
Influence of Static Navigation Technique on the Accuracy of Autotransplanted Teeth in Surgically Created Sockets


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
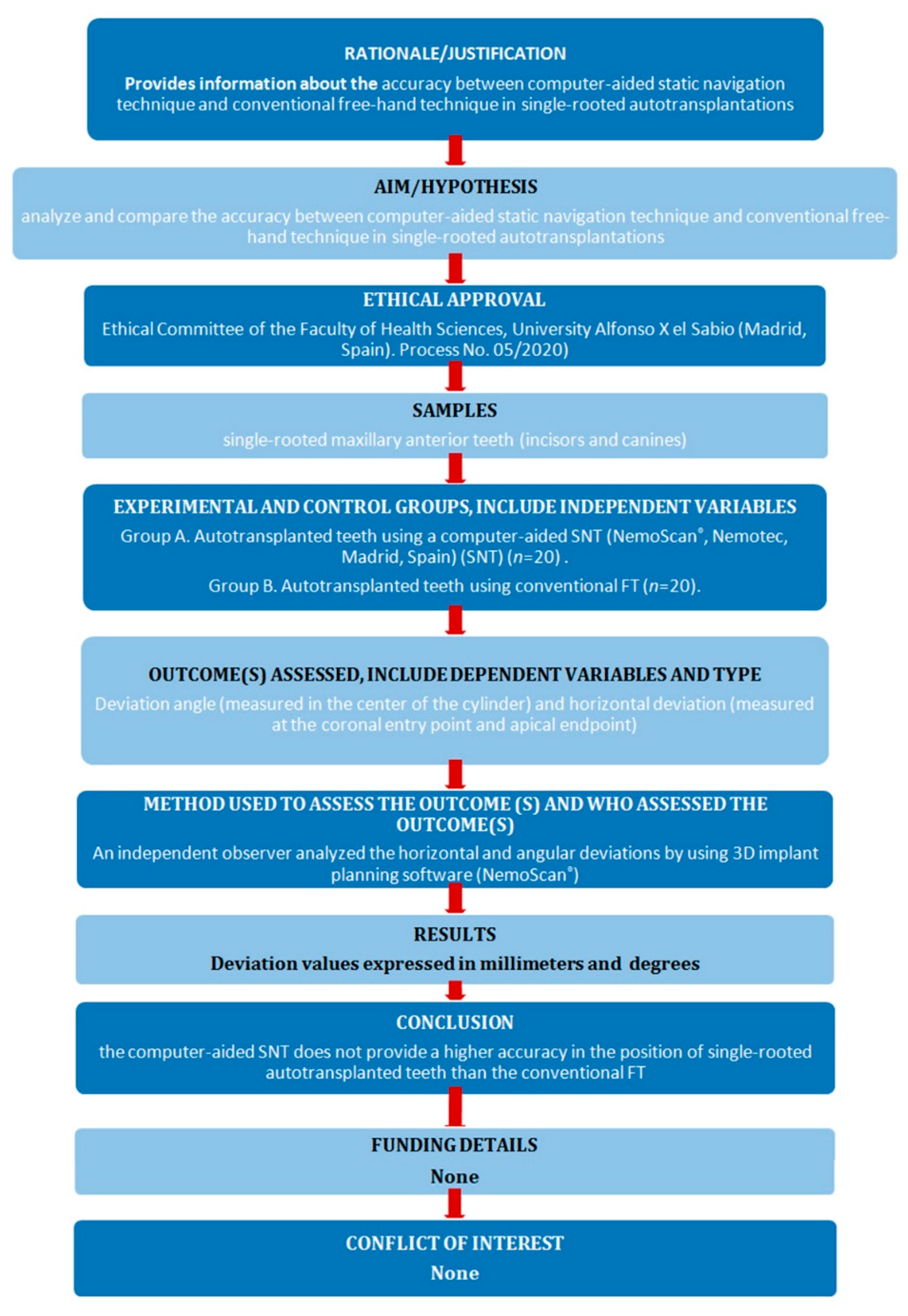
2.1. Study Design
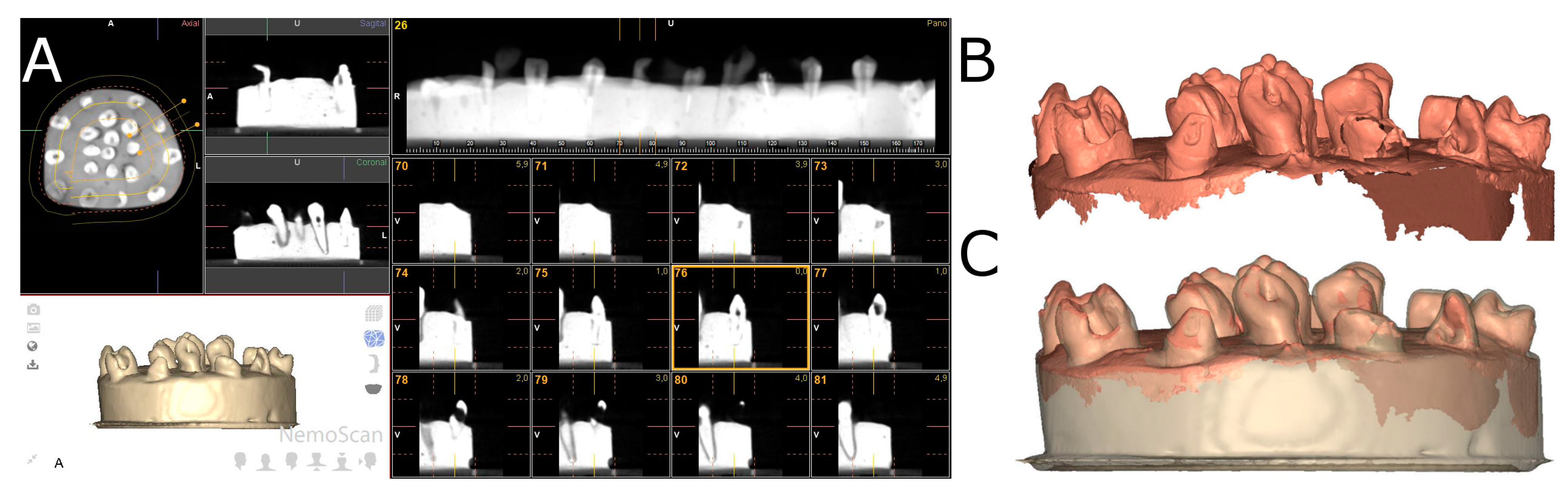
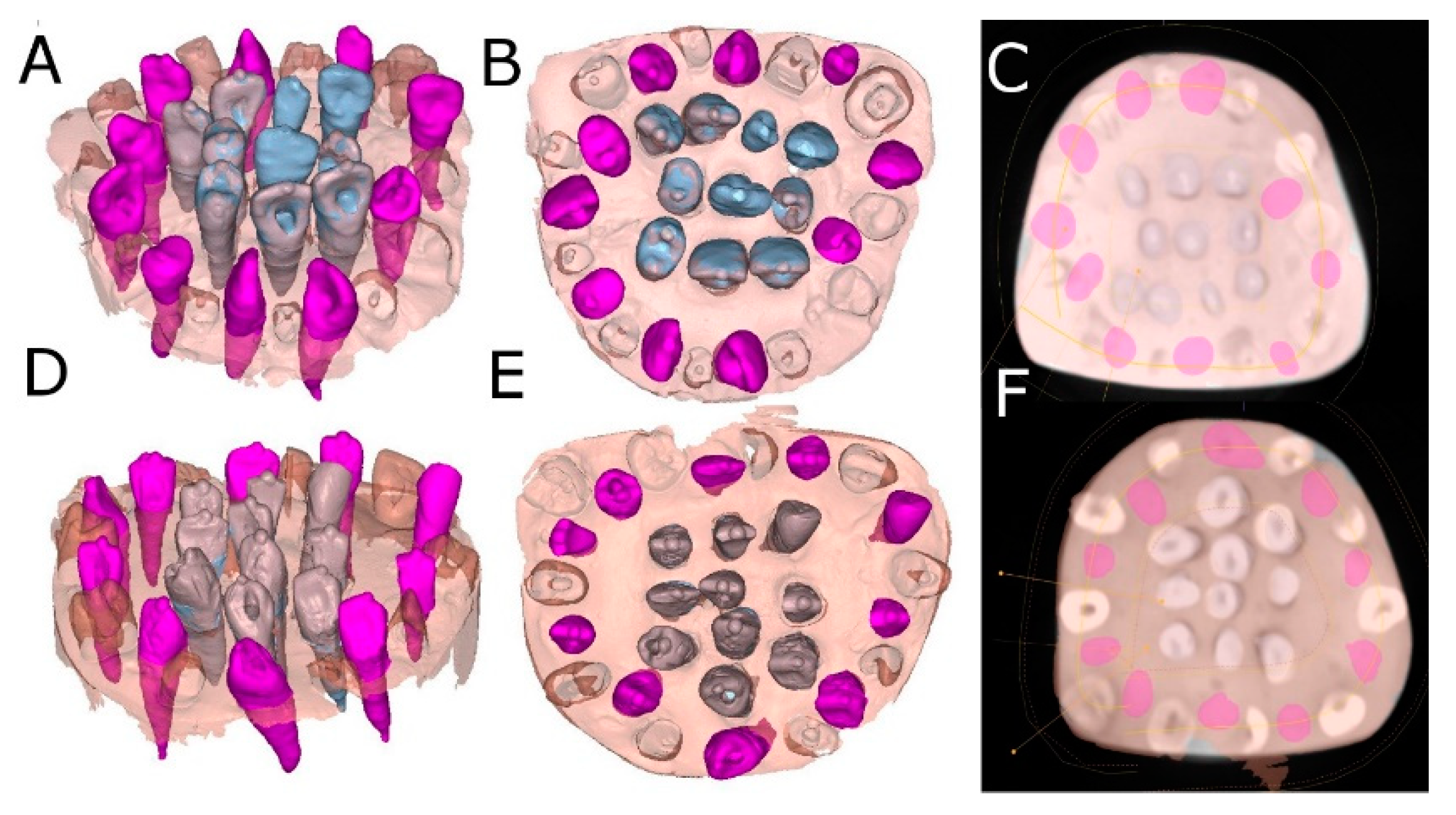
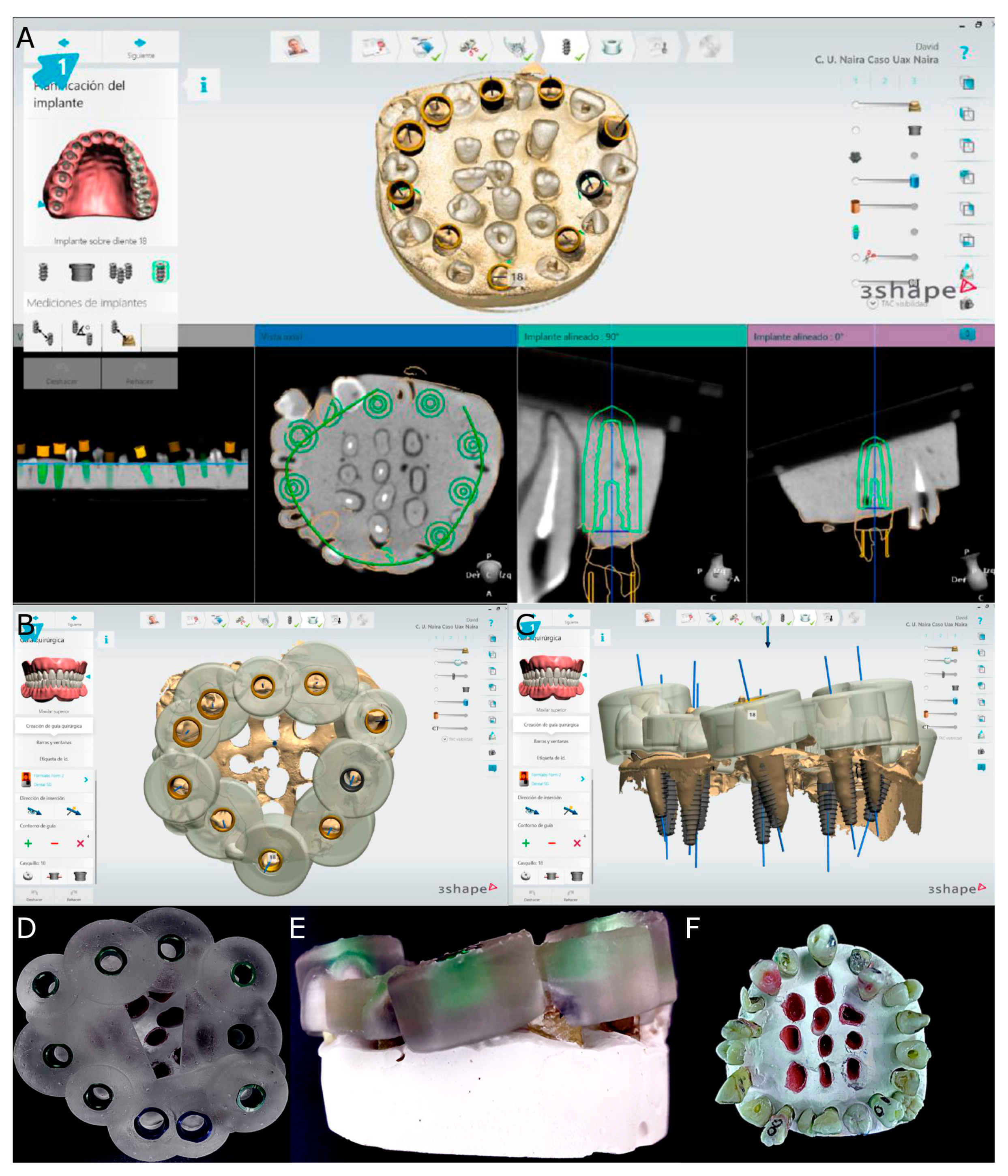
2.2. Experimental Procedure
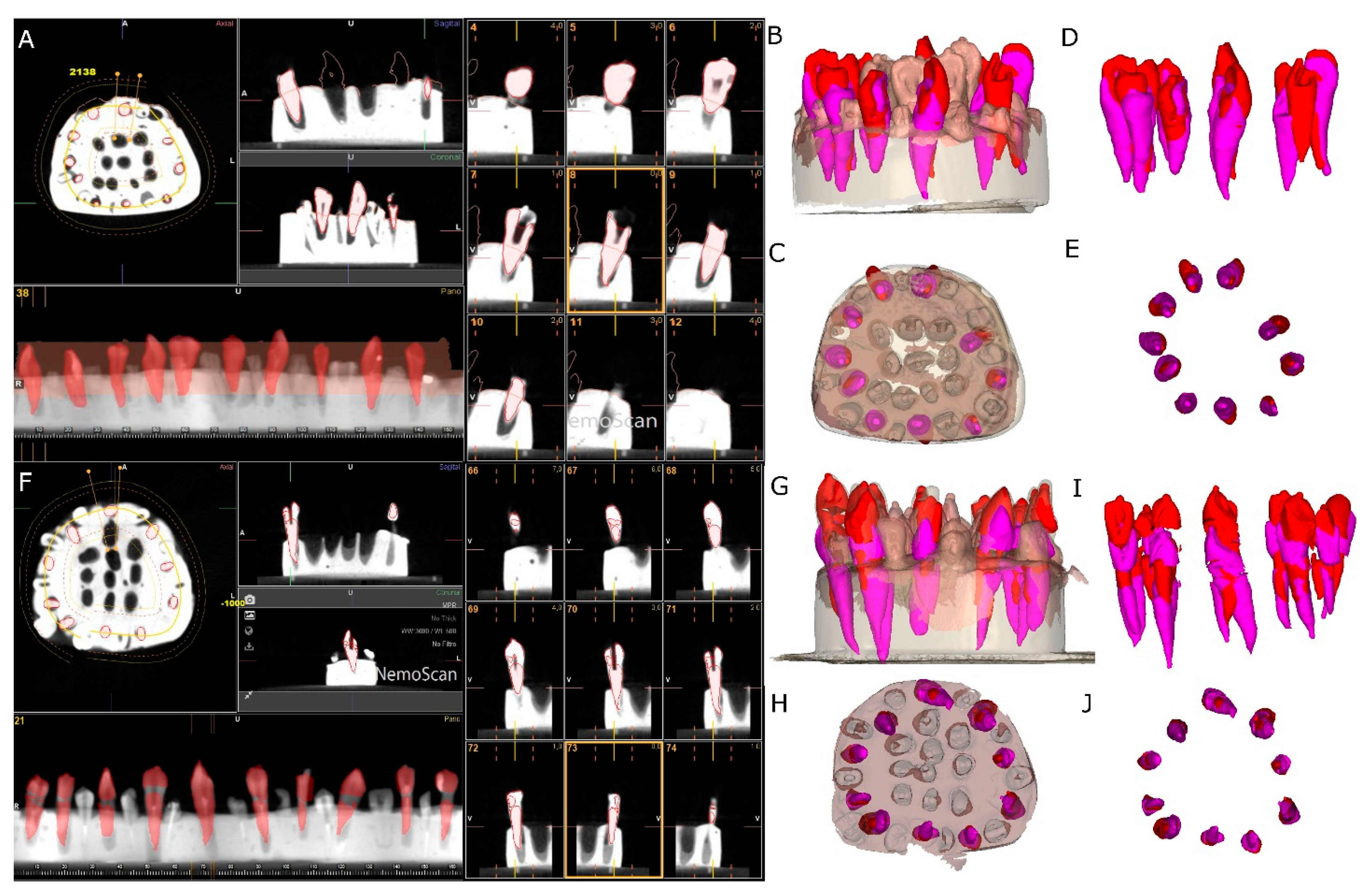
2.3. Measurement Procedure
2.4. Statistical Tests
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Natiella, J.R.; Armitage, J.E.; Greene, G.W. The replantation and transplantation of teeth. A review. Oral Surg. Oral Med. Oral Pathol. 1970, 29, 397–419. [Google Scholar] [CrossRef]
- Andreasen, J.O.; Paulsen, H.U.; Yu, Z.; Bayer, T.; Schwartz, O. A long-term study of 370 autotransplanted premolars. Part II. Tooth survival and pulp healing subsequent to transplantation. Eur. J. Orthod. 1990, 12, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Tsukiboshi, M. Autotransplantation of teeth: Requirements for predictable success. Dent. Traumatol. 2002, 18, 157–180. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Tai, K.; Hayashi, D. Tooth autotransplantation as a treatment option: A review. J. Clin. Pediatr. Dent. 2010, 35, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Lee, S.J.; Shin, Y.; Kim, E. Vertical bone growth after autotransplantation ofmature third molars: 2 case reports with long-term follow-up. J. Endod. 2015, 41, 1371–1374. [Google Scholar] [CrossRef]
- Chung, W.C.; Tu, Y.K.; Lin, Y.H.; Lu, H.K. Outcomes of autotransplanted teeth with complete root formation: A systematic review and meta-analysis. J. Clin. Periodontol. 2014, 41, 412–423. [Google Scholar] [CrossRef]
- Almpani, K.; Papageorgiou, S.N.; Papadopoulos, M.A. Autotransplantation of teeth in humans: A systematic review and meta-analysis. Clin. Oral Investig. 2015, 19, 1157–1179. [Google Scholar] [CrossRef]
- Apfel, H. Autoplasty of enucleated prefunctional third molars. J. Oral Surg. 1950, 8, 289–296. [Google Scholar]
- Miller, H.M. Transplantation; a case report. J. Am. Dent. Assoc. 1950, 40, 237. [Google Scholar]
- Lundberg, T.; Isaksson, S. A clinical follow-up study of 278 autotransplanted teeth. Br. J. Oral Maxillofac. Surg. 1996, 34, 181–185. [Google Scholar] [CrossRef]
- Mejàre, B.; Wannfors, K.; Jansson, L. A prospective study on transplantation of third molars with complete root formation. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2004, 97, 231–238. [Google Scholar] [CrossRef]
- Kumar, R.; Khambete, N.; Priya, E. Successful immediate autotransplantation of tooth with incomplete root formation: Case report. Oral Surg. Oral. Med. Oral Pathol. Oral Radiol. Endod. 2013, 115, e16–e21. [Google Scholar] [CrossRef] [PubMed]
- Slagsvold, O.; Bjercke, B. Applicability of autotransplantation in cases of missing upper anterior teeth. Am. J. Orthod. 1978, 74, 410–421. [Google Scholar] [CrossRef]
- Slagsvold, O.; Bjercke, B. Indications for autotransplantation in cases of missing premolars. Am. J. Orthod. 1978, 74, 241–257. [Google Scholar] [CrossRef]
- Kristerson, L.; Lagerstrom, L. Autotransplantation of teeth in cases with agenesis or traumatic loss of maxillary incisors. Eur. J. Orthod. 1991, 13, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Nethander, G. Autogenous free tooth transplantation with a two-stage operation technique. Swed. Dent. J. 2003, 161, 1–51. [Google Scholar]
- Kitahara, T.; Nakasima, A.; Shiatuschi, Y. Orthognathic treatment with autotransplantation of impacted maxillary third molar. Angle Orthod. 2009, 79, 401–406. [Google Scholar] [CrossRef] [Green Version]
- Czochrowska, E.M.; Stenvik, A.; Bjercke, B.; Zachrisson, B.U. Outcome of tooth transplantation: Survival and success rates 17-41 years posttreatment. Am. J. Orthod. Dent. Orthop. 2002, 121, 110–119. [Google Scholar] [CrossRef] [Green Version]
- Bae, J.H.; Choi, Y.H.; Cho, B.H.; Kim, Y.K.; Kim, S.G. Autotransplantation of teeth with complete root formation: A case series. J. Endod. 2010, 36, 1422–1426. [Google Scholar] [CrossRef]
- Sugai, T.; Yoshizawa, M.; Kobayashi, T.; Ono, K.; Takagi, R.; Kitamura, N.; Okiji, K.; Saito, C. Clinical study on prognostic factors for autotransplantation of teeth with complete root formation. Int. J. Oral Maxillofac. Surg. 2010, 39, 1193–1203. [Google Scholar] [CrossRef]
- Yu, H.J.; Jia, P.; Lv, Z.; Qiu, L.X. Autotransplantation of third molars with completely formed roots into surgically created sockets and fresh extraction sockets: A 10-year comparative study. Int. J. Oral Maxillofac. Surg. 2017, 46, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Jung, I.Y.; Lee, C.Y.; Choi, S.Y.; Kum, K.Y. Clinical application of computer-aided rapid prototyping for tooth transplantation. Dent. Traumatol. 2001, 17, 114–119. [Google Scholar] [CrossRef]
- Strbac, G.D.; Schnappauf, A.; Giannis, K.; Bertl, M.H.; Moritz, A.; Ulm, C. Guided autotransplantation of teeth: A novel method using virtually planned 3-dimensional templates. J. Endod. 2016, 42, 1844–1850. [Google Scholar] [CrossRef] [PubMed]
- Anssari Moin, D.; Verweij, J.P.; Waars, H.; van Merkesteyn, R.; Wismeijer, D. Accuracy of computer-assisted template-guided autotransplantation of teeth with custom three-dimensional designed/printed surgical tooling: A cadaveric study. J. Oral Maxillofac. Surg. 2017, 75, 925.e1–925.e7. [Google Scholar] [CrossRef] [PubMed]
- Verweij, J.P.; Jongkees, F.A.; Anssari Moin, D.; Wismeijer, D.; van Merkesteyn, J.P.R. Autotransplantation of teeth using computer-aided rapid prototyping of a three-dimensional replica of the donor tooth: A systematic literature review. Int. J. Oral Maxillofac. Surg. 2017, 46, 1466–1474. [Google Scholar] [CrossRef] [PubMed]
- Pogrel, M.A. Evaluation of over 400 autogenous tooth transplants. J. Oral Maxillofac. Surg. 1987, 45, 205–211. [Google Scholar] [CrossRef]
- Tahmaseb, A.; Wismeijer, D.; Coucke, W.; Derksen, W. Computer technology applications in surgical implant dentistry: A systematic review. Int. J. Oral Maxillofac. Implant. 2014, 29, 25–42. [Google Scholar] [CrossRef] [Green Version]
- Zubizarreta-Macho, Á.; Muñoz, A.P.; Deglow, E.R.; Agustín-Panadero, R.; Álvarez, J.M. Accuracy of Computer-Aided Dynamic Navigation Compared to Computer-Aided Static Procedure for Endodontic Access Cavities: An in Vitro Study. J. Clin. Med. 2020, 9, 129. [Google Scholar] [CrossRef] [Green Version]
- Nagendrababu, V.; Murray, P.E.; Ordinola-Zapata, R.; Peters, O.A.; Rôças, I.N.; Siqueira, J.F., Jr.; Priya, E.; Jayaraman, J.; Pulikkotil, S.J.; Dummer, P.M.H.; et al. PRILE 2021 guidelines for reporting laboratory studies in Endodontology: A consensus-based development. Int. Endod. J. 2021, 54, 1482–1490. [Google Scholar] [CrossRef]
- Nagendrababu, V.; Murray, P.E.; Ordinola-Zapata, R.; Peters, O.A.; Rôças, I.N.; Siqueira, J.F., Jr.; Priya, E.; Jayaraman, J.; Pulikkotil, S.J.; Dummer, P.M.H.; et al. PRILE 2021 guidelines for reporting laboratory studies in Endodontology: Explanation and elaboration. Int. Endod. J. 2021, 54, 1491–1515. [Google Scholar] [CrossRef]
- Renne, W.; Ludlow, M.; Fryml, J.; Schurch, Z.; Mennito, A.; Kessler, R.; Lauer, A. Evaluation of the accuracy of 7 digital scanners: An in vitro analysis based on 3-dimensional comparisons. J. Prosthet. Dent. 2017, 118, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Medina-Sotomayor, P.; Pascual-Moscardo, A.; Camps, A.I. Accuracy of 4 digital scanning systems on prepared teeth digitally isolated from a complete dental arch. J. Prosthet. Dent. 2019, 121, 811–820. [Google Scholar] [CrossRef] [PubMed]
- Abella Sans, F.; Ribas, F.; Doria, G.; Roig, M.; Durán-Sindreu, F. Guided tooth autotransplantation in edentulous areas post-orthodontic treatment. J. Esthet. Restor. Dent. 2021, 33, 685–691. [Google Scholar] [CrossRef] [PubMed]
- Plotino, G.; Abella Sans, F.; Duggal, M.S.; Grande, N.M.; Krastl, G.; Nagendrababu, V.; Gambarini, G. Clinical procedures and outcome of surgical extrusion, intentional replantation and tooth autotransplantation—A narrative review. Int. Endod. J. 2020, 53, 1636–1652. [Google Scholar] [CrossRef] [PubMed]
- Jang, Y.; Choi, Y.J.; Lee, S.J.; Roh, B.D.; Park, S.H.; Kim, E. Prognosis factors for clinical outcomes in autotransplantation in teeth with complete root formation: Survival analysis for up to 12 years. J. Endod. 2016, 42, 198–205. [Google Scholar] [CrossRef]
- Bauss, O.; Engelke, W.; Fenske, C.; Schilke, R.; Schwestka-Polly, R. Autotransplantation of immature third molars into edentulous and atrophied jaw sections. Int. J. Oral Maxillofac. Surg. 2004, 33, 558–563. [Google Scholar] [CrossRef]
- Bauss, O.; Zonios, I.; Rahman, A. Root development of immature third molars transplanted to surgically created sockets. J. Oral Maxillofac. Surg. 2008, 66, 1200–1211. [Google Scholar] [CrossRef]
- Kim, E.; Jung, J.Y.; Cha, I.H.; Kum, K.Y.; Lee, S.J. Evaluation of the prognosis and causes of failure in 182 cases of autogenous tooth transplantation. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2005, 100, 112–119. [Google Scholar] [CrossRef]
- Kafourou, V.; Tong, H.J.; Day, P.; Houghton, N.; Spencer, R.J.; Duggal, M. Outcomes and prognostic factors that influence the success of the tooth autotransplantation in children and adolescents. Dent. Traumatol. 2017, 33, 393–399. [Google Scholar] [CrossRef]
- Kristerson, L.; Andreasen, J.O. Autotransplantation and replantation of tooth germs in monkeys. Effect of damage to the dental follicle and position of transplant in the alveolus. Int. J. Oral Surg. 1984, 13, 324–333. [Google Scholar] [CrossRef]
- Andreasen, J.O.; Kristerson, L.; Andreasen, F.M. Damage of the Hertwig’s epithelial root sheath: Effect upon root growth after autotransplantation of teeth in monkeys. Endod. Dent. Traumatol. 1988, 4, 145–151. [Google Scholar] [CrossRef]
- Wu, D.; Zhou, L.; Yang, J.; Zhang, B.; Lin, Y.; Chen, J.; Huang, W.; Chen, Y. Accuracy of dynamic navigation compared to static surgical guide for dental implant placement. Int. J. Implant. Dent. 2020, 6, 78. [Google Scholar] [CrossRef] [PubMed]
- Cavuoti, S.; Matarese, G.; Isola, G.; Abdolreza, J.; Femiano, F.; Perillo, L. Combined orthodontic-surgical management of a transmigrated mandibular canine. Angle Orthod. 2016, 86, 681–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ender, A.; Zimmermann, M.; Mehl, A. Accuracy of complete- and partial-arch impressions of actual intraoral scanning systems in vitro. Int. J. Comput. Dent. 2019, 22, 11–19. [Google Scholar] [PubMed]
- Zimmermann, M.; Koller, C.; Rumetsch, M.; Ender, A.; Mehl, A. Precision of guided scanning procedures for full-arch digital impressions in vivo. J. Orofac. Orthop. 2017, 78, 466–471. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | Mean | Median | SD | Minimum | Maximum | ||
|---|---|---|---|---|---|---|---|
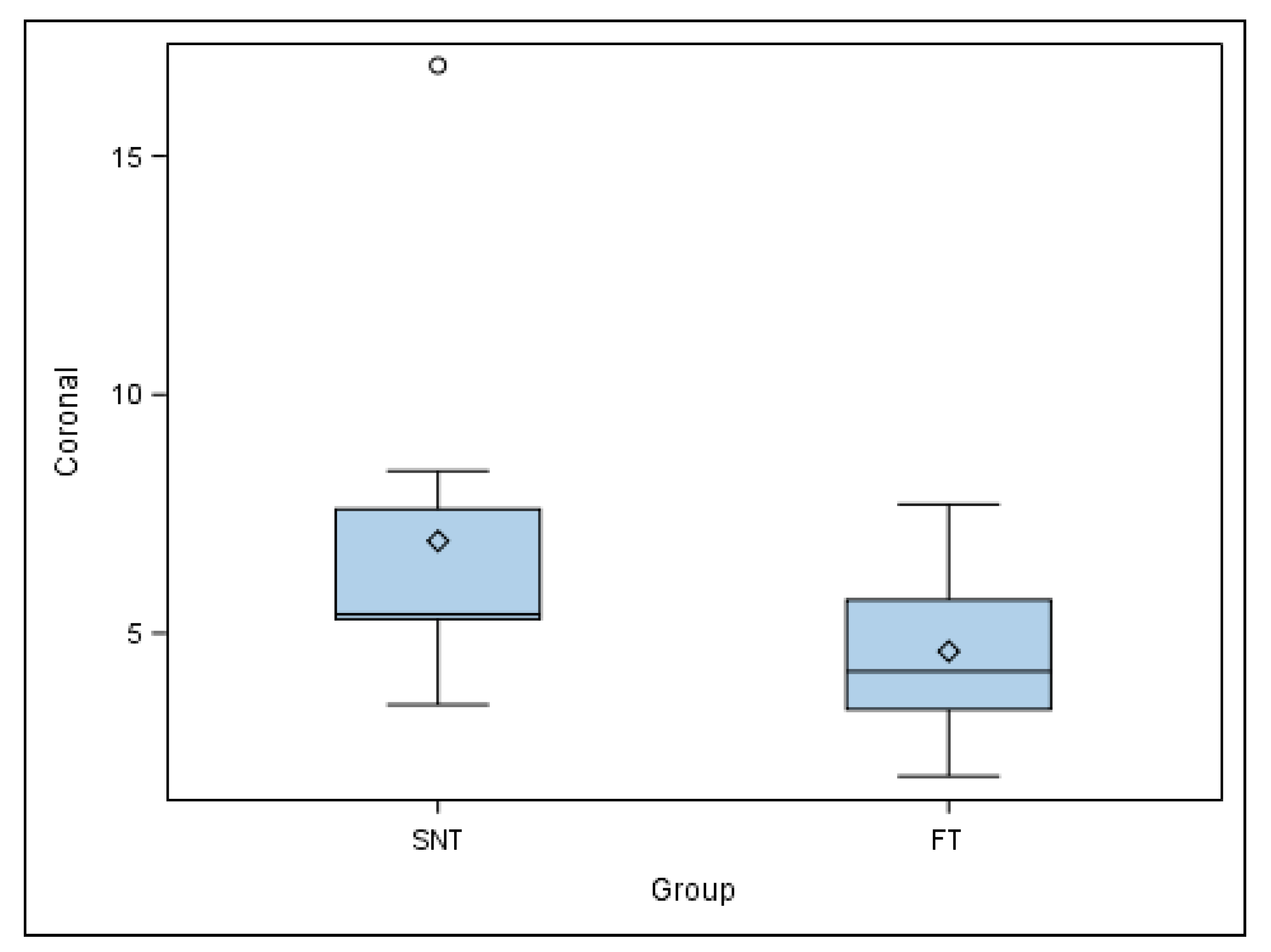
| SNT | Coronal | 10 | 6.93 | 5.40 a | 3.76 | 3.50 | 16.90 |
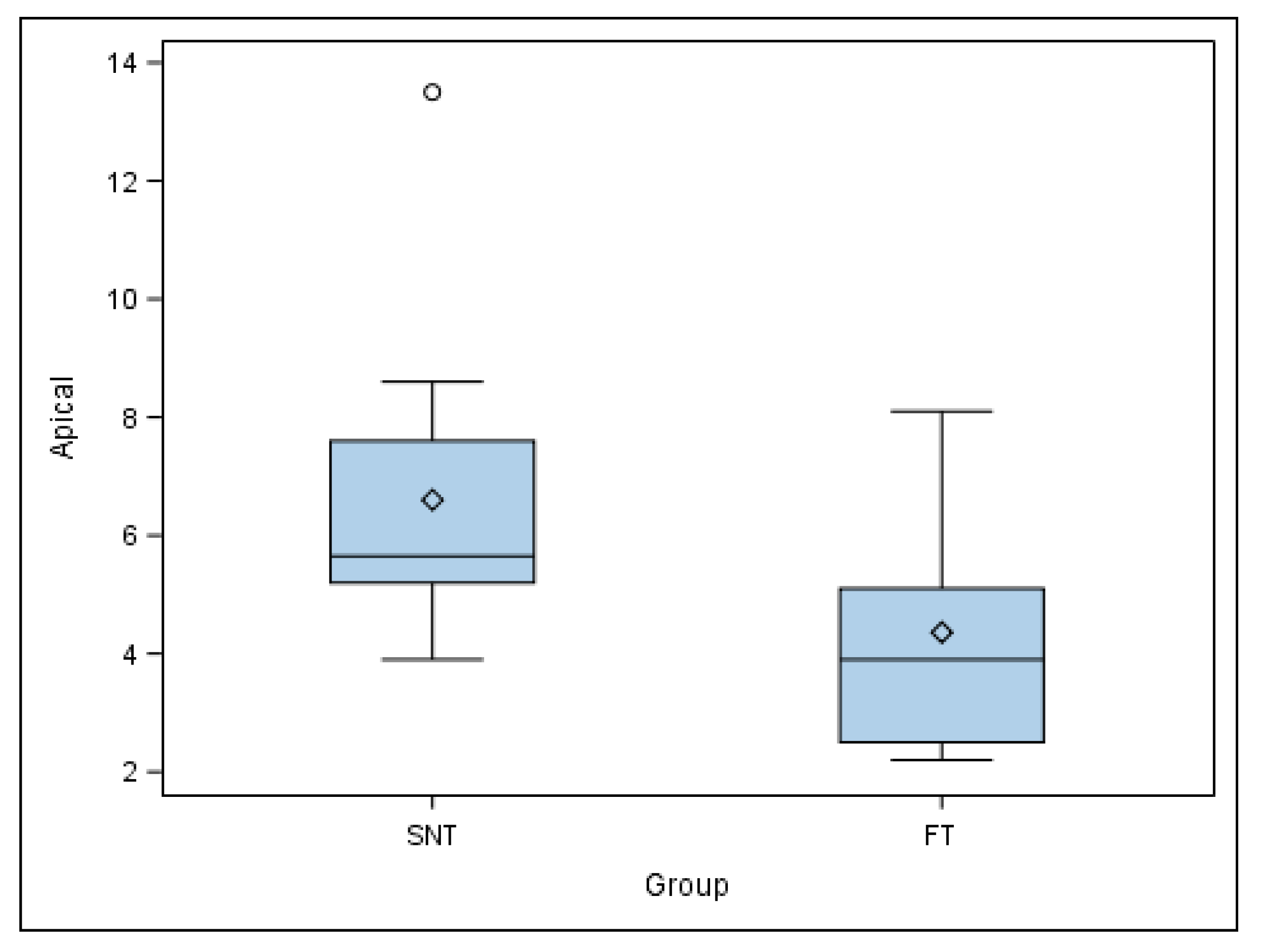
| Apical | 10 | 6.60 | 5.65 a | 2.81 | 3.90 | 13.50 | |
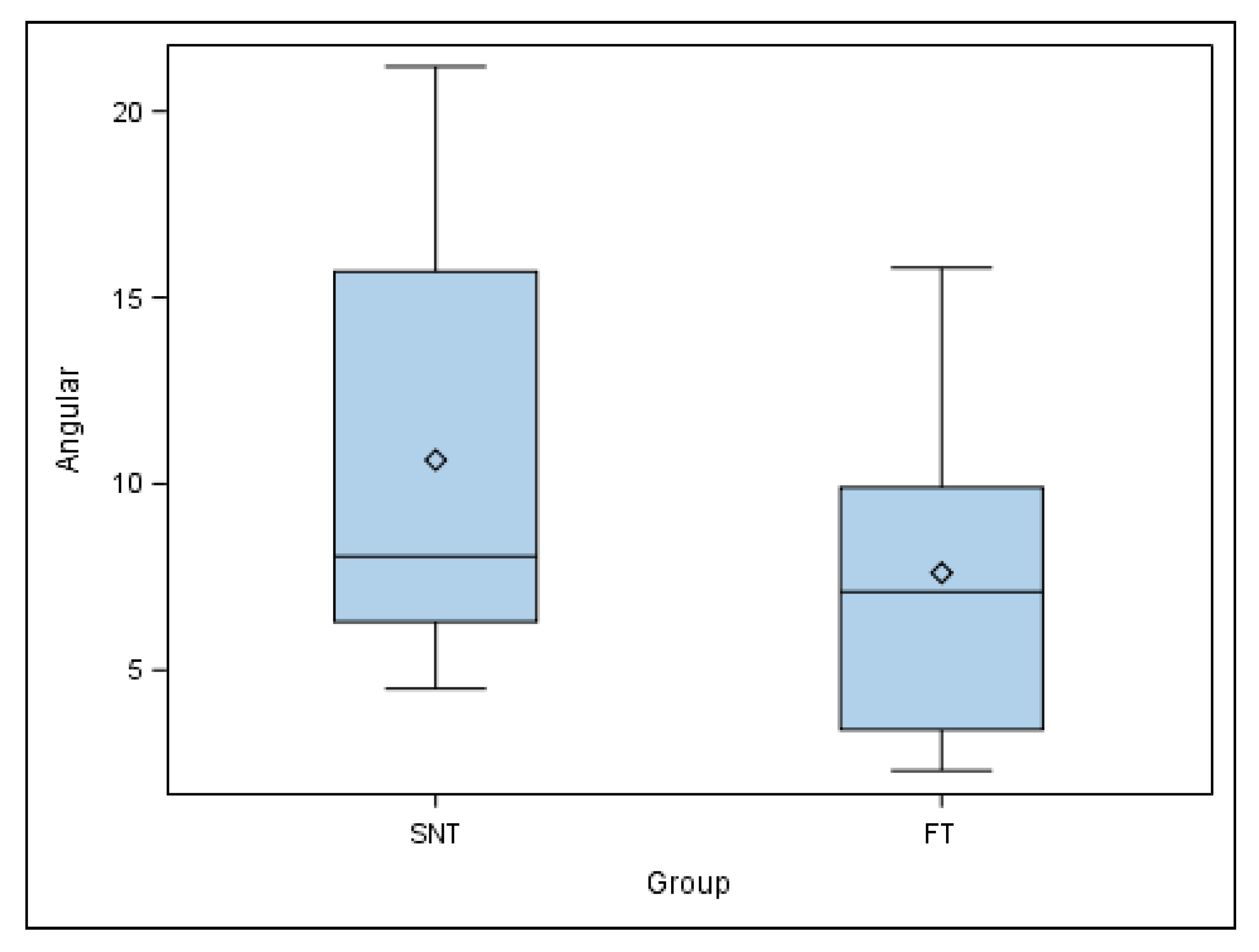
| Angular | 10 | 10.64 | 8.05 a | 5.78 | 4.50 | 21.20 | |
| FT | Coronal | 10 | 4.62 | 4.20 a | 1.85 | 2.00 | 7.70 |
| Apical | 10 | 4.36 | 3.90 b | 1.99 | 2.20 | 8.10 | |
| Angular | 10 | 7.61 | 7.10 a | 4.53 | 2.30 | 15.80 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riad Deglow, E.; Lazo Torres, N.Z.; Gutiérrez Muñoz, D.; Bufalá Pérez, M.; Galparsoro Catalán, A.; Zubizarreta-Macho, Á.; Abella Sans, F.; Hernández Montero, S. Influence of Static Navigation Technique on the Accuracy of Autotransplanted Teeth in Surgically Created Sockets. J. Clin. Med. 2022, 11, 1012. https://doi.org/10.3390/jcm11041012
Riad Deglow E, Lazo Torres NZ, Gutiérrez Muñoz D, Bufalá Pérez M, Galparsoro Catalán A, Zubizarreta-Macho Á, Abella Sans F, Hernández Montero S. Influence of Static Navigation Technique on the Accuracy of Autotransplanted Teeth in Surgically Created Sockets. Journal of Clinical Medicine. 2022; 11(4):1012. https://doi.org/10.3390/jcm11041012
Chicago/Turabian StyleRiad Deglow, Elena, Nayra Zurima Lazo Torres, David Gutiérrez Muñoz, María Bufalá Pérez, Agustín Galparsoro Catalán, Álvaro Zubizarreta-Macho, Francesc Abella Sans, and Sofía Hernández Montero. 2022. "Influence of Static Navigation Technique on the Accuracy of Autotransplanted Teeth in Surgically Created Sockets" Journal of Clinical Medicine 11, no. 4: 1012. https://doi.org/10.3390/jcm11041012
APA StyleRiad Deglow, E., Lazo Torres, N. Z., Gutiérrez Muñoz, D., Bufalá Pérez, M., Galparsoro Catalán, A., Zubizarreta-Macho, Á., Abella Sans, F., & Hernández Montero, S. (2022). Influence of Static Navigation Technique on the Accuracy of Autotransplanted Teeth in Surgically Created Sockets. Journal of Clinical Medicine, 11(4), 1012. https://doi.org/10.3390/jcm11041012