
Prognostic Value of Non-Invasive Global Myocardial Work in Asymptomatic Aortic Stenosis

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Echocardiographic Measurements
2.3. Myocardial Work Analysis
2.4. Cardiac Damage Staging Classification
2.5. Clinical Follow-Up and Endpoints
2.6. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. Staging Classification
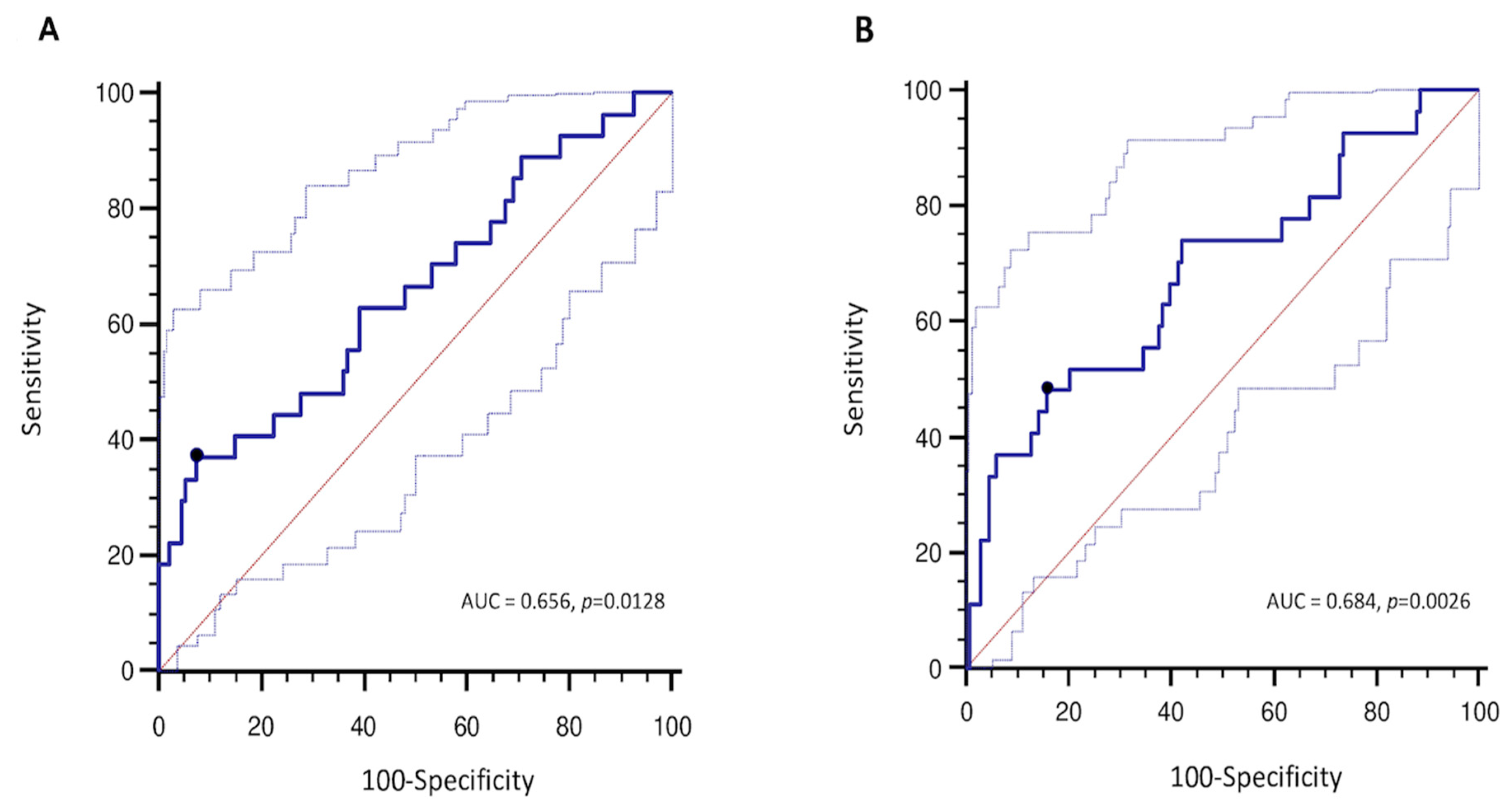
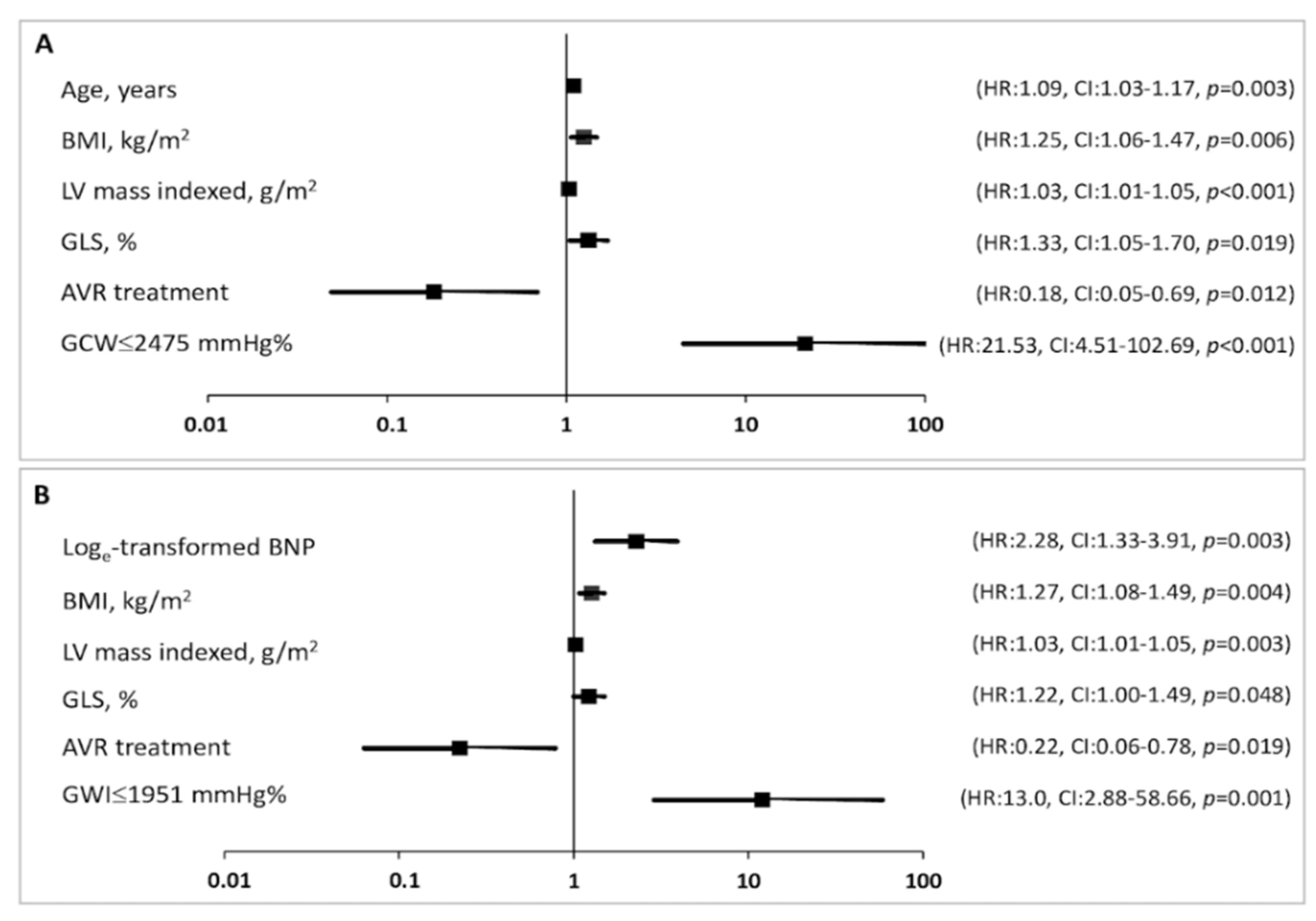
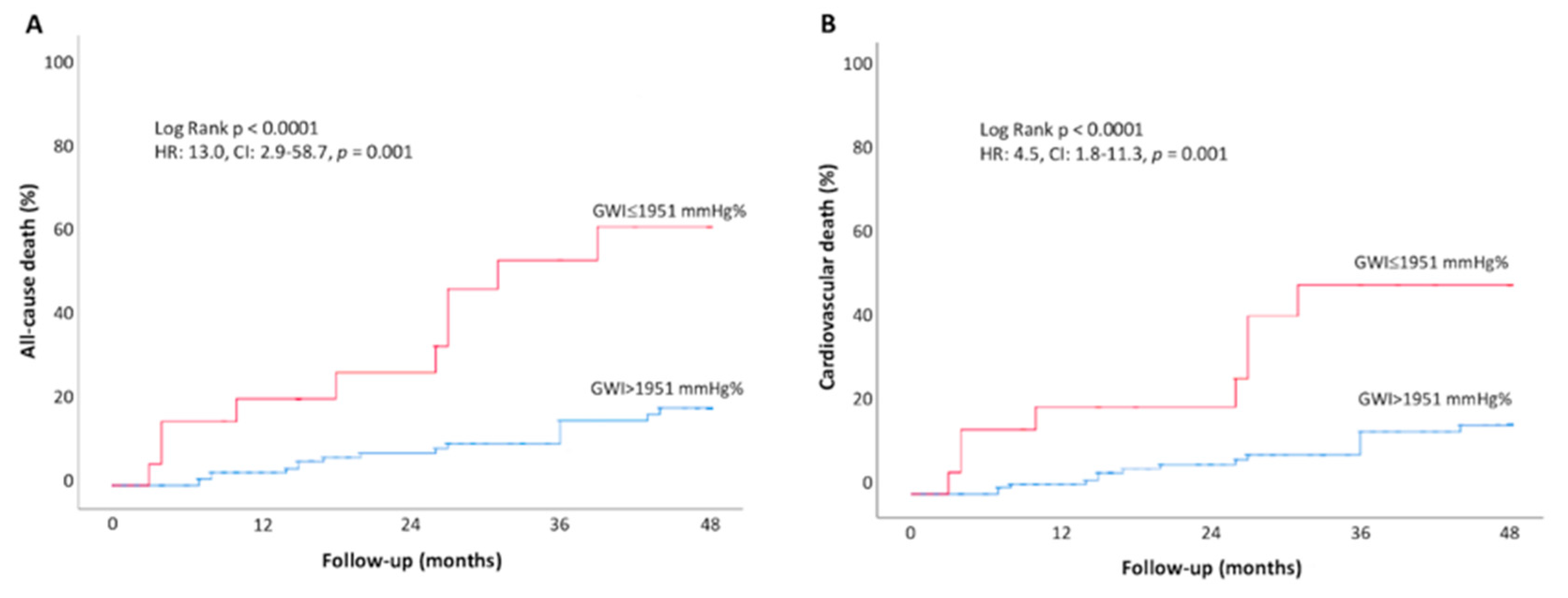
3.3. Prognostic Value of Global Work Index
4. Discussion
4.1. Myocardial Performance in Aortic Stenosis
4.2. Myocardial Work and Outcomes
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2021, 43, ehab395. [Google Scholar]
- Lancellotti, P.; Magne, J.; Dulgheru, R.; Clavel, M.A.; Donal, E.; Vannan, M.A.; Chambers, J.; Rosenhek, R.; Habib, G.; Lloyd, G.; et al. Outcomes of Patients with Asymptomatic Aortic Stenosis Followed up in Heart Valve Clinics. JAMA Cardiol. 2018, 3, 1060–1068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strange, G.; Stewart, S.; Celermajer, D.; Prior, D.; Scalia, G.M.; Marwick, T.; Ilton, M.; Joseph, M.; Codde, J.; Playford, D. Poor long-term survival in patients with moderate aortic stenosis. J. Am. Coll. Cardiol. 2019, 74, 1851–1863. [Google Scholar] [CrossRef] [PubMed]
- Tastet, L.; Tribouilloy, C.; Maréchaux, S.; Vollema, E.M.; Delgado, V.; Salaun, E.; Shen, M.; Capoulade, R.; Clavel, M.-A.; Arsenault, M.; et al. Staging Cardiac Damage in Patients with Asymptomatic Aortic Valve Stenosis. J. Am. Coll. Cardiol. 2019, 74, 550–563. [Google Scholar] [CrossRef] [PubMed]
- Ilardi, F.; D’Andrea, A.; D’Ascenzi, F.; Bandera, F.; Benfari, G.; Esposito, R.; Malagoli, A.; Mandoli, G.E.; Santoro, C.; Russo, V.; et al. Myocardial Work by Echocardiography: Principles and Applications in Clinical Practice. J. Clin. Med. 2021, 10, 4521. [Google Scholar] [CrossRef] [PubMed]
- Manganaro, R.; Marchetta, S.; Dulgheru, R.; Ilardi, F.; Sugimoto, T.; Robinet, S.; Cimino, S.; Go, Y.Y.; Bernard, A.; Kacharava, G.; et al. Echocardiographic reference ranges for normal non-invasive myocardial work indices: Results from the EACVI NORRE study. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 582–590. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, H.; Hung, J.; Bermejo, J.; Chambers, J.B.; Edvardsen, T.; Goldstein, S.; Lancellotti, P.; LeFevre, M.; Miller, F., Jr.; Otto, C.M. Recommendations on the echocardiographic assessment of aortic valve stenosis: A focused update from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 254–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Briand, M.; Dumesnil, J.G.; Kadem, L.; Tongue, A.G.; Rieu, R.; Garcia, D.; Pibarot, P. Reduced systemic arterial compliance impacts significantly on left ventricular afterload and function in aortic stenosis: Implications for diagnosis and treatment. J. Am. Coll. Cardiol. 2005, 46, 291–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Simone, G.; Chinali, M.; Galderisi, M.; Benincasa, M.; Girfoglio, D.; Botta, I.; D’Addeo, G.; de Divitiis, O. Myocardial mechano-energetic efficiency in hypertensive adults. J. Hypertens 2009, 27, 650–655. [Google Scholar] [CrossRef] [PubMed]
- Ilardi, F.; Marchetta, S.; Martinez, C.; Sprynger, M.; Ancion, A.; Manganaro, R.; Sugimoto, T.; Tsugu, T.; Postolache, A.; Piette, C.; et al. Impact of aortic stenosis on layer-specific longitudinal strain: Relationship with symptoms and outcome. Eur. Heart J. Cardiovasc. Imaging 2019, 21, 408–416. [Google Scholar] [CrossRef] [PubMed]
- Russell, K.; Eriksen, M.; Aaberge, L.; Wilhelmsen, N.; Skulstad, H.; Remme, E.W.; Huagaa, K.H.; Opdahl, A.; Fjeld, J.G.; Gjesdal, O.; et al. A novel clinical method for quantification of regional left ventricular pressure-strain loop area: A non-invasive index of myocardial work. Eur. Heart J. 2012, 33, 724–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, R.; Bajwa, T.; Roemer, S.; Huisheree, H.; Allaqaband, S.Q.; Kroboth, S.; Moreno, A.C.P.; Tajik, A.J.; Khandheria, B.K. Myocardial work assessment in severe aortic stenosis undergoing transcatheter aortic valve replacement. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 715–721. [Google Scholar] [CrossRef] [PubMed]
- Fortuni, F.; Butcher, S.C.; van der Kley, F.; Lustosa, R.P.; Karalis, I.; de Weger, A.; Priori, S.G.; van der Bijl, P.; Bax, J.J.; Delgado, V.; et al. Left Ventricular Myocardial Work in Patients with Severe Aortic Stenosis. J. Am. Soc. Echocardiogr. 2021, 34, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Henkel, D.M.; Malouf, J.F.; Connolly, H.M.; Michelena, H.I.; Sarano, M.E.; Schaff, H.V.; Scott, C.; Pellikka, P.A. Asymptomatic left ventricular systolic dysfunction in patients with severe aortic stenosis: Characteristics and outcomes. J. Am. Coll. Cardiol. 2012, 60, 2325–2329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Potter, E.; Marwick, T.H. Assessment of Left Ventricular Function by Echocardiography: The Case for Routinely Adding Global Longitudinal Strain to Ejection Fraction. JACC Cardiovasc. Imaging 2018, 11, 260–274. [Google Scholar] [CrossRef] [PubMed]
- Magne, J.; Cosyns, B.; Popescu, B.A.; Carstensen, H.G.; Dahl, J.; Desai, M.Y.; Kearney, L.; Lancellotti, P.; Marwick, T.H.; Sato, K.; et al. Distribution and Prognostic Significance of Left Ventricular Global Longitudinal Strain in Asymptomatic Significant Aortic Stenosis: An Individual Participant Data Meta-Analysis. JACC Cardiovasc. Imaging 2019, 12, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Reant, P.; Metras, A.; Detaille, D.; Reynaud, A.; Diolez, P.; Jaspard-Vinassa, B.; Roudaut, R.; Ouattara, A.; Barandon, L.; Dos Santos, P.; et al. Impact of afterload increase on left ventricular myocardial deformation indices. J. Am. Soc. Echocardiogr 2016, 29, 1217–1228. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, A.; Ilardi, F.; D’Ascenzi, F.; Bandera, F.; Benfari, G.; Esposito, R.; Malagoli, A.; Mandoli, G.E.; Santoro, C.; Russo, V.; et al. Impaired myocardial work efficiency in heart failure with preserved ejection fraction. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 1312–1320. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.; Edwards, N.F.A.; Khandheria, B.K.; Shiino, K.; Sabapathy, S.; Anderson, B.; Chamberlain, R.; Scalia, G.M. A new approach to assess myocardial work by non-invasive left ventricular pressure-strain relations in hypertension and dilated cardiomyopathy. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 31–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avvedimento, M.; Franzone, A.; Leone, A.; Piccolo, R.; Castiello, D.S.; Ilardi, F.; Mariani, A.; Esposito, R.; Iapicca, C.; Angellotti, D.; et al. Extent of Cardiac Damage and Mortality in Patients Undergoing Transcatheter Aortic Valve Implantation. J. Clin. Med. 2021, 10, 4563. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Controls (n = 50) | Asymptomatic AS Group (n = 170) | p Value |
|---|---|---|---|
| Clinical variables | |||
| Age ± SD, years | 71.1 ± 4.7 | 69.3 ± 13.4 | 0.358 |
| Male, gender n (%) | 25 (50) | 102 (60) | 0.135 |
| BMI ± SD, kg/m2 | 25.5 ± 3.4 | 26.5 ± 4.2 | 0.135 |
| BSA ± SD, m2 | 1.7 ± 0.1 | 1.8 ± 0.2 | 0.075 |
| Systolic arterial pressure ± SD, mmHg | 128 ± 11 | 136 ± 18 | 0.013 |
| Diastolic arterial pressure ± SD, mmHg | 77 ± 8 | 73 ± 10 | 0.004 |
| Loge-transformed BNP ± SD | - | 4.3 ± 1.3 | - |
| Diabetes mellitus, n (%) | - | 39 (23) | - |
| Hypertension, n (%) | - | 112 (66) | - |
| Hypercholesterolemia, n (%) | - | 106 (62) | - |
| Current smoking, n (%) | - | 29 (17) | - |
| Coronary artery disease, n (%) | - | 19 (11) | - |
| Previous PCI, n (%) | - | 15 (9) | - |
| Chronic kidney disease, n (%) | - | 40 (23) | |
| Atrial fibrillation | - | 6 (4) | - |
| LV dimensions and geometry | |||
| Interventricular septum ± SD, mm | 9.6 ± 1.2 | 12.4 ± 2.0 | <0.001 |
| LV posterior wall ± SD, mm | 9.8 ± 2.0 | 10.6 ± 1.6 | 0.004 |
| LV end-diastolic diameter ± SD, mm | 42.7 ± 5.3 | 45.4 ± 5.9 | 0.005 |
| LV end-systolic diameter ± SD, mm | 29.3 ± 5.1 | 29.9 ± 5.8 | 0.535 |
| LV mass indexed ± SD, g/m2 | 76.8 ± 20.2 | 103.9 ± 26.4 | <0.001 |
| Relative wall thickness ± SD | 0.46 ± 0.1 | 0.47 ± 0.09 | 0.514 |
| Aortic valve severity | |||
| Mean Pressure Gradient ± SD, mmHg | - | 37.3 ± 14.6 | - |
| Peak aortic Velocity ± SD, m/s | - | 3.8 ± 0.7 | - |
| Aortic Valve Area ± SD, cm2 | - | 1.02 ± 0.35 | - |
| Indexed aortic valve area ± SD, cm2/m2 | - | 0.55 ± 0.18 | - |
| Indexed Stroke Volume ± SD, mL/m2 | - | 48.0 ± 11.3 | - |
| Zva ± SD, mmHg/mL/m2 | - | 3.8 ± 1.0 | - |
| LV systolic and diastolic function | |||
| LV end-diastolic volume ± SD, mL | 83.0 ± 24.3 | 93.5 ± 34.2 | 0.065 |
| LV end-systolic volume ± SD, mL | 30.2 ± 10.4 | 36.3 ± 16.7 | 0.025 |
| LV EF ± SD, % | 64 ± 5 | 62 ± 6 | 0.130 |
| GLS ± SD, % | −20.7 ± 2.1 | −18.7 ± 2.8 | 0.014 |
| Indexed LA volume ± SD, mL/m2 | 26.5 ± 8.6 | 34.8 ± 13.0 | <0.001 |
| Mitral E/A ratio ± SD | 0.9 ± 0.2 | 0.9 ± 0.3 | 0.740 |
| E/e’ ± SD, average | 7.4 ± 1.8 | 11.9 ± 4.4 | <0.001 |
| TTPG ± SD, mmHg | 17.0 ± 8.9 | 26.3 ± 8.3 | <0.001 |
| TAPSE ± SD, mm | 22.8 ± 3.2 | 22.5 ± 3.9 | 0.601 |
| S’ ± SD, cm/s | 13.6 ± 3.0 | 12.6 ± 2.8 | 0.048 |
| Right atrial volume ± SD, mL | 32.7 ± 10.8 | 38.7 ± 16.4 | 0.017 |
| Myocardial work | |||
| GWI ± SD, mmHg% | 2005 ± 302 | 2528 ± 521 | <0.001 |
| GCW ± SD, mmHg% | 2360 ± 353 | 2948 ± 598 | <0.001 |
| GWW ± SD, mmHg% | 90 ± 49 | 139± 110 | 0.005 |
| GWE ± SD, % | 96 ± 2 | 95 ± 4 | 0.171 |
| Variables | Stage 0 (n = 36) | Stage 1 (n = 43) | Stage 2 (n = 65) | Stage 3–4 (n = 26) | p Value |
|---|---|---|---|---|---|
| GWI ± SD, mmHg% | 2609 ± 503 | 2495 ± 549 | 2611 ± 510 | 2264 ± 457 *,# | 0.024 |
| GCW ± SD, mmHg% | 2999 ± 633 | 2938 ± 645 | 3026 ± 564 | 2700 ± 507 | 0.119 |
| GWW ± SD, mmHg% | 131 ± 166 | 149 ± 92 | 139 ± 90 | 133 ± 90 | 0.901 |
| GWE ± SD, % | 95 ± 7 | 94 ± 3 | 95 ± 3 | 94 ± 3 | 0.917 |
| GLS ± SD, % | −20.0 ± 2.5 | −18.5 ± 2.6 | −18.6 ± 2.7 | −17.4 ± 3.2 * | 0.004 |
| Variables | Survivors (n = 134) | All-Cause Deaths (n = 27) | p Value |
|---|---|---|---|
| Clinical variables | |||
| Age ± SD, years | 68.4 ± 13.3 | 76.0 ± 9.4 | 0.005 |
| Male, gender n (%) | 77 (57) | 17 (63) | 0.597 |
| BMI ± SD, kg/m2 | 26.1 ± 4.0 | 28.0 ± 5.1 | 0.037 |
| BSA ± SD, m2 | 1.8 ± 0.2 | 1.8 ± 0.2 | 0.907 |
| Systolic arterial pressure ± SD, mmHg | 136.0 ± 18 | 135 ± 22 | 0.735 |
| Diastolic arterial pressure ± SD, mmHg | 73 ± 10 | 71 ± 9 | 0.262 |
| Loge-transformed BNP ± SD | 4.2 ± 1.3 | 5.1 ± 1.3 | 0.002 |
| Diabetes mellitus, n (%) | 27 (20) | 10 (37) | 0.045 |
| Hypertension, n (%) | 92 (69) | 17 (63) | 0.907 |
| Hypercholesterolemia, n (%) | 87 (133) | 16 (60) | 0.705 |
| Current smoking, n (%) | 26 (19) | 3 (11) | 0.319 |
| Coronary artery disease, n (%) | 15 (11) | 4 (15) | 0.502 |
| Previous PCI, n (%) | 12 (9) | 3 (11) | 0.639 |
| Chronic kidney disease, n (%) | 29 (22) | 9 (33) | 0.368 |
| Atrial fibrillation, n (%) | 5 (4) | 2 (7) | 0.391 |
| LV dimensions and geometry | |||
| Interventricular septum ± SD, mm | 10.5 ± 1.6 | 13.1 ± 1.9 | 0.063 |
| LV posterior wall ± SD, mm | 9.8 ± 2.0 | 11.0 ± 1.1 | 0.118 |
| LV end-diastolic diameter ± SD, mm | 45.1 ± 5.5 | 47.0 ± 7.1 | 0.132 |
| LV end-systolic diameter ± SD, mm | 29.9 ± 5.7 | 30.6 ± 6.1 | 0.619 |
| LV mass indexed ± SD, g/m2 | 101.7 ± 25.5 | 117.4 ± 28.1 | 0.007 |
| Relative wall thickness ± SD | 0.47 ± 0.10 | 0.48 ± 0.09 | 0.714 |
| Aortic valve severity | |||
| Mean Pressure Gradient ± SD, mmHg | 38.6 ± 14.8 | 38.3 ± 17.1 | 0.942 |
| Peak aortic Velocity ± SD, m/s | 3.9 ± 0.7 | 3.8 ± 0.7 | 0.605 |
| Aortic Valve Area ± SD, cm2 | 1.00 ± 0.35 | 1.01 ± 0.26 | 0.725 |
| Indexed aortic valve area ± SD, cm2/m2 | 0.54 ± 0.18 | 0.55 ± 0.15 | 0.664 |
| Indexed Stroke Volume ± SD, mL/m2 | 47.8 ± 10.6 | 48.9 ± 14.3 | 0.664 |
| Zva ± SD, mmHg/mL/m2 | 3.8 ± 1.0 | 3.8 ± 1.3 | 0.930 |
| LV systolic and diastolic function | |||
| LV end-diastolic volume ± SD, mL | 93.8 ± 33.6 | 93.1 ± 39.3 | 0.925 |
| LV end-systolic volume ± SD, mL | 36.2 ± 16.4 | 37.3 ± 20.2 | 0.763 |
| LV EF ± SD, % | 62 ± 6 | 61 ± 7 | 0.281 |
| GLS ± SD, % | −19.0 ± 2.7 | −17.5 ± 3.3 | 0.016 |
| Indexed LA volume ± SD, mL/m2 | 33.4 ± 11.9 | 42.6 ± 16.9 | 0.002 |
| Mitral E/A ratio ± SD | 0.9 ± 0.3 | 0.8 ± 0.2 | 0.050 |
| E/e’ ± SD, average | 11.8 ± 4.3 | 11.9 ± 3.7 | 0.924 |
| TTPG ± SD, mmHg | 26.5 ± 8.2 | 26.8 ± 8.8 | 0.900 |
| TAPSE ± SD, mm | 22.8 ± 3.28 | 21.3 ± 4.0 | 0.072 |
| S’ ± SD, cm/s | 12.6 ± 2.7 | 12.9 ± 3.3 | 0.694 |
| Right atrial volume ± SD, mL | 38.2 ± 16.3 | 39.8 ± 17.4 | 0.681 |
| Myocardial work | |||
| GWI ± SD, mmHg% | 2603 ± 503 | 2307 ± 532 | 0.006 |
| GCW ± SD, mmHg% | 3040 ± 582 | 2647 ± 602 | 0.002 |
| GWW ± SD, mmHg% | 137 ± 113 | 152 ± 96 | 0.513 |
| GWE ± SD, % | 95 ± 4 | 94 ± 3 | 0.199 |
| Variable | Univariable | Multivariable | ||
|---|---|---|---|---|
| HR (95%CI) | p-Value | HR (95%CI) | p-Value | |
| Model 1 | ||||
| Age, years | 1.063 (1.021–1.107) | 0.003 | 1.051 (0.991–1.115) | 0.099 |
| Loge-transformed BNP | 2.180 (1.448–3.281) | <0.001 | 1.877 (1.011–3.484) | 0.046 |
| BMI, kg/m2 | 1.091 (1.001–1.188) | 0.047 | 1.231 (1.046–1.449) | 0.012 |
| LV mass indexed, g/m2 | 1.023 (1.009–1.038) | 0.001 | 1.027 (1.007–1.047) | 0.008 |
| Indexed LA volume, mL/m2 | 1.053 (1.023–1.084) | <0.001 | 0.986 (0.937–1.039) | 0.602 |
| AVR treatment | 3.083 (1.342–7.080) | 0.008 | 0.336 (0.093–1.212) | 0.096 |
| GLS, % | 1.202 (1.045–1.382) | 0.010 | 1.286 (1.014–1.631) | 0.038 |
| GWI, mmHg% | 0.999 (0.998–1.000) | 0.003 | 0.998 (0.997–0.999) | 0.024 |
| Model 2 | ||||
| Age | 1.063 (1.021–1.107) | 0.003 | 1.070 (1.004–1.141) | 0.037 |
| Loge -transformed BNP | 2.180 (1.448–3.281) | <0.001 | 1.772 (0.939–3.344) | 0.077 |
| BMI, kg/m2 | 1.091 (1.001–1.188) | 0.047 | 1.232 (1.039–1.439) | 0.026 |
| LV mass indexed, g/m2 | 1.023 (1.009–1.038) | 0.001 | 1.032 (1.009–1.056) | 0.003 |
| Indexed LA volume, mL/m2 | 1.053 (1.023–1.084) | <0.001 | 1.010 (0.965–1.057) | 0.672 |
| AVR treatment | 3.083 (1.342–7.080) | 0.008 | 0.287 (0.080–1.025) | 0.055 |
| GLS, % | 1.202 (1.045–1.382) | 0.010 | 1.305 (1.035–1.645) | 0.025 |
| GCW, mmHg% | 0.999 (0.998–1.000) | <0.001 | 0.998 (0.997–0.999) | 0.003 |
| Variable | Univariable | Multivariable | ||
|---|---|---|---|---|
| HR (95%CI) | p-Value | HR (95%CI) | p-Value | |
| Model 1 | ||||
| Age, years | 1.077 (1.028–1.128) | 0.002 | 1.051 (0.985–1.122) | 0.132 |
| Loge-transformed BNP | 2.099 (1.371–3.213) | 0.001 | 2.245 (1.236–4.077) | 0.008 |
| BMI, kg/m2 | 1.088 (0.992–1.192) | 0.074 | 1.157 (0.998–1.340) | 0.053 |
| LV mass indexed, g/m2 | 1.027 (1.012–1.043) | 0.001 | 1.027 (1.005–1.049) | 0.014 |
| Indexed LA volume, mL/m2 | 1.053 (1.020–1.086) | 0.001 | 1.019 (0.973–1.067) | 0.421 |
| AVR treatment | 3.619 (1.419–9.228) | 0.007 | 0.451 (0.120–1.698) | 0.239 |
| GLS, % | 1.157 (0.996–1.343) | 0.057 | 1.291 (1.010–1.649) | 0.042 |
| GWI, mmHg% | 0.999 (0.998–1.000) | 0.018 | 0.998 (0.997–1.000) | 0.034 |
| Model 2 | ||||
| Age, years | 1.077 (1.028–1.128) | 0.002 | 1.075 (1.005–1.151) | 0.035 |
| Loge-transformed BNP | 2.099 (1.371–3.213) | 0.001 | 1.877 (0.931–3.782) | 0.078 |
| BMI, kg/m2 | 1.088 (0.992–1.192) | 0.074 | 1.125 (0.970–1.304) | 0.120 |
| LV mass indexed, g/m2 | 1.027 (1.012–1.043) | 0.001 | 1.030 (1.009–1.051) | 0.005 |
| Indexed LA volume, mL/m2 | 1.053 (1.020–1.086) | 0.001 | 1.014 (0.967–1.057) | 0.578 |
| AVR treatment | 3.619 (1.419–9.228) | 0.007 | 0.402 (0.108–1.500) | 0.175 |
| GLS, % | 1.157 (0.996–1.343) | 0.057 | 1.477 (1.122–1.945) | 0.005 |
| GCW, mmHg% | 0.999 (0.998–1.000) | 0.003 | 0.998 (0.997–0.999) | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilardi, F.; Postolache, A.; Dulgheru, R.; Trung, M.-L.N.; de Marneffe, N.; Sugimoto, T.; Go, Y.Y.; Oury, C.; Esposito, G.; Lancellotti, P. Prognostic Value of Non-Invasive Global Myocardial Work in Asymptomatic Aortic Stenosis. J. Clin. Med. 2022, 11, 1555. https://doi.org/10.3390/jcm11061555
Ilardi F, Postolache A, Dulgheru R, Trung M-LN, de Marneffe N, Sugimoto T, Go YY, Oury C, Esposito G, Lancellotti P. Prognostic Value of Non-Invasive Global Myocardial Work in Asymptomatic Aortic Stenosis. Journal of Clinical Medicine. 2022; 11(6):1555. https://doi.org/10.3390/jcm11061555
Chicago/Turabian StyleIlardi, Federica, Adriana Postolache, Raluca Dulgheru, Mai-Linh Nguyen Trung, Nils de Marneffe, Tadafumi Sugimoto, Yun Yun Go, Cécile Oury, Giovanni Esposito, and Patrizio Lancellotti. 2022. "Prognostic Value of Non-Invasive Global Myocardial Work in Asymptomatic Aortic Stenosis" Journal of Clinical Medicine 11, no. 6: 1555. https://doi.org/10.3390/jcm11061555
APA StyleIlardi, F., Postolache, A., Dulgheru, R., Trung, M.-L. N., de Marneffe, N., Sugimoto, T., Go, Y. Y., Oury, C., Esposito, G., & Lancellotti, P. (2022). Prognostic Value of Non-Invasive Global Myocardial Work in Asymptomatic Aortic Stenosis. Journal of Clinical Medicine, 11(6), 1555. https://doi.org/10.3390/jcm11061555