
Melatonin in the Prophylaxis of SARS-CoV-2 Infection in Healthcare Workers (MeCOVID): A Randomised Clinical Trial

 , , , , , , , , , and
, , , , , , , , , and  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design
2.2. Study Population
2.3. Randomisation, Treatment and Blinding
2.4. Study Procedures
2.5. Outcome Variables
2.6. Statistical Analysis
2.7. Role of the Funding Source
3. Results
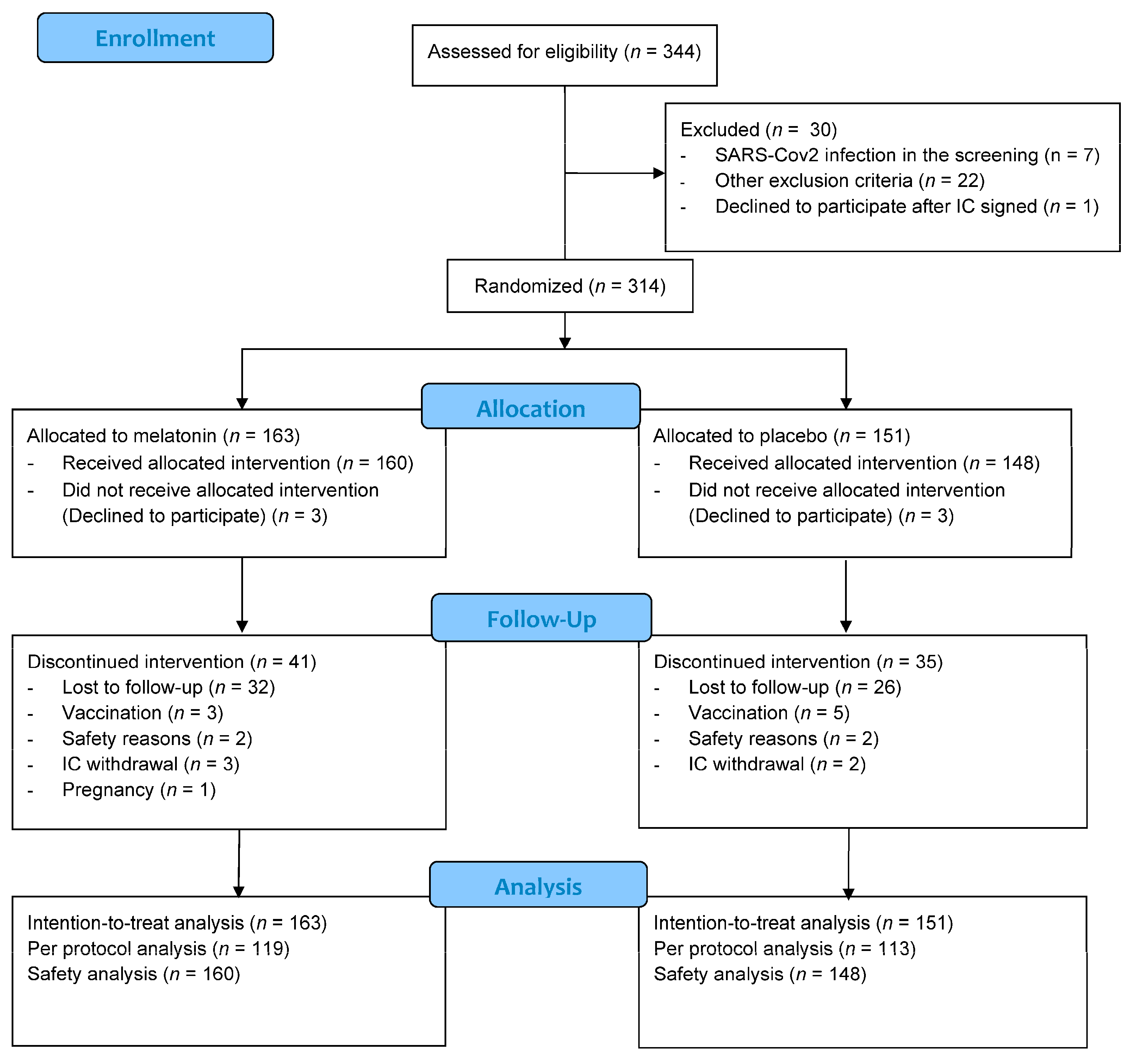
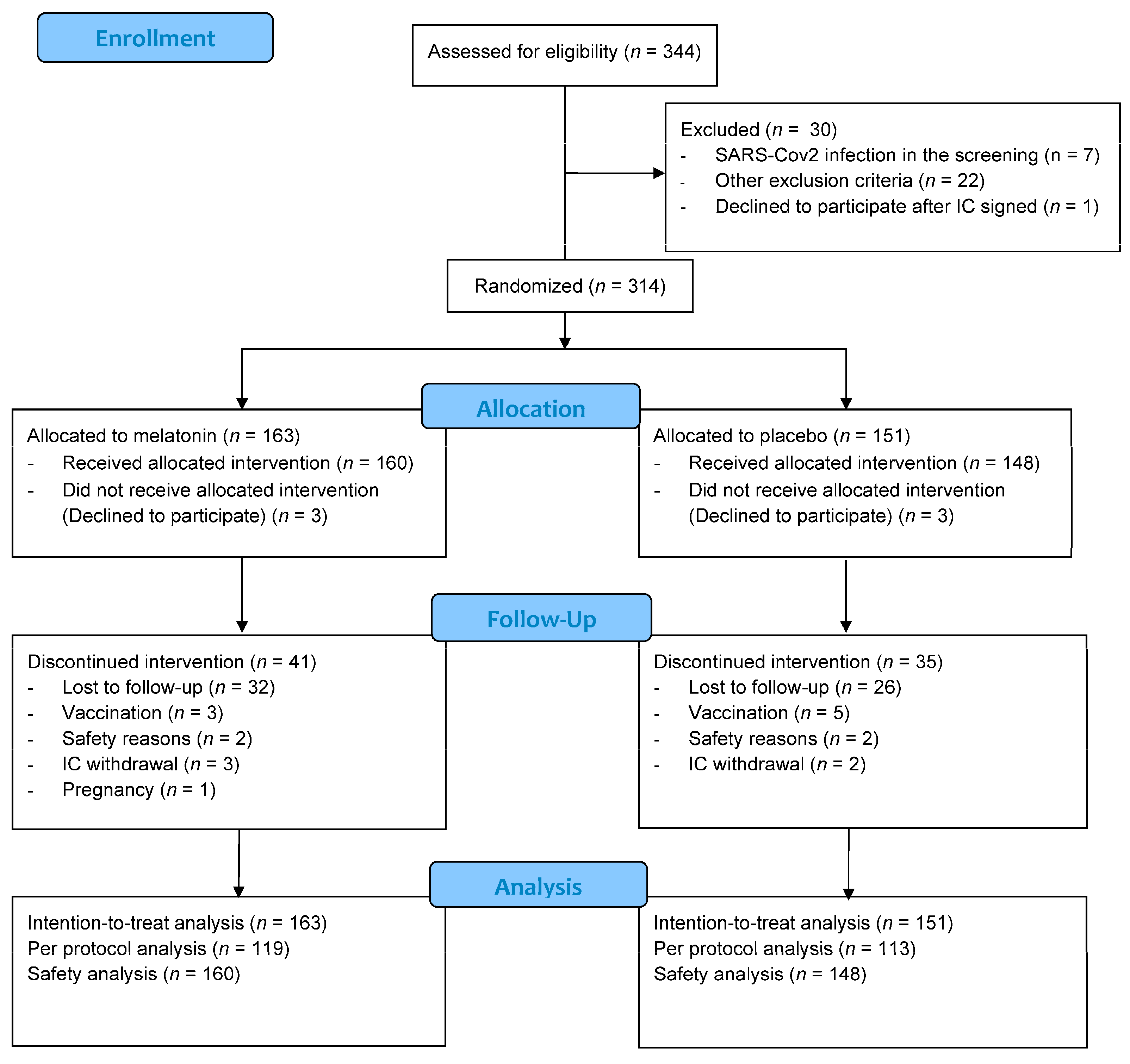
3.1. Population
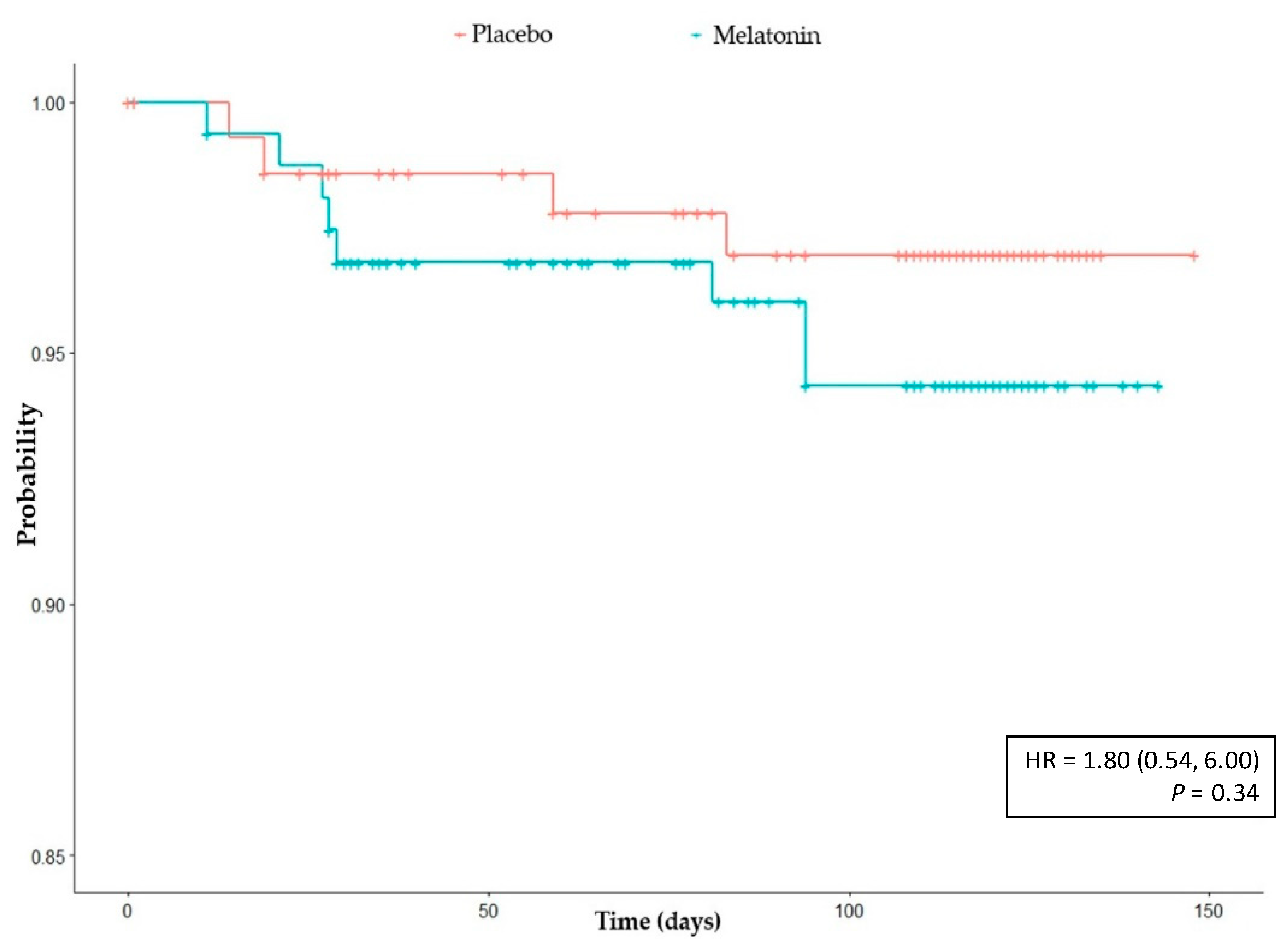
3.2. Primary Outcome
3.3. Secondary Outcomes
3.4. Safety Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease 2019 (COVID-19) Situation Report—51. 2020. Available online: www.who.int/docs/default-source/coronaviruse/situation-reports/20200311-sitrep-51-covid-19.pdf?sfvrsn=1ba62e57_10 (accessed on 9 January 2022).
- Zhao, J.; Zhao, S.; Ou, J.; Zhang, J.; Lan, W.; Guan, W.; Wu, X.; Yan, Y.; Zhao, W.; Wu, J.; et al. COVID-19: Coronavirus Vaccine Development Updates. Front. Immunol. 2020, 11, 602256. [Google Scholar] [CrossRef] [PubMed]
- Castilla, J.; Guevara, M.; Miqueleiz, A.; Baigorria, F.; Ibero-Esparza, C.; Navascués, A.; Trobajo-Sanmartín, C.; Martínez-Baz, I.; Casado, I.; Burgui, C.; et al. Risk Factors of Infection, Hospitalization and Death from SARS-CoV-2: A Population-Based Cohort Study. J. Clin. Med. 2021, 10, 2608. [Google Scholar] [CrossRef] [PubMed]
- Nainu, F.; Abidin, R.S.; Bahar, M.A.; Frediansyah, A.; Bin Emran, T.; Rabaan, A.A.; Dhama, K.; Harapan, H. SARS-CoV-2 reinfection and implications for vaccine development. Hum. Vaccines Immunother. 2020, 16, 3061–3073. [Google Scholar] [CrossRef] [PubMed]
- Sreepadmanabh, M.; Sahu, A.K.; Chande, A. COVID-19: Advances in diagnostic tools, treatment strategies, and vaccine development. J. Biosci. 2020, 45, 148. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, S.; Patel, K.K.; Dehari, D.; Agrawal, A.K.; Singh, S. Melatonin and its ubiquitous anticancer effects. Mol. Cell. Biochem. 2019, 462, 133–155. [Google Scholar] [CrossRef] [PubMed]
- Claustrat, B.; Leston, J. Melatonin: Physiological effects in humans. Neurochirurgie 2015, 61, 77–84. [Google Scholar] [CrossRef]
- Zhang, R.; Wang, X.; Ni, L.; Di, X.; Ma, B.; Niu, S.; Liu, C.; Reiter, R.J. COVID-19: Melatonin as a potential adjuvant treatment. Life Sci. 2020, 250, 117583. [Google Scholar] [CrossRef]
- Reiter, R.J.; Mayo, J.C.; Tan, D.-X.; Sainz, R.M.; Alatorre-Jimenez, M.; Qin, L. Melatonin as an antioxidant: Under promises but over delivers. J. Pineal Res. 2016, 61, 253–278. [Google Scholar] [CrossRef]
- Favero, G.; Franceschetti, L.; Bonomini, F.; Rodella, L.F.; Rezzani, R. Melatonin as an Anti-Inflammatory Agent Modulating Inflammasome Activation. Int. J. Endocrinol. 2017, 2017, 1835195. [Google Scholar] [CrossRef] [Green Version]
- Shiu, S.Y.W.; Reiter, R.J.; Tan, D.-X.; Pang, S.F. Urgent search for safe and effective treatments of severe acute respiratory syndrome: Is melatonin a promising candidate drug? J. Pineal Res. 2003, 35, 69–70. [Google Scholar] [CrossRef]
- Anderson, G.; Maes, M.; Markus, R.P.; Rodriguez, M. Ebola virus: Melatonin as a readily available treatment option. J. Med. Virol. 2015, 87, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Boga, J.A.; Coto-Montes, A.; Rosales-Corral, S.A.; Tan, D.-X.; Reiter, R.J. Beneficial actions of melatonin in the management of viral infections: A new use for this “molecular handyman”? Rev. Med. Virol. 2012, 22, 323–338. [Google Scholar] [CrossRef] [PubMed]
- Acuña-Castroviejo, D.; Escames, G.; Figueira, J.C.; De La Oliva, P.; Borobia, A.M.; Acuña-Fernández, C. Clinical trial to test the efficacy of melatonin in COVID-19. J. Pineal Res. 2020, 69, e12683. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Rubio, M.; Figueira, J.C.; Acuña-Castroviejo, D.; Borobia, A.M.; Escames, G.; De La Oliva, P. A phase II, single-center, double-blind, randomized placebo-controlled trial to explore the efficacy and safety of intravenous melatonin in patients with COVID-19 admitted to the intensive care unit (MelCOVID study): A structured summary of a study protocol for a randomized controlled trial. Trials 2020, 21, 699. [Google Scholar] [CrossRef]
- Scholtens, R.M.; van Munster, B.C.; van Kempen, M.F.; de Rooij, S.E. Physiological melatonin levels in healthy older people: A systematic review. J. Psychosom. Res. 2016, 86, 20–27. [Google Scholar] [CrossRef]
- Gunn, P.J.; Middleton, B.; Davies, S.K.; Revell, V.L.; Skene, D.J. Sex differences in the circadian profiles of melatonin and cortisol in plasma and urine matrices under constant routine conditions. Chronobiol. Int. 2016, 33, 39–50. [Google Scholar] [CrossRef] [Green Version]
- Cipolla-Neto, J.; Amaral, F.; Afeche, S.C.; Tan, D.X.; Reiter, R.J. Melatonin, energy metabolism, and obesity: A review. J. Pineal Res. 2014, 56, 371–381. [Google Scholar] [CrossRef] [Green Version]
- Sun, H.; Gusdon, A.M.; Qu, S. Effects of melatonin on cardiovascular diseases: Progress in the past year. Curr. Opin. Lipidol. 2016, 27, 408–413. [Google Scholar] [CrossRef] [Green Version]
- Álvez, F. SARS-CoV2 coronavirus: So far polite with children. Debatable immunological and non-immunological evidence. Allergol. Immunopathol. 2020, 48, 500–506. [Google Scholar] [CrossRef]
- García, I.G.; Rubio, M.R.; Mariblanca, A.R.; De Soto, L.M.; García, L.D.; Villatoro, J.M.; Parada, J.Q.; Meseguer, E.S.; Rosales, M.J.; González, J.; et al. A randomized multicenter clinical trial to evaluate the efficacy of melatonin in the prophylaxis of SARS-CoV-2 infection in high-risk contacts (MeCOVID Trial): A structured summary of a study protocol for a randomised controlled trial. Trials 2020, 21, 466. [Google Scholar] [CrossRef]
- WHO. Coronavirus Disease 2019 (COVID-19). 2020. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---11-january-2022 (accessed on 12 January 2022).
- Singh, H.; Chauhan, P.; Kakkar, A.K. Hydroxychloroquine for the treatment and prophylaxis of COVID-19: The journey so far and the road ahead. Eur. J. Pharmacol. 2021, 890, 173717. [Google Scholar] [CrossRef] [PubMed]
- Ben-Zvi, I.; Kivity, S.; Langevitz, P.; Shoenfeld, Y. Hydroxychloroquine: From Malaria to Autoimmunity. Clin. Rev. Allergy Immunol. 2011, 42, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Abella, B.S.; Jolkovsky, E.L.; Biney, B.T.; Uspal, J.E.; Hyman, M.C.; Frank, I.; Hensley, S.E.; Gill, S.; Vogl, D.T.; Maillard, I.; et al. Efficacy and Safety of Hydroxychloroquine vs Placebo for Pre-exposure SARS-CoV-2 Prophylaxis Among Health Care Workers: A Randomized Clinical Trial. JAMA Intern. Med. 2021, 181, 195. [Google Scholar] [CrossRef]
- Rajasingham, R.; Bangdiwala, A.S.; Nicol, M.R.; Skipper, C.P.; A Pastick, K.; Axelrod, M.L.; Pullen, M.F.; A Nascene, A.; A Williams, D.; Engen, N.W.; et al. Hydroxychloroquine as Pre-exposure Prophylaxis for Coronavirus Disease 2019 (COVID-19) in Healthcare Workers: A Randomized Trial. Clin. Infect. Dis. 2021, 72, e835–e843. [Google Scholar] [CrossRef] [PubMed]
- Smit, M.; Marinosci, A.; Agoritsas, T.; Calmy, A. Prophylaxis for COVID-19: A systematic review. Clin. Microbiol. Infect. 2021, 27, 532–537. [Google Scholar] [CrossRef]
- Alavian, G.; Kolahdouzan, K.; Mortezazadeh, M.; Dds, Z.S.T. Antiretrovirals for Prophylaxis Against COVID-19: A Comprehensive Literature Review. J. Clin. Pharmacol. 2021, 61, 581–590. [Google Scholar] [CrossRef]
- Del Amo, J.; Polo, R.; Moreno, S.; Diaz-Brito, V.; Martínez, E.; Arribas, J.R.; Jarrín, I.; Hernán, M.A. Incidence and Severity of COVID-19 in HIV-Positive Persons Receiving Antiretroviral Therapy: A Cohort Study. Ann. Intern. Med. 2020, 173, 536–541. [Google Scholar] [CrossRef]
- Ayerdi, O.; Puerta, T.; Clavo, P.; Vera, M.; Ballesteros, J.; Fuentes, M.E.; Estrada, V.; Rodríguez, C.; Del Romero, J.; Lejarraga, C.; et al. Preventive Efficacy of Tenofovir/Emtricitabine Against Severe Acute Respiratory Syndrome Coronavirus 2 Among Pre-Exposure Prophylaxis Users. Open Forum Infect. Dis. 2020, 7, ofaa455. [Google Scholar] [CrossRef]
- ClinicalTrials.gov Randomized Clinical Trial for the Prevention of SARS-CoV-2 Infection (COVID-19) in Healthcare Personnel. Available online: https://ClinicalTrials.gov/show/NCT04334928 (accessed on 14 January 2022).
- ClinicalTrials.gov TAF/FTC for Pre-exposure Prophylaxis of COVID-19 in Healthcare Workers (CoviPrep Study). Available online: https://ClinicalTrials.gov/show/NCT04405271 (accessed on 14 January 2022).
- ClinicalTrials.gov Daily Regimen of Tenofovir/Emtricitabine as Prevention for COVID-19 in Health Care Personnel in Colombia. Available online: https://ClinicalTrials.gov/show/NCT04519125 (accessed on 14 January 2022).
- de Wit, E.; Feldmann, F.; Cronin, J.; Jordan, R.; Okumura, A.; Thomas, T.; Scott, D.; Cihlar, T.; Feldmann, H. Prophylactic and therapeutic remdesivir (GS-5734) treatment in the rhesus macaque model of MERS-CoV infection. Proc. Natl. Acad. Sci. USA 2020, 117, 6771–6776. [Google Scholar] [CrossRef] [Green Version]
- Malin, J.J.; Suárez, I.; Priesner, V.; Fätkenheuer, G.; Rybniker, J. Remdesivir against COVID-19 and Other Viral Diseases. Clin. Microbiol. Rev. 2020, 34, e00162-20. [Google Scholar] [CrossRef]
- Hellwig, M.D.; Maia, A. A COVID-19 prophylaxis? Lower incidence associated with prophylactic administration of ivermectin. Int. J. Antimicrob. Agents 2021, 57, 106248. [Google Scholar] [CrossRef] [PubMed]
- Cruciani, M.; Pati, I.; Masiello, F.; Malena, M.; Pupella, S.; De Angelis, V. Ivermectin for Prophylaxis and Treatment of COVID-19: A Systematic Review and Meta-Analysis. Diagnostics 2021, 11, 1645, Correction in Diagnostics 2021, 11, 2359. [Google Scholar] [CrossRef] [PubMed]
- Hadizadeh, F. Supplementation with vitamin D in the COVID-19 pandemic? Nutr. Rev. 2020, 79, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Ali, N. Role of vitamin D in preventing of COVID-19 infection, progression and severity. J. Infect. Public Health 2020, 13, 1373–1380. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Parameter | Placebo | Melatonin |
|---|---|---|
| ITT Population (N = 314) | N = 151 | N = 163 |
| Age, years (median, [IQR]) | 39 [31, 49] | 41 [32, 49.5] |
| Female sex, n (%) | 123 (81.5%) | 132 (81%) |
| Blood pressure (median, [IQR]) | ||
| Systolic | 118.00 [110.00, 128.00] | 116.00 [105.00, 125.00] |
| Diastolic | 73.00 [66.00, 79.00] | 73.00 [67.50, 78.00] |
| Heart rate (median, [IQR]) | 77.00 [68.00, 83.00] | 75.00 [66.50, 83.00] |
| Weight (median, [IQR]) | 64.40 [57.05, 74.15] | 63.60 [56.10, 71.50] |
| Height (median, [IQR]) | 1.65 [1.60, 1.70] | 1.64 [1.58, 1.70] |
| Comorbidities a n (%) | 64 (42.4) | 56 (34.4) |
| Risk factor for severe COVID-19 b | 24 (15.9) | 16 (9.8) |
| Hypertension c | 6 (4.0) | 4 (2.5) |
| Dyslipidemia c | 4 (2.6) | 3 (1.8) |
| Neoplasia c | 6 (4.0) | 2 (1.2) |
| Respiratory diseases c | 8 (5.3) | 7 (4.3) |
| Obesity c | 0 (0.0) | 1 (0.6) |
| Heart diseases c | 1 (0.6) | 0 (0.0) |
| SARS-CoV-2 Infections | Placebo n (%) | Melatonin n (%) | p-Value a | RR (IC95%) | p-Value b |
|---|---|---|---|---|---|
| ITT (n = 314) | 4 (2.6) | 9 (5.5) | 0.20 | 2.02 (0.64, 6.45) | 0.26 |
| PP (n = 232) | 4 (3.5) | 9 (7.6) | 0.18 | 2.05 (0.65, 6.50) | 0.26 |
| Reported AEs | Placebo Na = 148 | Melatonin Na =160 | p |
|---|---|---|---|
| Nb (%) | Nb (%) | ||
| Related | 31 (20.9) | 44 (27.5) | 1.000 |
| Not Related | 44 (29.7) | 38 (23.8) | 0.290 |
| Related AEs * | |||
| Abnormal dreams | 4 (2.7) | 3 (1.9) | 0.917 |
| Dizziness | 1 (0.7) | 2 (1.2) | 1.000 |
| Dysmenorrhoea | 0 (0.0) | 3 (1.9) | 0.274 |
| Headache | 18 (12.2) | 25 (15.6) | 0.477 |
| Insomnia | 11 (7.4) | 15 (9.4) | 0.684 |
| Somnolence | 2 (1.4) | 14 (8.8) | 0.008 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-García, I.; Seco-Meseguer, E.; Ruiz-Seco, P.; Navarro-Jimenez, G.; Martínez-Porqueras, R.; Espinosa-Díaz, M.; Ortega-Albás, J.J.; Sagastagoitia, I.; García-Morales, M.T.; Jiménez-González, M.; et al. Melatonin in the Prophylaxis of SARS-CoV-2 Infection in Healthcare Workers (MeCOVID): A Randomised Clinical Trial. J. Clin. Med. 2022, 11, 1139. https://doi.org/10.3390/jcm11041139
García-García I, Seco-Meseguer E, Ruiz-Seco P, Navarro-Jimenez G, Martínez-Porqueras R, Espinosa-Díaz M, Ortega-Albás JJ, Sagastagoitia I, García-Morales MT, Jiménez-González M, et al. Melatonin in the Prophylaxis of SARS-CoV-2 Infection in Healthcare Workers (MeCOVID): A Randomised Clinical Trial. Journal of Clinical Medicine. 2022; 11(4):1139. https://doi.org/10.3390/jcm11041139
Chicago/Turabian StyleGarcía-García, Irene, Enrique Seco-Meseguer, Pilar Ruiz-Seco, Gema Navarro-Jimenez, Raúl Martínez-Porqueras, María Espinosa-Díaz, Juan José Ortega-Albás, Iñigo Sagastagoitia, María Teresa García-Morales, María Jiménez-González, and et al. 2022. "Melatonin in the Prophylaxis of SARS-CoV-2 Infection in Healthcare Workers (MeCOVID): A Randomised Clinical Trial" Journal of Clinical Medicine 11, no. 4: 1139. https://doi.org/10.3390/jcm11041139
APA StyleGarcía-García, I., Seco-Meseguer, E., Ruiz-Seco, P., Navarro-Jimenez, G., Martínez-Porqueras, R., Espinosa-Díaz, M., Ortega-Albás, J. J., Sagastagoitia, I., García-Morales, M. T., Jiménez-González, M., Martínez de Soto, L., Bajo-Martínez, A. I., del Palacio-Tamarit, M., López-García, R., Díaz-García, L., Queiruga-Parada, J., Giesen, C., Pérez-Villena, A., de Castro-Martínez, M., ... Borobia, A. M. (2022). Melatonin in the Prophylaxis of SARS-CoV-2 Infection in Healthcare Workers (MeCOVID): A Randomised Clinical Trial. Journal of Clinical Medicine, 11(4), 1139. https://doi.org/10.3390/jcm11041139