
Abuse Potential of Cathinones in Humans: A Systematic Review

 , , , , and
, , , , and
Abstract
:1. Introduction
1.1. Cathinones from Plant to Synthetics
1.2. Chemistry
1.3. Mechanism of Action
1.4. Pharmacological Effects
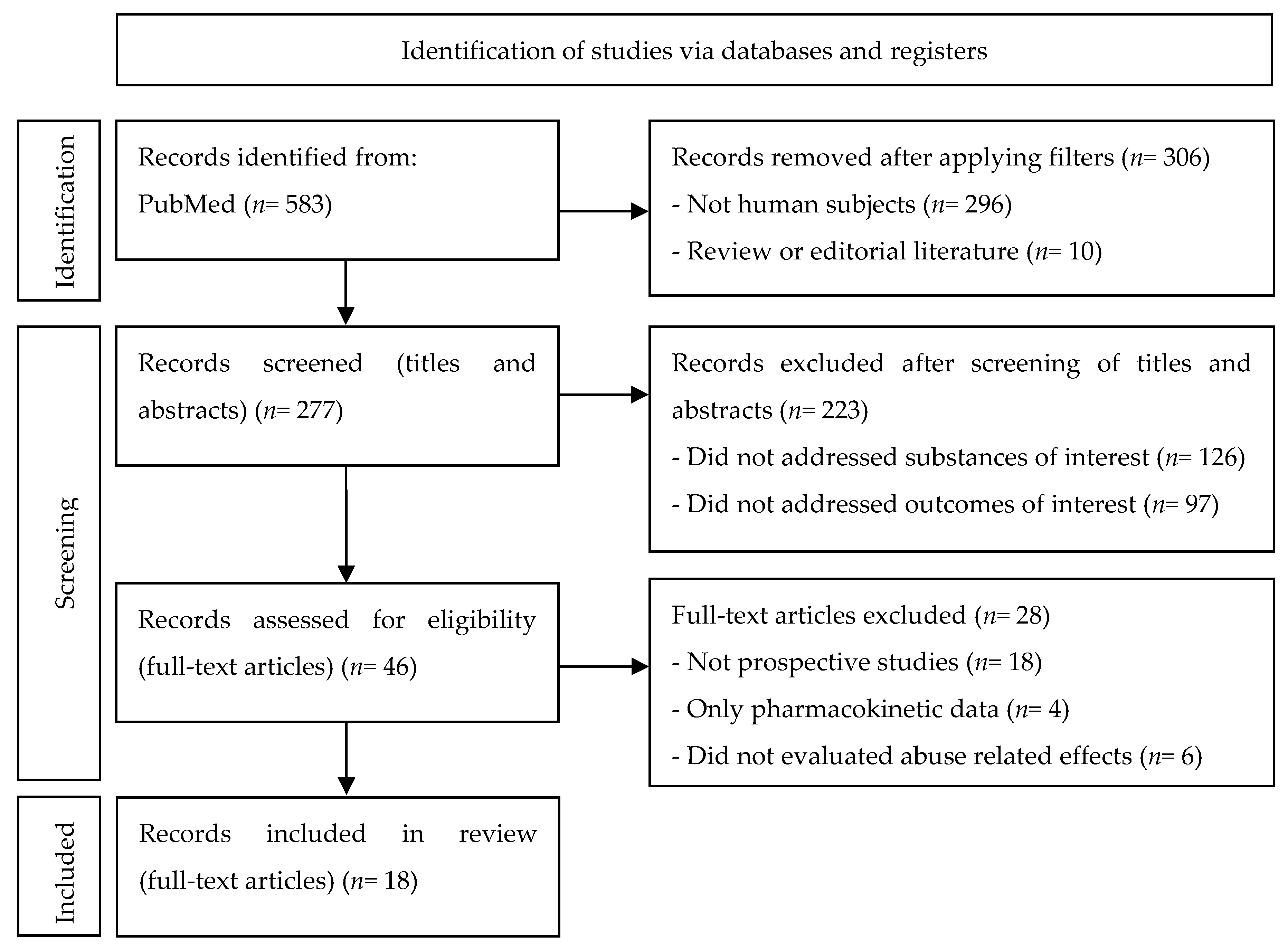
2. Materials and Methods
3. Results
3.1. Cathinone
3.2. Mephedrone
3.3. Methylone
3.4. Diethylpropion
4. Discussion
4.1. Cathinone
4.2. Mephedrone
4.3. Methylone
4.4. Diethylpropion
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Food and Drug Administration (FDA). Assessment of Abuse Potential of Drugs—Guidance for Industry; Food and Drug Administration (FDA): Silver Spring, MD, USA, 2017; pp. 1–37.
- Directive of the European Parliament and of the Council. 2010/84/EU Directive 2010/84/EU of the European Parliament and the Council of 15 December 2010 Amending as Regards Pharmacovigilance, Directive 2001/83/EC on the Community Code Relating to Medicinal Products for Human Use; European Union: Maastricht, The Netherlands, 2010. [Google Scholar]
- Papaseit, E.; Moltó, J.; Muga, R.; Torrens, M.; de la Torre, R.; Farré, M. Clinical Pharmacology of the Synthetic Cathinone Mephedrone. Curr. Top. Behav. Neurosci. 2017, 32, 313–331. [Google Scholar] [CrossRef]
- Widler, P.; Mathys, K.; Brenneisen, R.; Kalix, P.; Fisch, H. Pharmacodynamics and pharmacokinetics of khat: A controlled study. Clin. Pharmacol. Ther. 1994, 55, 556–562. [Google Scholar] [CrossRef]
- Engidawork, E. Pharmacological and Toxicological Effects of Catha edulis F. (Khat). Phyther. Res. 2017, 31, 1019–1028. [Google Scholar] [CrossRef]
- Abebe, W. Khat: A Substance of Growing Abuse with Adverse Drug Interaction Risks. J. Natl. Med. Assoc. 2018, 110, 624–634. [Google Scholar] [CrossRef]
- Bedada, W.; de Andrés, F.; Engidawork, E.; Hussein, J.; LLerena, A.; Aklillu, E. Effects of Khat (Catha edulis) use on catalytic activities of major drug-metabolizing cytochrome P450 enzymes and implication of pharmacogenetic variations. Sci. Rep. 2018, 8, 12726. [Google Scholar] [CrossRef]
- Nencini, P.; Ahmed, A.M.; Elmi, A.S. Subjective effects of khat chewing in humans. Drug Alcohol. Depend. 1986, 18, 97–105. [Google Scholar] [CrossRef]
- Sallam, M.A.; Sheikh, K.A.; Baxendale, R.; Azam, M.N.; El-Setouhy, M. The physiological and perceptual effects of plant extracts (Catha Edulis Forsk) during sustained exercise. Subst. Abus. Treat. Prev. Policy 2016, 11, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Khat Drug Profile. Available online: https://www.emcdda.europa.eu/publications/drug-profiles/khat_en (accessed on 23 January 2022).
- Gebrie, A.; Alebel, A.; Zegeye, A.; Tesfaye, B. Prevalence and predictors of khat chewing among Ethiopian university students: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0195718. [Google Scholar] [CrossRef]
- Ayano, G.; Yohannis, K.; Abraha, M. Epidemiology of khat (Catha edulis) consumption among university students: A meta-analysis. BMC Public Health 2019, 19, 150. [Google Scholar] [CrossRef] [Green Version]
- Anderson, D.M.; Carrier, N.C.M. Khat: Social Harms and Legislation—A Literature Review; Home Office: London, UK, 2011; pp. 1–46.
- World Health Organization (WHO). Assessment of Khat (Catha edulis Forsk); WHO: Geneva, Switzerland, 2006. [Google Scholar]
- United Nations Office on Drug and Crime (UNODC). Global Overview: Drug Demand Drug Supply; United Nations Office on Drug and Crime (UNODC): Vienna, Austria, 2021; ISBN 9789211483611. [Google Scholar]
- Johnson, L.A.; Johnson, R.L.; Portier, R.-B. Current “Legal highs”. J. Emerg. Med. 2013, 44, 1108–1115. [Google Scholar] [CrossRef]
- Valente, M.J.; Guedes De Pinho, P.; De Lourdes Bastos, M.; Carvalho, F.; Carvalho, M.; João, M.; Paula, V.; Pinho, G. De Khat and synthetic cathinones: A review. Arch. Toxicol. 2014, 88, 15–45. [Google Scholar] [CrossRef]
- European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). European Drug Report: Trends and Developments; EMCDDA: Lisbon, Portugal, 2021. [Google Scholar]
- Australian Criminal Intelligence Commission. National Wastewater Drug Monitoring Program Report 10; ACIC: Sydney, Australia, 2020; pp. 1–86.
- Toennes, S.W.; Harder, S.; Schramm, M.; Niess, C.; Kauert, G.F. Pharmacokinetics of cathinone, cathine and norephedrine after the chewing of khat leaves. Br. J. Clin. Pharmacol. 2003, 56, 125–130. [Google Scholar] [CrossRef] [Green Version]
- Baumann, M.H.; Walters, H.M.; Niello, M.; Sitte, H.H. Neuropharmacology of Synthetic Cathinones. Handb. Exp. Pharmacol. 2018, 252, 113–142. [Google Scholar] [CrossRef]
- Simmler, L.D.; Buser, T.A.; Donzelli, M.; Schramm, Y.; Dieu, L.H.; Huwyler, J.; Chaboz, S.; Hoener, M.C.; Liechti, M.E. Pharmacological characterization of designer cathinones in vitro. Br. J. Pharmacol. 2013, 168, 458–470. [Google Scholar] [CrossRef] [Green Version]
- Baumann, M.H.; Jr, M.A.A.; Partilla, J.S.; Sink, J.R.; Shulgin, A.T.; Daley, P.F.; Brandt, S.D.; Rothman, R.B.; Ruoho, A.E.; Cozzi, N.V.; et al. The designer methcathinone analogs, mephedrone and methylone, are substrates for monoamine transporters in brain tissue. Neuropsychopharmacology 2012, 37, 1192–1203. [Google Scholar] [CrossRef]
- López-Arnau, R.; Martínez-Clemente, J.; Pubill, D.; Escubedo, E.; Camarasa, J. Comparative neuropharmacology of three psychostimulant cathinone derivatives: Butylone, mephedrone and methylone. Br. J. Pharmacol. 2012, 167, 407–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luethi, D.; Kolaczynska, K.E.; Docci, L.; Krähenbühl, S.; Hoener, M.C.; Liechti, M.E. Pharmacological profile of mephedrone analogs and related new psychoactive substances. Neuropharmacology 2018, 134, 4–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalix, P. The amphetamine-like releasing effect of the alkaloid (-)cathinone on rat nucleus accumbens and rabbit caudate nucleus. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 1982, 6, 43–49. [Google Scholar] [CrossRef]
- Pehek, E.A.; Schechter, D.; Yamamoto, B.K. Effects of cathinone and amphetamine on the neurochemistry of dopamine in vivo. Neuropharmacology 1990, 29, 1171–1176. [Google Scholar] [CrossRef]
- Kehr, J.; Ichinose, F.; Yoshitake, S.; Goiny, M.; Sievertsson, T.; Nyberg, F. Mephedrone, compared with MDMA (ecstasy) and amphetamine, rapidly increases both dopamine and 5-HT levels in nucleus accumbens of awake rats. Br. J. Pharmacol. 2011, 164, 1949–1958. [Google Scholar] [CrossRef] [Green Version]
- Simmons, S.J.; Leyrer-Jackson, J.M.; Oliver, C.F.; Hicks, C.; Muschamp, J.W.; Rawls, S.M.; Olive, M.F. DARK Classics in Chemical Neuroscience: Cathinone-Derived Psychostimulants. ACS Chem. Neurosci. 2018, 9, 2379–2394. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.B. Mechanism of action of cathinone: The active ingredient of khat (Catha edulis). East Afr. Med. J. 2000, 77, 329–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brenneisen, R.; Fisch, H.; Koelbing, U.; Geisshusler, S.; Kalix, P. Amphetamine-like effects in humans of the khat alkaloid cathinone. Br. J. Clin. Pharmacol. 1990, 30, 825–828. [Google Scholar] [CrossRef] [Green Version]
- Zwartsen, A.; Olijhoek, M.E.; Westerink, R.H.S.; Hondebrink, L. Hazard Characterization of Synthetic Cathinones Using Viability, Monoamine Reuptake, and Neuronal Activity Assays. Front. Neurosci. 2020, 14, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Volkow, N.D.; Baler, R. Emergency department visits from edible versus inhalable cannabis. Ann. Intern. Med. 2019, 170, 569–570. [Google Scholar] [CrossRef] [PubMed]
- Luethi, D.; Liechti, M.E. Designer Drugs: Mechanism of Action and Adverse Effects; Springer: Berlin/Heidelberg, Germany, 2020; Volume 94, ISBN 0020402002693. [Google Scholar]
- Santamaría, A.; Arias, H.R. Neurochemical and behavioral effects elicited by bupropion and diethylpropion in rats. Behav. Brain Res. 2010, 211, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Opacka-juffry, J.; Pinnel, T.; Patel, N.; Bevin, M.; Meintel, M.; Davidson, C. Stimulant mechanisms of cathinones—Effects of mephedrone and other cathinones on basal and electrically evoked dopamine efflux in rat accumbens brain slices. Prog. Neuropsychopharmacol. Biol. Psychiatry 2014, 54, 122–130. [Google Scholar] [CrossRef]
- Peterson, D.W.; Maitai, C.K.; Sparber, S.B. Relative potencies of two phenylalkylamines found in the abused plant Catha edulis, Khat. Life Sci. 1980, 27, 2143–2147. [Google Scholar] [CrossRef]
- Cox, G.; Rampes, H. Adverse effects of khat: A review. Adv. Psychiatr. Treat. 2003, 9, 456–463. [Google Scholar] [CrossRef]
- World Health Organization. Mephedrone: Critical Review Report; WHO: Geneva, Switzerland, 2014; pp. 1–34. [Google Scholar]
- Winstock, A.; Mitcheson, L.; Ramsey, J.; Davies, S.; Puchnarewicz, M.; Marsden, J. Mephedrone: Use, subjective effects and health risks. Addiction 2011, 106, 1991–1996. [Google Scholar] [CrossRef]
- Kapitány-Föveny, M.; Kertesz, M.; Winstock, A.; Deluca, P.; Corazza, O.; Farkas, J.; Zacher, G.; Urbán, R.; Demetrovics, Z. Substitutional potential of mephedrone: An analysis of the subjective effects. Hum. Psychopharmacol. 2013, 28, 308–316. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.; Reed, P.; Parrott, A. Mephedrone and 3,4-methylenedioxy-methamphetamine: Comparative psychobiological effects as reported by recreational polydrug users. J. Psychopharmacol. 2016, 30, 1313–1320. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Methylone (bk-MDMA). Critical Review Report; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Kang, J.G.; Park, C.Y. Anti-obesity drugs: A review about their effects and safety. Diabetes Metab. J. 2012, 36, 13–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, S. Diethylpropion (Tenuate): An Infrequently Abused Anorectic. Psychosomatics 1977, 18, 28–33. [Google Scholar] [CrossRef]
- Halket, J.M.; Karasu, Z.; Murray-Lyon, I.M. Plasma cathinone levels following chewing khat leaves (Catha edulis Forsk.). J. Ethnopharmacol. 1995, 49, 111–113. [Google Scholar] [CrossRef]
- Gómez-Silva, M.; Piñeyro-Garza, E.; Vargas-Zapata, R.; Gamino-Peña, M.E.; León-García, A.; de León, M.B.; Llerena, A.; León-Cachón, R.B.R. Pharmacogenetics of amfepramone in healthy Mexican subjects reveals potential markers for tailoring pharmacotherapy of obesity: Results of a randomised trial. Sci. Rep. 2019, 9, 17833. [Google Scholar] [CrossRef]
- Czerwinska, J.; Parkin, M.C.; Cilibrizzi, A.; George, C.; Kicman, A.T.; Dargan, P.I.; Abbate, V. Pharmacokinetics of mephedrone enantiomers in whole blood after a controlled intranasal administration to healthy human volunteers. Pharmaceuticals 2021, 14, 5. [Google Scholar] [CrossRef]
- Czerwinska, J.; Parkin, M.C.; George, C.; Kicman, A.T.; Dargan, P.I.; Abbate, V. Pharmacokinetics of Mephedrone and Its Metabolites in Whole Blood and Plasma after Controlled Intranasal Administration to Healthy Human Volunteers. J. Anal. Toxicol. 2021, 45, 730–738. [Google Scholar] [CrossRef]
- Sallam, M.A.; Sheikh, K.A.; Baxendale, R.; Azam, M.N.; Hossain, A.M.; El-Setouhy, M. The Physiological and Ergogenic Effects of Khat (Catha edulis Forsk) Extract. Subst. Use Misuse 2018, 53, 94–100. [Google Scholar] [CrossRef]
- Seaton, D.A.; Duncan, L.J.P.; Rose, K.; Scott, A.M. Diethylpropion In The Treatment of “Refractory” Obesity. Br. Med. J. 1961, 1, 1009–1011. [Google Scholar] [CrossRef]
- Silverstone, J.T.; Turner, P.; Humpherson, P.L. Direct Measurement of the Anorectic Activity Of Diethylpropion (Tenuate Dospan). J. Clin. Pharmacol. J. New Drugs 1968, 8, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Cercato, C.; Roizenblatt, V.; Leança, C.; Segal, A.; Lopes Filho, A.; Mancini, M.; Halpern, A. A randomized double-blind placebo-controlled study of the long-term efficacy and safety of diethylpropion in the treatment of obese subjects. Int. J. Obes. 2009, 33, 857–865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suplicy, H.; Boguszewski, C.L.; Dos Santos, C.M.C.; Do Desterro De Figueiredo, M.; Cunha, D.R.; Radominski, R. A comparative study of five centrally acting drugs on the pharmacological treatment of obesity. Int. J. Obes. 2014, 38, 1097–1103. [Google Scholar] [CrossRef] [PubMed]
- Toennes, S.W.; Kauert, G.F. Excretion and detection of cathinone, cathine, and phenylpropanolamine in urine after kath chewing. Clin. Chem. 2002, 48, 1715–1719. [Google Scholar] [CrossRef] [Green Version]
- Freeman, T.P.; Morgan, C.J.A.A.; Vaughn-jones, J.; Hussain, N.; Karimi, K.; Curran, H.V. Cognitive and subjective effects of mephedrone and factors influencing use of a “new legal high”. Addiction 2012, 107, 792–800. [Google Scholar] [CrossRef]
- Papaseit, E.; Pérez-Mañá, C.; Mateus, J.A.; Pujadas, M.; Fonseca, F.; Torrens, M.; Olesti, E.; De La Torre, R.; Farre, M. Human pharmacology of mephedrone in comparison with MDMA. Neuropsychopharmacology 2016, 41, 2704–2713. [Google Scholar] [CrossRef] [Green Version]
- De Sousa Fernandes Perna, E.B.; Papaseit, E.; Pérez-Mañá, C.; Mateus, J.; Theunissen, E.L.; Kuypers, K.P.C.; De La Torre, R.; Farré, M.; Ramaekers, J.G. Neurocognitive performance following acute mephedrone administration, with and without alcohol. J. Psychopharmacol. 2016, 30, 1305–1312. [Google Scholar] [CrossRef]
- Papaseit, E.; Pérez-Mañá, C.; de Sousa Fernandes Perna, E.B.; Olesti, E.; Mateus, J.; Kuypers, K.P.C.; Theunissen, E.L.; Fonseca, F.; Torrens, M.; Ramaekers, J.G.; et al. Mephedrone and alcohol interactions in humans. Front. Pharmacol. 2020, 10, 1588. [Google Scholar] [CrossRef]
- Olesti, E.; Farré, M.; Papaseit, E.; Krotonoulas, A.; Pujadas, M.; de la Torre, R.; Pozo, Ó.J. Pharmacokinetics of Mephedrone and Its Metabolites in Human by LC-MS/MS. AAPS J. 2017, 19, 1767–1778. [Google Scholar] [CrossRef]
- Olesti, E.; Farré, M.; Carbó, M.; Papaseit, E.; Perez-Mañá, C.; Torrens, M.; Yubero-Lahoz, S.; Pujadas, M.; Pozo, Ó.J.; de la Torre, R. Dose-Response Pharmacological Study of Mephedrone and Its Metabolites: Pharmacokinetics, Serotoninergic Effects, and Impact of CYP2D6 Genetic Variation. Clin. Pharmacol. Ther. 2019, 106, 596–604. [Google Scholar] [CrossRef]
- Papaseit, E.; Olesti, E.; Pérez-Mañá, C.; Torrens, M.; Fonseca, F.; Grifell, M.; Ventura, M.; de la Torre, R.; Farré, M. Acute pharmacological effects of oral and intranasal mephedrone: An observational study in humans. Pharmaceuticals 2021, 14, 100. [Google Scholar] [CrossRef] [PubMed]
- Poyatos, L.; Papaseit, E.; Olesti, E.; Pérez-Mañá, C.; Ventura, M.; Carbón, X.; Grifell, M.; Fonseca, F.; Torrens, M.; de la Torre, R.; et al. A comparison of acute pharmacological effects of methylone and mdma administration in humans and oral fluid concentrations as biomarkers of exposure. Biology 2021, 10, 788. [Google Scholar] [CrossRef] [PubMed]
- Jonsson, C.O. Behavioural studies of diethylpropion in man. In Abuse of Central Stimulants; Sjoquist, F., Tottie, M., Eds.; Raven Press: New York, NY, USA, 1969; pp. 71–80. [Google Scholar]
- Jasinski, D.R.; Nutt, J.G.; Griffith, J.D. Effects of diethylpropion and d-amphetamine after subcutaneous and oral administration. Clin. Pharmacol. Ther. 1974, 16, 645–652. [Google Scholar] [CrossRef] [PubMed]
- Johanson, C.E.; Uhlenhuth, E.H. Self-administration of abused substances: Methods for study. NIDA Res. Monogr. 1978, 20, 68–85. [Google Scholar]
- Bigelow, G.E.; Brady, J.V.; Griffiths, R.R.; Stitzer, M.L.; Ator, N.A.; Higgins, S.T.; Liebson, I.A.; Lucas, S.E. Progress report from the Division of Behavioral Biology, the Johns Hopkins University School of Medicine. NIDA Res. Monogr. 1984, 55, 66–75. [Google Scholar] [PubMed]
- Jasinski, D.R.; Krishnan, S.S. Abuse liability and safety of oral lisdexamfetamine dimesylate in individuals with a history of stimulant abuse. J. Psychopharmacol. 2009, 23, 419–427. [Google Scholar] [CrossRef]
- La Maida, N.; Di Trana, A.; Giorgetti, R.; Tagliabracci, A.; Busardò, F.P.; Huestis, M.A. A Review of Synthetic Cathinone-Related Fatalities From 2017 to 2020. Therapy 2021, 43, 52–68. [Google Scholar] [CrossRef]
- Riley, A.L.; Nelson, K.H.; To, P.; López-arnau, R.; Xu, P.; Wang, D.; Wang, Y.; Shen, H.; Kuhn, D.M.; Angoa-perez, M.; et al. Abuse potential and toxicity of the synthetic cathinones (i.e., “Bath salts”). Neurosci. Biobehav. Rev. 2020, 110, 150–173. [Google Scholar] [CrossRef]
- Pendl, E.; Pauritsch, U.; Kollroser, M.; Schmid, M.G. Determination of cathinone and cathine in Khat plant material by LC–MS/MS: Fresh vs. dried leaves. Forensic. Sci. Int. 2021, 319, 110658. [Google Scholar] [CrossRef]
- Graziani, M.; Milella, M.S.; Nencini, P. Khat chewing from the pharmacological point of view: An update. Subst. Use Misuse 2008, 43, 762–783. [Google Scholar] [CrossRef]
- Lucchetta, R.C.; Riveros, B.S.; Pontarolo, R.; Radominski, R.B.; Otuki, M.F.; Fernandez-Llimos, F.; Correr, C.J. Systematic review and meta-analysis of the efficacy and safety of amfepramone and mazindol as a monotherapy for the treatment of obese or overweight patients. Clinics 2017, 72, 317–324. [Google Scholar] [CrossRef]
- Garcia Ramirez, A.V.; Filho, D.R.; Zotarelli Filho, I.J. Meta-analysis and Approach of the Real Impact of Anorexigenic Drugs in the Obesity in Humans: The Last Five Years of the Randomized Studies. Curr. Diabetes Rev. 2019, 16, 750–758. [Google Scholar] [CrossRef] [PubMed]
- Holze, F.; Vizeli, P.; Müller, F.; Ley, L.; Duerig, R.; Varghese, N.; Eckert, A.; Borgwardt, S.; Liechti, M.E. Distinct acute effects of LSD, MDMA, and d-amphetamine in healthy subjects. Neuropsychopharmacology 2020, 45, 462–471. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Reference | Type of Study | Sample Size | Dose | Pharmacokinetics [Mean ± SD, (Range)] | Assessments | Abuse-Related Effects |
|---|---|---|---|---|---|---|
| Nencini et al., 1986 [8] | Experimental, non-controlled, open-label. | 14 male volunteers, habitual khat users. | Two khat bundles of 200 g, considered the usual dose for an experienced khat user. | Not reported. | Subjective effects: ARCI, VAS (appetite, vigilance and euphoria/dysphoria). Physiological effects: Supine SBP, DBP and HR. | Subjective effects: 10 subjects experienced euphoria and increased intellectual efficiency and alertness (ARCI MBG, A, and BG). These effects were progressively replaced by mild dysphoria and sedation (ARCI LSD and PCAG). The other four subjects reported minimal amphetamine-like effects although they also experienced dysphoric effects. CATH showed mild anorectic effects. Physiological effects: CATH increased SBP, DBP, and HR in all the subjects. |
| Brenneisen et al., 1990 [31] | Experimental, placebo- controlled, double-blind, randomized and crossover study. | Six healthy male volunteers. | Orally administered gelatin capsules of 0.5 mg CATH/kg body weight. Placebo | Data deduced from a figure. CATH: Cmax: approx. 105 ng/mL AUC0–9: 307 ± 71 ng/mL·h * Tmax: 1.2 ± 0.55 h * T1/2: 4.81 ± 1.05 h * Norephedrine: Cmax: approx. 75 ng/mL AUC0–9: 489 ± 228 ng/mL·h * Tmax: 2 h | Subjective effects: ARCI. Physiological effects: SBP, DBP, and HR were monitored. | Subjective effects: CATH induced psychostimulant and euphorigenic effects, reflected by an increase in scores for ARCI stimulation/ euphoria and amphetamine-like effects. Physiological effects: CATH produced an increase in blood pressure and HR. |
| Widler et al., 1994 [4] | Experimental, placebo-controlled, double blind. | Six healthy males without previous khat chewing experience. | 0.8 mg cathinone/kg body weight (54 to 71 g fresh khat leaves) of a standardized preparation of khat leaves chewed for 1 h. CATH: 1.02 ± 0.11 mg Cathine: 0.86 ± 0.06 mg Norephedrine: 0.47 ± 0.05 mg Placebo: alkaloid-free khat. | CATH: Cmax: 127 ± 53 ng/mL AUC0–9: 415 ± 207 ng/mL·h Tmax: 2.12 ± 0.5 h Cathine: Cmax: 89 ± 51 ng/mL AUC0–9: 466 ± 299 ng/mL·h Tmax: 3.05 ± 1.22 h Norephedrine: Cmax: 110 ± 51 ng/mL Tmax: 3.33 ± 2.23 h AUC0–9: 633 ± 337 ng/mL·h | Subjective effects: ARCI, VAS. Physiological effects: SBP, DBP, and HR were continuously monitored. | Subjective effects: CATH increased scores in the amphetamine–effect, stimulation–euphoria, and stimulation–motor ARCI scales. Subjects reported feeling more excited and energetic in VAS. Physiological effects: CATH produced a significant mild and slow increase in SBP and DBP that persisted for 4 h. The increase in HR was not significant. |
| Toennes et al., 2002; 2003 [20,55] | Experimental, non-controlled, open label. | Four (two M, two F) healthy, without previous khat chewing experience | 0.6 g of khat leaves per kg body weight chewed for 1 h: CATH: 1.14 mg/g khat (0.684 mg cathinone/kg body weight) Cathine: 0.83 mg/g khat Norephedrine: 0.44 mg/g khat | Blood concentrations: CATH: Cmax: 58.9 ± 18.8 ng/mL AUC: 245 ± 49 ng·min/L Tmax: 2.31 ± 0.65 h t ½ α: 0.39 ± 0.07 h t ½ β: 1.50 ± 0.81 h Cathine: Cmax: 71.2 ± 13.9 ng/mL AUC: 713 ± 131 ng·min/mL Tmax: 2.62 ± 0.77 h t ½ α: 0.24 ± 0.17 t ½ β: 5.22 ± 3.36 Norephedrine: Cmax: 72.1 ± 12.2 ng/mL AUC: 710 ± 173 ng·min/mL Tmax: 2.84 ± 0.42 h Urine concentrations: CATH: Cmax: 2.5 mg/L Cathine: Cmax: 20 mg/L Norephedrine: Cmax: 30 mg/L | Subjective effects: The mental state of the subjects was assessed using a list of paired terms describing opposite states of emotion (“Befindlichkeitsskala”). Physiological effects: SBP, DBP, HR, PD, and rotator nystagmus. Reaction to visual and acoustic stimuli was tested using the Wiener Determinations test, and the individual attention and concentration performance was tested using Test d2. | Subjective effects: All participants reported the personal feeling of being alert and “energetic”. Physiological effects: Participants experienced an increase in blood pressure that might not be caused by the pharmacological action of the alkaloids. HR, PD, and reaction to light showed no changes. Rotatory nystagmus and an impairment of mental condition were not observed. |
| Reference | Type of Study | Sample Size | Dose | Pharmacokinetics [Mean ± SD, (Range)] | Assessments | Abuse-Related Effects |
|---|---|---|---|---|---|---|
| Freeman et al., 2012 [56] | Observational-naturalistic controlled, open label | 20 MEPHE users (14 M, 6 F) and 20 controls drug free (11 M, 9 F) | Not reported. MEPHE users self-administered the drug as they normally would (dose and route of administration). | Not reported. | Subjective effects: VAS, BDI, O-LIFE, and MFUQ. Physiological effects: - Cognitive assessments: Prose recall (rivermead behavioral memory test), spatial N-back, phonological fluency, semantic fluency, trail making test, Wechsler adult reading test. | Subjective effects: MEPHE produced an increase in stimulant effects, particularly “self-confidence”, “buzzing”, and “dizziness”. Physiological effects: - Cognitive assessments: MEPHE impaired concentration and memory and also enhanced psychomotor speed. |
| Papaseit et al., 2016 [57] | Experimental placebo- controlled double-blind, double dummy, randomized, and crossover trial | 12 healthy males who were recreational users of amphetamines MDMA, MEPHE, and cathinones. | 200 mg of oral MEPHE 100 mg of oral MDMA Placebo | Cmax: 134.6 ± 63.5 ng/mL AUC0–12: 519.5 ± 287.0 ng/mL·h AUC0–24: 556.2 ± 320.2 ng/mL·h AUC0–inf: 556.2 ± 320.2 ng/mL·h Tmax: 1.25 (0.5–4) h Ke: 0.33 ± 0.07 per h t1/2: 2.15 ± 0.4 h | Subjective effects: VAS, VESSPA, ARCI, and pharmacological class identification questionnaire. Physiological effects: Non-invasive SBP, DBP, HR, and PD. Electrocardiogram was continuously monitored. | Subjective effects: MEPHE induced stimulant-like effects, euphoria, and well-being and induced mild changes in perceptions comparable to those of MDMA. Physiological effects: MEPHE increased SBP, DBP, HR, and PD. |
| De Sousa et al., 2016 [58]; Papaseit et al., 2020 [59] | Experimental placebo-controlled, double-blind, randomized, crossover phase I clinical trial. | 11 healthy males, recreational users of amphetamines, MDMA, MEPHE, or cathinones. | 200 mg of oral MEPHE + 0.8 g/kg alcohol 200 mg of oral MEPHE + placebo alcohol Placebo MEPHE + 0.8 g/kg alcohol Placebo MEPHE + placebo alcohol | MEPHE alone Cmax: 172.6 ± 82.9 ng/mL AUC0–6: 549.0 ± 315.0 ng/mL·h AUC0–24: 778.4 ± 512.9 ng/mL·h Tmax: 1.5 (0.5–2) h Ke: 0.29 ± 0.09 per h t1/2: 2.68 ± 0.92 h MEPHE with alcohol Cmax: 175.7 ± 71.1 ng/mL AUC0–6: 516.8 ± 264.6 ng/mL·h AUC0–24: 709.8 ± 477.1 ng/mL·h Tmax: 1.5 (0.75–2) h Ke: 0.35 ± 0.14 per h t1/2: 2.32 ± 1.01 h | Subjective effects: VAS, VESSPA, ARCI, and pharmacological class identification questionnaire. Physiological effects: SBP, DBP, and HR were continuously monitored. Oral temperature was measured, and DP and the Maddox wing were recorded. Neurocognitive assessment: SMT, CTT, DAT. | Subjective effects: MEPHE induced stimulant-like effects (euphoria, well-being, feelings of pleasure) and mild changes in perceptions that were more intense and prolonged in combination with alcohol. Physiological effects: MEPHE produced a significant increase in BP, HR, and PD. Cardiovascular effects were increased in combination with alcohol. Neurocognitive assessment: MEPHE improves psychomotor performance, impairs spatial memory, and does not affect divided attention performance. |
| Olesti et al., 2017; 2019 [60,61] | Experimental double-blind, placebo controlled, randomized, crossover, phase I clinical trial. | Nine healthy males, recreational users of NPS. | 50 and 100 mg of oral MEPHE (n = 3) 150 and 200 mg of oral MEPHE (n = 6) | MEPHE 50 mg Cmax: 37.4 ± 16.4 ng/mL AUC0–8: 122.5 ± 59.7 ng/mL·h Tmax: 2 (1–2) h MEPHE 100 mg Cmax: 51.7 ± 20.5 ng/mL AUC0–8: 169.4 ± 93.5 ng/mL·h Tmax: 1 (1–2) h MEPHE 150 mg Cmax: 179.0 ± 29.3 ng/mL AUC0–8: 588.2 ± 93.4 ng/mL·h Tmax: 1 (1–2) h MEPHE 200 mg Cmax: 255.6 ± 70.0 ng/mL AUC0–8: 879.4 ± 194.1 ng/mL·h Tmax: 1 (1–2) h | Subjective effects: VAS. Physiological effects: SBP, DBP, and HR were continuously monitored. | Subjective effects: MEPHE induced subjective effects (VAS high, good effects, stimulated) that showed a positive correlation with drug concentrations in the plasma at each tested MEPHE dose. Physiological effects: MEPHE produced cardiovascular effects that correlated positively with drug concentrations in the plasma at each tested MEPHE dose. |
| Papaseit et al., 2021 [62] | Observational-naturalistic, non-controlled, open label. | 10 (4 F, 6 M) healthy subjects, recreational users. | Self-administration of oral MEPHE (n = 5, 100–200 mg; mean 150 mg) Self-administration of intranasal MEPHE (n = 5, 50–100 mg, mean 70 mg) | Oral fluid concentrations Oral MEPHE: Cmax: 1571 ± 1367 ng/mL AUC0–4: 3684 ± 3443 ng/mL·h Tmax: 2 (1–2) h Intranasal MEPHE: Cmax: 4950 ± 5545 ng/mL AUC0–4: 7919 ± 7717 ng/mL·h Tmax: 1 (1–1) h | Subjective effects: VAS, VESSPA, ARCI. Physiological effects: Non-invasive SBP, DBP, HR, and cutaneous temperature. | Subjective effects: MEPHE oral self-administration in comparison to intranasal produced greater and larger effects on some subjective measures. Physiological effects: Both MEPHE self-administrations produced an increase in SBP, DBP, HR. |
| Reference | Type of Study | Sample Size | Dose | Pharmacokinetics [Mean ± SD (Range)] | Assessments | Abuse-Related Effects |
|---|---|---|---|---|---|---|
| Poyatos et al., 2021 [63] | Observational- naturalistic non-controlled, open label. | 14 (4 F, 10 M) healthy subjects, recreational users. | Self-administration of oral METHY (n = 8, 100–300 mg; mean 187.5 mg) Self-administration of oral MDMA (n = 6, 75–100 mg, mean 87.5 mg) | Oral fluid concentrations: Cmax: 15,514.00 ± 9748.86 ng/mL AUC0–4: 40,623.79 ± 20,001.70 ng/mL·h Tmax: 2 (2–2) h | Subjective effects: VAS, VESSPA, ARCI. Physiological effects: Non-invasive SBP, DBP, HR, and cutaneous temperature. | Subjective effects: METHY induced similar psychostimulant and empathogenic effects to MDMA, but they were less intense. Physiological effects: METHY produced an increase in SBP and HR. |
| Reference | Type of Study | Sample Size | Dose | Pharmacokinetics [Mean ± SD, (Range)] | Assessments | Abuse-Related Effects |
|---|---|---|---|---|---|---|
| Jonsson et al., 1969 [64] | Double-blind study in natural environment. | 116 subjects of both genders. | 25, 50 mg of oral DEP 20 mg of oral pipradrol 100 mg of oral amobarbital Placebo | Not reported. | Subjective effects: Scales comprising 20 variables (e.g., happiness, alertness, relaxation, flight of thoughts), Physiological effects: - | Subjective effects: Relative to placebo, both doses of DEP gave results in the same direction as pipradrol. Compared to placebo, DEP obtained higher scores for “happy”, “alert”, and “flight of thoughts” and lower scores in “relaxed”. Physiological effects: - |
| Jonsson et al., 1969 [64] | Experimental, triple-blind study in laboratory conditions. | 30 young males. | 50 mg of oral DEP 10 mg of oral dexamphetamine 50 mg oral phenmetrazine 250 mg caffeine Placebo | Not reported. | Subjective effects: Scales comprising ratings of pleasantness. Physiological effects: - | Subjective effects: DEP produced stimulant-like effects reflected in feelings of “happiness” similar to dexamphetamine, “alertness”, and “pleasantness”. The effects of “pleasantness” came in between phenmetrazine and dexamphetamine. Physiological effects: - |
| Jasinski et al., 1974 [65] | Experimental, comparative, placebo controlled, double-blind, randomized, crossover. | nine healthy federal prisoners with documented histories of narcotic abuse. All admitted prior abuse of amphetamine-like agents. | 150, 300, and 600 mg of subcutaneous DEP 100, 200, and 400 mg of oral DEP 7.5, 15, and 30 mg of subcutaneous d-amphetamine 10, 20, and 40 mg of oral d-amphetamine Placebo condition | Not reported. | Subjective effects: Drug identifications and “liking scores” from the subject’s and observer’s single-dose opiate questionnaires and ARCI (BG, MBG, A). Physiological effects: SBP, DBP, HR, rectal temperature, and PD. | Subjective effects: DEP produced effects that were qualitatively similar to those of d-amphetamine including euphoria. Orally DEP was 1/6 to 1/11 as potent as d-amphetamine, while subcutaneously, DEP was 1/10 to 1/20 as potent as d-amphetamine. Physiological effects: DEP increased blood pressure and body temperature and decreased caloric intake and sleep. |
| Johanson et al., 1978 [66] | Drug preference, placebo controlled. | 10 (7 M, 3 F) healthy volunteers. | Subjects participated in three to six different choice experiments self-administering oral capsules of: 25, 50 mg of DEP 5, 10 mg of d-amphetamine Placebo | Not reported. | Subjective effects: POMS, choice procedure. Physiological effects: - | Subjective effects: In comparisons between DEP and d-amphetamine, d-amphetamine was generally preferred. However, as the dose of DEP increased, preference for d-amphetamine decreased. Physiological effects: - |
| Bigelow et al., 1984 [67] | Drug preference, placebo controlled. | Not reported. Overweight patients. | 75 mg of DEP Placebo | Not reported. | Subjective effects: Choice procedure. Physiological effects: - | Subjective effects: DEP, with a similar profile to amphetamine, maintained drug preference well above placebo levels (approx. 75%). Physiological effects: - |
| Jasinski et al., 2009 [68] | Experimental, placebo controlled, double-blind, randomized, six-period crossover study. | 38 (32 M, 6 F) volunteers with a history of stimulant abuse. Only 36 completed the study. | 200 mg of oral DEP 50, 100, and 150 mg of oral LDX 40 mg of oral d-amphetamine Placebo | Not reported. | Subjective effects: DRQS, ARCI, SVAQ. Physiological effects: SBP, DBP, HR. | Subjective effects: In terms of abuse potential, 200 mg of DEP was appraised as having a comparable street value as 100 and 150 mg of LDX. Physiological effects: All treatments produced cardiovascular effects. Increases in SBP and DBP were significantly lower for 50 mg LDX and DEP than for d-amphetamine. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poyatos, L.; Torres, A.; Papaseit, E.; Pérez-Mañá, C.; Hladun, O.; Núñez-Montero, M.; de la Rosa, G.; Torrens, M.; Fuster, D.; Muga, R.; et al. Abuse Potential of Cathinones in Humans: A Systematic Review. J. Clin. Med. 2022, 11, 1004. https://doi.org/10.3390/jcm11041004
Poyatos L, Torres A, Papaseit E, Pérez-Mañá C, Hladun O, Núñez-Montero M, de la Rosa G, Torrens M, Fuster D, Muga R, et al. Abuse Potential of Cathinones in Humans: A Systematic Review. Journal of Clinical Medicine. 2022; 11(4):1004. https://doi.org/10.3390/jcm11041004
Chicago/Turabian StylePoyatos, Lourdes, Adrián Torres, Esther Papaseit, Clara Pérez-Mañá, Olga Hladun, Melani Núñez-Montero, Georgina de la Rosa, Marta Torrens, Daniel Fuster, Robert Muga, and et al. 2022. "Abuse Potential of Cathinones in Humans: A Systematic Review" Journal of Clinical Medicine 11, no. 4: 1004. https://doi.org/10.3390/jcm11041004
APA StylePoyatos, L., Torres, A., Papaseit, E., Pérez-Mañá, C., Hladun, O., Núñez-Montero, M., de la Rosa, G., Torrens, M., Fuster, D., Muga, R., & Farré, M. (2022). Abuse Potential of Cathinones in Humans: A Systematic Review. Journal of Clinical Medicine, 11(4), 1004. https://doi.org/10.3390/jcm11041004