
Portal Vein Thrombosis in the Setting of Cirrhosis: A Comprehensive Review

 , , and
, , and
Abstract
1. Introduction
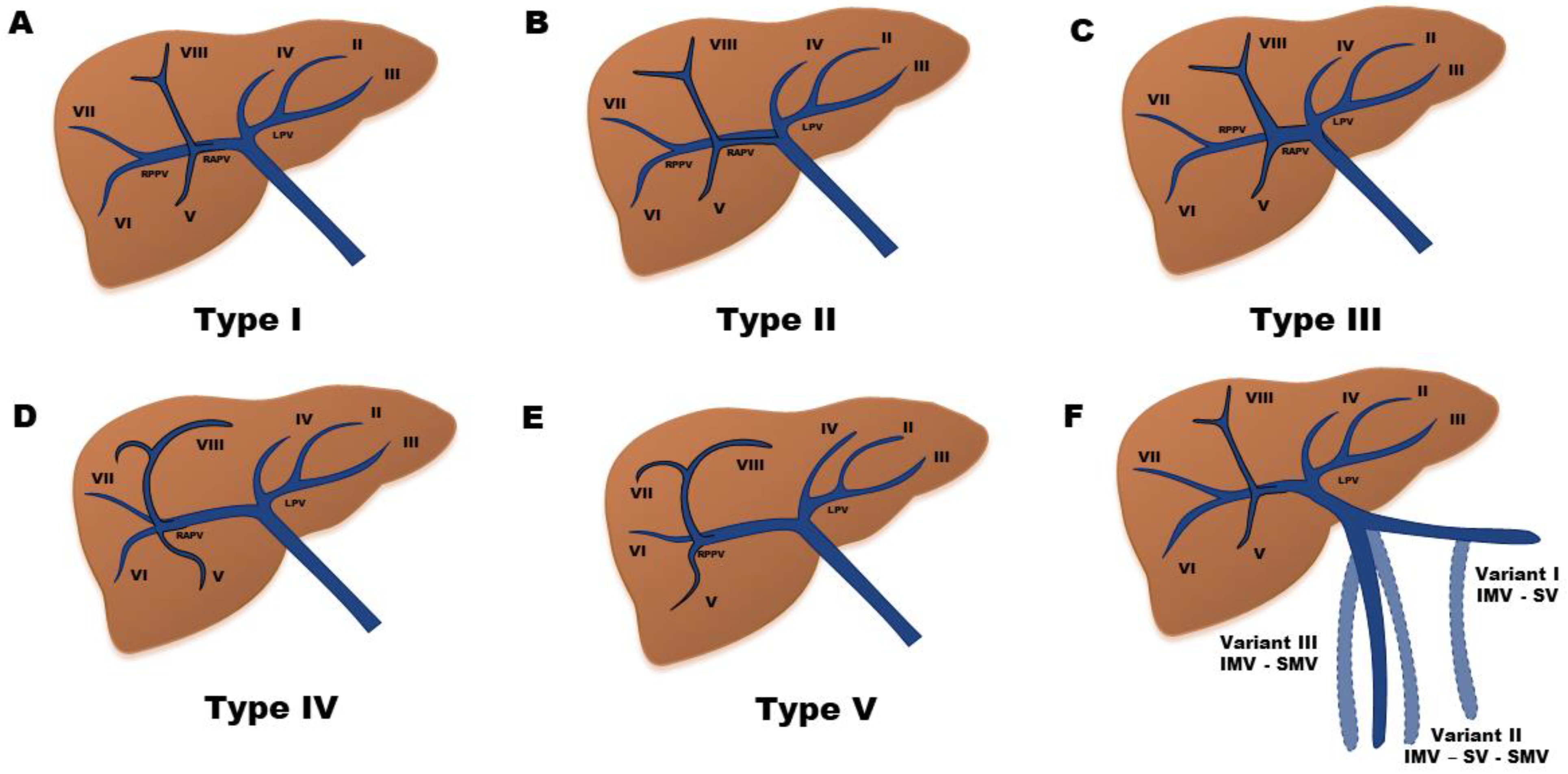
2. Anatomy of the Venous Portal System
3. Classification
4. Pathophysiology and Risk Factors
4.1. Reduced Blood Flow
4.2. Alterations in Coagulation
4.3. Endothelial Damage
5. Epidemiology
6. Clinical Manifestations and Prognostic Impact
7. Natural History
8. Diagnosis
9. Prophylaxis
10. Treatment
10.1. No Treatment
10.2. Anticoagulation
10.2.1. Unfractionated Heparin
10.2.2. Low Molecular Weight Heparin (LMWH)
10.2.3. Fondaparinux
10.2.4. Vitamin K Antagonists
10.2.5. Direct Oral Anticoagulants
10.3. Transjugular Intrahepatic Porto-Systemic Shunt
10.4. Thrombolysis
10.5. Other Considerations
11. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Vascular diseases of the liver. J. Hepatol. 2016, 64, 179–202. [Google Scholar] [CrossRef] [PubMed]
- Simonetto, D.A.; Singal, A.K.; Garcia-Tsao, G.; Caldwell, S.H.; Ahn, J.; Kamath, P.S. ACG Clinical Guideline: Disorders of the Hepatic and Mesenteric Circulation. Am. J. Gastroenterol. 2020, 115, 18–40. [Google Scholar] [CrossRef] [PubMed]
- Northup, P.G.; Garcia-Pagan, J.C.; Garcia-Tsao, G.; Intagliata, N.M.; Superina, R.A.; Roberts, L.N.; Lisman, T.; Valla, D.C. Vascular Liver Disorders, Portal Vein Thrombosis, and Procedural Bleeding in Patients With Liver Disease: 2020 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2021, 73, 366–413. [Google Scholar] [CrossRef]
- de Franchis, R.; Bosch, J.; Garcia-Tsao, G.; Reiberger, T.; Ripoll, C. Baveno VII - Renewing consensus in portal hypertension. J. Hepatol. 2022, 76, 959–974. [Google Scholar] [CrossRef] [PubMed]
- Janssen, H.L.; Meinardi, J.R.; Vleggaar, F.P.; van Uum, S.H.; Haagsma, E.B.; van Der Meer, F.J.; van Hattum, J.; Chamuleau, R.A.; Adang, R.P.; Vandenbroucke, J.P.; et al. Factor V Leiden mutation, prothrombin gene mutation, and deficiencies in coagulation inhibitors associated with Budd-Chiari syndrome and portal vein thrombosis: Results of a case-control study. Blood 2000, 96, 2364–2368. [Google Scholar] [PubMed]
- Janssen, H.L.; Wijnhoud, A.; Haagsma, E.B.; Van Uum, S.H.M.; Van Nieuwkerk, C.M.J.; Adang, R.P.; Chamuleau, R.A.; Van Hattum, J.; Vleggaar, F.P.; Hansen, B.; et al. Extrahepatic portal vein thrombosis: Aetiology and determinants of survival. Gut 2001, 49, 720–724. [Google Scholar] [CrossRef] [PubMed]
- Sogaard, K.K.; Astrup, L.B.; Vilstrup, H.; Gronbaek, H. Portal vein thrombosis; risk factors, clinical presentation and treatment. BMC Gastroenterol. 2007, 7, 34. [Google Scholar] [CrossRef]
- Valla, D.; Casadevall, N.; Huisse, M.G.; Tulliez, M.; Grange, J.D.; Muller, O.; Binda, T.; Varet, B.; Rueff, B.; Benhamou, J.P. Etiology of portal vein thrombosis in adults. A prospective evaluation of primary myeloproliferative disorders. Gastroenterol. 1988, 94, 1063–1069. [Google Scholar] [CrossRef]
- Martin-Llahi, M.; Albillos, A.; Banares, R.; Berzigotti, A.; Garcia-Criado, M.A.; Genesca, J.; Hernandez-Gea, V.; Llop-Herrera, E.; Masnou-Ridaura, H.; Mateoet, J.; et al. Vascular diseases of the liver. Clinical Guidelines from the Catalan Society of Digestology and the Spanish Association for the Study of the Liver. Gastroenterol. Hepatol. 2017, 40, 538–580. [Google Scholar] [CrossRef]
- Intagliata, N.M.; Argo, C.K.; Stine, J.G.; Lisman, T.; Caldwell, S.H.; Violi, F. faculty of the 7th International Coagulation in Liver D. Concepts and Controversies in Haemostasis and Thrombosis Associated with Liver Disease: Proceedings of the 7th International Coagulation in Liver Disease Conference. Thromb. Haemost. 2018, 118, 1491–1506. [Google Scholar]
- O’Leary, J.G.; Greenberg, C.S.; Patton, H.M.; Caldwell, S.H. AGA Clinical Practice Update: Coagulation in Cirrhosis. Gastroenterology 2019, 157, 34–43.e1. [Google Scholar] [CrossRef] [PubMed]
- Di Nisio, M.; Valeriani, E.; Riva, N.; Schulman, S.; Beyer-Westendorf, J.; Ageno, W. Anticoagulant therapy for splanchnic vein thrombosis: ISTH SSC Subcommittee Control of Anticoagulation. J. Thromb. Haemost. 2020, 18, 1562–1568. [Google Scholar] [CrossRef] [PubMed]
- Fortea, J.I.; Puente, Á.; Cuadrado, A.; Huelin, P.; Pellón, R.; González Sánchez, F.J.; Mayorga, M.; Cagigal, M.L.; Carrera, I.G.; Cobreros, M.; et al. Congestive Hepatopathy. Int. J. Mol. Sci. 2020, 21, 9420. [Google Scholar] [CrossRef] [PubMed]
- Krumm, P.; Schraml, C.; Bretschneider, C.; Seeger, A.; Klumpp, B.; Kramer, U.; Claussen, C.D.; Miller, S. Depiction of variants of the portal confluence venous system using multidetector row CT: Analysis of 916 cases. Rofo 2011, 183, 1123–1129. [Google Scholar] [CrossRef]
- Cheng, Y.F.; Huang, T.L.; Lee, T.Y.; Chen, T.Y.; Chen, C.L. Variation of the intrahepatic portal vein; angiographic demonstration and application in living-related hepatic transplantation. Transplant. Proc. 1996, 28, 1667–1668. [Google Scholar] [PubMed]
- Yerdel, M.A.; Gunson, B.; Mirza, D.; Karayalçin, K.; Olliff, S.; Buckels, J.; Mayer, D.; McMaster, P.; Pirenne, J. Portal vein thrombosis in adults undergoing liver transplantation: Risk factors, screening, management, and outcome. Transplantation 2000, 69, 1873–1881. [Google Scholar] [CrossRef]
- Bauer, J.; Johnson, S.; Durham, J.; Ludkowski, M.; Trotter, J.; Bak, T.; Wachs, M. The role of TIPS for portal vein patency in liver transplant patients with portal vein thrombosis. Liver Transplant. 2006, 12, 1544–1551. [Google Scholar] [CrossRef]
- Sarin, S.K.; Philips, C.A.; Kamath, P.S.; Choudhury, A.; Maruyama, H.; Nery, F.G.; Valla, D.C. Toward a Comprehensive New Classification of Portal Vein Thrombosis in Patients with Cirrhosis. Gastroenterology 2016, 151, 574–577.e573. [Google Scholar] [CrossRef]
- Bhangui, P.; Lim, C.; Levesque, E.; Salloum, C.; Lahat, E.; Feray, C.; Azoulay, D. Novel classification of non-malignant portal vein thrombosis: A guide to surgical decision-making during liver transplantation. J. Hepatol. 2019, 71, 1038–1050. [Google Scholar] [CrossRef]
- Plessier, A.; Darwish-Murad, S.; Hernandez-Guerra, M.; Consigny, Y.; Fabris, F.; Trebicka, J.; Heller, J.; Morard, I.; Lasser, L.; Langlet, P.; et al. Acute portal vein thrombosis unrelated to cirrhosis: A prospective multicenter follow-up study. Hepatology 2010, 51, 210–218. [Google Scholar] [CrossRef]
- Senzolo, M.; Sartori, T.M.; Rossetto, V.; Burra, P.; Cillo, U.; Boccagni, P.; Gasparini, D.; Miotto, D.; Simioni, P.; Tsochatzis, E.; et al. Prospective evaluation of anticoagulation and transjugular intrahepatic portosystemic shunt for the management of portal vein thrombosis in cirrhosis. Liver Int. 2012, 32, 919–927. [Google Scholar] [CrossRef] [PubMed]
- Maruyama, H.; Takahashi, M.; Shimada, T.; Yokosuka, O. Emergency anticoagulation treatment for cirrhosis patients with portal vein thrombosis and acute variceal bleeding. Scand. J. Gastroenterol. 2012, 47, 686–691. [Google Scholar] [CrossRef] [PubMed]
- De Gaetano, A.M.; Lafortune, M.; Patriquin, H.; De Franco, A.; Aubin, B.; Paradis, K. Cavernous transformation of the portal vein: Patterns of intrahepatic and splanchnic collateral circulation detected with Doppler sonography. AJR Am. J. Roentgenol. 1995, 165, 1151–1155. [Google Scholar] [CrossRef] [PubMed]
- Anton, A.; Campreciós, G.; Pérez-Campuzano, V.; Orts, L.; García-Pagán, J.C.; Hernández-Gea, V. The Pathophysiology of Portal Vein Thrombosis in Cirrhosis: Getting Deeper into Virchow’s Triad. J. Clin. Med. 2022, 11, 800. [Google Scholar] [CrossRef] [PubMed]
- Zocco, M.A.; Di Stasio, E.; De Cristofaro, R.; Novi, M.; Ainora, M.E.; Ponziani, F.; Riccardi, L.; Lancellotti, S.; Santoliquido, A.; Flore, R.; et al. Thrombotic risk factors in patients with liver cirrhosis: Correlation with MELD scoring system and portal vein thrombosis development. J. Hepatol. 2009, 51, 682–689. [Google Scholar] [CrossRef]
- Abdel-Razik, A.; Mousa, N.; Elhelaly, R.; Tawfik, A. De-novo portal vein thrombosis in liver cirrhosis: Risk factors and correlation with the Model for End-stage Liver Disease scoring system. Eur. J. Gastroenterol. Hepatol. 2015, 27, 585–592. [Google Scholar] [CrossRef]
- Stine, J.G.; Wang, J.; Shah, P.M.; Argo, C.K.; Intagliata, N.; Uflacker, A.; Caldwell, S.H.; Northup, P.G. Decreased portal vein velocity is predictive of the development of portal vein thrombosis: A matched case-control study. Liver Int. 2018, 38, 94–101. [Google Scholar] [CrossRef]
- Turon, F.; Driever, E.G.; Baiges, A.; Cerda, E.; García-Criado, Á.; Gilabert, R.; Bru, C.; Berzigotti, A.; Nuñez, I.; Orts, L.; et al. Predicting portal thrombosis in cirrhosis: A prospective study of clinical, ultrasonographic and hemostatic factors. J. Hepatol. 2021, 75, 1367–1376. [Google Scholar] [CrossRef]
- Nery, F.; Chevret, S.; Condat, B.; de Raucourt, E.; Boudaoud, L.; Rautou, P.E.; Plessier, A.; Roulot, D.; Chaffaut, C.; Bourcier, V.; et al. Causes and consequences of portal vein thrombosis in 1,243 patients with cirrhosis: Results of a longitudinal study. Hepatology 2015, 61, 660–667. [Google Scholar] [CrossRef]
- Maruyama, H.; Okugawa, H.; Takahashi, M.; Yokosuka, O. De novo portal vein thrombosis in virus-related cirrhosis: Predictive factors and long-term outcomes. Am. J. Gastroenterol. 2013, 108, 568–574. [Google Scholar] [CrossRef]
- Dong, G.; Huang, X.Q.; Zhu, Y.L.; Ding, H.; Li, F.; Chen, S.Y. Increased portal vein diameter is predictive of portal vein thrombosis development in patients with liver cirrhosis. Ann. Transl. Med. 2021, 9, 289. [Google Scholar] [CrossRef] [PubMed]
- Luca, A.; Miraglia, R.; Caruso, S.; Milazzo, M.; Sapere, C.; Maruzzelli, L.; Vizzini, G.; Tuzzolino, F.; Gridelli, B.; Bosch, J. Short- and long-term effects of the transjugular intrahepatic portosystemic shunt on portal vein thrombosis in patients with cirrhosis. Gut 2011, 60, 846–852. [Google Scholar] [CrossRef] [PubMed]
- Nery, F.; Correia, S.; Macedo, C.; Gandara, J.; Lopes, V.; Valadares, D.; Ferreira, S.; Oliveira, J.; Gomes, M.T.; Lucas, R.; et al. Nonselective beta-blockers and the risk of portal vein thrombosis in patients with cirrhosis: Results of a prospective longitudinal study. Aliment. Pharmacol. Ther. 2019, 49, 582–588. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Xu, S.; Primignani, M.; De Stefano, V.; He, Y.; Yi, F.; Guo, X.; Valla, D.; Qi, X. Nonselective β-Blockers May Progress the Thrombosis of Portal Venous System in Cirrhotic Patients: A Retrospective Observational Study. Adv. Ther. 2020, 37, 1452–1463. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Guo, X.; De Stefano, V.; Silva-Junior, G.; Goyal, H.; Bai, Z.; Zhao, Q.; Qi, X. Nonselective beta-blockers and development of portal vein thrombosis in liver cirrhosis: A systematic review and meta-analysis. Hepatol. Int. 2019, 13, 468–481. [Google Scholar] [CrossRef]
- EASL. Clinical Practice Guidelines on prevention and management of bleeding and thrombosis in patients with cirrhosis. J. Hepatol. 2022, 76, 1151–1184. [Google Scholar] [CrossRef]
- Turco, L.; de Raucourt, E.; Valla, D.C.; Villa, E. Anticoagulation in the cirrhotic patient. JHEP Rep. 2019, 1, 227–239. [Google Scholar] [CrossRef]
- Tripodi, A.; Primignani, M.; Chantarangkul, V.; Dell’Era, A.; Clerici, M.; de Franchis, R.; Colombo, M.; Mannucci, P.M. An imbalance of pro- vs anti-coagulation factors in plasma from patients with cirrhosis. Gastroenterology 2009, 137, 2105–2111. [Google Scholar] [CrossRef]
- Scheiner, B.; Balcar, L.; Nussbaumer, R.J.; Weinzierl, J.; Paternostro, R.; Simbrunner, B.; Hartl, L.; Jachs, M.; Bauer, D.; Stättermayer, A.F.; et al. Factor VIII/protein C ratio independently predicts liver-related events but does not indicate a hypercoagulable state in ACLD. J. Hepatol. 2022, 76, 1090–1099. [Google Scholar] [CrossRef]
- Kalambokis, G.N.; Oikonomou, A.; Christou, L.; Baltayiannis, G. High von Willebrand factor antigen levels and procoagulant imbalance may be involved in both increasing severity of cirrhosis and portal vein thrombosis. Hepatology 2016, 64, 1383–1385. [Google Scholar] [CrossRef]
- Ren, W.; Zhang, J.; Chen, Y.; Wen, M.; Su, Y.; Zhao, Y.; Lu, S.; Wu, J. Evaluation of Coagulation, Fibrinolysis and Endothelial Biomarkers in Cirrhotic Patients With or Without Portal Venous Thrombosis. Clin. Appl Thromb. Hemost. 2020, 26, 1076029620982666. [Google Scholar] [CrossRef] [PubMed]
- Zanetto, A.; Pelizzaro, F.; Campello, E.; Bulato, C.; Balcar, L.; Gu, W.; Gavasso, S.; Saggiorato, G.; Zeuzem, S.; Russo, F.P.; et al. Severity of systemic inflammation is the main predictor of ACLF and bleeding in patients with acutely decompensated cirrhosis. J. Hepatol. 2022, S0168-8278(22)03110-5. [Google Scholar] [CrossRef]
- Delahousse, B.; Labat-Debelleix, V.; Decalonne, L.; d’Alteroche, L.; Perarnau, J.M.; Gruel, Y. Comparative study of coagulation and thrombin generation in the portal and jugular plasma of patients with cirrhosis. Thromb. Haemost. 2010, 104, 741–749. [Google Scholar] [PubMed]
- Praktiknjo, M.; Trebicka, J.; Carnevale, R.; Pastori, D.; Queck, A.; Ettorre, E.; Violi, F. Von Willebrand and Factor VIII Portosystemic Circulation Gradient in Cirrhosis: Implications for Portal Vein Thrombosis. Clin. Transl. Gastroenterol. 2020, 11, e00123. [Google Scholar] [CrossRef]
- Driever, E.G.; Magaz, M.; Adelmeijer, J.; Turon, F.; Baiges, A.; Olivas, P.; Pérez-Campuzano, V.; Hernandez-Gea, V.; Blasi, A.; Garcia-Pagan, J.; et al. The portal vein in patients with cirrhosis is not an excessively inflammatory or hypercoagulable vascular bed, a prospective cohort study. J. Thromb. Haemost. 2022, 20, 2075–2082. [Google Scholar] [CrossRef]
- Shalaby, S.; Zanetto, A.; Campello, E.; Gavasso, S.; Barbiero, G.; Battistel, M.; Feltracco, P.; Bizzaro, D.; Burra, P.; Simioni, P.; et al. Reply to “Peripheral versus central venous blood sampling does not influence the assessment of platelet activation in cirrhosis”. Platelets 2022, 33, 1104–1106. [Google Scholar] [CrossRef]
- Zanetto, A.; Campello, E.; Bulato, C.; Gavasso, S.; Farinati, F.; Russo, F.P.; Tormene, D.; Burra, P.; Senzolo, M.; Simioni, P. Increased platelet aggregation in patients with decompensated cirrhosis indicates higher risk of further decompensation and death. J. Hepatol. 2022, 77, 660–669. [Google Scholar] [CrossRef]
- Quan, X.; Ye, X.; Qian, S.; Wei, B.; Tong, H.; Wang, Z.; Tai, Y.; Guo, X.; Gao, J.; Wu, H. Portal vein thrombosis associates with high platelet-fibrin clot strength and platelet activation in decompensated cirrhosis: A retrospective study. Dig. Liver Dis. 2022. [Google Scholar] [CrossRef]
- Zanetto, A.; Campello, E.; Burra, P.; Senzolo, M.; Simioni, P. Increased platelet ratio in patients with decompensated cirrhosis indicates higher risk of portal vein thrombosis. Liver Int. 2022. [Google Scholar] [CrossRef]
- Sacco, M.; Tardugno, M.; Lancellotti, S.; Ferretti, A.; Ponziani, F.R.; Riccardi, L.; Zocco, M.A.; De Magistris, A.; Santopaolo, F.; Pompili, M.; et al. ADAMTS-13/von Willebrand factor ratio: A prognostic biomarker for portavein thrombosis in compensated cirrhosis. A prospective observational study. Dig. Liver Dis. 2022, S1590-8658(22)00543-6. [Google Scholar] [CrossRef]
- Arroyo, V.; Angeli, P.; Moreau, R.; Jalan, R.; Clària, J.; Trebicka, J.; Fernández, J.; Gustot, T.; Caraceni, P.; Bernardi, M. The systemic inflammation hypothesis: Towards a new paradigm of acute decompensation and multiorgan failure in cirrhosis. J. Hepatol. 2021, 74, 670–685. [Google Scholar] [CrossRef] [PubMed]
- Zanetto, A.; Campello, E.; Pelizzaro, F.; Farinati, F.; Burra, P.; Simioni, P.; Senzolo, M. Haemostatic alterations in patients with cirrhosis and hepatocellular carcinoma: Laboratory evidence and clinical implications. Liver Int. 2022, 42, 1229–1240. [Google Scholar] [CrossRef] [PubMed]
- Basili, S.; Carnevale, R.; Nocella, C.; Bartimoccia, S.; Raparelli, V.; Talerico, G.; Stefanini, L.; Romiti, G.F.; Perticone, F.; Corazza, G.R.; et al. Serum Albumin Is Inversely Associated With Portal Vein Thrombosis in Cirrhosis. Hepatol. Commun. 2019, 3, 504–512. [Google Scholar] [CrossRef]
- Caraceni, P.; Riggio, O.; Angeli, P.; Alessandria, C.; Neri, S.; Foschi, F.G.; Levantesi, F.; Airoldi, A.; Boccia, S.; Svegliati-Baroni, G.; et al. Long-term albumin administration in decompensated cirrhosis (ANSWER): An open-label randomised trial. Lancet 2018, 391, 2417–2429. [Google Scholar] [CrossRef]
- Solà, E.; Solé, C.; Simón-Talero, M.; Martín-Llahí, M.; Castellote, J.; Garcia-Martínez, R.; Moreira, R.; Torrens, M.; Márquez, F.; Fabrellas, N.; et al. Midodrine and albumin for prevention of complications in patients with cirrhosis awaiting liver transplantation. A randomized placebo-controlled trial. J. Hepatol. 2018, 69, 1250–1259. [Google Scholar] [CrossRef]
- Mahmoud, A.E.; Elias, E.; Beauchamp, N.; Wilde, J.T. Prevalence of the factor V Leiden mutation in hepatic and portal vein thrombosis. Gut 1997, 40, 798–800. [Google Scholar] [CrossRef]
- Amitrano, L.; Guardascione, M.A.; Brancaccio, V.; Margaglione, M.; Manguso, F.; Iannaccone, L.; Grandone, E.; Balzano, A. Risk factors and clinical presentation of portal vein thrombosis in patients with liver cirrhosis. J. Hepatol. 2004, 40, 736–741. [Google Scholar] [CrossRef]
- Amitrano, L.; Brancaccio, V.; Guardascione, M.A.; Margaglione, M.; Iannaccone, L.; D’Andrea, G.; Marmo, R.; Ames, P.R.; Balzano, A. Inherited coagulation disorders in cirrhotic patients with portal vein thrombosis. Hepatology 2000, 31, 345–348. [Google Scholar] [CrossRef]
- Amitrano, L.; Guardascione, M.A.; Ames, P.R.; Margaglione, M.; Iannaccone, L.; Brancaccio, V.; Balzano, A. Increased plasma prothrombin concentration in cirrhotic patients with portal vein thrombosis and prothrombin G20210A mutation. Thromb. Haemost. 2006, 95, 221–223. [Google Scholar]
- Amitrano, L.; Ames, P.R.; Guardascione, M.A.; Lopez, L.R.; Menchise, A.; Brancaccio, V.; Iannaccone, L.; Balzano, A. Antiphospholipid antibodies and antiphospholipid syndrome: Role in portal vein thrombosis in patients with and without liver cirrhosis. Clin. Appl. Thromb. Hemost. 2011, 17, 367–370. [Google Scholar] [CrossRef]
- Mangia, A.; Villani, M.R.; Cappucci, G.; Santoro, R.; Ricciardi, R.; Facciorusso, D.; Leandro, G.; Caruso, N.; Andriulli, A. Causes of portal venous thrombosis in cirrhotic patients: The role of genetic and acquired factors. Eur. J. Gastroenterol. Hepatol. 2005, 17, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Pasta, L.; Marrone, C.; D’Amico, M.; Virdone, R.; D'Amico, G.; Sammarco, P.; Fabiano, C.; Pagliaro, L. MTHFR C677T mutations in liver cirrhosis with and without portal vein thrombosis. Liver Int. 2006, 26, 269–270. [Google Scholar] [CrossRef] [PubMed]
- Pasta, L.; Pasta, F.; D’Amico, M. PAI-1 4G-4G, MTHFR 677TT, V Leiden 506Q, and Prothrombin 20210A in Splanchnic Vein Thrombosis: Analysis of Individual Patient Data from Three Prospective Studies. J. Clin. Exp. Hepatol. 2016, 6, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Colaizzo, D.; Amitrano, L.; Guardascione, M.A.; Balzano, A.; Margaglione, M. Janus kinase-2 mutation, cirrhosis and splanchnic vein thrombosis. Eur. J. Gastroenterol. Hepatol. 2008, 20, 245–246. [Google Scholar] [CrossRef] [PubMed]
- Gabr, M.A.; Bessa, S.S.; El-Zamarani, E.A. Portal vein thrombosis in Egyptian patients with liver cirrhosis: Role of methylenetetrahydrofolate reductase C677T gene mutation. Hepatol. Res. 2010, 40, 486–493. [Google Scholar] [CrossRef]
- Ayala, R.; Grande, S.; Bustelos, R.; Ribera, C.; García-Sesma, A.; Jimenez, C.A.; Moreno, E.; Martínez-López, J. Obesity is an independent risk factor for pre-transplant portal vein thrombosis in liver recipients. BMC Gastroenterol. 2012, 12, 114. [Google Scholar] [CrossRef]
- Qi, X.; Zhang, C.; Han, G.; Zhang, W.; He, C.; Yin, Z.; Liu, Z.; Bai, W.; Li, R.; Bai, M.; et al. Prevalence of the JAK2V617F mutation in Chinese patients with Budd-Chiari syndrome and portal vein thrombosis: A prospective study. J. Gastroenterol. Hepatol. 2012, 27, 1036–1043. [Google Scholar] [CrossRef]
- Werner, K.T.; Sando, S.; Carey, E.J.; Vargas, H.E.; Byrne, T.J.; Douglas, D.D.; Harrison, M.E.; Rakela, J.; Aqel, B.A. Portal vein thrombosis in patients with end stage liver disease awaiting liver transplantation: Outcome of anticoagulation. Dig. Dis. Sci. 2013, 58, 1776–1780. [Google Scholar] [CrossRef]
- Karakose, S.; Oruc, N.; Zengin, M.; Akarca, U.S.; Ersoz, G. Diagnostic value of the JAK2 V617F mutation for latent chronic myeloproliferative disorders in patients with Budd-Chiari syndrome and/or portal vein thrombosis. Turk. J. Gastroenterol. 2015, 26, 42–48. [Google Scholar] [CrossRef]
- Saugel, B.; Lee, M.; Feichtinger, S.; Hapfelmeier, A.; Schmid, R.M.; Siveke, J.T. Thrombophilic factor analysis in cirrhotic patients with portal vein thrombosis. J. Thromb. Thrombolysis 2015, 40, 54–60. [Google Scholar] [CrossRef]
- Lancellotti, S.; Basso, M.; Veca, V.; Sacco, M.; Riccardi, L.; Pompili, M.; De Cristofaro, R. Presence of portal vein thrombosis in liver cirrhosis is strongly associated with low levels of ADAMTS-13: A pilot study. Intern. Emerg. Med. 2016, 11, 959–967. [Google Scholar] [CrossRef] [PubMed]
- Ventura, P.; Venturelli, G.; Marcacci, M.; Fiorini, M.; Marchini, S.; Cuoghi, C.; Pietrangelo, A. Hyperhomocysteinemia and MTHFR C677T polymorphism in patients with portal vein thrombosis complicating liver cirrhosis. Thromb. Res. 2016, 141, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Artaza, T.; Lopes, M.; Romero, M.; Gomez, A.Z.; de la Cruz, G.; Sanchez, J.J.; Gonzalez, C.; Gómez, R. Efficacy and safety of anticoagulation in non-malignant portal vein thrombosis in patients with liver cirrhosis. Gastroenterol. Hepatol. 2018, 41, 611–617. [Google Scholar] [CrossRef] [PubMed]
- Senzolo, M.; Riva, N.; Dentali, F.; Rodriguez-Castro, K.; Sartori, M.T.; Bang, S.-M.; Martinelli, I.; Schulman, S.; Alatri, A.; Beyer-Westendorf, J.; et al. Long-Term Outcome of Splanchnic Vein Thrombosis in Cirrhosis. Clin. Transl. Gastroenterol. 2018, 9, 176. [Google Scholar] [CrossRef]
- Cagin, Y.F.; Bilgic, Y.; Berber, I.; Yildirim, O.; Erdogan, M.A.; Firat, F.; Arslan, A.K.; Colak, C.; Seckin, Y.; Harputluoglu, M. The risk factors of portal vein thrombosis in patients with liver cirrhosis. Exp. Ther. Med. 2019, 17, 3189–3194. [Google Scholar] [CrossRef]
- Tremblay, D.; Naymagon, L.; Troy, K.; Cromwell, C.; Edwards, C.; Schiano, T.; Kremyanskaya, M.; Mascarenhas, J. The utility of thrombophilia testing in patients with newly diagnosed portal vein thrombosis. Blood Coagul. Fibrinolysis 2020, 31, 213–218. [Google Scholar] [CrossRef]
- Fortea, J.I.; Carrera, I.G.; Puente, Á.; Cuadrado, A.; Huelin, P.; Tato, C.; Fernández, P.; Montes, M.D.R.P.; Céspedes, J.N.; López, A.B.; et al. Portal Thrombosis in Cirrhosis: Role of Thrombophilic Disorders. J. Clin. Med. 2020, 9, 2822. [Google Scholar] [CrossRef]
- Dentali, F.; Galli, M.; Gianni, M.; Ageno, W. Inherited thrombophilic abnormalities and risk of portal vein thrombosis. a meta-analysis. Thromb. Haemost. 2008, 99, 675–682. [Google Scholar]
- Qi, X.; Ren, W.; De Stefano, V.; Fan, D. Associations of coagulation factor V Leiden and prothrombin G20210A mutations with Budd-Chiari syndrome and portal vein thrombosis: A systematic review and meta-analysis. Clin. Gastroenterol. Hepatol. 2014, 12, 1801–1812.e1807. [Google Scholar] [CrossRef]
- Ma, S.D.; Wang, J.; Bezinover, D.; Kadry, Z.; Northup, P.G.; Stine, J.G. Inherited thrombophilia and portal vein thrombosis in cirrhosis: A systematic review and meta-analysis. Res. Pract. Thromb. Haemost. 2019, 3, 658–667. [Google Scholar] [CrossRef]
- Qi, X.; Chen, H.; Han, G. Effect of antithrombin, protein C and protein S on portal vein thrombosis in liver cirrhosis: A meta-analysis. Am. J. Med. Sci. 2013, 346, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Colucci, G.; Tsakiris, D.A. Thrombophilia screening revisited: An issue of personalized medicine. J. Thromb. Thrombolysis 2020, 49, 618–629. [Google Scholar] [CrossRef] [PubMed]
- Intagliata, N.M.; Caldwell, S.H.; Tripodi, A. Diagnosis, Development, and Treatment of Portal Vein Thrombosis in Patients with and without Cirrhosis. Gastroenterology 2019, 156, 1582–1599.e1581. [Google Scholar] [CrossRef] [PubMed]
- Shukla, A.; Giri, S. Portal Vein Thrombosis in Cirrhosis. J. Clin. Exp. Hepatol. 2022, 12, 965–979. [Google Scholar] [CrossRef] [PubMed]
- Noronha Ferreira, C.; Marinho, R.T.; Cortez-Pinto, H.; Ferreira, P.; Dias, M.S.; Vasconcelos, M.; Alexandrino, P.; Serejo, F.; Pedro, A.J.; Gonçalves, A.; et al. Incidence, predictive factors and clinical significance of development of portal vein thrombosis in cirrhosis: A prospective study. Liver Int. 2019, 39, 1459–1467. [Google Scholar] [CrossRef]
- Violi, F.; Corazza, G.R.; Caldwell, S.H.; Talerico, G.; Romiti, G.F.; Napoleone, L.; Perticone, F.; Bolondi, L.; Pietrangelo, A.; Vestri, A.R.; et al. Incidence and Recurrence of Portal Vein Thrombosis in Cirrhotic Patients. Thromb. Haemost. 2019, 119, 496–499. [Google Scholar] [CrossRef]
- Pan, J.; Wang, L.; Gao, F.; An, Y.; Yin, Y.; Guo, X.; Nery, F.G.; Yoshida, E.M.; Qi, X. Epidemiology of portal vein thrombosis in liver cirrhosis: A systematic review and meta-analysis. Eur. J. Intern. Med. 2022, 104, 21–32. [Google Scholar] [CrossRef]
- Ogren, M.; Bergqvist, D.; Björck, M.; Acosta, S.; Eriksson, H.; Sternby, N.H. Portal vein thrombosis: Prevalence, patient characteristics and lifetime risk: A population study based on 23,796 consecutive autopsies. World J. Gastroenterol. 2006, 12, 2115–2119. [Google Scholar] [CrossRef]
- Stine, J.G.; Shah, N.L.; Argo, C.K.; Pelletier, S.J.; Caldwell, S.H.; Northup, P.G. Increased risk of portal vein thrombosis in patients with cirrhosis due to nonalcoholic steatohepatitis. Liver Transplant. 2015, 21, 1016–1021. [Google Scholar] [CrossRef]
- Zanetto, A.; Garcia-Tsao, G. Some Answers and More Questions About Portal Vein Thrombosis in Patients with Decompensated Cirrhosis. Clin. Gastroenterol. Hepatol. 2020, 18, 2432–2434. [Google Scholar] [CrossRef]
- Berry, K.; Taylor, J.; Liou, I.W.; Ioannou, G.N. Portal vein thrombosis is not associated with increased mortality among patients with cirrhosis. Clin. Gastroenterol. Hepatol. 2015, 13, 585–593. [Google Scholar] [CrossRef] [PubMed]
- John, B.V.; Konjeti, R.; Aggarwal, A.; Lopez, R.; Atreja, A.; Miller, C.; Zein, N.N.; Carey, W. Impact of untreated portal vein thrombosis on pre and post liver transplant outcomes in cirrhosis. Ann. Hepatol. 2013, 12, 952–958. [Google Scholar] [CrossRef]
- Luca, A.; Caruso, S.; Milazzo, M.; Marrone, G.; Mamone, G.; Crinò, F.; Maruzzelli, L.; Miraglia, R.; Floridia, G.; Vizzini, G. Natural course of extrahepatic nonmalignant partial portal vein thrombosis in patients with cirrhosis. Radiology 2012, 265, 124–132. [Google Scholar] [CrossRef]
- Villa, E.; Cammà, C.; Marietta, M.; Luongo, M.; Critelli, R.; Colopi, S.; Tata, C.; Zecchini, R.; Gitto, S.; Petta, S.; et al. Enoxaparin prevents portal vein thrombosis and liver decompensation in patients with advanced cirrhosis. Gastroenterology 2012, 143, 1253–1260.e4. [Google Scholar] [CrossRef]
- D’Amico, G.; De Franchis, R. Upper digestive bleeding in cirrhosis. Post-therapeutic outcome and prognostic indicators. Hepatology 2003, 38, 599–612. [Google Scholar] [CrossRef] [PubMed]
- Amitrano, L.; Guardascione, M.A.; Scaglione, M.; Menchise, A.; Martino, R.; Manguso, F.; Lanza, A.G.; Lampasi, F. Splanchnic vein thrombosis and variceal rebleeding in patients with cirrhosis. Eur. J. Gastroenterol. Hepatol. 2012, 24, 1381–1385. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Xu, B.-Y.; Wang, X.-B.; Zheng, X.; Huang, Y.; Chen, J.; Meng, Z.-J.; Gao, Y.-H.; Qian, Z.-P.; Liu, F.; et al. Prevalence and Clinical Significance of Portal Vein Thrombosis in Patients with Cirrhosis and Acute Decompensation. Clin. Gastroenterol. Hepatol. 2020, 18, 2564–2572.e1. [Google Scholar] [CrossRef]
- Chen, H.; Turon, F.; Hernandez-Gea, V.; Fuster, J.; Garcia-Criado, A.; Barrufet, M.; Darnell, A.; Fondevila, C.; Garcia-Valdecasas, J.C.; Garcia-Pagán, J.C. Nontumoral portal vein thrombosis in patients awaiting liver transplantation. Liver Transpl. 2016, 22, 352–365. [Google Scholar] [CrossRef]
- Englesbe, M.J.; Schaubel, D.E.; Cai, S.; Guidinger, M.K.; Merion, R.M. Portal vein thrombosis and liver transplant survival benefit. Liver Transplant. 2010, 16, 999–1005. [Google Scholar] [CrossRef]
- Ghabril, M.; Agarwal, S.; Lacerda, M.; Chalasani, N.; Kwo, P.; Tector, A.J. Portal Vein Thrombosis Is a Risk Factor for Poor Early Outcomes After Liver Transplantation: Analysis of Risk Factors and Outcomes for Portal Vein Thrombosis in Waitlisted Patients. Transplantation 2016, 100, 126–133. [Google Scholar] [CrossRef]
- Englesbe, M.J.; Kubus, J.; Muhammad, W.; Sonnenday, C.J.; Welling, T.; Punch, J.D.; Lynch, R.J.; Marrero, J.A.; Pelletier, S.J. Portal vein thrombosis and survival in patients with cirrhosis. Liver Transplant. 2010, 16, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Francoz, C.; Belghiti, J.; Vilgrain, V.; Sommacale, D.; Paradis, V.; Condat, B.; Denninger, M.H.; Sauvanet, A.; Valla, D.; Durand, F. Splanchnic vein thrombosis in candidates for liver transplantation: Usefulness of screening and anticoagulation. Gut 2005, 54, 691–697. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Castro, K.I.; Porte, R.J.; Nadal, E.; Germani, G.; Burra, P.; Senzolo, M. Management of nonneoplastic portal vein thrombosis in the setting of liver transplantation: A systematic review. Transplantation 2012, 94, 1145–1153. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Liu, L.; Qi, X.; He, C.; Wu, F.; Fan, D.; Han, G. Efficacy and safety of anticoagulation in more advanced portal vein thrombosis in patients with liver cirrhosis. Eur. J. Gastroenterol. Hepatol. 2016, 28, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Loffredo, L.; Pastori, D.; Farcomeni, A.; Violi, F. Effects of Anticoagulants in Patients with Cirrhosis and Portal Vein Thrombosis: A Systematic Review and Meta-analysis. Gastroenterology 2017, 153, 480–487.e1. [Google Scholar] [CrossRef]
- Francoz, C.; Valla, D.; Durand, F. Portal vein thrombosis, cirrhosis, and liver transplantation. J. Hepatol. 2012, 57, 203–212. [Google Scholar] [CrossRef]
- Driever, E.G.; von Meijenfeldt, F.A.; Adelmeijer, J.; de Haas, R.J.; van den Heuvel, M.C.; Nagasami, C.; Weisel, J.W.; Fondevila, C.; Porte, R.J.; Blasi, A.; et al. Nonmalignant portal vein thrombi in patients with cirrhosis consist of intimal fibrosis with or without a fibrin-rich thrombus. Hepatology 2022, 75, 898–911. [Google Scholar] [CrossRef]
- Bach, A.M.; Hann, L.E.; Brown, K.T.; Getrajdman, G.I.; Herman, S.K.; Fong, Y.; Blumgart, L.H. Portal vein evaluation with US: Comparison to angiography combined with CT arterial portography. Radiology 1996, 201, 149–154. [Google Scholar] [CrossRef]
- Brunaud, L.; Antunes, L.; Collinet-Adler, S.; Marchal, F.; Ayav, A.; Bresler, L.; Boissel, P. Acute mesenteric venous thrombosis: Case for nonoperative management. J. Vasc. Surg. 2001, 34, 673–679. [Google Scholar] [CrossRef]
- Lee, H.K.; Park, S.J.; Yi, B.H.; Yeon, E.K.; Kim, J.H.; Hong, H.S. Portal vein thrombosis: CT features. Abdom. Imaging 2008, 33, 72–79. [Google Scholar] [CrossRef]
- Lai, L.; Brugge, W.R. Endoscopic ultrasound is a sensitive and specific test to diagnose portal venous system thrombosis (PVST). Am. J. Gastroenterol. 2004, 99, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Calvet, X.; Bruix, J.; Brú, C.; Ginés, P.; Vilana, R.; Solé, M.; Ayuso, M.D.C.; Bruguera, M.; Rodes, J. Natural history of hepatocellular carcinoma in Spain. Five year’s experience in 249 cases. J. Hepatol. 1990, 10, 311–317. [Google Scholar] [CrossRef]
- Stuart, K.E.; Anand, A.J.; Jenkins, R.L. Hepatocellular carcinoma in the United States. Prognostic features, treatment outcome, and survival. Cancer 1996, 77, 2217–2222. [Google Scholar] [CrossRef]
- Tublin, M.E.; Dodd, G.D.; 3rd Baron, R.L. Benign and malignant portal vein thrombosis: Differentiation by CT characteristics. AJR Am. J. Roentgenol. 1997, 168, 719–723. [Google Scholar] [CrossRef]
- Sandrasegaran, K.; Tahir, B.; Nutakki, K.; Akisik, F.M.; Bodanapally, U.; Tann, M.; Chalasani, N. Usefulness of conventional MRI sequences and diffusion-weighted imaging in differentiating malignant from benign portal vein thrombus in cirrhotic patients. AJR Am. J. Roentgenol. 2013, 201, 1211–1219. [Google Scholar] [CrossRef]
- Sherman, C.B.; Behr, S.; Dodge, J.L.; Roberts, J.P.; Yao, F.Y.; Mehta, N. Distinguishing Tumor from Bland Portal Vein Thrombus in Liver Transplant Candidates with Hepatocellular Carcinoma: The A-VENA Criteria. Liver Transplant. 2019, 25, 207–216. [Google Scholar] [CrossRef]
- Fortea, J.I.; Zipprich, A.; Fernandez-Mena, C.; Puerto, M.; Bosoi, C.R.; Almagro, J.; Hollenbach, M.; Bañares, J.; Rodríguez-Sánchez, B.; Cercenado, E.; et al. Enoxaparin does not ameliorate liver fibrosis or portal hypertension in rats with advanced cirrhosis. Liver Int. 2018, 38, 102–112. [Google Scholar] [CrossRef]
- Amitrano, L.; Guardascione, M.A.; Menchise, A.; Martino, R.; Scaglione, M.; Giovine, S.; Romano, L.; Balzano, A. Safety and efficacy of anticoagulation therapy with low molecular weight heparin for portal vein thrombosis in patients with liver cirrhosis. J. Clin. Gastroenterol. 2010, 44, 448–451. [Google Scholar] [CrossRef]
- Delgado, M.G.; Seijo, S.; Yepes, I.; Achecar, L.; Catalina, M.V.; Garcia-Criado, A.; Abraldes, J.G.; de la Peña, J.; Bañares, R.; Albillos, A.; et al. Efficacy and safety of anticoagulation on patients with cirrhosis and portal vein thrombosis. Clin. Gastroenterol. Hepatol. 2012, 10, 776–783. [Google Scholar] [CrossRef]
- Chung, J.W.; Kim, G.H.; Lee, J.H.; Ok, K.S.; Jang, E.S.; Jeong, S.H.; Kim, J.W. Safety, efficacy, and response predictors of anticoagulation for the treatment of nonmalignant portal-vein thrombosis in patients with cirrhosis: A propensity score matching analysis. Clin. Mol. Hepatol. 2014, 20, 384–391. [Google Scholar] [CrossRef]
- Cui, S.B.; Shu, R.H.; Yan, S.P.; Wu, H.; Chen, Y.; Wang, L.; Zhu, Q. Efficacy and safety of anticoagulation therapy with different doses of enoxaparin for portal vein thrombosis in cirrhotic patients with hepatitis B. Eur. J. Gastroenterol. Hepatol. 2015, 27, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Naeshiro, N.; Aikata, H.; Hyogo, H.; Kan, H.; Fujino, H.; Kobayashi, T.; Fukuhara, T.; Honda, Y.; Nakahara, T.; Ohno, A.; et al. Efficacy and safety of the anticoagulant drug, danaparoid sodium, in the treatment of portal vein thrombosis in patients with liver cirrhosis. Hepatol. Res. 2015, 45, 656–662. [Google Scholar] [CrossRef] [PubMed]
- Noronha Ferreira, C.; Reis, D.; Cortez-Pinto, H.; Tato Marinho, R.; Goncalves, A.; Palma, S.; Leite, I.; Rodrigues, T.; Pedro, A.J.; Alexandrino, P.; et al. Anticoagulation in Cirrhosis and Portal Vein Thrombosis Is Safe and Improves Prognosis in Advanced Cirrhosis. Dig. Dis. Sci. 2019, 64, 2671–2683. [Google Scholar] [CrossRef] [PubMed]
- Pettinari, I.; Vukotic, R.; Stefanescu, H.; Pecorelli, A.; Morelli, M.; Grigoras, C.; Sparchez, Z.; Andreone, P.; Piscaglia, F.; BO-LIVES; et al. Clinical Impact and Safety of Anticoagulants for Portal Vein Thrombosis in Cirrhosis. Am. J. Gastroenterol. 2019, 114, 258–266. [Google Scholar] [CrossRef] [PubMed]
- Bergere, M.; Erard-Poinsot, D.; Boillot, O.; Valette, P.J.; Guillaud, O.; Chambon-Augoyard, C.; Dumortier, J. Portal vein thrombosis and liver cirrhosis: Long-term anticoagulation is effective and safe. Clin. Res. Hepatol. Gastroenterol. 2019, 43, 395–402. [Google Scholar] [CrossRef] [PubMed]
- La Mura, V.; Braham, S.; Tosetti, G.; Branchi, F.; Bitto, N.; Moia, M.; Fracanzani, A.L.; Colombo, M.; Tripodi, A.; Primignani, M.; et al. Harmful and Beneficial Effects of Anticoagulants in Patients With Cirrhosis and Portal Vein Thrombosis. Clin. Gastroenterol. Hepatol. 2018, 16, 1146–1152.e1144. [Google Scholar] [CrossRef] [PubMed]
- Qi, X.; De Stefano, V.; Li, H.; Dai, J.; Guo, X.; Fan, D. Anticoagulation for the treatment of portal vein thrombosis in liver cirrhosis: A systematic review and meta-analysis of observational studies. Eur. J. Intern. Med. 2015, 26, 23–29. [Google Scholar] [CrossRef]
- Ghazaleh, S.; Beran, A.; Aburayyan, K.; Nehme, C.; Patel, D.; Khader, Y.; Sharma, S.; Aziz, M.; Abdel-Aziz, Y.; Hammad, T.; et al. Efficacy and safety of anticoagulation in non-malignant portal vein thrombosis in patients with liver cirrhosis: A systematic review and meta-analysis. Ann. Gastroenterol. 2021, 34, 104–110. [Google Scholar] [CrossRef]
- Wang, L.; Guo, X.; Xu, X.; De Stefano, V.; Plessier, A.; Noronha Ferreira, C.; Qi, X. Anticoagulation Favors Thrombus Recanalization and Survival in Patients with Liver Cirrhosis and Portal Vein Thrombosis: Results of a Meta-Analysis. Adv. Ther. 2021, 38, 495–520. [Google Scholar] [CrossRef]
- Rodriguez-Castro, K.I.; Vitale, A.; Fadin, M.; Shalaby, S.; Zerbinati, P.; Sartori, M.T.; Landi, S.; Pettinari, I.; Piscaglia, F.; Han, G.; et al. A prediction model for successful anticoagulation in cirrhotic portal vein thrombosis. Eur. J. Gastroenterol. Hepatol. 2019, 31, 34–42. [Google Scholar] [CrossRef]
- Nicoară-Farcău, O.; Soy, G.; Magaz, M.; Baiges, A.; Turon, F.; Garcia-Criado, A.; Barrufet, M.; Burrel, M.; Hernández-Gea, V.; García-Pagán, J.C. New Insights into the Pathogenesis, Risk Factors, and Treatment of Portal Vein Thrombosis in Patients with Cirrhosis. Semin. Thromb. Hemost. 2020, 46, 673–681. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Castro, K.I.; Senzolo, M.; Sartori, M.T. Optimal length of anticoagulant therapy in cirrhotic patients with portal vein thrombosis. Clin. Gastroenterol. Hepatol. 2012, 10, 820–821. [Google Scholar] [CrossRef] [PubMed]
- Guerrero, A.; Campo, L.; Piscaglia, F.; Reiberger, T.; Han, G.; Violi, F.E.A. Anticoagulation improves overall survival through portal vein recanalization in patients with cirrhosis and portal vein thrombosis: Individual patient data meta-analysis (IMPORTAL study). J. Hepatol. 2021, 75, S201–S293. [Google Scholar]
- Cerini, F.; Gonzalez, J.M.; Torres, F.; Puente, A.; Casas, M.; Vinaixa, C.; Berenguer, M.; Ardevol, A.; Augustin, S.; Llop, E.; et al. Impact of anticoagulation on upper-gastrointestinal bleeding in cirrhosis. A retrospective multicenter study. Hepatology 2015, 62, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Bechmann, L.P.; Sichau, M.; Wichert, M.; Gerken, G.; Kröger, K.; Hilgard, P. Low-molecular-weight heparin in patients with advanced cirrhosis. Liver Int. 2011, 31, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Senzolo, M.; Rodriguez-Castro, K.I.; Rossetto, V.; Radu, C.; Gavasso, S.; Carraro, P.; Zerbinati, P.; Sartori, M.T.; Simioni, P. Increased anticoagulant response to low-molecular-weight heparin in plasma from patients with advanced cirrhosis. J. Thromb. Haemost. 2012, 10, 1823–1829. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, M.; Tan, L.; Pan, N.; Zhang, L. The clinical use of Fondaparinux: A synthetic heparin pentasaccharide. Prog. Mol. Biol. Transl. Sci. 2019, 163, 41–53. [Google Scholar]
- Lobo, B.; Finch, C.; Howard, A.; Minhas, S. Fondaparinux for the treatment of patients with acute heparin-induced thrombocytopenia. Thromb. Haemost. 2008, 99, 208–214. [Google Scholar]
- Senzolo, M.; Piano, S.; Shalaby, S.; Tonon, M.; Tonello, S.; Zanetto, A.; Sacerdoti, D.; Simioni, P.; Bombonato, G.; Burra, P.; et al. Comparison of Fondaparinux and Low-Molecular-Weight Heparin in the Treatment of Portal Vein Thrombosis in Cirrhosis. Am. J. Med. 2021, 134, 1278–1285.e2. [Google Scholar] [CrossRef]
- Biolato, M.; Paratore, M.; Di Gialleonardo, L.; Marrone, G.; Grieco, A. Direct oral anticoagulant administration in cirrhotic patients with portal vein thrombosis: What is the evidence? World J. Hepatol. 2022, 14, 682–695. [Google Scholar] [CrossRef]
- Potze, W.; Arshad, F.; Adelmeijer, J.; Blokzijl, H.; van den Berg, A.P.; Meijers, J.C.; Porte, R.J.; Lisman, T. Differential in vitro inhibition of thrombin generation by anticoagulant drugs in plasma from patients with cirrhosis. PLoS ONE 2014, 9, e88390. [Google Scholar] [CrossRef] [PubMed]
- Potze, W.; Adelmeijer, J.; Lisman, T. Decreased in vitro anticoagulant potency of Rivaroxaban and Apixaban in plasma from patients with cirrhosis. Hepatology 2015, 61, 1435–1436. [Google Scholar] [CrossRef] [PubMed]
- Serper, M.; Weinberg, E.M.; Cohen, J.B.; Reese, P.P.; Taddei, T.H.; Kaplan, D.E. Mortality and Hepatic Decompensation in Patients with Cirrhosis and Atrial Fibrillation Treated with Anticoagulation. Hepatology 2021, 73, 219–232. [Google Scholar] [CrossRef] [PubMed]
- De Gottardi, A.; Trebicka, J.; Klinger, C.; Plessier, A.; Seijo, S.; Terziroli, B.; Magenta, L.; Semela, D.; Buscarini, E.; Langlet, P.; et al. Antithrombotic treatment with direct-acting oral anticoagulants in patients with splanchnic vein thrombosis and cirrhosis. Liver Int. 2017, 37, 694–699. [Google Scholar] [CrossRef]
- Intagliata, N.M.; Henry, Z.H.; Maitland, H.; Shah, N.L.; Argo, C.K.; Northup, P.G.; Caldwell, S.H. Direct Oral Anticoagulants in Cirrhosis Patients Pose Similar Risks of Bleeding When Compared to Traditional Anticoagulation. Dig. Dis. Sci. 2016, 61, 1721–1727. [Google Scholar] [CrossRef]
- Hum, J.; Shatzel, J.J.; Jou, J.H.; Deloughery, T.G. The efficacy and safety of direct oral anticoagulants vs traditional anticoagulants in cirrhosis. Eur. J. Haematol. 2017, 98, 393–397. [Google Scholar] [CrossRef]
- Semmler, G.; Pomej, K.; Bauer, D.J.M.; Balcar, L.; Simbrunner, B.; Binter, T.; Hartl, L.; Becker, J.; Pinter, M.; Quehenberger, P.; et al. Safety of direct oral anticoagulants in patients with advanced liver disease. Liver Int. 2021, 41, 2159–2170. [Google Scholar] [CrossRef]
- Nisly, S.A.; Mihm, A.E.; Gillette, C.; Davis, K.A.; Tillett, J. Safety of direct oral anticoagulants in patients with mild to moderate cirrhosis: A systematic review and meta-analysis. J. Thromb. Thrombolysis 2021, 52, 817–827. [Google Scholar] [CrossRef]
- Menichelli, D.; Ronca, V.; Di Rocco, A.; Pignatelli, P.; Marco Podda, G. Direct oral anticoagulants and advanced liver disease: A systematic review and meta-analysis. Eur. J. Clin. Investig. 2021, 51, e13397. [Google Scholar] [CrossRef]
- Hanafy, A.S.; Abd-Elsalam, S.; Dawoud, M.M. Randomized controlled trial of rivaroxaban versus warfarin in the management of acute non-neoplastic portal vein thrombosis. Vasc. Pharmacol. 2019, 113, 86–91. [Google Scholar] [CrossRef]
- Nagaoki, Y.; Aikata, H.; Daijyo, K.; Teraoka, Y.; Shinohara, F.; Nakamura, Y.; Hatooka, M.; Morio, K.; Nakahara, T.; Kawaoka, T.; et al. Efficacy and safety of edoxaban for treatment of portal vein thrombosis following danaparoid sodium in patients with liver cirrhosis. Hepatol. Res. 2018, 48, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Ai, M.H.; Dong, W.G.; Tan, X.P.; Xu, L.; Xu, C.; Zhang, Q.; Zhang, Y.; Li, J. Efficacy and safety study of direct-acting oral anticoagulants for the treatment of chronic portal vein thrombosis in patients with liver cirrhosis. Eur. J. Gastroenterol. Hepatol. 2020, 32, 1395–1400. [Google Scholar] [PubMed]
- Radosevich, P.M.; Ring, E.J.; LaBerge, J.M.; Peltzer, M.Y.; Haskal, Z.J.; Doherty, M.M.; Gordon, R.L. Transjugular intrahepatic portosystemic shunts in patients with portal vein occlusion. Radiology 1993, 186, 523–527. [Google Scholar] [CrossRef] [PubMed]
- Walser, E.M.; NcNees, S.W.; DeLa Pena, O.; Crow, W.N.; Morgan, R.A.; Soloway, R.; Broughan, T. Portal venous thrombosis: Percutaneous therapy and outcome. J. Vasc. Interv. Radiol. 1998, 9, 119–127. [Google Scholar] [CrossRef]
- Stein, M.; Link, D.P. Symptomatic spleno-mesenteric-portal venous thrombosis: Recanalization and reconstruction with endovascular stents. J. Vasc. Interv. Radiol. 1999, 10, 363–371. [Google Scholar] [CrossRef]
- Rodrigues, S.G.; Sixt, S.; Abraldes, J.G.; De Gottardi, A.; Klinger, C.; Bosch, J.; Baumgartner, I.; Berzigotti, A. Systematic review with meta-analysis: Portal vein recanalisation and transjugular intrahepatic portosystemic shunt for portal vein thrombosis. Aliment Pharmacol. Ther. 2019, 49, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Valentin, N.; Korrapati, P.; Constantino, J.; Young, A.; Weisberg, I. The role of transjugular intrahepatic portosystemic shunt in the management of portal vein thrombosis: A systematic review and meta-analysis. Eur. J. Gastroenterol. Hepatol. 2018, 30, 1187–1193. [Google Scholar] [CrossRef]
- Lv, Y.; Bai, W.; Li, K.; Wang, Z.; Guo, W.; Luo, B.; Wang, J.; Wang, Q.; Wang, E.; Xia, D.; et al. Anticoagulation and Transjugular Intrahepatic Portosystemic Shunt for the Management of Portal Vein Thrombosis in Cirrhosis: A Prospective Observational Study. Am. J. Gastroenterol. 2021, 116, 1447–1464. [Google Scholar] [CrossRef]
- Zhan, C.; Prabhu, V.; Kang, S.K.; Li, C.; Zhu, Y.; Kim, S.; Olsen, S.; Jacobson, I.M.; Dagher, N.N.; Carney, B.; et al. Comparison of Non-Tumoral Portal Vein Thrombosis Management in Cirrhotic Patients: TIPS Versus Anticoagulation Versus No Treatment. J. Clin. Med. 2021, 10, 2316. [Google Scholar] [CrossRef]
- Lv, Y.; Qi, X.; He, C.; Wang, Z.; Yin, Z.; Niu, J.; Guo, W.; Bai, W.; Zhang, H.; Xie, H.; et al. Covered TIPS versus endoscopic band ligation plus propranolol for the prevention of variceal rebleeding in cirrhotic patients with portal vein thrombosis: A randomised controlled trial. Gut 2018, 67, 2156–2168. [Google Scholar] [CrossRef]
- Luo, X.; Wang, Z.; Tsauo, J.; Zhou, B.; Zhang, H.; Li, X. Advanced Cirrhosis Combined with Portal Vein Thrombosis: A Randomized Trial of TIPS versus Endoscopic Band Ligation Plus Propranolol for the Prevention of Recurrent Esophageal Variceal Bleeding. Radiology 2015, 276, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Jiang, M.S.; Zhang, H.L.; Weng, N.N.; Luo, X.F.; Li, X.; Yang, L. Is Post-TIPS Anticoagulation Therapy Necessary in Patients with Cirrhosis and Portal Vein Thrombosis? A Randomized Controlled Trial. Radiology 2016, 279, 943–951. [Google Scholar] [CrossRef] [PubMed]
- Han, G.; Qi, X.; He, C.; Yin, Z.; Wang, J.; Xia, J.; Yang, Z.; Bai, M.; Meng, X.; Niu, J.; et al. Transjugular intrahepatic portosystemic shunt for portal vein thrombosis with symptomatic portal hypertension in liver cirrhosis. J. Hepatol. 2011, 54, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Habib, A.; Desai, K.; Hickey, R.; Thornburg, B.; Vouche, M.; Vogelzang, R.L.; Salem, R. Portal vein recanalization-transjugularintrahepatic portosystemic shunt using the transsplenic approach to achieve transplant candidacy in patients with chronic portal vein thrombosis. J. Vasc. Interv. Radiol. 2015, 26, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Thornburg, B.; Desai, K.; Hickey, R.; Hohlastos, E.; Kulik, L.; Ganger, D.; Baker, T.; Abecassis, M.; Caicedo, J.C.; Ladner, D.; et al. Pretransplantation Portal Vein Recanalization and Transjugular Intrahepatic Portosystemic Shunt Creation for Chronic Portal Vein Thrombosis: Final Analysis of a 61-Patient Cohort. J. Vasc. Interv. Radiol. 2017, 28, 1714–1721.e2. [Google Scholar] [CrossRef]
- Salem, R.; Vouche, M.; Baker, T.; Herrero, J.I.; Caicedo, J.C.; Fryer, J.; Hickey, R.; Habib, A.; Abecassis, M.; Koller, F.; et al. Pretransplant Portal Vein Recanalization-Transjugular Intrahepatic Portosystemic Shunt in Patients with Complete Obliterative Portal Vein Thrombosis. Transplantation 2015, 99, 2347–2355. [Google Scholar] [CrossRef]
- Thornburg, B.; Desai, K.; Hickey, R.; Kulik, L.; Ganger, D.; Baker, T.; Abecassis, M.; Lewandowski, R.J.; Salem, R. Portal Vein Recanalization and Transjugular Intrahepatic Portosystemic Shunt Creation for Chronic Portal Vein Thrombosis: Technical Considerations. Tech. Vasc. Interv. Radiol. 2016, 19, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Boike, J.R.; Thornburg, B.G.; Asrani, S.K.; Fallon, M.B.; Fortune, B.E.; Izzy, M.J.; Verna, E.C.; Abraldes, J.G.; Allegretti, A.S.; Bajaj, J.S.; et al. North American Practice-Based Recommendations for Transjugular Intrahepatic Portosystemic Shunts in Portal Hypertension. Clin. Gastroenterol. Hepatol. 2022, 20, 1636–1662.e1636. [Google Scholar] [CrossRef]
- Hollingshead, M.; Burke, C.T.; Mauro, M.A.; Weeks, S.M.; Dixon, R.G.; Jaques, P.F. Transcatheter thrombolytic therapy for acute mesenteric and portal vein thrombosis. J. Vasc. Interv. Radiol. 2005, 16, 651–661. [Google Scholar] [CrossRef]
- Liu, K.; Li, W.D.; Du, X.L.; Li, C.L.; Li, X.Q. Comparison of Systemic Thrombolysis Versus Indirect Thrombolysis via the Superior Mesenteric Artery in Patients with Acute Portal Vein Thrombosis. Ann. Vasc. Surg. 2017, 39, 264–269. [Google Scholar] [CrossRef]
- Smalberg, J.H.; Spaander, M.V.; Jie, K.S.; Pattynama, P.M.; van Buuren, H.R.; van den Berg, B.; Janssen, H.L.A.; Leebeek, F.W.G. Risks and benefits of transcatheter thrombolytic therapy in patients with splanchnic venous thrombosis. Thromb. Haemost. 2008, 100, 1084–1088. [Google Scholar] [CrossRef] [PubMed]
- Bianchini, M.; Cavani, G.; Bonaccorso, A.; Turco, L.; Vizzutti, F.; Sartini, A.; Gitto, S.; Merighi, A.; Banchelli, F.; Villa, E.; et al. Low molecular weight heparin does not increase bleeding and mortality post-endoscopic variceal band ligation in cirrhotic patients. Liver Int. 2018, 38, 1253–1262. [Google Scholar] [CrossRef] [PubMed]
- Guillaume, M.; Christol, C.; Plessier, A.; Corbic, M.; Péron, J.-M.; Sommet, A.; Rautou, P.-E.; Consigny, Y.; Vinel, J.-P.; Valla, C.-D.; et al. Bleeding risk of variceal band ligation in extrahepatic portal vein obstruction is not increased by oral anticoagulation. Eur. J. Gastroenterol. Hepatol. 2018, 30, 563–568. [Google Scholar] [CrossRef] [PubMed]
- Montalvá, E.; Rodríguez-Perálvarez, M.; Blasi, A.; Bonanad, S.; Gavín, O.; Hierro, L.; Lladó, L.; Llop, E.; Pozo-Laderas, J.C.; Colmenero, J.; et al. Consensus Statement on Hemostatic Management, Anticoagulation, and Antiplatelet Therapy in Liver Transplantation. Transplantation 2022, 106, 1123–1131. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Classification | Description | Categories | Strengths vs. Weaknesses |
|---|---|---|---|
| Yerdel et al., 2000 [16] | Post-transplant survival (i) Involvement of MPV, SMV and SV (ii) Degree of occlusion | Grade 1: <50% occlusion Grade 2: >50% occlusion Grade 3: Complete PV or SV occlusionGrade 4: Complete PV occlusion with SMV extension |
|
| Bauer et al., 2006 [17] | PVT response to TIPS placement in patients listed for LT (i) Involvement of MPV, SMV and SV (ii) Degree of occlusion (iii) Stratification by location of clot and cavernous transformation | Grade 1: <25% occlusion of PV Grade 2: 26–50% occlusion Grade 3: 51–75% occlusion Grade 4: 76–100% occlusion |
|
| Sarin et al., 2016 [18] | Based on revision of previous PVT classifications (i) Involvement of MPV, SMV, and SV (ii) Degree of occlusion (iii) Underlying liver disease | Site of PVT (Type 1, 2a, 2b, 3) * Type 1: only trunk * Type II: only branches (a: one, b: both branches) * Type 3: trunk and branches Degree of occlusion * Occlusive * Non-occlusive Duration and presentation * Recent or chronic * Symptomatic or asymptomatic Extension * SV, SMV, or both Underlying liver disease |
|
| Bhangui et al., 2019 [19] | (i) Involvement of MPV, SMV and SV (ii) LT surgery choices based on collaterals | Complex
|
|
| Baveno VII 2022 | AASLD 2021 | ACG 2020 | ICLDC 2018 | EASL 2015 | |
|---|---|---|---|---|---|
| Screening for PVT | Listed or potential candidates for LT at the time of HCC screening | - | (i) new diagnosis of cirrhosis (ii) onset of PH (iii) decompensation. | US every 6 months in (i) patients with cirrhosis and PH, or (ii) Listed or potential candidates for LT | Listed or potential candidates for LT |
| Imaging test |
|
|
|
|
|
| Screening for thrombophilia | - | (i) family history of MPN (ii) suggestive laboratory findings | (i) previous thrombosis (ii) thrombosis at unusual sites (iii) family history | “Consider on an individual basis” | “Consider screening” |
| Indications for treatment |
(ii) symptomatic PVT (iii) potential candidates for LT
| (i) Recent (<6 m) completely or partially occlusive of the main PV or SMV (ii) Ischemic symptoms | (i) evidence of thrombophilia, (ii) progression into the mesenteric veins, or (iii) current or previous evidence of bowel ischemia | (i) LT candidates with occlusive main PVT with or without extension to SMV (ii) Yerdel Grade ≥ 2 PVT considered on an individual basis | (i) SMV thrombosis, with a past history suggestive of intestinal ischemia or (ii) liver transplant candidates |
| Medical therapies | Initial agent: preferably LWMH Maintenance:
| LWMH, VKAs or DOACs | Initial agent: UH or LWMH Maintenance: L
| - | - |
| TIPS | (i) PVT of the main PV without recanalization on AC, especially in patients listed for LT | (i) PVT that hinders a physiological anastomosis between the graft and recipient (ii) refractary PH complications | - | (i) acute and chronic PVT in patients with cirrhosis requiring treatment for significant PH | (i) LT candidates not responding to AC |
| Unfractionated Heparin | Low-Weight Molecular Heparin | Vitamin-K Antagonists | Direct Oral Anticoagulants | |
|---|---|---|---|---|
| Administration | Endovenous | Subcutaneous | Oral | Oral |
| Posology | Daily infusion | qd/bid | Qd | Apixaban/dabigatran: bid Edoxaban: qd Rivaroxaban: bd for 3 weeks, qd thereafter |
| Half-life | Minutes to 1–2 h | 4–12 h | 10–24 h | 6–18 h |
| Absorption and bioavailability | Caution if hypoalbuminemia | BA 85–95%, caution if hypoalbuminemia | Affected from bowel edema in PH and diet | Affected from bowel edema in PH |
| Monitoring | antiXa factor or aPTT | Not needed, but caution if GFR < 15 mL/min/m2, obesity, and female sex | PT and INR (2–3) | Not needed, especially if GFR > 15 mL/min/m2, non-obese, and male sex |
| Renal function | Dose change not necessary but monitor with antiXa and aPTT | Contraindicated if severe renal failure or dialysis, caution in mild/moderate renal failure | Contraindicated if severe renal failure or dialysis, caution in mild/moderate renal failure |
|
| Side Effects |
|
| Hemorrhage/hematoma |
|
| Bleeding risk | ++ | ++ | ++ | Apixaban: + Dabigatran/Edoxaban: ++ Rivaroxaban: +++ |
| Antidote | Protamine sulfate | Protamine sulfate * | Vitamin-K | AntiX: andexanet alpha ** Dabigatran: idarucizumab ** |
| Pros in cirrhosis |
|
| Oral administration |
|
| Cons in cirrhosis | Not suitable for maintainance therapy Fluctuating levels of ATIII |
|
| Not recommended in Child C Caution in Child B Higher costs |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Odriozola, A.; Puente, Á.; Cuadrado, A.; Rivas, C.; Anton, Á.; González, F.J.; Pellón, R.; Fábrega, E.; Crespo, J.; Fortea, J.I. Portal Vein Thrombosis in the Setting of Cirrhosis: A Comprehensive Review. J. Clin. Med. 2022, 11, 6435. https://doi.org/10.3390/jcm11216435
Odriozola A, Puente Á, Cuadrado A, Rivas C, Anton Á, González FJ, Pellón R, Fábrega E, Crespo J, Fortea JI. Portal Vein Thrombosis in the Setting of Cirrhosis: A Comprehensive Review. Journal of Clinical Medicine. 2022; 11(21):6435. https://doi.org/10.3390/jcm11216435
Chicago/Turabian StyleOdriozola, Aitor, Ángela Puente, Antonio Cuadrado, Coral Rivas, Ángela Anton, Francisco José González, Raúl Pellón, Emilio Fábrega, Javier Crespo, and José Ignacio Fortea. 2022. "Portal Vein Thrombosis in the Setting of Cirrhosis: A Comprehensive Review" Journal of Clinical Medicine 11, no. 21: 6435. https://doi.org/10.3390/jcm11216435
APA StyleOdriozola, A., Puente, Á., Cuadrado, A., Rivas, C., Anton, Á., González, F. J., Pellón, R., Fábrega, E., Crespo, J., & Fortea, J. I. (2022). Portal Vein Thrombosis in the Setting of Cirrhosis: A Comprehensive Review. Journal of Clinical Medicine, 11(21), 6435. https://doi.org/10.3390/jcm11216435