
Quality of Life in the Postpartum Recovery of Women Who Practice Hypopressive Exercise: Randomized Clinical Trial

 ,
,  , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Subjects
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Study
2.6. Variables and Assessment Tools
2.6.1. Social-Demographic and Anthropometric Variables
2.6.2. Level of Effort and Workout Intensity
2.6.3. Health Related Quality of Life (HRQoL)
2.7. Sample Size
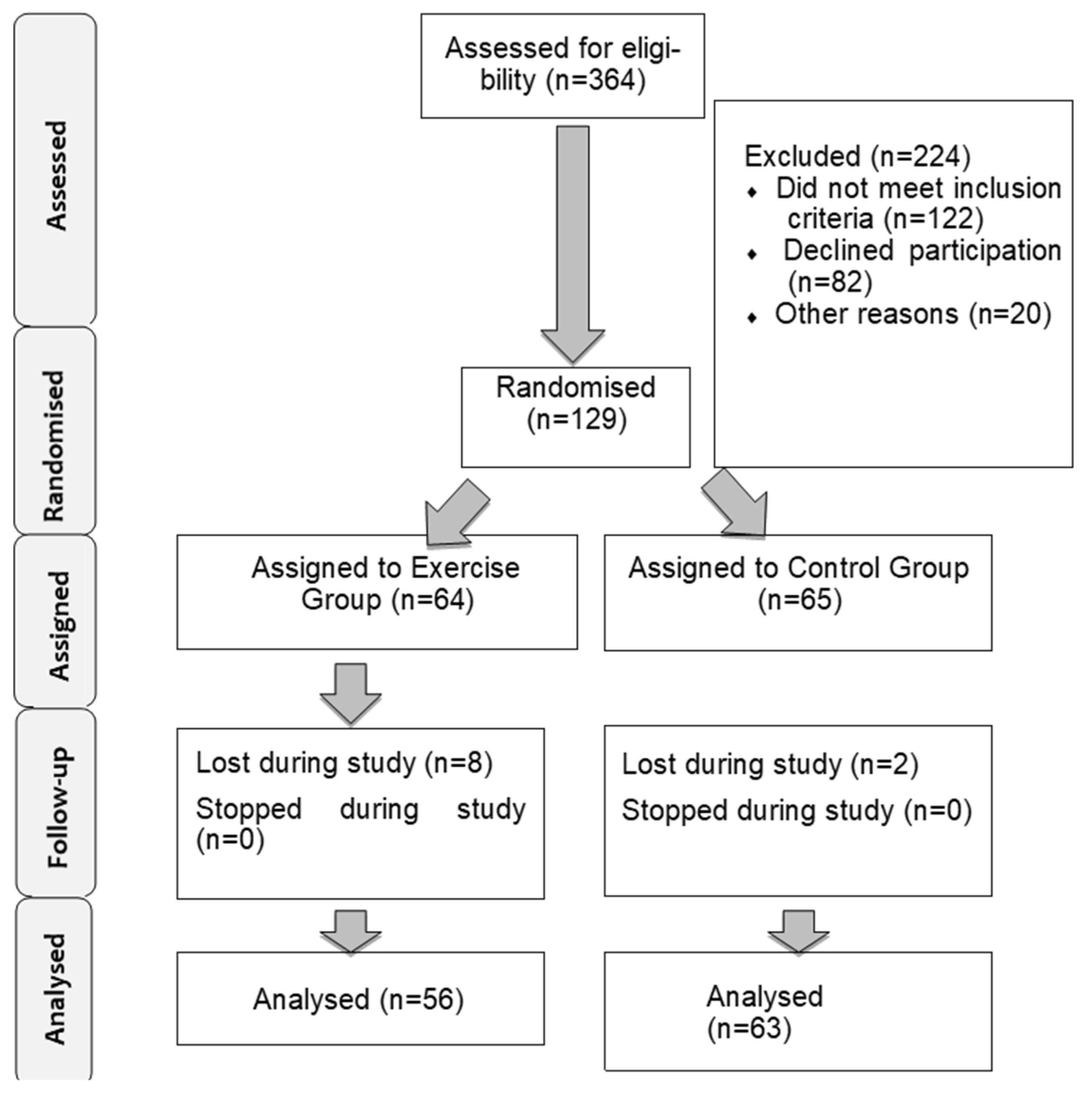
2.8. Randomization
2.9. Statistical Analysis
3. Results
4. Discussion
5. Conclusions

Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Urzúa, M.A.; Caqueo-Urízar, A. Quality of life: A theoretical review of the concept. Ter. Psicol. 2012, 30, 61–71. [Google Scholar]
- Pescatello, L.S.; American College of Sports Medicine (Eds.) ACSM’s Guidelines for Exercise Testing and Prescription, 9th ed; Wolters Kluwer/Lippincott Williams & Wilkins Health: Philadelphia, PA, USA, 2014; 456p. [Google Scholar]
- Syed, H.; Slayman, T.; Thoma, K.D. American college of obstetricians and gynecologists committee opinion no. 804: Physical activity and exercise during pregnancy and the postpartum period. Obstet. Gynecol. 2021, 137, 375–376. [Google Scholar] [CrossRef]
- Uthaipaisanwong, A.; Rungruxsirivorn, T.; Roomruangwong, C.; Taechakraichana, N.; Chaithongwongwatthana, S. Associated factors of prenatal depression among teenage pregnant women at King Chulalongkorn Memorial Hospital. J. Med. Assoc. Thai. 2015, 98, 437–443. [Google Scholar]
- Odalovic, M.; Tadic, I.; Lakic, D.; Nordeng, H.; Lupattelli, A.; Tasic, L. Translation and factor analysis of structural models of Edinburgh postnatal depression scale in Serbian pregnant and postpartum women–web-based study. Women Birth 2015, 28, e31–e35. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists. Exersice After Pregnancy. 2019. Available online: https://www.acog.org/store/products/patient-education/pamphlets/labor-delivery-and-postpartum-care/exercise-after-pregnancy (accessed on 1 September 2022).
- Vilagut, G.; Ferrer, M.; Rajmil, L.; Rebollo, P.; Permanyer-Miralda, G.; Quintana, J.M.; Santed, R.; Valderas, J.M.; Ribera, A.; Domingo-Salvany, A.; et al. The Spanish version of the short form 36 health survey: A decade of experience and new developments. Gac. Sanit. 2005, 19, 135–150. [Google Scholar] [CrossRef]
- CONSORT Checklist. 2017. Available online: http://www.consort-statement.org/checklists/view/32-consorte/66-title (accessed on 1 February 2017).
- Rial, T.; Pinsach, P. Hypopressive Techniques, 7th ed.; Ediciones Cardeñoso: Vigo, Spain, 2014; 152p, Available online: http://edicionescardenoso.blogspot.com/2014/07/tecnicas-hipopresivas-de-tamara-rial-y.html (accessed on 1 September 2022).
- Sandoval, T.; Manzano, C.; Ramos, J.; Martínez, M. Evaluation of the body mass index, maternal weight gain and ideal weight of women with normal pregnancy. Ginecol. Obstet. Mex. 1999, 67, 404–407. [Google Scholar]
- Cuentas, M.; Domínguez, J.L.; Mendoza, M.C.; Montoya, J.G.; Mori, N.; Perez, D.S.; Larrabure, G.; Córdova, D. Estado nutricional de la gestante según los índices de Quetelet, Quetelet modificado y monograma de Rosso. CIMEL Cienc. e Investig. Médica Estud. Latinoam. 2002, 7, 30–34. Available online: http://www.redalyc.org/pdf/717/71700707.pdf (accessed on 16 March 2016).
- Jordan, M.; Arce, R.M.; López, R. Nutritional status of pregnant women and their relationship with birth weight: 1997–1999. Cuad. Hosp. Clín. 2004, 49, 11–20. [Google Scholar]
- Álvarez-Dardet, C.; Alonso, J.; Domingo, A.; Regidor, E. The Measurement of Social Class in Health Sciences; SEG Editores: Barcelona, Sapin, 1995; 124p, Available online: https://www.iberlibro.com/MEDICI%C3%93N-CLASE-SOCIAL-CIENCIAS-SALUD-INFORME/18209145026/bd (accessed on 21 March 2018).
- World Health Organization. Global Physical Activity Questionnaire (GPAQ)-Analysis Guide; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Ware, J.E.; Kosinski, M.; Bjorner, J.B.; Turner-Bowker, D.; Gandek, B.; Maruish, M.E. SF-36v2 Health Survey: Administration Guide for Clinical Trial Investigators; QualityMetric, Incorporated: Lincoln, RI, USA, 2008; 34p. [Google Scholar]
- Barakat, R.; Pelaez, M.; Montejo, R.; Luaces, M.; Zakynthinaki, M. Exercise during pregnancy improves maternal health perception: A randomized controlled trial. Am. J. Obstet. Gynecol. 2011, 204, 402.e1–402.e7. [Google Scholar] [CrossRef]
- Ware, J.E.; Snow, K.K.; Kosinski, M.; Gandek, B. New England Medical Center Hospital, Health Institute. In SF-36 Health Survey: Manual and Interpretation Guide; Health Institute, New England Medical Center: Boston, MA, USA, 1993. [Google Scholar]
- Singh, S.; Kaur, R.; Singh, S. Relationship of parity and health related quality of life among women. Hum. Biol. Rev. 2015, 4, 159–166. [Google Scholar]
- Haas, J.S.; Jackson, R.A.; Fuentes-Afflick, E.; Stewart, A.L.; Dean, M.L.; Brawarsky, P.; Escobar, G.J. Changes in the health status of women during and after pregnancy. J. Gen. Intern. Med. 2005, 20, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Doya, R.; Pinti, A.; Lenne, B.; Garnier, C.; Toumi, H.; Watelain, E. Therapeutic Gymnastic: Effects on the Quality of Life at Two Months in Postpartum Period-Semantic Scholar; IWBBIO: Granada, Spain, 2013. [Google Scholar]
- Haruna, M.; Watanabe, E.; Matsuzaki, M.; Ota, E.; Shiraishi, M.; Murayama, R.; Yoshida, M.; Yeo, S. The effects of an exercise program on health-related quality of life in postpartum mothers: A randomized controlled trial. Health 2013, 5, 432. [Google Scholar] [CrossRef]
- Sánchez-García, J.C.; Rodríguez-Blanque, R.; Mur-Villar, N.; Sánchez-López, A.M.; Levet-Hernández, M.C.; Aguilar-Cordero, M.J. Influence of physical exercise on quality of life during pregnancy and postpartum. Systematic review. Nutr. Hosp. 2016, 33 (Suppl. 5), 1–9. [Google Scholar]
- Yang, C.-L.; Chen, C.-H. Effectiveness of aerobic gymnastic exercise on stress, fatigue, and sleep quality during postpartum: A pilot randomized controlled trial. Int. J. Nurs. Stud. 2018, 77, 1–7. [Google Scholar] [CrossRef]
- Wu, J.; Einerson, B.; Shaw, J.M.; Nygaard, I.E.; Sheng, X.; Wolpern, A.; Egger, M.J. Association between sleep quality and physical activity in postpartum women. Sleep Health 2019, 5, 598–605. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Exercise Group (n = 65) | Control Group (n = 64) | p-Value |
|---|---|---|---|
| Age in years (Mean ± SD) | 32.12 ± 4.43 | 30.58 ± 4.75 | 0.331 |
| min–max | 21–43 | 22–43 | |
| Marital Status (Freq. (%)) | 57 (44.2) | 59 (45.7) | 0.396 |
| Height (Mean ± SD) | 1.646 ± 0.06 | 1.651 ± 0.05 | 0.604 |
| Weight1 (Mean ± SD) | 67.07 ± 12.23 | 67.89 ± 12.58 | 0.71 |
| BMI 1 (Median [Q1–Q3]) | 23.89 [21.52–27.51] | 24.01 [21.78–26.58] | 0.953 |
| Normal weight(Mean ± SD) | 19 (29.2) | 12 (18.8) | 0.322 |
| Overweight (Mean ± SD) | 31 (48.4) | 30 (46.2) | |
| Obesity (Mean ± SD) | 21 (32.8) | 16 (24.6) | |
| Parity (Freq. (%)) | 20 (30.77) | 17 (26.56) | 0.739 |
| Gestation Time in days(Mean ± SD) | 280.09 ± 8.257 | 279.70 ± 8.919 | 0.996 |
| Physical Activity Domains (according to intensity) GPAQ | |||
| Daily Activity | 0.880 | ||
| Moderate | 57 (93.4) | 56 (94.9) | |
| Vigorous | 4 (6.6) | 3 (5.1) | |
| Moderate Movement | 0.497 | 44 (68.8) | 0.497 |
| Recreational Activity | |||
| Moderate | 52 (80.0) | 53 (82.8) | 0.681 |
| Vigorous | 13 (20.0) | 11 (17.2) | |
| Aspect | Group | Postpartum Week | Interaction Group * Week | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| LPF | Seden | p | η2 | |||||||||||
| EG | CG | p | η2 | 16 Post | 28 Post | p | η2 | 16 Post | 28 Post | 16 Post | 28 Post | |||
| PF | 75.54 (14.40) | 74.56 (14.27) | 0.597 | 0.001 | 72.52 (15.46) | 77.52 (12.64) | 0.007 | 0.031 | 72.86 (14.95) | 78.21 (13.43) | 72.22 (16.01) | 76.90 (11.96) | 0.855 | 0.000 |
| RP | 44.87 (16.40) | 43.95 (13.44) | 0.611 | 0.001 | 38.97 (14.84) | 49.79 (12.86) | <0.001 | 0.137 | 38.06 (15.55) | 51.67 (14.38) | 39.78 (14.26) | 48.12 (11.20) | 0.144 | 0.009 |
| BP | 60.27 (17.53) | 60.46 (12.71) | 0.922 | 0.000 | 58.55 (14.89) | 62.19 (15.22) | 0.054 | 0.016 | 57.21 (16.75) | 63.32 (17.90) | 59.73 (13.04) | 61.19 (12.44) | 0.237 | 0.006 |
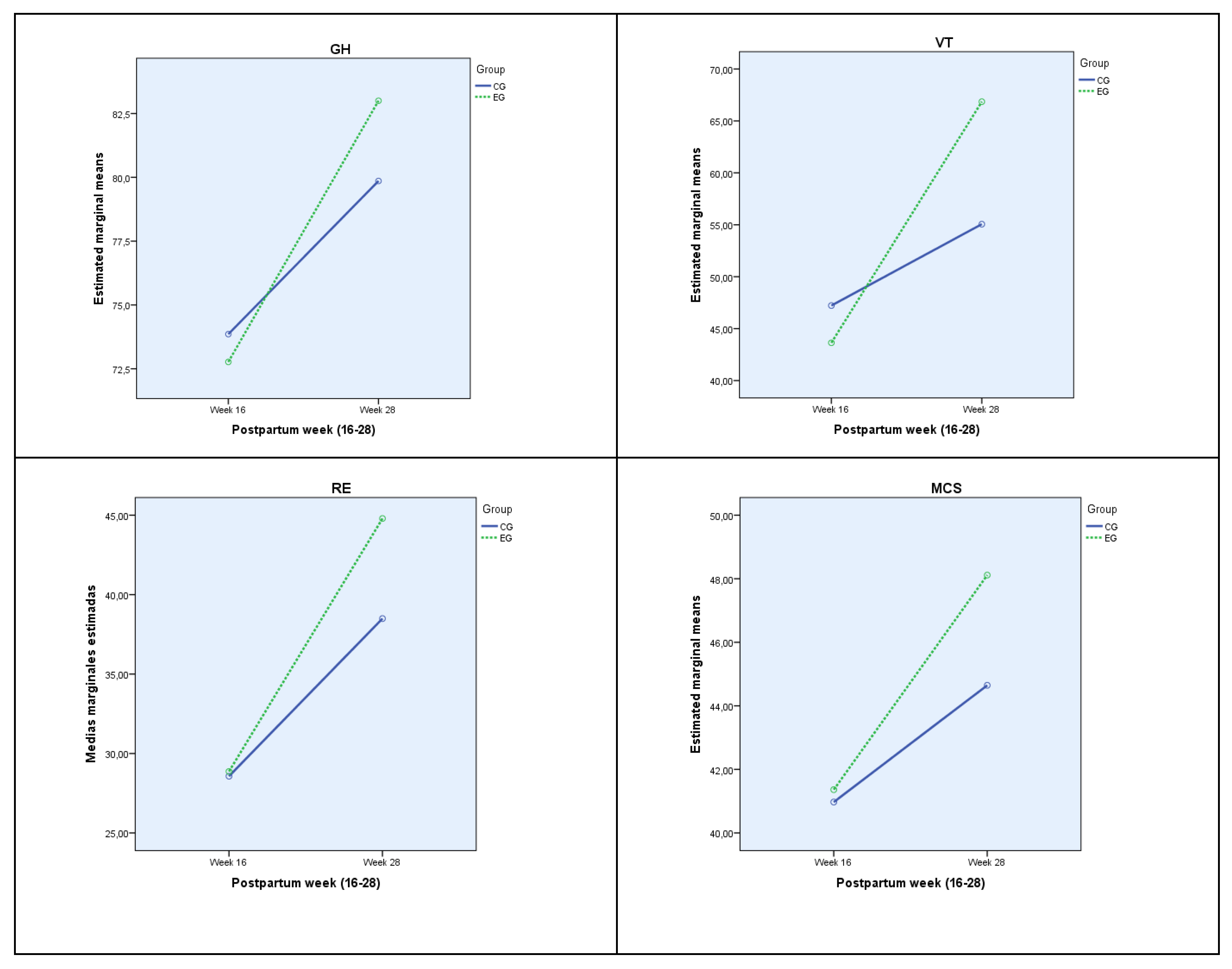
| GH | 77.88 (9.60) | 76.86 (7.63) | 0.298 | 0.005 | 73.34 (8.78) | 81.34 (6.30) | <0.001 | 0.225 | 72.77 (9.67) | 83.00 (6.26) | 73.86 (7.95) | 79.86 (6.01) | 0.033 | 0.019 |
| VT | 55.25 (17.25) | 51.14 (14.56) | 0.020 | 0.023 | 45.54 (14.94) | 60.61 (13.23) | <0.001 | 0.252 | 43.64 (14.08) | 66.85 (11.30) | 47.22 (15.59) | 55.06 (12.39) | <0.001 | 0.076 |
| SF | 83.37 (11.79) | 81.15 (12.92) | 0.158 | 0.008 | 79.31 (13.26) | 85.08 (10.83) | <0.001 | 0.057 | 79.46 (12.25) | 87.28 (9.97) | 79.17 (14.20) | 83.14 (11.26) | 0.221 | 0.006 |
| RE | 36.83 (12.64) | 33.53 (9.69) | 0.006 | 0.032 | 28.71 (9.19) | 41.46 (9.42) | <0.001 | 0.340 | 28.87 (9.40) | 44.79 (10.24) | 28.57 (9.07) | 38.49 (7.55) | 0.012 | 0.027 |
| MH | 78.30 (10.45) | 75.32 (9.89) | 0.018 | 0.024 | 73.53 (10.94) | 79.92 (8.41) | <0.001 | 0.101 | 74.73 (11.46) | 81.88 (7.95) | 72.46 (10.43) | 78.17 (8.49) | 0.570 | 0.001 |
| PCS | 48.28 (5.15) | 48.47 (4.16) | 0.749 | 0.000 | 47.37 (4.71) | 49.39 (4.36) | 0.001 | 0.050 | 46.89 (4.96) | 49.67 (5.00) | 47.80 (4.48) | 49.15 (3.73) | 0.228 | 0.006 |
| MCS | 44.74 (5.16) | 42.81 (3.97) | <0.001 | 0.064 | 41.16 (4.25) | 46.28 (3.51) | <0.001 | 0.333 | 41.36 (4.66) | 48.11 (2.99) | 40.97 (3.89) | 44.65 (3.13) | 0.002 | 0.042 |
| Aspect | BMI | Group | Postpartum Week | Interaction Week * Group | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| EG | CG | p | η2 | ||||||||||||
| EG | CG | p | η2 | 16 post | 28 post | p | η2 | 16 post | 28 post | 16 post | 28 post | ||||
| PCS | Normal Weight | 48.06 (4.40) | 49.31 (4.50) | 0.103 | 0.021 | 47.83 (4.53) | 49.58 (4.28) | 0.022 | 0.041 | 46.79 (4.02) | 49.33 (4.46) | 48.81 (4.82) | 49.81 (4.16) | 0.315 | 0.008 |
| Overweight | 48.01 (6.41) | 48.35 (3.26) | 0.757 | 0.001 | 46.85 (4.96) | 49.55 (4.43) | 0.011 | 0.084 | 46.11 (6.31) | 49.90 (6.12) | 47.42 (3.65) | 49.27 (2.58) | 0.373 | 0.011 | |
| Obesity | 49.96 (4.97) | 44.78 (2.91) | 0.003 | 0.310 | 46.66 (4.98) | 48.07 (4.66) | 0.382 | 0.032 | 49.27 (5.27) | 50.64 (4.96) | 44.05 (3.17) | 45.50 (2.67) | 0.979 | 0.000 | |
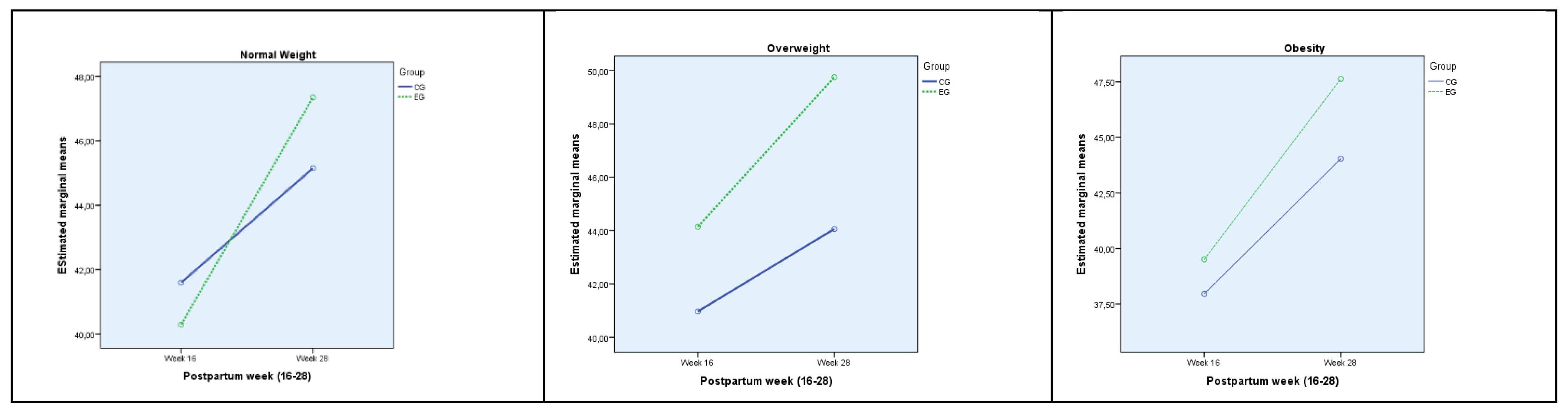
| MCS | Normal Weight | 43.82 (4.94) | 43.37 (4.33) | 0.491 | 0.004 | 40.96 (4.30) | 46.21 (3.25) | <0.001 | 0.343 | 40.29 (4.15) | 47.35 (2.56) | 41.59 (4.40) | 45.15 (3.49) | 0.008 | 0.054 |
| Overweight | 46.95 (4.79) | 42.51 (3.12) | <0.001 | 0.320 | 42.36(4.01) | 46.55(3.97) | <0.001 | 0.311 | 44.15 (4.54) | 49.77 (3.15) | 40.97 (2.96) | 44.06 (2.48) | 0.099 | 0.036 | |
| Obesity | 43.57 (5.75) | 50.00 (4.13) | 0.062 | 0.137 | 38.73 (3.73) | 45.83 (3.55) | <0.001 | 0.548 | 39.96 (4.75) | 47.63 (3.24) | 37.96 (2.47) | 44.03 (3.04) | 0.445 | 0.025 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanchez-Garcia, J.C.; Aguilar-Cordero, M.J.; Montiel-Troya, M.; Marín-Jiménez, A.E.; Cortes-Martin, J.; Rodriguez-Blanque, R. Quality of Life in the Postpartum Recovery of Women Who Practice Hypopressive Exercise: Randomized Clinical Trial. J. Clin. Med. 2022, 11, 5592. https://doi.org/10.3390/jcm11195592
Sanchez-Garcia JC, Aguilar-Cordero MJ, Montiel-Troya M, Marín-Jiménez AE, Cortes-Martin J, Rodriguez-Blanque R. Quality of Life in the Postpartum Recovery of Women Who Practice Hypopressive Exercise: Randomized Clinical Trial. Journal of Clinical Medicine. 2022; 11(19):5592. https://doi.org/10.3390/jcm11195592
Chicago/Turabian StyleSanchez-Garcia, Juan Carlos, María José Aguilar-Cordero, Maria Montiel-Troya, Ana Eugenia Marín-Jiménez, Jonathan Cortes-Martin, and Raquel Rodriguez-Blanque. 2022. "Quality of Life in the Postpartum Recovery of Women Who Practice Hypopressive Exercise: Randomized Clinical Trial" Journal of Clinical Medicine 11, no. 19: 5592. https://doi.org/10.3390/jcm11195592
APA StyleSanchez-Garcia, J. C., Aguilar-Cordero, M. J., Montiel-Troya, M., Marín-Jiménez, A. E., Cortes-Martin, J., & Rodriguez-Blanque, R. (2022). Quality of Life in the Postpartum Recovery of Women Who Practice Hypopressive Exercise: Randomized Clinical Trial. Journal of Clinical Medicine, 11(19), 5592. https://doi.org/10.3390/jcm11195592