

Cardiovascular Risk Profile and Lipid Management in the Population-Based Cohort Study LATINO: 20 Years of Real-World Data
 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participant Selection
2.2. Patient Characterization
2.3. LDL-C Levels, Lipid-Lowering Therapy, and LDL-C Target Achievement
2.4. LLT Exposure
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics and CVD Risk Profile
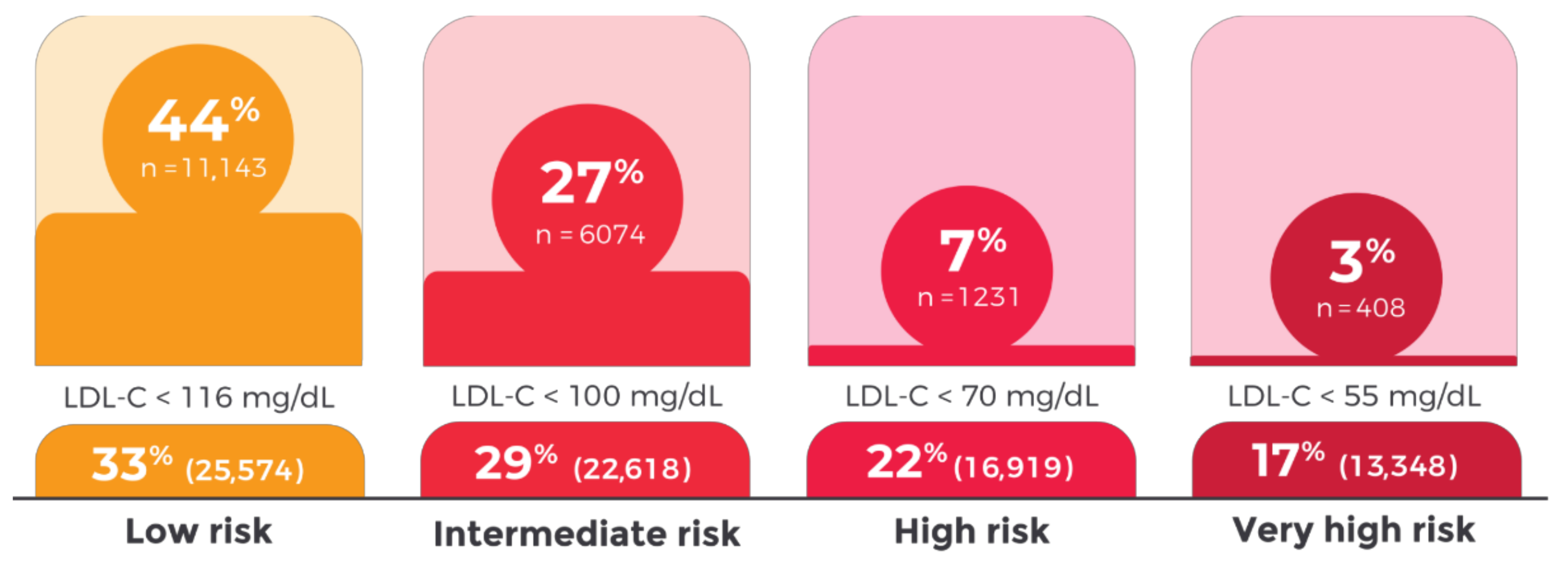
3.2. LDL-C Levels and LDL-C Targets Achieved by CVD Risk
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bourbon, M.; Alves, A.C.; Rato, Q. Prevalência de Fatores de Risco Cardiovascular Na População Portuguesa; Instituto Nacional de Saúde Doutor Ricardo Jorge (INSA, IP): Lisbon, Portugal, 2019. [Google Scholar]
- GBD 2019 Diseases and Injuries Collaborators Global Burden of 369 Diseases and Injuries in 204 Countries and Territories, 1990-2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [CrossRef]
- Gavina, C.; Carvalho, D.S.; Valente, F.; Bernardo, F.; Dinis-Oliveira, R.J.; Santos-Araújo, C.; Taveira-Gomes, T. 20 Years of Real-World Data to Estimate the Prevalence of Heart Failure and Its Subtypes in an Unselected Population of Integrated Care Units. J. Cardiovasc. Dev. Dis. 2022, 9, 149. [Google Scholar] [CrossRef] [PubMed]
- Costa, J.; Alarcão, J.; Amaral-Silva, A.; Araújo, F.; Ascenção, R.; Caldeira, D.; Cardoso, M.F.; Correia, M.; Fiorentino, F.; Gavina, C.; et al. Os Custos Da Aterosclerose Em Portugal. Rev. Port. Cardiol. 2021, 40, 409–419. [Google Scholar] [CrossRef]
- Costa, J.; Alarcão, J.; Araujo, F.; Ascenção, R.; Caldeira, D.; Fiorentino, F.; Gil, V.; Gouveia, M.; Lourenço, F.; Mello E Silva, A.; et al. The Burden of Atherosclerosis in Portugal. Eur. Heart J. Qual. Care Clin. Outcomes 2021, 7, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; John, M.; Backer, D.; Guy, G.; Delgado, V.; et al. 2019 ESC/EAS Guidelines for the Management of Dyslipidaemias: Lipid Modification to Reduce Cardiovascular Risk: The Task Force for the Management of Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur. Heart J. 2019, 41, 111–188. [Google Scholar] [CrossRef]
- Ference, B.A.; Ginsberg, H.N.; Graham, I.; Ray, K.K.; Packard, C.J.; Bruckert, E.; Hegele, R.A.; Krauss, R.M.; Raal, F.J.; Schunkert, H.; et al. Low-Density Lipoproteins Cause Atherosclerotic Cardiovascular Disease. 1. Evidence from Genetic, Epidemiologic, and Clinical Studies. A Consensus Statement from the European Atherosclerosis Society Consensus Panel. Eur. Heart J. 2017, 38, 2459–2472. [Google Scholar] [CrossRef]
- Ference, B.A.; Yoo, W.; Alesh, I.; Mahajan, N.; Mirowska, K.K.; Mewada, A.; Kahn, J.; Afonso, L.; Williams, K.A., Sr.; Flack, J.M. Effect of Long-Term Exposure to Lower Low-Density Lipoprotein Cholesterol Beginning Early in Life on the Risk of Coronary Heart Disease: A Mendelian Randomization Analysis. J. Am. Coll. Cardiol. 2012, 60, 2631–2639. [Google Scholar] [CrossRef]
- Administração Central do Sistema de Saúde Operacionalização Da Contratualização Nos Cuidados de Saúde Primários Para 2019. Available online: https://www.acss.min-saude.pt/wp-content/uploads/2019/02/20190214_Operacionalizacao_CSP_2019_vf.pdf (accessed on 11 November 2022).
- INE—Plataforma de Divulgação Dos Censos 2021—Resultados Provisórios. Available online: https://www.ine.pt/scripts/db_censos_2021.html (accessed on 1 November 2022).
- Portability, I.; Act, A. Guidance Regarding Methods for de-Identification of Protected Health Information in Accordance with the Health Insurance Portability and Accountability Act. Available online: https://privacysecurityacademy.com/wp-content/uploads/2021/03/HHS-OCR-Guidance-on-De-Identification-of-PHI-2012.pdf (accessed on 11 November 2022).
- Scientific Steering Committee on Behalf of the Simon Broome Register Group. Risk of Fatal Coronary Heart Disease in Familial Hypercholesterolaemia. BMJ 1991, 303, 893–896. [Google Scholar] [CrossRef]
- Al-Rasadi, K.; Al-Waili, K.; Al-Sabti, H.A.; Al-Hinai, A.; Al-Hashmi, K.; Al-Zakwani, I.; Banerjee, Y. Criteria for Diagnosis of Familial Hypercholesterolemia: A Comprehensive Analysis of the Different Guidelines, Appraising Their Suitability in the Omani Arab Population. Oman Med. J. 2014, 29, 85–91. [Google Scholar] [CrossRef]
- OMOP CDM v5.3. Available online: https://ohdsi.github.io/CommonDataModel/cdm53.html (accessed on 11 November 2022).
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the Concentration of Low-Density Lipoprotein Cholesterol in Plasma, without Use of the Preparative Ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Catapano, A.L.; Graham, I.; De Backer, G.; Wiklund, O.; Chapman, M.J.; Drexel, H.; Hoes, A.W.; Jennings, C.S.; Landmesser, U.; Pedersen, T.R.; et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias. Eur. Heart J. 2016, 37, 2999–3058. [Google Scholar] [CrossRef] [PubMed]
- Stone, N.J.; Robinson, J.G.; Lichtenstein, A.H.; Bairey Merz, C.N.; Blum, C.B.; Eckel, R.H.; Goldberg, A.C.; Gordon, D.; Levy, D.; Lloyd-Jones, D.M.; et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 129, S1–S45. [Google Scholar] [CrossRef]
- Silverman, M.G.; Ference, B.A.; Im, K.; Wiviott, S.D.; Giugliano, R.P.; Grundy, S.M.; Braunwald, E.; Sabatine, M.S. Association Between Lowering LDL-C and Cardiovascular Risk Reduction Among Different Therapeutic Interventions: A Systematic Review and Meta-Analysis. JAMA 2016, 316, 1289–1297. [Google Scholar] [CrossRef]
- Morieri, M.L.; Avogaro, A.; Fadini, G.P. The DARWIN-T2D Network of the Italian Diabetes Society Cholesterol Lowering Therapies and Achievement of Targets for Primary and Secondary Cardiovascular Prevention in Type 2 Diabetes: Unmet Needs in a Large Population of Outpatients at Specialist Clinics. Cardiovasc. Diabetol. 2020, 19, 190. [Google Scholar]
- Araújo, P.M.; Nunes, A.; Torres, S.; Resende, C.X.; Leite, S.M.; Rodrigues, J.D.; Amorim, S.; Martins, E.; Campelo, M.; Maciel, M.J. Temporal Trends of Lipid Control in Very High Cardiovascular Risk Patients. Rev. Port. Cardiol. 2021, 40, 641–648. [Google Scholar] [CrossRef]
- Lu, Z.; Kou, W.; Du, B.; Wu, Y.; Zhao, S.; Brusco, O.A.; Morgan, J.M.; Capuzzi, D.M.; Chinese Coronary Secondary Prevention Study Group; Li, S. Effect of Xuezhikang, an Extract from Red Yeast Chinese Rice, on Coronary Events in a Chinese Population with Previous Myocardial Infarction. Am. J. Cardiol. 2008, 101, 1689–1693. [Google Scholar] [CrossRef]
- Presta, V.; Figliuzzi, I.; Miceli, F.; Coluccia, R.; Fogacci, F.; Cicero, A.F.G.; Ferrucci, A.; Borghi, C.; Volpe, M.; Tocci, G.; et al. Achievement of Low Density Lipoprotein (LDL) Cholesterol Targets in Primary and Secondary Prevention: Analysis of a Large Real Practice Database in Italy. Atherosclerosis 2019, 285, 40–48. [Google Scholar] [CrossRef]
- März, W.; Dippel, F.-W.; Theobald, K.; Gorcyca, K.; Iorga, Ş.R.; Ansell, D. Utilization of Lipid-Modifying Therapy and Low-Density Lipoprotein Cholesterol Goal Attainment in Patients at High and Very-High Cardiovascular Risk: Real-World Evidence from Germany. Atherosclerosis 2018, 268, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Ray, K.K.; Molemans, B.; Schoonen, W.M.; Giovas, P.; Bray, S.; Kiru, G.; Murphy, J.; Banach, M.; De Servi, S.; Gaita, D.; et al. EU-Wide Cross-Sectional Observational Study of Lipid-Modifying Therapy Use in Secondary and Primary Care: The DA VINCI Study. Eur. J. Prev. Cardiol. 2021, 28, 1279–1289. [Google Scholar] [CrossRef] [PubMed]
- Kotseva, K.; Wood, D.; De Bacquer, D.; De Backer, G.; Rydén, L.; Jennings, C.; Gyberg, V.; Amouyel, P.; Bruthans, J.; Castro Conde, A.; et al. EUROASPIRE IV: A European Society of Cardiology Survey on the Lifestyle, Risk Factor and Therapeutic Management of Coronary Patients from 24 European Countries. Eur. J. Prev. Cardiol. 2016, 23, 636–648. [Google Scholar] [CrossRef]
- Kim, N.H.; Kim, S.G. Fibrates Revisited: Potential Role in Cardiovascular Risk Reduction. Diabetes Metab. J. 2020, 44, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Morieri, M.L.; Pipino, C.; Doria, A. Pharmacogenetics of Cardiovascular Prevention in Diabetes: From Precision Medicine to Identification of Novel Targets. J. Pers. Med. 2022, 12, 1402. [Google Scholar] [CrossRef] [PubMed]
- Keene, D.; Price, C.; Shun-Shin, M.J.; Francis, D.P. Effect on Cardiovascular Risk of High Density Lipoprotein Targeted Drug Treatments Niacin, Fibrates, and CETP Inhibitors: Meta-Analysis of Randomised Controlled Trials Including 117,411 Patients. BMJ 2014, 349, g4379. [Google Scholar] [CrossRef]
- Pradhan, A.D.; Paynter, N.P.; Everett, B.M.; Glynn, R.J.; Amarenco, P.; Elam, M.; Ginsberg, H.; Hiatt, W.R.; Ishibashi, S.; Koenig, W.; et al. Rationale and Design of the Pemafibrate to Reduce Cardiovascular Outcomes by Reducing Triglycerides in Patients with Diabetes (PROMINENT) Study. Am. Heart J. 2018, 206, 80–93. [Google Scholar] [CrossRef] [PubMed]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on Cardiovascular Disease Prevention in Clinical Practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Overall N = 78,459 | Low n = 25,574 | Intermediate n = 22,618 | High n = 16,919 | Very High n = 13,348 | |
|---|---|---|---|---|---|
| Female, n (%) | 45,328 (58) | 18,951 (74) | 12,833 (57) | 7868 (47) | 5676 (43) |
| Age (years), mean (SD) | 59 (11) | 47 (5) | 61 (7) | 67 (10) | 67 (10) |
| Systolic blood pressure (mmHg), median (IQR) | 132 (18) | 125 (18) | 133 (16) | 136 (17) | 137 (19) |
| Diastolic blood pressure (mmHg), median (IQR) | 80 (12) | 80 (12) | 81 (12) | 80 (12) | 80 (13) |
| Body mass index (Kg/m2), median (IQR) | 27 (6) | 26 (6) | 27 (6) | 27 (6) | 28 (6) |
| Waist circumference (cm), median (IQR) | 97 (15) | 92 (17) | 96 (15) | 99 (14) | 101 (15) |
| Smoking history, n (%) | |||||
| Never | 58,388 (74) | 18,870 (74) | 16,167 (72) | 13,480 (80) | 9871 (74) |
| Current | 14,379 (18) | 4797 (19) | 5055 (22) | 2050 (12) | 2477 (19) |
| Former | 3142 (4) | 654 (3) | 907 (4) | 883 (5) | 698 (5) |
| Unknown | 2550 (3) | 1253 (5) | 489 (2) | 506 (3) | 302 (2) |
| Comorbidities, n (%) | |||||
| Hypertension | 39,305 (50) | 5859 (23) | 11,775 (52) | 11,140 (66) | 10,531 (79) |
| Hypercholesterolemia | 39,593 (50) | 12,552 (49) | 12,290 (54) | 8574 (51) | 6177 (46) |
| Obesity | 19,513 (25) | 5045 (20) | 5335 (24) | 4658 (28) | 4475 (34) |
| Type 2 diabetes mellitus | 13,464 (17) | 120 (0.5) | 229 (1) | 4653 (28) | 8462 (63) |
| Structural heart disease | 10,462 (13) | 1098 (4) | 1859 (8) | 2265 (13) | 5240 (39) |
| Microvascular disease | 4019 (5) | 697 (3) | 854 (4) | 725 (4) | 1743 (13) |
| Stable angina | 1957 (2) | 15 (0.1) | 94 (0.4) | 173 (1) | 1675 (13) |
| Atrial fibrillation | 1805 (2) | 49 (0.2) | 304 (1) | 420 (2) | 1032 (8) |
| Chronic kidney disease | 4313 (6) | 0 (0) | 0 (0) | 1669 (10) | 2644 (20) |
| Familial hypercholesterolemia | 767 (1) | 0 (0) | 0 (0) | 46 (0.3) | 721 (5) |
| Definite | 746 (1) | 0 (0) | 0 (0) | 45 (0.3) | 701 (5) |
| Possible | 23 (0) | 0 (0) | 0 (0) | 2 (0) | 21 (0.2) |
| Cardiovascular disease | 43,222 (55) | 6100 (24) | 12,298 (54) | 12,113 (72) | 12,711 (95) |
| Atherosclerotic cardiovascular disease | 5088 (6) | 0 (0) | 0 (0) | 0 (0) | 5088 (38) |
| Ischemic stroke | 3207 (4) | 0 (0) | 0 (0) | 0 (0) | 3207 (24) |
| Peripheral artery disease | 569 (1) | 0 (0) | 0 (0) | 0 (0) | 569 (4) |
| Myocardial infarction | 1665 (2) | 0 (0) | 0 (0) | 0 (0) | 1665 (12) |
| Unstable angina | 309 (0.4) | 0 (0) | 0 (0) | 0 (0) | 309 (2) |
| Overall N = 78,299 | Low n = 25,718 | Intermediate n = 23,357 | High n = 12,857 | Very High n = 16,367 | |
|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | n (%) | |
| Any LLT | 40,281 (52) | 4902 (19) | 13,065 (56) | 9152 (71) | 13,162 (80) |
| Statin | 38,990 (50) | 4566 (18) | 12,662 (54) | 8851 (69) | 12,911 (79) |
| Low-intensity statin | 3163 (8) | 416 (9) | 1094 (9) | 804 (9) | 849 (7) |
| Moderate-intensity statin | 32,965 (85) | 3973 (87) | 10,933 (86) | 7594 (86) | 10,465 (81) |
| High-intensity statin | 2862 (7) | 177 (4) | 635 (5) | 453 (5) | 1597 (12) |
| Ezetimibe + Statin | 3202 (4) | 226 (1) | 849 (4) | 651 (5) | 1476 (9) |
| Ezetimibe + Low-intensity statin | 234 (7) | 24 (11) | 79 (9) | 59 (9) | 72 (5) |
| Ezetimibe + Moderate-intensity statin | 2482 (78) | 193 (85) | 678 (80) | 515 (79) | 1096 (74) |
| Ezetimibe + High-intensity statin | 486 (15) | 9 (4) | 92 (11) | 77 (12) | 308 (21) |
| Ezetimibe mono | 3335 (4) | 244 (1) | 888 (4) | 684 (5) | 1519 (9) |
| Fibrates | 7903 (10) | 917 (4) | 210 (9) | 1824 (14) | 3059 (19) |
| Fibrates + Statin | 2906 (3) | 323 (1) | 688 (3) | 650 (4) | 1215 (7) |
| PCSK9 inhibitors | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Other | 170 (0) | 18 (0) | 51 (0) | 31(0) | 70 (0) |
| Overall N = 78,299 | Low n = 25,718 | Intermediate n = 23,357 | High n = 12,857 | Very High n = 16,367 | |
|---|---|---|---|---|---|
| median (IQR) | median (IQR) | median (IQR) | median (IQR) | median (IQR) | |
| LDL-C, mg/dL | 118 (52) | 114 (47) | 116 (48) | 126 (80) | 120 (60) |
| HDL-C, mg/dL | 48 (16) | 51 (17) | 49 (15) | 47 (16) | 45 (16) |
| Non-HDL-C, mg/dL | 144 (48) | 142 (41) | 144 (47) | 148 (54) | 146 (58) |
| TC, mg/dL | 195 (50) | 194 (43) | 193 (51) | 198 (56) | 195 (60) |
| TG, mg/dL | 102 (66) | 86 (54) | 100 (58) | 114 (77) | 120 (80) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gavina, C.; Carvalho, D.S.; Pardal, M.; Afonso-Silva, M.; Grangeia, D.; Dinis-Oliveira, R.J.; Araújo, F.; Taveira-Gomes, T. Cardiovascular Risk Profile and Lipid Management in the Population-Based Cohort Study LATINO: 20 Years of Real-World Data. J. Clin. Med. 2022, 11, 6825. https://doi.org/10.3390/jcm11226825
Gavina C, Carvalho DS, Pardal M, Afonso-Silva M, Grangeia D, Dinis-Oliveira RJ, Araújo F, Taveira-Gomes T. Cardiovascular Risk Profile and Lipid Management in the Population-Based Cohort Study LATINO: 20 Years of Real-World Data. Journal of Clinical Medicine. 2022; 11(22):6825. https://doi.org/10.3390/jcm11226825
Chicago/Turabian StyleGavina, Cristina, Daniel Seabra Carvalho, Marisa Pardal, Marta Afonso-Silva, Diana Grangeia, Ricardo Jorge Dinis-Oliveira, Francisco Araújo, and Tiago Taveira-Gomes. 2022. "Cardiovascular Risk Profile and Lipid Management in the Population-Based Cohort Study LATINO: 20 Years of Real-World Data" Journal of Clinical Medicine 11, no. 22: 6825. https://doi.org/10.3390/jcm11226825
APA StyleGavina, C., Carvalho, D. S., Pardal, M., Afonso-Silva, M., Grangeia, D., Dinis-Oliveira, R. J., Araújo, F., & Taveira-Gomes, T. (2022). Cardiovascular Risk Profile and Lipid Management in the Population-Based Cohort Study LATINO: 20 Years of Real-World Data. Journal of Clinical Medicine, 11(22), 6825. https://doi.org/10.3390/jcm11226825