
Yearly Incidence of Stroke and Bleeding in Atrial Fibrillation with Concomitant Hyperthyroidism: A National Discharge Database Study

 , ,
, ,  and
and
Abstract
:1. Introduction
Aims
2. Methods
Statistical Analysis
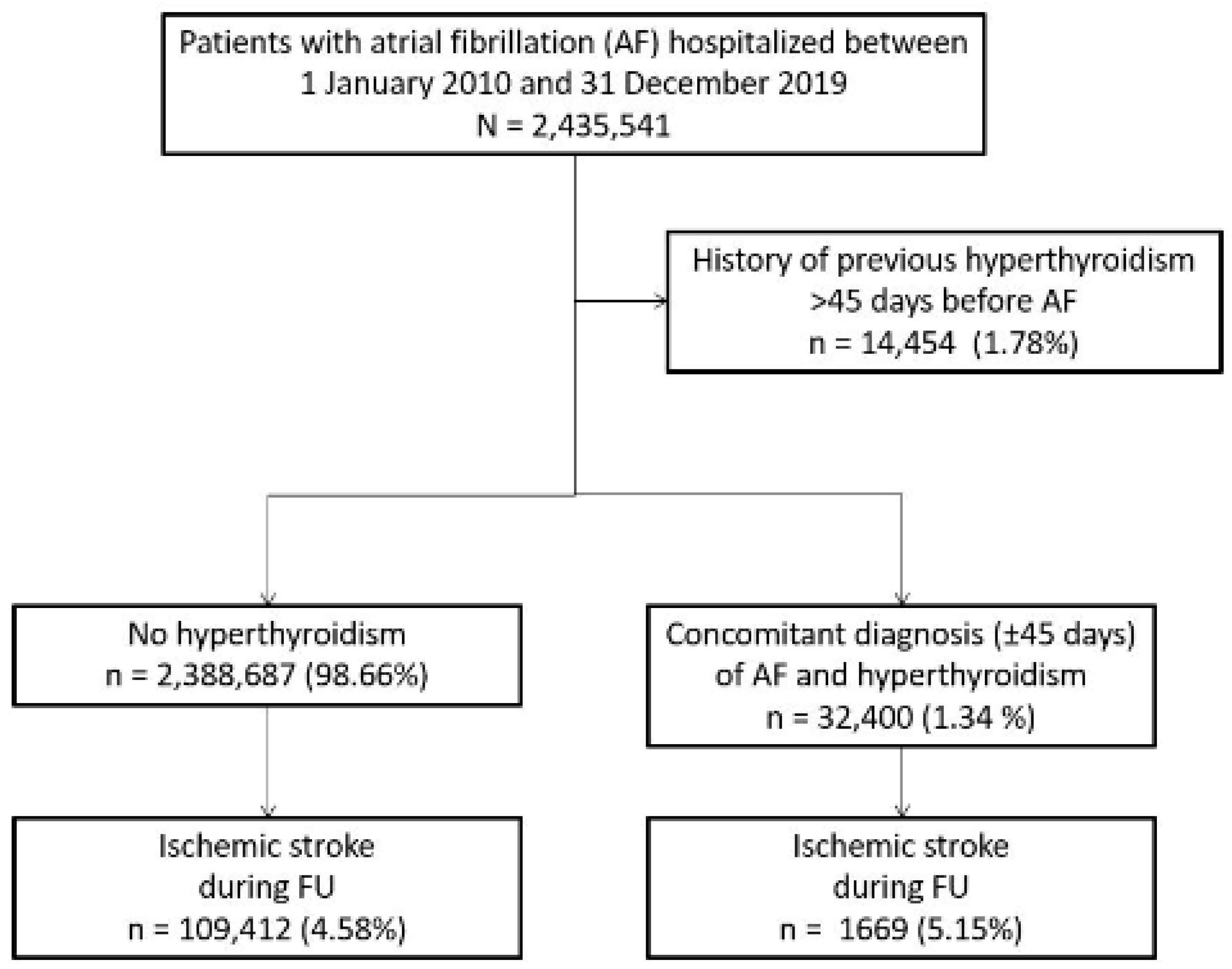
3. Results
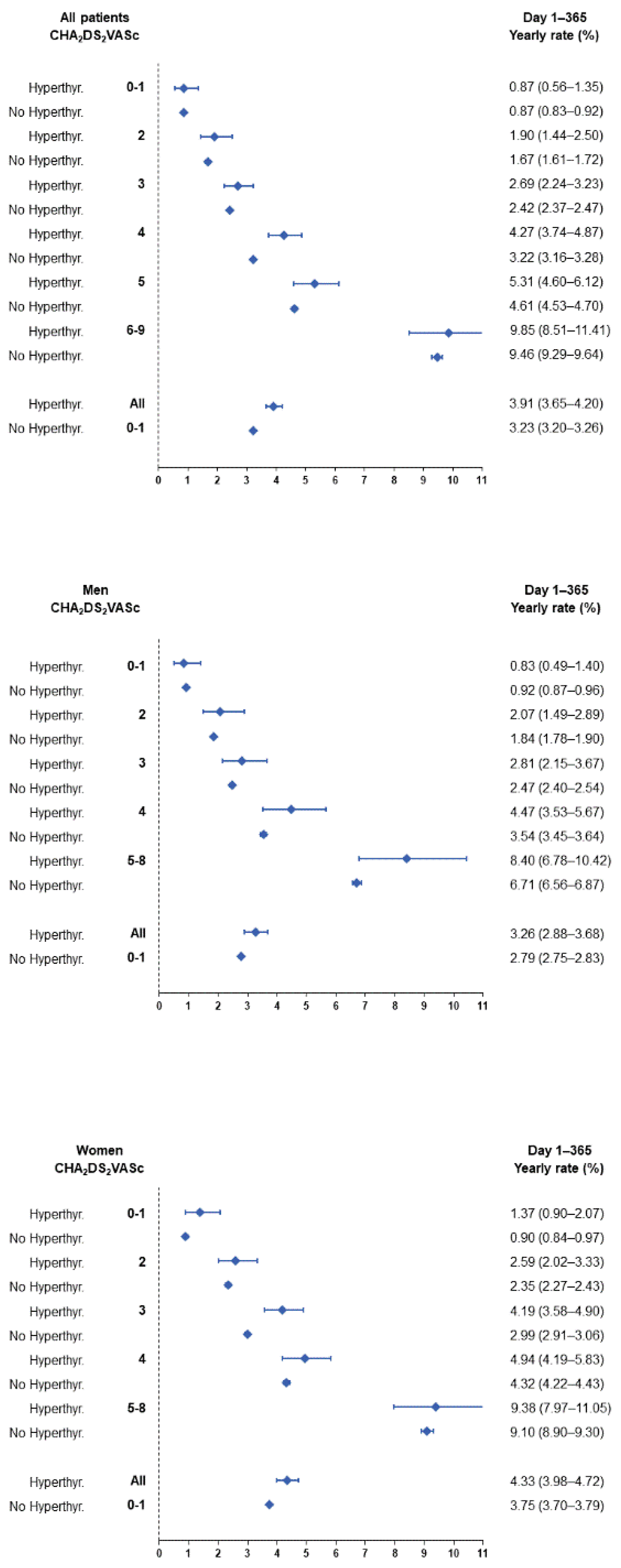
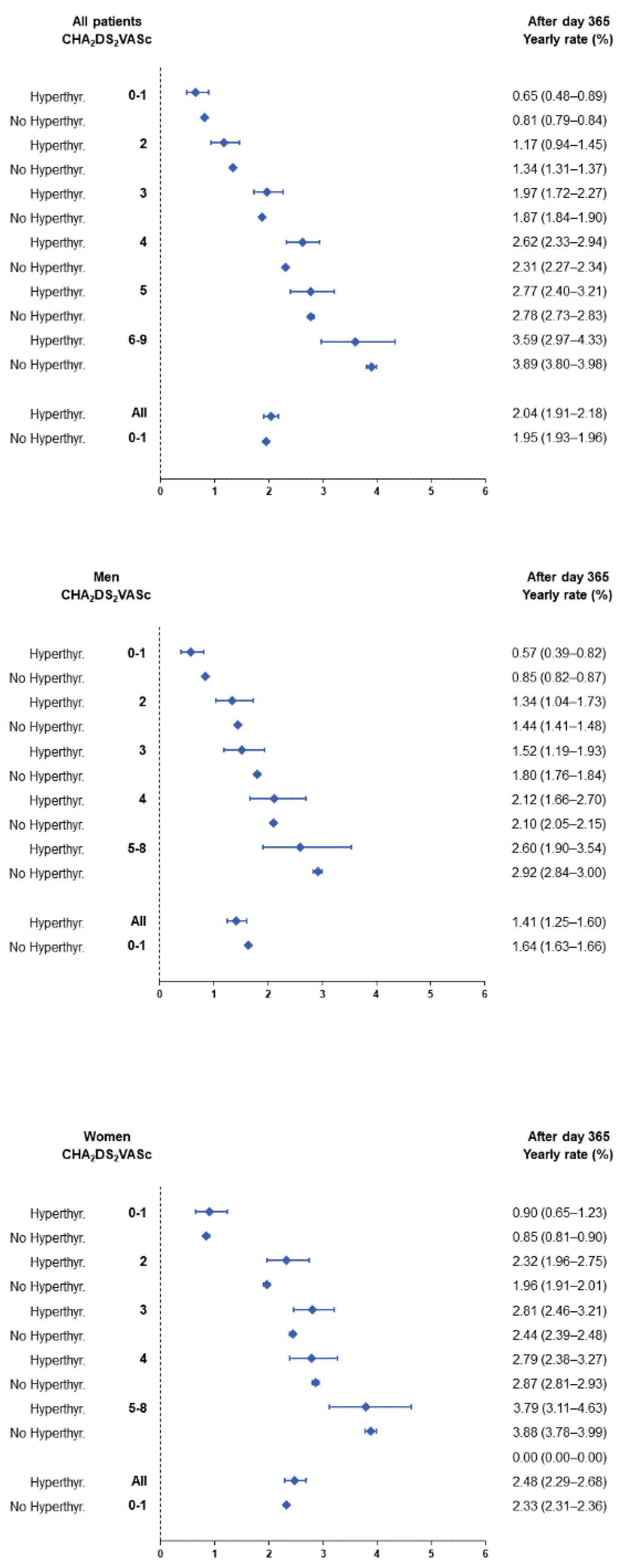
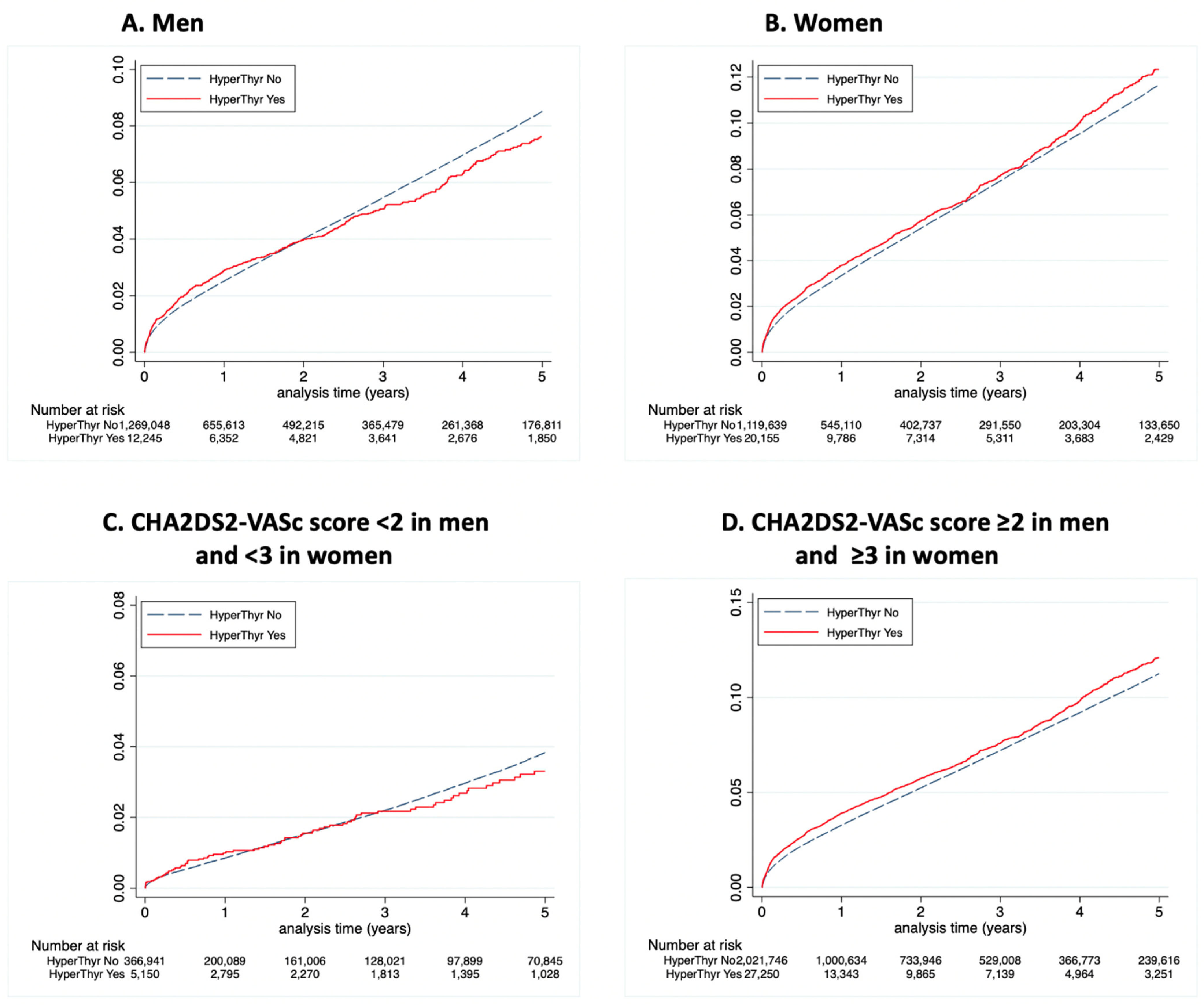
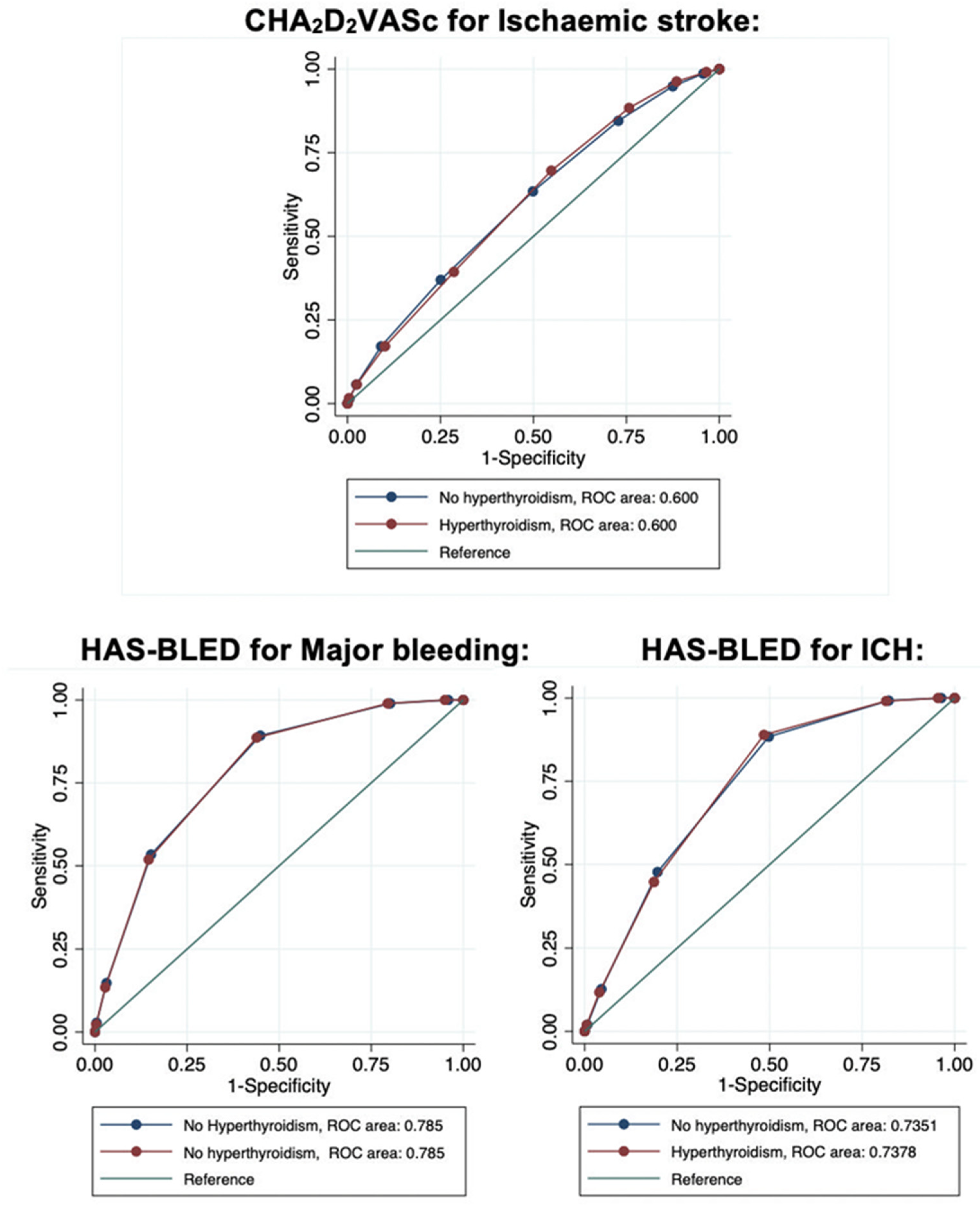
3.1. Hyperthyroidism and Ischaemic Stroke
3.2. Hyperthyroidism and Mortality
3.3. Bleeding Events and HAS-BLED Score
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Flynn, R.W.V.; MacDonald, T.; Morris, A.D.; Jung, R.T.; Leese, G.P. The Thyroid Epidemiology, Audit, and Research Study: Thyroid Dysfunction in the General Population. J. Clin. Endocrinol. Metab. 2004, 89, 3879–3884. [Google Scholar] [CrossRef] [PubMed]
- Petersen, P.; Hansen, J.M. Stroke in thyrotoxicosis with atrial fibrillation. Stroke 1988, 19, 15–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selmer, C.; Olesen, J.B.; Hansen, M.L.; Lindhardsen, J.; Olsen, A.-M.S.; Madsen, J.C.; Faber, J.; Hansen, P.R.; Pedersen, O.D.; Torp-Pedersen, C.; et al. The spectrum of thyroid disease and risk of new onset atrial fibrillation: A large population cohort study. BMJ 2012, 345, e7895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selmer, C.; Hansen, M.L.; Olesen, J.B.; Mérie, C.; Lindhardsen, J.; Olsen, A.-M.S.; Madsen, J.C.; Schmidt, U.; Faber, J.; Hansen, P.R.; et al. New-Onset Atrial Fibrillation Is a Predictor of Subsequent Hyperthyroidism: A Nationwide Cohort Study. PLoS ONE 2013, 8, e57893. [Google Scholar] [CrossRef] [Green Version]
- Sohn, S.Y.; Lee, E.; Lee, M.K.; Lee, J.H. The Association of Overt and Subclinical Hyperthyroidism with the Risk of Cardiovascular Events and Cardiovascular Mortality: Meta-Analysis and Systematic Review of Cohort Studies. Endocrinol. Metab. 2020, 35, 786–800. [Google Scholar] [CrossRef]
- Cutlip, D.E.; Windecker, S.; Mehran, R.; Boam, A.; Cohen, D.J.; van Es, G.-A.; Steg, P.G.; Morel, M.-A.; Mauri, L.; Vrancks, P.; et al. Clinical end points in coronary stent trials: A case for standardized definitions. Circulation 2007, 115, 2344–2351. [Google Scholar] [CrossRef] [Green Version]
- Chen, Q.; Yan, Y.; Zhang, L.; Cheng, K.; Liu, Y.; Zhu, W. Effect of Hyperthyroidism on the Hypercoagulable State and Thromboembolic Events in Patients with Atrial Fibrillation. Cardiology 2014, 127, 176–182. [Google Scholar] [CrossRef]
- Bruere, H.; Fauchier, L.; Brunet, A.B.; Pierre, B.; Simeon, E.; Babuty, D.; Clementy, N. History of Thyroid Disorders in Relation to Clinical Outcomes in Atrial Fibrillation. Am. J. Med. 2015, 128, 30–37. [Google Scholar] [CrossRef]
- Sheu, J.J.; Kang, J.-H.; Lin, H.-C.; Lin, H.-C. Hyperthyroidism and risk of ischemic stroke in young adults: A 5-year follow-up study. Stroke 2010, 41, 961–966. [Google Scholar] [CrossRef] [Green Version]
- Marouli, E.; Kus, A.; Del Greco, M.F.; Chaker, L.; Peeters, R.; Teumer, A.; Deloukas, P.; Medici, M. Thyroid Function Affects the Risk of Stroke via Atrial Fibrillation: A Mendelian Randomization Study. J. Clin. Endocrinol. Metab. 2020, 105, 2634–2641. [Google Scholar] [CrossRef]
- Dekkers, O.M.; Horváth-Puhó, E.; Cannegieter, S.C.; Vandenbroucke, J.P.; Sørensen, H.T.; Jørgensen, J.O.L. Acute cardiovascular events and all-cause mortality in patients with hyperthyroidism: A population-based cohort study. Eur. J. Endocrinol. 2017, 176, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.; Yang, P.-S.; Jang, E.; Yu, H.T.; Kim, T.-H.; Uhm, J.-S.; Kim, J.-Y.; Sung, J.-H.; Pak, H.-N.; Lee, M.-H.; et al. Increased risk of ischemic stroke and systemic embolism in hyperthyroidism-related atrial fibrillation: A nationwide cohort study. Am. Hear. J. 2021, 242, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Siu, C.-W.; Pong, V.; Zhang, X.; Chan, Y.-H.; Jim, M.-H.; Liu, S.; Yiu, K.-H.; Kung, A.W.; Lau, C.-P.; Tse, H.-F. Risk of ischemic stroke after new-onset atrial fibrillation in patients with hyperthyroidism. Hear. Rhythm 2009, 6, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Elbers, L.P.B.; Moran, C.; Gerdes, V.E.; van Zaane, B.; Meijers, J.; Endert, E.; Lyons, G.; Chatterjee, V.K.; Bisschop, P.H.; Fliers, E. The Hypercoagulable state in Hyperthyroidism is mediated via the Thyroid Hormone beta Receptor pathway. Eur. J. Endocrinol. 2016, 174, 755–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yildiz, C.; Altay, M.; Yildiz, S.; Çağir, Y.; Akkan, T.; Ünsal, Y.A.; Beyan, E. Arterial stiffness in hyperthyroid patients is deteriorated due to thyroid hormones. Arch. Endocrinol. Metab. 2019, 63, 258–264. [Google Scholar] [CrossRef]
- Tsai, M.-S.; Chuang, P.-Y.; Shih, S.-R.; Chang, W.-T.; Chen, N.-C.; Yu, P.-H.; Cheng, H.-J.; Tang, C.-H.; Chen, W.-J. Better adherence to antithyroid drug is associated with decreased risk of stroke in hyperthyroidism patients. Int. J. Clin. Practic. 2015, 69, 1473–1485. [Google Scholar] [CrossRef]
- Lillevang-Johansen, M.; Abrahamsen, B.; Jørgensen, H.L.; Brix, T.H.; Hegedüs, L. Duration of Hyperthyroidism and Lack of Sufficient Treatment Are Associated with Increased Cardiovascular Risk. Thyroid 2019, 29, 332–340. [Google Scholar] [CrossRef]
- Chan, Y.-H.; Wu, L.-S.; See, L.-C.; Liu, J.-R.; Chang, S.-H.; Chao, T.-F.; Yeh, Y.-H.; Kuo, C.-T.; Lee, H.-F.; Lip, G.Y.H. Direct Oral Anticoagulants in Atrial Fibrillation Patients With Concomitant Hyperthyroidism. J. Clin. Endocrinol. Metab. 2020, 105, 2893–2904. [Google Scholar] [CrossRef]
- E Okosieme, O.; Taylor, P.N.; Evans, C.; Thayer, D.; Chai, A.; Khan, I.; Draman, M.S.; Tennant, B.; Geen, J.; Sayers, A.; et al. Primary therapy of Graves’ disease and cardiovascular morbidity and mortality: A linked-record cohort study. Lancet Diabetes Endocrinol. 2019, 7, 278–287. [Google Scholar] [CrossRef]
- Fauchier, L.; Clementy, N.; Bisson, A.; Stamboul, K.; Ivanes, F.; Angoulvant, D.; Babuty, D.; Lip, G.Y.H. Prognosis in patients with atrial fibrillation and a presumed “temporary cause” in a community-based cohort study. Clin. Res. Cardiol. 2016, 106, 202–210. [Google Scholar] [CrossRef]
- Lin, Y.-S.; Tsai, H.-Y.; Lin, C.-Y.; Wu, V.C.-C.; Chen, T.-H.; Yang, T.-Y.; Aboyans, V.; Chen, M.-C. Risk of Thromboembolism in Non-Valvular Atrial Fibrillation With or Without Clinical Hyperthyroidism. Glob. Hear. 2021, 16, 45. [Google Scholar] [CrossRef] [PubMed]
- Krahn, A.D.; Klein, G.J.; Kerr, C.R.; Boone, J.; Sheldon, R.; Green, M.; Talajic, M.; Wang, X.; Connolly, S. How useful is thyroid function testing in patients with recent-onset atrial fibrillation? The Canadian Registry of Atrial Fibrillation Investigators. Arch. Intern. Med. 1996, 156, 2221–2224. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, S.A.; Green, J.; Huber, K.; Wojdyla, D.M.; Lopes, R.D.; Alexander, J.H.; Vinereanu, D.; Wallentin, L.; Granger, C.B.; Al-Khatib, S.M. Characteristics and Outcomes of Atrial Fibrillation in Patients with Thyroid Disease (from the Aristotle Trial). Am. J. Cardiol. 2019, 124, 1406–1412. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No Hyperthyroidism | Hyperthyroidism | p | Total | |
|---|---|---|---|---|
| (n = 2,388,687) | (n = 32,400) | (n = 2,421,087) | ||
| Age, years | 77.2 ± 12.1 | 77.0 ± 12.5 | 0.01 | 77.2 ± 12.1 |
| Sex (male) | 1,269,048 (53.1) | 12,245 (37.8) | <0.0001 | 1,281,293 (52.9) |
| CHA2DS2VASc score | 3.5 ± 1.6 | 3.6 ± 1.6 | <0.0001 | 3.5 ± 1.6 |
| HAS-BLED score | 2.4 ± 1.2 | 2.3 ± 1.2 | <0.0001 | 2.4 ± 1.2 |
| Charlson comorbidity index | 3.5 ± 2.8 | 3.4 ± 2.7 | 0.34 | 3.5 ± 2.8 |
| Frailty index | 9.2 ± 9.1 | 10.5 ± 9.4 | <0.0001 | 9.3 ± 9.1 |
| Hypertension | 1,428,261 (59.8) | 19,496 (60.2) | 0.17 | 1,447,757 (59.8) |
| Diabetes mellitus | 498,572 (20.9) | 6706 (20.7) | 0.44 | 505,278 (20.9) |
| Heart failure | 861,573 (36.1) | 13,234 (40.8) | <0.0001 | 874,807 (36.1) |
| History of pulmonary oedema | 59,076 (2.5) | 725 (2.2) | 0.01 | 59,801 (2.5) |
| Mitral regurgitation | 139,496 (5.8) | 2180 (6.7) | <0.0001 | 141,676 (5.9) |
| Aortic regurgitation | 58,330 (2.4) | 807 (2.5) | 0.57 | 59,137 (2.4) |
| Aortic stenosis | 146,768 (6.1) | 1742 (5.4) | <0.0001 | 148,510 (6.1) |
| Previous endocarditis | 10,537 (0.4) | 110 (0.3) | 0.01 | 10,647 (0.4) |
| Dilated cardiomyopathy | 164,626 (6.9) | 2720 (8.4) | <0.0001 | 167,346 (6.9) |
| Coronary artery disease | 584,941 (24.5) | 6798 (21.0) | <0.0001 | 591,739 (24.4) |
| Previous myocardial infarction | 116,836 (4.9) | 1354 (4.2) | <0.0001 | 118,190 (4.9) |
| Previous PCI | 95,351 (4.0) | 978 (3.0) | <0.0001 | 96,329 (4.0) |
| Previous CABG | 78,453 (3.3) | 713 (2.2) | <0.0001 | 79,166 (3.3) |
| Vascular disease | 419,415 (17.6) | 5003 (15.4) | <0.0001 | 424,418 (17.5) |
| Previous pacemaker or ICD | 92,335 (3.9) | 998 (3.1) | <0.0001 | 93,333 (3.9) |
| Previous ischaemic stroke | 170,283 (7.1) | 1953 (6.0) | <0.0001 | 172,236 (7.1) |
| Previous intracranial bleeding | 51,496 (2.2) | 582 (1.8) | <0.0001 | 52,078 (2.2) |
| Smoker | 159,153 (6.7) | 2136 (6.6) | 0.61 | 161,289 (6.7) |
| Dyslipidaemia | 513,732 (21.5) | 6107 (18.8) | <0.0001 | 519,839 (21.5) |
| Obesity | 339,579 (14.2) | 4174 (12.9) | <0.0001 | 343,753 (14.2) |
| Alcohol-related diagnoses | 120,241 (5.0) | 1208 (3.7) | <0.0001 | 121,449 (5.0) |
| Abnormal renal function | 162,550 (6.8) | 2265 (7.0) | 0.19 | 164,815 (6.8) |
| Lung disease | 393,587 (16.5) | 5458 (16.8) | 0.08 | 399,045 (16.5) |
| Sleep apnoea syndrome | 124,669 (5.2) | 1323 (4.1) | <0.0001 | 125,992 (5.2) |
| COPD | 223,243 (9.3) | 3063 (9.5) | 0.51 | 226,306 (9.3) |
| Liver disease | 86,786 (3.6) | 1105 (3.4) | 0.03 | 87,891 (3.6) |
| History of hypothyroidism | 168,451 (7.1) | 2550 (7.9) | <0.0001 | 171,001 (7.1) |
| Inflammatory disease | 141,804 (5.9) | 1954 (6.0) | 0.48 | 143,758 (5.9) |
| Anaemia | 404,101 (16.9) | 5647 (17.4) | 0.01 | 409,748 (16.9) |
| Previous cancer | 420,077 (17.6) | 4843 (14.9) | <0.0001 | 424,920 (17.6) |
| Univariate Analysis HR, 95%CI | p | Multivariable Analysis HR, 95%CI | p | |
|---|---|---|---|---|
| Age, years | 1.038 (1.038–1.039) | <0.0001 | 1.034 (1.033–1.035) | <0.0001 |
| Sex (male) | 0.721 (0.712–0.729) | <0.0001 | 0.863 (0.853–0.875) | <0.0001 |
| Hypertension | 1.279 (1.263–1.295) | <0.0001 | 1.052 (1.038–1.066) | <0.0001 |
| Diabetes mellitus | 1.148 (1.132–1.164) | <0.0001 | 1.185 (1.168–1.202) | <0.0001 |
| Heart failure with congestion | 1.095 (1.081–1.110) | <0.0001 | 1.053 (1.037–1.068) | <0.0001 |
| History of pulmonary oedema | 0.987 (0.944–1.033) | 0.57 | 1.002 (0.957–1.050) | 0.92 |
| Mitral regurgitation | 0.984 (0.959–1.010) | 0.22 | 0.973 (0.947–0.999) | 0.05 |
| Aortic regurgitation | 0.999 (0.961–1.038) | 0.97 | 0.975 (0.937–1.015) | 0.22 |
| Aortic stenosis | 1.060 (1.034–1.087) | <0.0001 | 1.009 (0.983–1.035) | 0.50 |
| Previous endocarditis | 1.388 (1.279–1.506) | <0.0001 | 1.402 (1.290–1.522) | <0.0001 |
| Dilated cardiomyopathy | 0.940 (0.918–0.963) | <0.0001 | 1.053 (1.027–1.079) | <0.0001 |
| Coronary artery disease | 1.013 (0.999–1.027) | 0.07 | 0.998 (0.981–1.015) | 0.78 |
| Previous myocardial infarction | 1.122 (1.091–1.155) | <0.0001 | 1.029 (0.994–1.064) | 0.11 |
| Previous PCI | 0.949 (0.918–0.980) | 0.002 | 0.969 (0.934–1.005) | 0.09 |
| Previous CABG | 0.914 (0.884–0.946) | <0.0001 | 0.956 (0.923–0.992) | 0.02 |
| Vascular disease | 1.249 (1.230–1.267) | <0.0001 | 1.167 (1.146–1.188) | <0.0001 |
| Previous pacemaker or ICD | 1.012 (0.980–1.045) | 0.47 | 0.915 (0.886–0.945) | <0.0001 |
| Previous ischaemic stroke | 5.207 (5.133–5.282) | <0.0001 | 4.681 (4.612–4.750) | <0.0001 |
| Previous intracranial bleeding | 2.588 (2.507–2.672) | <0.0001 | 1.719 (1.664–1.775) | <0.0001 |
| Smoker | 0.839 (0.817–0.861) | <0.0001 | 1.137 (1.105–1.170) | <0.0001 |
| Dyslipidaemia | 1.022 (1.008–1.037) | 0.002 | 0.928 (0.914–0.942) | <0.0001 |
| Obesity | 0.765 (0.751–0.780) | <0.0001 | 0.875 (0.858–0.893) | <0.0001 |
| Alcohol related diagnoses | 0.957 (0.930–0.985) | 0.003 | 1.244 (1.205–1.283) | <0.0001 |
| Abnormal renal function | 1.167 (1.138–1.197) | <0.0001 | 1.021 (0.995–1.048) | 0.12 |
| Lung disease | 0.920 (0.904–0.936) | <0.0001 | 0.979 (0.956–1.003) | 0.09 |
| Sleep apnoea syndrome | 0.718 (0.697–0.740) | <0.0001 | 0.908 (0.879–0.936) | <0.0001 |
| COPD | 0.789 (0.771–0.808) | <0.0001 | 0.853 (0.826–0.882) | <0.0001 |
| Liver disease | 0.893 (0.860–0.927) | <0.0001 | 0.991 (0.952–1.030) | 0.64 |
| Hyperthyroidism | 1.114 (1.061–1.169) | <0.0001 | 1.133 (1.080–1.189) | <0.0001 |
| History of hypothyroidism | 1.050 (1.026–1.074) | <0.0001 | 0.939 (0.918–0.962) | <0.0001 |
| Inflammatory disease | 1.070 (1.043–1.098) | <0.0001 | 0.979 (0.954–1.005) | 0.11 |
| Anaemia | 1.146 (1.127–1.165) | <0.0001 | 1.078 (1.059–1.096) | <0.0001 |
| Previous cancer | 0.905 (0.888–0.922) | <0.0001 | 0.941 (0.923–0.958) | <0.0001 |
| All Patients, Hyperthyroidism | All Patients, No Hyperthyroidism | Men, Hyperthyroidism | Men, No Hyperthyroidism | Women, History of Hyperthyroidism | Women, No History of Hyperthyroidism | |
| All-cause death | ||||||
| Whole FU | 12.4 (12.2–12.7) | 12.7 (12.6–12.7) | 12.6 (12.1–13.0) | 12.6 (12.5–12.6) | 12.3 (12.0–12.7) | 12.8 (12.7–12.8) |
| Day 1–365 | 21.7 (21.1–22.3) | 22.8 (22.7–22.9) | 22.4 (21.4–23.5) | 22.6 (22.5–22.7) | 21.2 (20.4–22.0) | 23.1 (22.9–23.2) |
| After Day 365 | 8.3 (8.0-8.6) | 8.2 (8.1-8.2) | 8.3 (7.9-8.8) | 8.2 (8.2-8.2) | 8.2 (7.9-8.6) | 8.1 (8.1-8.1) |
| Cardiovascular death | ||||||
| Whole FU | 3.9 (3.7–4.0) | 3.8 (3.8–3.9) | 3.5 (3.3–3.7) | 3.4 (3.4–3.5) | 4.2 (4.0–4.4) | 4.3 (4.3–4.3) |
| Day 1–365 | 6.9 (6.5–7.3) | 7.2 (7.1–7.2) | 6.1 (5.6–6.7) | 6.4 (6.4–6.5) | 7.4 (6.9–7.9) | 8.1 (8.0–8.2) |
| After Day 365 | 2.6 (2.4–2.7) | 2.3 (2.3–2.4) | 2.4 (2.2–2.7) | 2.2 (2.1–2.2) | 2.7 (2.5–2.9) | 2.6 (2.6–2.6) |
| Whole FU | Day 1–365 | After Day 365 | |
| All-cause mortality | |||
| All patients | 0.973 (0.952–0.994) | 0.939 (0.911–0.968) | 1.016 (0.983–1.049) |
| Men | 0.997 (0.963–1.032) | 0.982 (0.937–1.029) | 1.014 (0.965–1.067) |
| Women | 0.957 (0.930–0.985) | 0.910 (0.876–0.946) | 1.018 (0.976–1.062) |
| Cardiovascular mortality | |||
| All patients | 1.006 (0.967–1.046) | 0.946 (0.897–0.998) | 1.088 (1.027–1.153) |
| Men | 1.015 (0.951–1.083) | 0.940 (0.859–1.028) | 1.110 (1.011–1.219) |
| Women | 0.955 (0.909–1.003) | 0.904 (0.846–0.965) | 1.030 (0.957–1.110) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, J.; Bisson, A.; Fauchier, G.; Bodin, A.; Herbert, J.; Ducluzeau, P.H.; Lip, G.Y.H.; Fauchier, L. Yearly Incidence of Stroke and Bleeding in Atrial Fibrillation with Concomitant Hyperthyroidism: A National Discharge Database Study. J. Clin. Med. 2022, 11, 1342. https://doi.org/10.3390/jcm11051342
Zhang J, Bisson A, Fauchier G, Bodin A, Herbert J, Ducluzeau PH, Lip GYH, Fauchier L. Yearly Incidence of Stroke and Bleeding in Atrial Fibrillation with Concomitant Hyperthyroidism: A National Discharge Database Study. Journal of Clinical Medicine. 2022; 11(5):1342. https://doi.org/10.3390/jcm11051342
Chicago/Turabian StyleZhang, Juqian, Arnaud Bisson, Grégoire Fauchier, Alexandre Bodin, Julien Herbert, Pierre Henri Ducluzeau, Gregory Y. H. Lip, and Laurent Fauchier. 2022. "Yearly Incidence of Stroke and Bleeding in Atrial Fibrillation with Concomitant Hyperthyroidism: A National Discharge Database Study" Journal of Clinical Medicine 11, no. 5: 1342. https://doi.org/10.3390/jcm11051342
APA StyleZhang, J., Bisson, A., Fauchier, G., Bodin, A., Herbert, J., Ducluzeau, P. H., Lip, G. Y. H., & Fauchier, L. (2022). Yearly Incidence of Stroke and Bleeding in Atrial Fibrillation with Concomitant Hyperthyroidism: A National Discharge Database Study. Journal of Clinical Medicine, 11(5), 1342. https://doi.org/10.3390/jcm11051342