
Sedentary Behaviour, Physical Activity, and Their Associations with Health Outcomes at the Time of Diagnosis in People with Inoperable Lung Cancer

 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measurement/Assessments
2.3. Sedentary Behaviour and Physical Activity
2.4. Symptoms
2.5. Health-Related Quality of Life
2.6. Muscle Force
2.7. Comorbidities
2.8. Clinical Covariates
2.9. Data Management and Analysis
3. Results
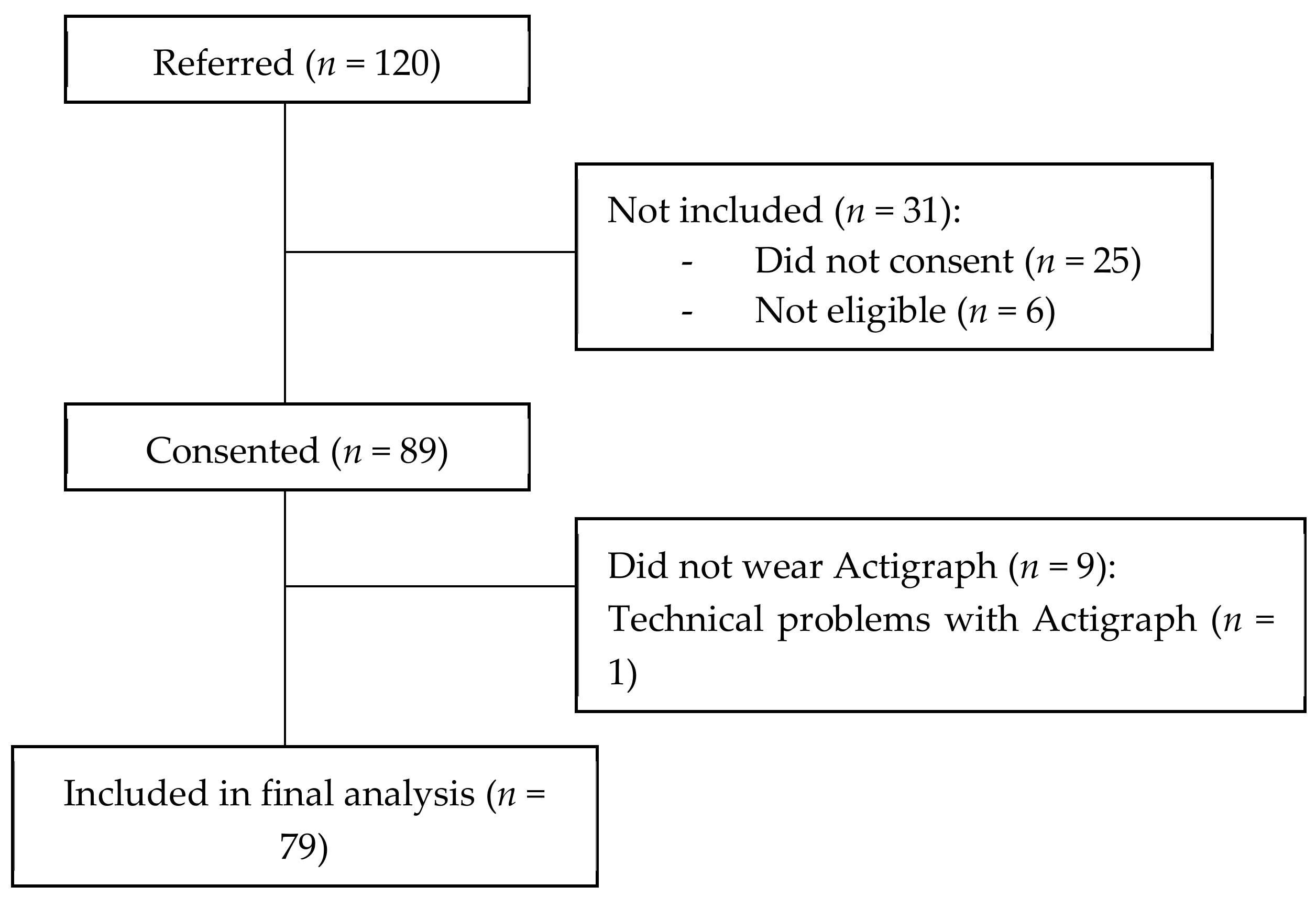
3.1. Participant Characteristics and Compliance with Actigraphy
3.2. Sedentary Behaviour and Physical Activity
3.3. Correlations
3.4. Summary of the Adjusted Regression Models
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cancer in Australia 2019; Australian Institute of Health and Welfare: Canberra, Ausrtalia, 2019.
- Howington, J.A.; Blum, M.G.; Chang, A.C.; Balekian, A.A.; Murthy, S.C. Treatment of stage I and II non-small cell lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013, 143 (Suppl. S5), e278S. [Google Scholar] [CrossRef] [PubMed]
- Cavalheri, V.; Granger, C.L. Exercise training as part of lung cancer therapy. Respirology 2020, 25 (Suppl. S2), 80–87. [Google Scholar] [CrossRef] [PubMed]
- Edbrooke, L.; Granger, C.L.; Clark, R.A.; Denehy, L. Physical activity levels are low in inoperable lung cancer: Exploratory analyses from a randomised controlled trial. J. Clin. Med. 2019, 8, 1288. [Google Scholar] [CrossRef] [PubMed]
- Granger, C.L.; McDonald, C.F.; Irving, L.; Clark, R.A.; Gough, K.; Murnane, A.; Mileshkin, L.; Krishnasamy, M.; Denehy, L. Low physical activity levels and functional decline in individuals with lung cancer. Lung Cancer 2014, 83, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Travers, J.; Dudgeon, D.J.; Amjadi, K.; McBride, I.; Dillon, K.; Laveneziana, P.; Ofir, D.; Webb, K.A.; O’Donnell, D.E. Mechanisms of exertional dyspnea in patients with cancer. J. Appl. Physiol. 2008, 104, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.J.; Yu, D.; White, E.; Lee, D.H.; Blot, W.; Robien, K.; Sinha, R.; Park, Y.; Takata, Y.; Gao, Y.T.; et al. Prediagnosis Leisure-Time Physical Activity and Lung Cancer Survival: A Pooled Analysis of 11 Cohorts. JNCI Cancer Spectr. 2022, 6, pkac009. [Google Scholar] [CrossRef]
- Campbell, K.L.; Winters-Stone, K.M.; Wiskemann, J.; May, A.M.; Schwartz, A.L.; Courneya, K.S.; Zucker, D.S.; Matthews, C.E.; Ligibel, J.A.; Gerber, L.H.; et al. Exercise Guidelines for Cancer Survivors: Consensus Statement from International Multidisciplinary Roundtable. Med. Sci. Sport. Exerc. 2019, 51, 2375–2390. [Google Scholar] [CrossRef]
- Schmitz, K.H.; Courneya, K.S.; Matthews, C.; Demark-Wahnefried, W.; Galvão, D.A.; Pinto, B.M.; Irwin, M.L.; Wolin, K.Y.; Segal, R.J.; Lucia, A.; et al. American college of sports medicine roundtable on exercise guidelines for cancer survivors. Med. Sci. Sport. Exerc. 2010, 42, 1409–1426. [Google Scholar] [CrossRef]
- Hayes, S.C.; Newton, R.U.; Spence, R.R.; Galvao, D.A. The Exercise and Sports Science Australia position statement: Exercise medicine in cancer management. J. Sci. Med. Sport 2019, 22, 1175–1199. [Google Scholar] [CrossRef]
- Caspersen, C.J.; Powell, K.E.; Christenson, G. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar]
- Stout, N.L.; Baima, J.; Swisher, A.K.; Winters-Stone, K.M.; Welsh, J. A Systematic Review of Exercise Systematic Reviews in the Cancer Literature (2005–2017). PM&R 2017, 9, S347–S384. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M. Sedentary Behavior Research Network (SBRN)—Terminology consensus project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [PubMed]
- Montoye, A.H.K.; Pivarnik, J.M.; Mudd, L.M.; Biswas, S.; Pfeiffer, K.A. Validation and comparison of accelerometers worn on the hip, thigh, and wrists for measuring physical activity and sedentary behavior. AIMS Public Health 2016, 3, 298–312. [Google Scholar] [CrossRef] [PubMed]
- Edbrooke, L.; Denehy, L.; Parry, S.M.; Astin, R.; Jack, S.; Granger, C.L. How is physical activity measured in lung cancer? A systematic review of outcome measures and their psychometric properties. Respirology 2017, 22, 263–277. [Google Scholar] [CrossRef] [PubMed]
- D’Silva, A.; Gardiner, P.A.; Boyle, T.; Bebb, D.G.; Johnson, S.T.; Vallance, J.K. Associations of objectively assessed physical activity and sedentary time with health-related quality of life among lung cancer survivors: A quantile regression approach. Lung Cancer 2018, 119, 78–84. [Google Scholar] [CrossRef]
- D’Silva, A.; Bebb, G.; Boyle, T.; Johnson, S.T.; Vallance, J.K. Demographic and clinical correlates of accelerometer assessed physical activity and sedentary time in lung cancer survivors. Psychooncology 2018, 27, 1042–1049. [Google Scholar] [CrossRef]
- Bade, B.C.; Brooks, M.C.; Nietert, S.B.; Ulmer, A.; Thomas, D.D.; Nietert, P.J.; Scott, J.B.; Silvestri, G.A. Assessing the correlation between physical activity and quality of life in advanced lung cancer. Integr. Cancer Ther. 2018, 17, 73–79. [Google Scholar] [CrossRef]
- Fujisawa, D.; Temel, J.S.; Greer, J.A.; El-Jawahri, A.; Traeger, L.; Jacobs, J.M.; Cutrono, S.; Pirl, W.F. Actigraphy as an assessment of performance status in patients with advanced lung cancer. Pall. Supp. Care 2019, 17, 574–578. [Google Scholar] [CrossRef]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef]
- Yellen, S.B.; Cella, D.F.; Webster, K.; Blendowski, C.; Kaplan, E. Measuring fatigue and other anemia-related symptoms with the Functional Assessment of Cancer Therapy (FACT) measurement system. J. Pain Symptom Manag. 1997, 13, 63–74. [Google Scholar] [CrossRef]
- Tinsley, A.; Macklin, E.A.; Korzenik, J.R.; Sands, B.E. Validation of the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) in patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2011, 34, 1328–1336. [Google Scholar] [CrossRef] [PubMed]
- Nordin, Å.; Taft, C.; Lundgren-Nilsson, Å.; Dencker, A. Minimal important differences for fatigue patient reported outcome measures—A systematic review. BMC Med. Res. Methodol. 2016, 16, 62. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, C.M.; Elmes, P.C.; Fairbairn, A.S.; Wood, C.H. Significance of Respiratory Symptoms and the Diagnosis of Chronic Bronchitis in a Working Population. Br. Med. J. 1959, 2, 257–266. [Google Scholar] [CrossRef]
- Celli, B.R.; Cote, C.G.; Marin, J.M.; Casanova, C.; Montes de Oca, M.; Mendez, R.A.; Pinto Plata, V.; Cabral, H.J. The Body-Mass Index, Airflow Obstruction, Dyspnea, and Exercise Capacity Index in Chronic Obstructive Pulmonary Disease. N. Engl. J. Med. 2004, 350, 1005–1012. [Google Scholar] [CrossRef] [PubMed]
- Bestall, J.C.; Paul, E.A.; Garrod, R.; Garnham, R.; Jones, P.W.; Wedzicha, J.A. Usefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax 1999, 54, 581–586. [Google Scholar] [CrossRef]
- De Torres, J.P.; Pinto-Plata, V.; Ingenito, E.; Bagley, P.; Gray, A.; Berger, R.; Celli, B. Power of outcome measurements to detect clinically significant changes in pulmonary rehabilitation of patients with COPD. Chest 2002, 121, 1092–1098. [Google Scholar] [CrossRef]
- Ware, J.E.; Sherbourne, C.D. The MOS 36-Item Short-Form Health Survey (SF-36): I. Conceptual Framework and Item Selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- McHorney, C.A.; Ware, J.E.; Lu, R.J.F.; Sherbourne, C.D. The MOS 36-Item Short-Form Health Survey (SF-36): III. Tests of data quality, scaling assumptions, and reliability across diverse patient groups. Med. Care 1994, 32, 40–66. [Google Scholar] [CrossRef]
- Anita, L.S.; Ron, D.H.; John, E.W. The MOS short-form general health survey: Reliability and validity in a patient population. Med. Care 1988, 26, 724–735. [Google Scholar] [CrossRef]
- Prieto, L.; Alonso, J.; Ferrer, M.; Antó, J.M. Are results of the SF-36 health survey and the nottingham health profile similar? A comparison in COPD patients. J. Clin. Epidemiol. 1997, 50, 463–473. [Google Scholar] [CrossRef]
- Samsa, G.; Edelman, D.; Rothman, M.L.; Williams, G.R.; Lipscomb, J.; Matchar, D. Determining clinically important differences in health status measures: A general approach with illustration to the health utilities index mark II. Pharmacoeconomics 1999, 15, 141–155. [Google Scholar] [CrossRef] [PubMed]
- Cella, D.F.; Bonomi, A.E.; Lloyd, S.R.; Tulsky, D.S.; Kaplan, E.; Bonomi, P. Reliability and validity of the Functional Assessment of Cancer Therapy—Lung (FACT-L) quality of life instrument. Lung Cancer 1995, 12, 199–220. [Google Scholar] [CrossRef]
- Butt, Z.; Webster, K.; Eisenstein, A.R.; Beaumont, J.; Eton, D.; Beaumont, G.A.; Cella, D. Quality of life in lung cancer: The validity and cross-cultural applicability of the Functional Assessment of Cancer Therapy-Lung scale. Hematol. Oncol. 2005, 19, 389–420. [Google Scholar] [CrossRef] [PubMed]
- Cella, D.; Eton, D.T.; Fairclough, D.L.; Bonomi, P.; Heyes, A.E.; Silberman, C.; Wolf, M.K.; Johnson, D.H. What is a clinically meaningful change on the Functional Assessment of Cancer Therapy–Lung (FACT-L) questionnaire?: Results from Eastern Cooperative Oncology Group (ECOG) Study 5592. J. Clin. Epidemiol. 2002, 55, 285–295. [Google Scholar] [CrossRef]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C.; et al. The European organization for research and treatment of cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef]
- Spruit, M.A.; Sillen, M.J.H.; Groenen, M.T.J.; Wouters, E.F.M.; Franssen, F.M.E. New normative values for handgrip strength: Results from the UK Biobank. J. Am. Med. Dir. Assoc. 2013, 14, 775.e5–775.e11. [Google Scholar] [CrossRef]
- Sangha, O.; Stucki, G.; Liang, M.H.; Fossel, A.H.; Katz, J.N. The self-administered comorbidity questionnaire: A new method to assess comorbidity for clinical and health services research. Arthritis Care Res. 2003, 49, 156–163. [Google Scholar] [CrossRef]
- Matthew, C.E. Calibration of accelerometer output for adults. Med. Sci. Sport. Exerc. 2005, 37, S512–S522. [Google Scholar] [CrossRef]
- Freedson, P.S.; Melanson, E.; Sirard, J. Calibration of the computer science and applications, Inc. accelerometer. Med. Sci. Sport. Exerc. 1998, 30, 777–781. [Google Scholar] [CrossRef]
- Chastin, S.F.M.; Granat, M.H. Methods for objective measure, quantification and analysis of sedentary behaviour and inactivity. Gait Posture 2009, 31, 82–86. [Google Scholar] [CrossRef]
- Demeyer, H.; Burtin, C.; Hornikx, M.; Camillo, C.A.; Van Remoortel, H.; Langer, D.; Janssens, W.; Troosters, T. The Minimal Important Difference in Physical Activity in Patients with COPD. PLoS ONE 2016, 11, e0154587. [Google Scholar] [CrossRef] [PubMed]
- Cavalheri, V.; Jenkins, S.; Cecins, N.; Phillips, M.; Sanders, L.H.; Hill, K. Patterns of sedentary behaviour and physical activity in people following curative intent treatment for non-small cell lung cancer. Chron. Respir. Dis. 2016, 13, 82–85. [Google Scholar] [CrossRef]
- Langer, D.; Gosselink, R.; Sena, R.; Burtin, C.; Decramer, M.; Troosters, T. Validation of two activity monitors in patients with COPD. Thorax 2009, 64, 641–642. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Gaskin, C.J.; Craike, M.; Mohebbi, M.; Salmon, J.; Courneya, K.S.; Broadbent, S.; Livingston, P.M. Associations of objectively measured moderate-to-vigorous physical activity and sedentary behavior with quality of life and psychological well-being in prostate cancer survivors. Cancer Causes Control 2016, 27, 1093–1103. [Google Scholar] [CrossRef]
- Boyle, T.; Vallance, J.K.; Ransom, E.K.; Lynch, B.M. How sedentary and physically active are breast cancer survivors, and which population subgroups have higher or lower levels of these behaviors? Support. Care Cancer 2016, 24, 2181–2190. [Google Scholar] [CrossRef]
- Phillips, S.M.; Awick, E.A.; Conroy, D.E.; Pellegrini, C.A.; Mailey, E.L.; McAuley, E. Objectively measured physical activity and sedentary behavior and quality of life indicators in survivors of breast cancer. Cancer 2015, 121, 4044–4052. [Google Scholar] [CrossRef] [PubMed]
- Vallance, J.K.; Boyle, T.; Courneya, K.S.; Lynch, B.M. Associations of objectively assessed physical activity and sedentary time with health-related quality of life among colon cancer survivors. Cancer 2014, 120, 2919–2926. [Google Scholar] [CrossRef] [PubMed]
- Boyle, T.; Lynch, B.M.; Ransom, E.K.; Vallance, J.K. Volume and correlates of objectively measured physical activity and sedentary time in non-Hodgkin lymphoma survivors. Psychooncology 2017, 26, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Hassapidou, M.; Papadopoulou, S.K.; Vlahavas, G.; Kapantais, E.; Kaklamanou, D.; Pagkalos, I.; Kaklamanou, M.; Tzotzas, T. Association of physical activity and sedentary lifestyle patterns with obesity and cardiometabolic comorbidities in Greek adults: Data from the national epidemiological survey. Hormones 2013, 12, 265–274. [Google Scholar] [CrossRef]
- Warren, T.Y.; Barry, V.; Hooker, S.P.; Sui, X.; Church, T.S.; Blair, S.N. Sedentary behaviors increase risk of cardiovascular disease mortality in men. Med. Sci. Sport. Exerc. 2010, 42, 879–885. [Google Scholar] [CrossRef]
- Hu, F.B.; Li, T.Y.; Colditz, G.A.; Willett, W.C.; Manson, J.E. Television watching and other sedentary behaviors in relation to risk of obesity and type 2 diabetes mellitus in women. JAMA 2003, 289, 1785–1791. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.W.; Lee, E.Y.; An, K.Y.; Min, J.; Jeon, J.Y.; Courneya, K.S. Associations between physical activity and comorbidities in Korean cancer survivors. J. Cancer Surviv. 2018, 12, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Vardar-Yagli, N.; Sener, G.; Saglam, M.; Calik-Kutukcu, E.; Arikan, H.; Inal-Ince, D.; Savci, S.; Altundag, K.; Kutluk, T.; Ozisik, Y.; et al. Associations among physical activity, comorbidity, functional capacity, peripheral muscle strength and depression in breast cancer survivors. Asian Pac. J. Cancer Prev. 2015, 16, 585–589. [Google Scholar] [CrossRef] [PubMed]
- Castillo, S.S.; Smith, L.; Suárez, A.D.; Sánchez, G.F.L. Associations between physical activity and comorbidities in people with COPD residing in Spain: A cross-sectional analysis. Int. J. Environ. Res. Public Health 2020, 17, 594. [Google Scholar] [CrossRef]
- Dhillon, H.M.; Bell, M.L.; van der Ploeg, H.P.; Turner, J.D.; Kabourakis, M.; Spencer, L.; Lewis, C.; Hui, R.; Blinman, P.; Clarke, S.J.; et al. Impact of physical activity on fatigue and quality of life in people with advanced lung cancer: A randomized controlled trial. Ann. Oncol. 2017, 28, 1889–1897. [Google Scholar] [CrossRef]
- Valkenet, K.; Veenhof, C. Validity of three accelerometers to investigate lying, sitting, standing and walking. PLoS ONE 2019, 14, e0217545. [Google Scholar] [CrossRef]


{kind=link}
| Variable | n | Value 1 |
|---|---|---|
| Age, year | 79 | 70.5 ± 11.1 |
| Sex, female (%)/male (%) | 79 | 29 (37%)/50 (63%) |
| BMI, kg·m−2 | 79 | 25.1 [22.0 to 30.5] |
| Employment status, n (%) | 79 | |
| Disability | 8 (10%) | |
| Retired | 46 (58%) | |
| Part time | 7 (9%) | |
| Full time | 11 (44%) | |
| Homemaker | 1 (1%) | |
| Temporarily unemployed | 6 (8%) | |
| Smoking status, n (%) | 79 | |
| Current smoker | 19 (24%) | |
| Ex-smoker | 53 (67%) | |
| Never smoked | 7 (9%) | |
| Smoking, pack·years | 72 | 40 [25 to 62] |
| Type of cancer, n (%) | 79 | |
| Non-small cell lung cancer | ||
| Adenocarcinoma | 44 (56%) | |
| Squamous cell carcinoma | 24 (30%) | |
| Large cell | 2 (3%) | |
| Adenosquamous carcinoma | 1 (1.3%) | |
| Small cell lung cancer | 5 (6%) | |
| Poorly differentiated carcinoma/unknown | 1 (1.3%)/2 (2.6%) | |
| NSCLC/SCLC stage, n (%) | 79 | |
| Early (I to IIIA)/limited | 32 (41%) | |
| Advanced (IIIB to IV)/extensive | 47 (59%) | |
| ECOG status, n (%) | 79 | |
| 0 / 1 / 2 | 26 (33%)/40 (51%)/13 (17%) | |
| COPD, n (%) | 79 | |
| Yes | 33 (42%) | |
| No | 41 (52%) | |
| Unsure | 5 (7%) | |
| FEV1, L | 63 | 1.9 ± 0.7 |
| FEV1, %pred | 63 | 72.6 ± 25.1 |
| FVC, L | 63 | 3.0 ± 1.0 |
| FVC, %pred | 63 | 85.3 ± 22.1 |
| FEV1/FVC, % | 63 | 63.1 ± 15.9 |
| HRQoL | 79 | |
| FACT-LCS (0 to 28) | 20 ± 5 | |
| SF-36 PCS (0 to 100) | 44 ± 11 | |
| SF-36 MCS (0 to 100) | 41 ± 10 | |
| EORTC QLQ-C30-GH (0 to 100) | 61 ± 23 | |
| Symptoms | 79 | |
| Fatigue (FACIT-F) | 38 ± 12 | |
| Dyspnoea (mMRC), n (%) | ||
| 0 / 1 / 2 / 3 / 4 | 17 (22%)/38 (48%)/16 (20%)/7 (9%)/1 (1%) | |
| Comorbidities | 79 | |
| SCQ Number of comorbidities | 5 ± 4 | |
| SCQ Total score | 10 ± 4 | |
| SCQ comorb. affecting activities | 2 ± 1 | |
| Muscle force | 78 ** | |
| Hand grip force, Nm | 30 ± 9 | |
| Hand grip force, %pred | 94 ± 24 | |
| Blood cell count | 78 ** | |
| Neutrophils, ×109/L | 7 ± 4 | |
| Platelets, ×109/L | 312 ± 136 | |
| Lymphocytes, ×109/L | 2 ± 1 | |
| NLR | 3.2 [2.4 to 5.4] |
| Variable | Value 1 |
|---|---|
| Number of valid days | 7 [6 to 7] |
| Waking wear time, min/day | 887.4 ± 86.3 |
| Time spent sedentary, min/day | 630.3 ± 111.2 |
| Time spent in LIPA, min/day | 245.6 ± 88.0 |
| Time spent in MVPA, min/day | 4.6 [1 to 14.6] |
| Daily step count, steps/day | 7768 ± 3758 |
| UBD (min) | 18.1 [13.4 to 23.8] |
| Time spent in sedentary bouts 30 to <60 min, min/day | 136.7 [101.5 to 184.7] |
| Time spent in sedentary bouts ≥60 min, min/day | 79.5 [31.4 to 123.4] |
| Number of sedentary bouts of >60 min, bouts/day | 1 [0.3 to 1.4] |
| Variables | FACIT-F † (r-Value) | mMRC (OR [95% CI]) | SF-36 PCS (r-Value) | SF-36 MCS (r-Value) | FACT-LCS (r-Value) | EORTC QLQ-C30-GH (r-Value) | Hand Grip Force (%pred) (r-Value) | SCQ Total Score (r-Value) | FEV1 % pred) (r-Value) |
|---|---|---|---|---|---|---|---|---|---|
| Sedentary behaviour | |||||||||
| Time spent in sedentary behaviour (h/day) | −0.22 * | 1.46 (1.08, 1.96) ** | −0.39 ** | −0.06 | −0.12 | −0.28 * | −0.38 ** | 0.21 | 0.04 |
| UBD (min) | −0.20 * | 1.09 (1.03, 1.17) ** | −0.35 ** | −0.07 | −0.02 | −0.23 * | −0.37 ** | 0.21 | −0.04 |
| Physical activity | |||||||||
| Time spent in light intensity physical activity (h/day) | 0.40 ** | 0.48 (0.31, 0.74) ** | 0.50 ** | 0.13 | 0.26 * | 0.43 ** | 0.30 ** | −0.25 * | 0.02 |
| Time spent in moderate-to-vigorous physical activity (min/day) | 0.29 ** | 0.94 (0.88, 0.99) * | 0.40 ** | 0.04 | 0.15 | 0.34 ** | 0.34 ** | −0.37 ** | 0.28 * |
| Daily step count (steps/day) | 0.46 ** | 0.84 (0.76, 0.92) ** | 0.58 * | 0.10 | 0.30 * | 0.46 ** | 0.34 ** | −0.35 ** | 0.06 |
| Variables | FACIT-F * (β) | mMRC (OR) | SF-36 PCS (β) | FACT-LCS (β) | EORTC QLQ-C30-GH (β) | Hand Grip Force (%pred) (β) | SCQ Total Score (β) | FEV1 (%pred) (β) |
|---|---|---|---|---|---|---|---|---|
| Sedentary behaviour | ||||||||
| Time spent in sedentary behaviour (h/day) | −1.65 (−3.03, −0.27) p = 0.02 | 2.3 (1.45, 3.65) p < 0.001 | −1.97 (−3.17, −0.77) p < 0.01 | −0.40 (−0.97, 0.16) p = 0.17 | −3.63 (−6.26, −1.00) p < 0.01 | −2.55 (−4.98, −0.11) p = 0.04 | 0.44 (−0.05, 0.93) p = 0.08 | −1.57 (−4.42, 1.29) p = 0.28 |
| UBD (min) | −0.33 (−0.55, −0.10) p < 0.01 | 1.12 (1.04, 1.20) p < 0.01 | −0.33 (−0.53, −0.13) p < 0.01 | −0.04 (−0.13, 0.06) p = 0.43 | −0.52 (−0.97, −0.08) p = 0.02 | −0.45 (−0.86, −0.04) p = 0.03 | 0.06 (−0.03, 0.14) p = 0.17 | −0.34 (−0.80, 0.13) p = 0.16 |
| Physical activity | ||||||||
| Time spent in light intensity physical activity (h/day) | 3.73 (2.13, 5.33) p < 0.01 | 0.44 (0.27, 0.71) p < 0.01 | 3.60 (2.20, 5.00) p < 0.01 | 1.00 (0.31, 1.68) p < 0.01 | 6.44 (3.28, 9.61) p < 0.01 | 3.61 (0.55, 6.66) p = 0.02 | −0.59 (−1.21, 0.02) p = 0.06 | 3.46 (−0.38, 7.30) p = 0.08 |
| Time spent in moderate-to-vigorous physical activity (min/day) | 0.24 (0.08, 0.39) p < 0.01 | 0.92 (0.85, 0.99) p = 0.02 | 0.21 (0.07, 0.35) p < 0.01 | 0.05 (−0.02, 0.12) p = 0.13 | 0.51 (0.21, 0.81) p < 0.01 | 0.09 (−0.20, 0.38) p = 0.55 | −0.05 (−0.11, 0.01) p = 0.10 | 0.38 (0.03, 0.72) p = 0.03 |
| Accelerometer filtered steps (500 steps increments) | 0.86 (0.55, 1.17) p < 0.01 | 0.81 (0.72, 0.91) p < 0.001 | 0.85 (0.58, 1.11) p < 0.01 | 0.26 (0.12, 0.39) p < 0.01 | 1.69 (1.10, 2.29) p < 0.01 | 0.64 (0.01, 1.26) p = 0.045 | −0.15 (−0.28, −0.03) p = 0.01 | 0.81 (0.02, 1.59) p = 0.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ch’ng, S.N.; McVeigh, J.A.; Manners, D.; Boyle, T.; Peddle-McIntyre, C.J.; Thomas, R.; Leong, J.; Bowyer, S.; Mooney, K.; Straker, L.; et al. Sedentary Behaviour, Physical Activity, and Their Associations with Health Outcomes at the Time of Diagnosis in People with Inoperable Lung Cancer. J. Clin. Med. 2022, 11, 5870. https://doi.org/10.3390/jcm11195870
Ch’ng SN, McVeigh JA, Manners D, Boyle T, Peddle-McIntyre CJ, Thomas R, Leong J, Bowyer S, Mooney K, Straker L, et al. Sedentary Behaviour, Physical Activity, and Their Associations with Health Outcomes at the Time of Diagnosis in People with Inoperable Lung Cancer. Journal of Clinical Medicine. 2022; 11(19):5870. https://doi.org/10.3390/jcm11195870
Chicago/Turabian StyleCh’ng, Shu Ning, Joanne A. McVeigh, David Manners, Terry Boyle, Carolyn J. Peddle-McIntyre, Rajesh Thomas, Jeanie Leong, Samantha Bowyer, Kirsten Mooney, Leon Straker, and et al. 2022. "Sedentary Behaviour, Physical Activity, and Their Associations with Health Outcomes at the Time of Diagnosis in People with Inoperable Lung Cancer" Journal of Clinical Medicine 11, no. 19: 5870. https://doi.org/10.3390/jcm11195870
APA StyleCh’ng, S. N., McVeigh, J. A., Manners, D., Boyle, T., Peddle-McIntyre, C. J., Thomas, R., Leong, J., Bowyer, S., Mooney, K., Straker, L., Galvão, D. A., & Cavalheri, V. (2022). Sedentary Behaviour, Physical Activity, and Their Associations with Health Outcomes at the Time of Diagnosis in People with Inoperable Lung Cancer. Journal of Clinical Medicine, 11(19), 5870. https://doi.org/10.3390/jcm11195870