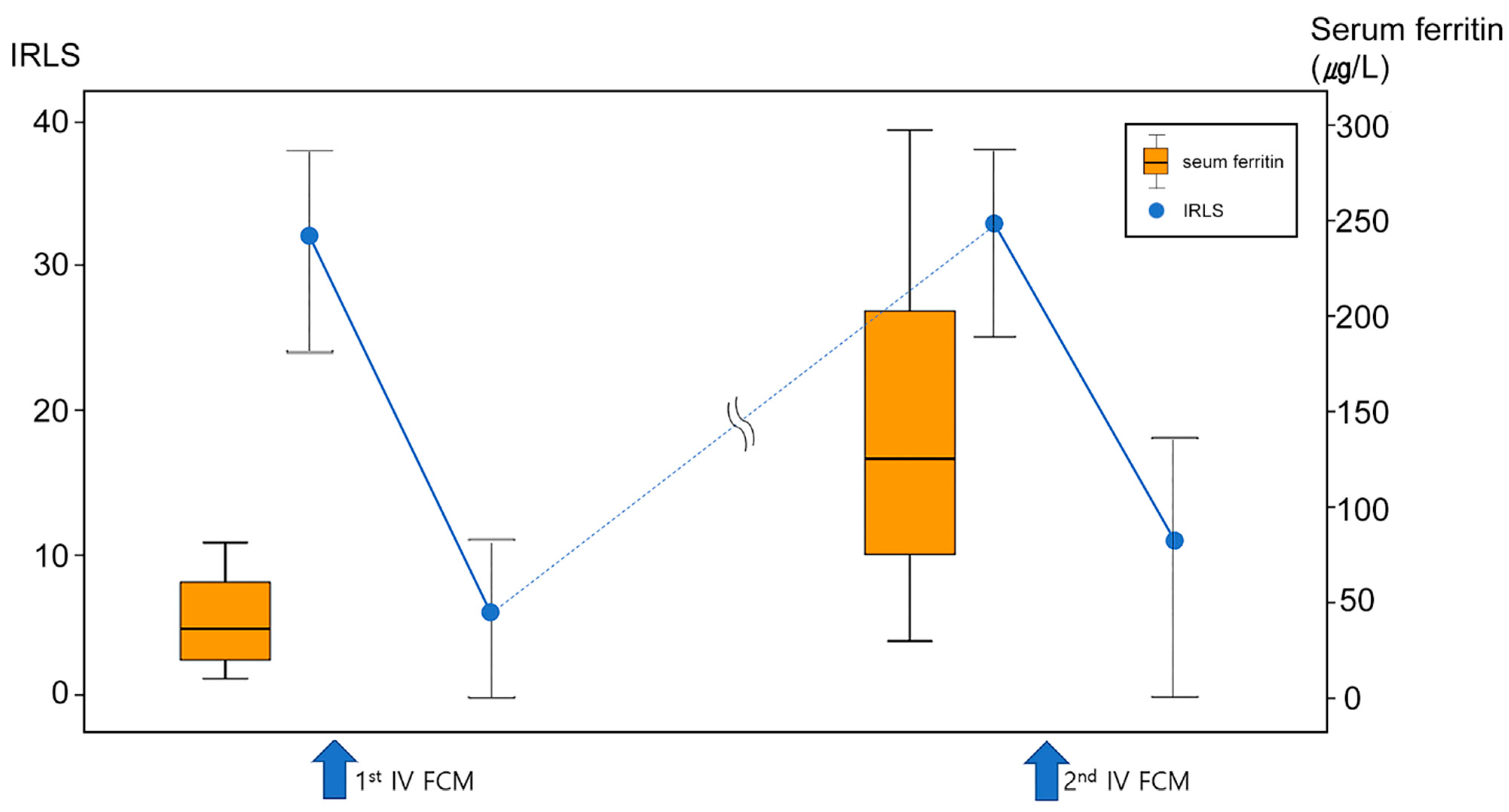
3.2. Comparison of Iron Characteristics in Patients with Primary RLS following Exposure to First and Second IV FCM
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Earley, C.J.; Allen, R.P.; Beard, J.L.; Connor, J.R. Insight into the pathophysiology of restless legs syndrome. J. Neurosci. Res. 2000, 62, 623–628. [Google Scholar] [CrossRef]
- Allen, R.P.; Earley, C.J. The role of iron in restless legs syndrome. Mov. Disord. 2007, 22 (Suppl. 18), S440–S448. [Google Scholar] [CrossRef] [PubMed]
- Connor, J.R.; Ponnuru, P.; Wang, X.-S.; Patton, S.M.; Allen, R.P.; Earley, C.J. Profile of altered brain iron acquisition in restless legs syndrome. Brain 2011, 134, 959–968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, R.P.; Adler, C.H.; Du, W.; Butcher, A.; Bregman, D.B.; Earley, C.J. Clinical efficacy and safety of IV ferric carboxymaltose (FCM) treatment of RLS: A multi-centred, placebo-controlled preliminary clinical trial. Sleep Med. 2011, 12, 906–913. [Google Scholar] [CrossRef] [PubMed]
- Earley, C.J.; Heckler, D.; Allen, R.P. The treatment of restless legs syndrome with intravenous iron dextran. Sleep Med. 2004, 5, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Beshara, S.; Lundqvist, H.; Sundin, J.; Lubberink, M.; Tolmachev, V.; Valind, S.; Antoni, G.; Långström, B.; Danielson, B.G. Pharmacokinetics and red cell utilization of iron(III) hydroxide-sucrose complex in anaemic patients: A study using positron emission tomography. Br. J. Haematol. 1999, 104, 296–302. [Google Scholar] [CrossRef]
- Friedrisch, J.R.; Cançado, R.D. Intravenous ferric carboxymaltose for the treatment of iron deficiency anemia. Rev. Bras. Hematol. Hemoter. 2015, 37, 400–405. [Google Scholar] [CrossRef] [Green Version]
- Allen, R.P.; Picchietti, D.L.; Auerbach, M.; Cho, Y.W.; Connor, J.R.; Earley, C.J.; Garcia-Borreguero, D.; Kotagal, S.; Manconi, M.; Ondo, W.; et al. Evidence-based and consensus clinical practice guidelines for the iron treatment of restless legs syndrome/Willis-Ekbom disease in adults and children: An IRLSSG task force report. Sleep Med. 2018, 41, 27–44. [Google Scholar] [CrossRef]
- Hornyak, M.; Scholz, H.; Kiemen, A.; Kassubek, J. Investigating the response to intravenous iron in restless legs syndrome: An observational study. Sleep Med. 2012, 13, 732–735. [Google Scholar] [CrossRef]
- Lieske, B.; Becker, I.; Schulz, R.J.; Polidori, M.C.; Kassubek, J.; Roehrig, G. Intravenous iron administration in restless legs syndrome: An observational study in geriatric patients. Z. Gerontol. Geriatr. 2016, 49, 626–631. [Google Scholar] [CrossRef]
- Park, H.R.; Park, H.S.; Choi, S.J.; Joo, E.Y. Clinical Factors Related to the Response of IV Ferric Carboxymaltose Treatment in Patients with Restless Legs Syndrome. J. Sleep Med. 2018, 15, 8–14. [Google Scholar] [CrossRef]
- Park, H.R.; Choi, S.J.; Joo, E.Y.; Allen, R.P. Patient characteristics predicting responses to intravenous ferric carboxymaltose treatment of restless legs syndrome. Sleep Med. 2020, 75, 81–87. [Google Scholar] [CrossRef]
- Cho, Y.W.; Allen, R.P.; Earley, C.J. Clinical efficacy of ferric carboxymaltose treatment in patients with restless legs syndrome. Sleep Med. 2016, 25, 16–23. [Google Scholar] [CrossRef]
- Trenkwalder, C.; Winkelmann, J.; Oertel, W.; Virgin, G.; Roubert, B.; Mezzacasa, A.; Investigators, F.-R.S. Ferric carboxymaltose in patients with restless legs syndrome and nonanemic iron deficiency: A randomized trial. Mov. Disord. 2017, 32, 1478–1482. [Google Scholar] [CrossRef] [Green Version]
- Earley, C.J.; Heckler, D.; Allen, R.P. Repeated IV doses of iron provides effective supplemental treatment of restless legs syndrome. Sleep Med. 2005, 6, 301–305. [Google Scholar] [CrossRef]
- Earley, C.J.; Horska, A.; Mohamed, M.A.; Barker, P.B.; Beard, J.L.; Allen, R.P. A randomized, double-blind, placebo-controlled trial of intravenous iron sucrose in restless legs syndrome. Sleep Med. 2009, 10, 206–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grote, L.; Leissner, L.; Hedner, J.; Ulfberg, J. A randomized, double-blind, placebo controlled, multi-center study of intravenous iron sucrose and placebo in the treatment of restless legs syndrome. Mov. Disord. 2009, 24, 1445–1452. [Google Scholar] [CrossRef] [PubMed]
- Allen, R.P.; Picchietti, D.L.; Garcia-Borreguero, D.; Ondo, W.G.; Walters, A.S.; Winkelman, J.W.; Zucconi, M.; Ferri, R.; Trenkwalder, C.; Lee, H.B. Restless legs syndrome/Willis-Ekbom disease diagnostic criteria: Updated International Restless Legs Syndrome Study Group (IRLSSG) consensus criteria--history, rationale, description, and significance. Sleep Med. 2014, 15, 860–873. [Google Scholar] [CrossRef]
- Cho, Y.W.; Allen, R.P.; Earley, C.J. Efficacy of ferric carboxymaltose (FCM) 500 mg dose for the treatment of Restless Legs Syndrome. Sleep Med. 2018, 42, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Walters, A.S.; LeBrocq, C.; Dhar, A.; Hening, W.; Rosen, R.; Allen, R.P.; Trenkwalder, C. Validation of the International Restless Legs Syndrome Study Group rating scale for restless legs syndrome. Sleep Med. 2003, 4, 121–132. [Google Scholar]
- Ekbom, K. Restless legs syndrome after partial gastrectomy. Acta Neurol. Scand. 1966, 42, 79–89. [Google Scholar] [CrossRef]
- Mehmood, T.; Auerbach, M.; Earley, C.J.; Allen, R.P. Response to intravenous iron in patients with iron deficiency anemia (IDA) and restless leg syndrome (Willis-Ekbom disease). Sleep Med. 2014, 15, 1473–1476. [Google Scholar] [CrossRef]
- Bae, H.; Cho, Y.W.; Kim, K.T.; Allen, R.P.; Earley, C.J. Randomized, placebo-controlled trial of ferric carboxymaltose in restless legs syndrome patients with iron deficiency anemia. Sleep Med. 2021, 84, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Manconi, M.; Garcia-Borreguero, D.; Schormair, B.; Videnovic, A.; Berger, K.; Ferri, R.; Dauvilliers, Y. Restless legs syndrome. Nat. Rev. Dis. Primers 2021, 7, 80. [Google Scholar] [CrossRef] [PubMed]
- Lopez, A.; Cacoub, P.; Macdougall, I.C.; Peyrin-Biroulet, L. Iron deficiency anaemia. Lancet 2016, 387, 907–916. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Primary (n = 26) | Gastrectomy (n = 5) | Anemia (n = 11) | p | |
|---|---|---|---|---|
| Age, years | 50.8 ± 18.9 | 68.6 ± 17.7 | 41.1 ± 16.2 | 0.028 * |
| Female, n (%) | 22 (84.6) | 3 (60.0) | 11 (100.0) | 0.067 |
| Disease duration, years | 11.2 ± 13.7 | 5.7 ± 8.1 | 6.9 ± 6.5 | 0.561 |
| Pittsburgh sleep quality index | 10.3 ± 4.7 | 10.5 ± 3.8 | 11.7 ± 4.2 | 0.777 |
| Insomnia severity index | 15.9 ± 7.0 | 19.5 ± 5.8 | 14.0 ± 7.7 | 0.502 |
| HADS_Anxiety | 8.0 ± 3.8 | 6.7 ± 5.5 | 11.6 ± 3.8 | 0.168 |
| HADS_Depression | 6.4 ± 4.7 | 9.7 ± 5.5 | 11.8 ± 2.0 | 0.061 |
| Family history of RLS, n (%) | 6 (23.1) | 1 (20.0) | 1 (9.1) | 0.611 |
| Previous RLS medication, n (%) | 7 (26.9) | 1 (20.0) | 3 (27.3) | 0.945 |
| Baseline IRLS | 30.5 ± 7.7 | 31.8 ± 4.7 | 27.8 ± 9.0 | 0.540 |
| hemoglobin, g/dL | 13.7 ± 1.0 | 11.0 ± 1.2 | 10.7 ± 1.5 | <0.001 ** |
| ferritin, ug/L | 44.8 ± 28.7 | 12.9 ± 9.7 | 23.3 ± 28.3 | 0.020 *** |
| %TSAT | 27.8 ± 10.2 | 6.2 ± 2.5 | 11.9 ± 7.7 | <0.001 ** |
| Primary (n = 26) | Gastrectomy (n = 5) | Anemia (n = 11) | p | |
|---|---|---|---|---|
| Number of FCM administration | 0.131 | |||
| twice, n (%) | 24 (92.3) | 4(80.0) | 7 (63.6) | |
| Three times, n (%) | 2 (7.7) | - | 2 (18.2) | |
| Four times, n (%) | - | 1 (20.0) | 2 (18.2) | |
| Time interval between 1st–2nd FCM, months | 14.5 ± 8.0 | 10.6 ± 3.2 | 11.6 ± 3.0 | 0.313 |
| Responders, n (%) | N.A * | |||
| 2nd treatment | 22 (84.6) | 4 (80.0) | 9 (81.8) | |
| 3rd treatment | 2 (100) | 1 (100) | 3 (75) | |
| 4th treatment | - | 1 (100) | 1 (50) | |
| IRLS change, % (after 2nd treatment) | 62.2 (32.3) | 73.9 (42.1) | 64.9 (26.7) | 0.760 |
| Before 1st Therapy | Before 2nd Therapy | p * | |
|---|---|---|---|
| Female hemoglobin, g/dL | 13.4 ± 0.8 | 13.2 ± 0.9 | 0.473 |
| Male hemoglobin, g/dL | 15.1 ± 0.6 | 15.1 ± 1.1 | 0.943 |
| Female ferritin, μg/L | 45.1 ± 30.9 | 147.5 ± 91.3 | <0.001 † |
| Male ferritin, μg/L | 42.7 ± 13.0 | 174.3 ± 77.7 | 0.050 † |
| Female %TSAT | 26.7 ± 10.5 | 27.1 ± 7.2 | 0.942 |
| Male %TSAT | 35.1 ± 4.8 | 33.3 ± 5.4 | 0.195 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, H.R.; Choi, S.J.; Joo, E.Y. Does Repeated Dosing of Intravenous Ferric Carboxymaltose Alleviate Symptoms of Restless Legs Syndrome? J. Clin. Med. 2022, 11, 1673. https://doi.org/10.3390/jcm11061673
Park HR, Choi SJ, Joo EY. Does Repeated Dosing of Intravenous Ferric Carboxymaltose Alleviate Symptoms of Restless Legs Syndrome? Journal of Clinical Medicine. 2022; 11(6):1673. https://doi.org/10.3390/jcm11061673
Chicago/Turabian StylePark, Hea Ree, Su Jung Choi, and Eun Yeon Joo. 2022. "Does Repeated Dosing of Intravenous Ferric Carboxymaltose Alleviate Symptoms of Restless Legs Syndrome?" Journal of Clinical Medicine 11, no. 6: 1673. https://doi.org/10.3390/jcm11061673
APA StylePark, H. R., Choi, S. J., & Joo, E. Y. (2022). Does Repeated Dosing of Intravenous Ferric Carboxymaltose Alleviate Symptoms of Restless Legs Syndrome? Journal of Clinical Medicine, 11(6), 1673. https://doi.org/10.3390/jcm11061673