
Group-Based Trajectory Analysis for Postpartum Depression Symptoms among Chinese Primiparous Women


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Instruments
2.3. Data Collection
2.4. Statistical Analysis
2.5. Building the GBTM
2.6. Evaluating Trajectory Model Fit
3. Results
3.1. Participant Profile
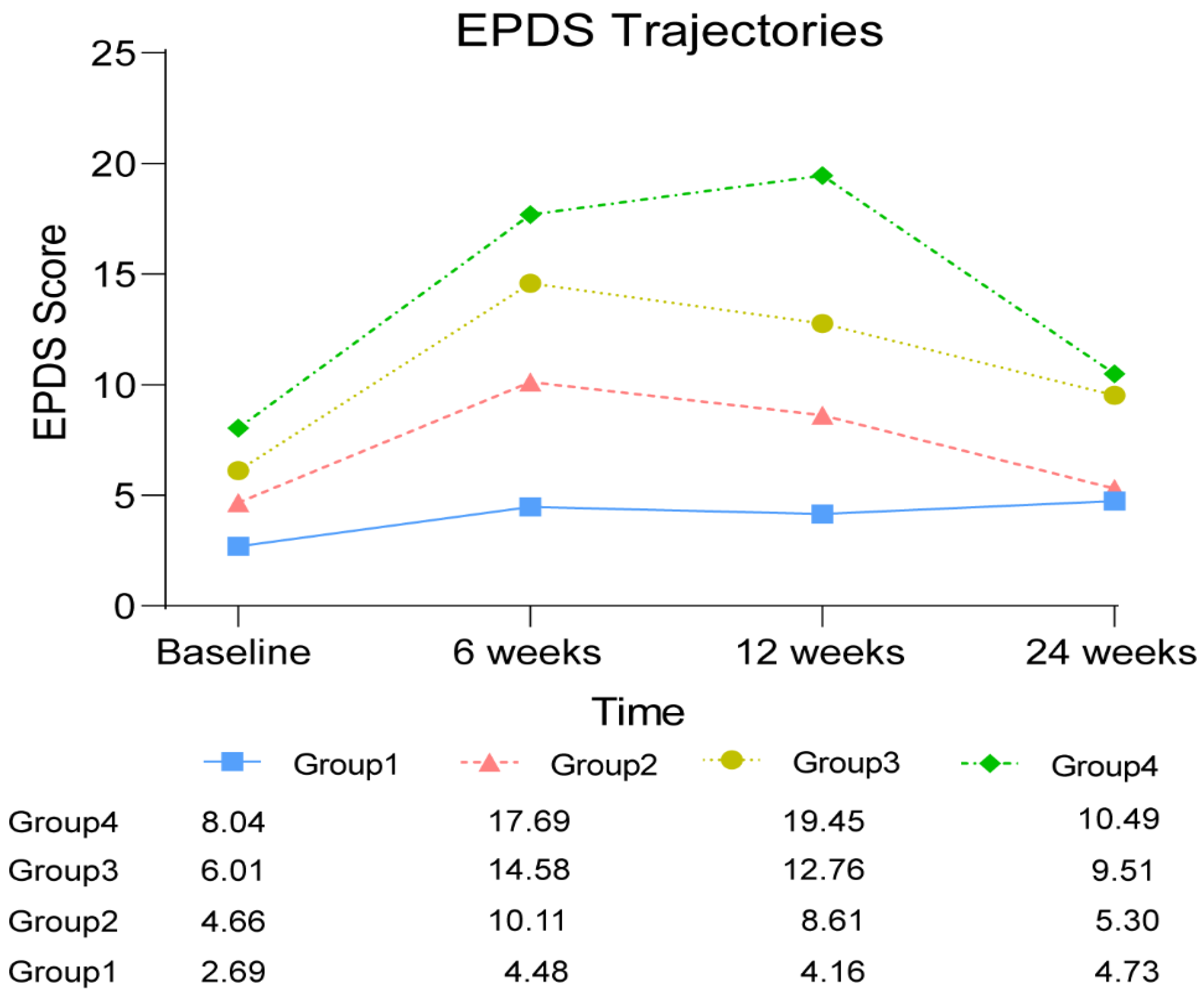
3.2. Trajectory Model Development
3.3. Predictors of PPD Trajectory Membership
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cox, J.L.; Murray, D.; Chapman, G. A Controlled Study of the Onset, Duration and Prevalence of Postnatal Depression. Br. J. Psychiatry 1993, 163, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Craig, M.; Howard, L. Postnatal depression. BMJ Clin. Evid. 2009, 2009, 1407. [Google Scholar]
- El-Gilany, A.-H.; Elkhawaga, G.O.; Sarraf, B.B. Depression and its associated factors among elderly: A community-based study in Egypt. Arch. Gerontol. Geriatr. 2018, 77, 103–107. [Google Scholar] [CrossRef]
- Radzi, C.W.J.B.W.M.; Jenatabadi, H.S.; Samsudin, N. Postpartum depression symptoms in survey-based research: A structural equation analysis. BMC Public Health 2021, 21, 27. [Google Scholar] [CrossRef]
- Zeng, N.; Pope, Z.; Lee, J.; Gao, Z. Virtual Reality Exercise for Anxiety and Depression: A Preliminary Review of Current Research in an Emerging Field. J. Clin. Med. 2018, 7, 42. [Google Scholar] [CrossRef] [PubMed]
- Daley, A.; Jolly, K.; MacArthur, C. The effectiveness of exercise in the management of post-natal depression: Systematic review and meta-analysis. Fam. Pract. 2009, 26, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Goweda, R.; Metwally, T. Prevalence and associated risk factors of postpartum depression: A cross sectional study. Arch. Clin. Psychiatry 2020, 47, 106–109. [Google Scholar] [CrossRef]
- Zejnullahu, V.A.; Ukella-Lleshi, D.; Zejnullahu, V.A.; Miftari, E.; Govori, V. Prevalence of postpartum depression at the clinic for obstetrics and gynecology in Kosovo teaching hospital: Demographic, obstetric and psychosocial risk factors. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 256, 215–220. [Google Scholar] [CrossRef]
- Zheng, X.; Morrell, J.; Watts, K. Changes in maternal self-efficacy, postnatal depression symptoms and social support among Chinese primiparous women during the initial postpartum period: A longitudinal study. Midwifery 2018, 62, 151–160. [Google Scholar] [CrossRef]
- Dadi, A.F.; Miller, E.R.; Mwanri, L. Postnatal depression and its association with adverse infant health outcomes in low- and middle-income countries: A systematic review and meta-analysis. BMC Pregnancy Childbirth 2020, 20, 416. [Google Scholar] [CrossRef]
- Slomian, J.; Honvo, G.; Emonts, P.; Reginster, J.-Y.; Bruyère, O. Consequences of maternal postpartum depression: A systematic review of maternal and infant outcomes. Women’s Health 2019, 15, 1745506519844044. [Google Scholar] [CrossRef] [PubMed]
- Puente, C.P.; Suso-Ribera, C.; Rico, S.B.; Marín, D.; Montero, J.S.R.; Catalá, P. Is the Association between Postpartum Depression and Early Maternal–Infant Relationships Contextually Determined by Avoidant Coping in the Mother? Int. J. Environ. Res. Public Health 2021, 18, 562. [Google Scholar] [CrossRef]
- Wang, Q.; Zhang, Y.; Li, X.; Ye, Z.; Huang, L.; Zhang, Y.; Zheng, X. Exploring Maternal Self-Efficacy of First-Time Mothers among Rural-to-Urban Floating Women: A Quantitative Longitudinal Study in China. Int. J. Environ. Res. Public Health 2021, 18, 2793. [Google Scholar] [CrossRef]
- Zheng, X.; Morrell, J.; Watts, K. A quantitative longitudinal study to explore factors which influence maternal self-efficacy among Chinese primiparous women during the initial postpartum period. Midwifery 2017, 59, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Woldeyohannes, D.; Tekalegn, Y.; Sahiledengle, B.; Ermias, D.; Ejajo, T.; Mwanri, L. Effect of postpartum depression on exclusive breast-feeding practices in sub-Saharan Africa countries: A systematic review and meta-analysis. BMC Pregnancy Childbirth 2021, 21, 113. [Google Scholar] [CrossRef]
- Wilkinson, R.B.; Mulcahy, R. Attachment and interpersonal relationships in postnatal depression. J. Reprod. Infant Psychol. 2010, 28, 252–265. [Google Scholar] [CrossRef]
- Nagin, D.S. Group-Based Trajectory Modeling: An Overview. Ann. Nutr. Metab. 2014, 65, 205–210. [Google Scholar] [CrossRef]
- Nguefack, H.L.N.; Pagé, M.G.; Katz, J.; Choinière, M.; Vanasse, A.; Dorais, M.; Samb, O.M.; Lacasse, A. Trajectory Modelling Techniques Useful to Epidemiological Research: A Comparative Narrative Review of Approaches. Clin. Epidemiol. 2020, 12, 1205–1222. [Google Scholar] [CrossRef]
- Baron, E.; Bass, J.; Murray, S.M.; Schneider, M.; Lund, C. A systematic review of growth curve mixture modelling literature investigating trajectories of perinatal depressive symptoms and associated risk factors. J. Affect. Disord. 2017, 223, 194–208. [Google Scholar] [CrossRef]
- Barban, N.; Billari, F.C. Classifying life course trajectories: A comparison of latent class and sequence analysis. J. R. Stat. Soc. Ser. C (Applied Stat.) 2012, 61, 765–784. [Google Scholar] [CrossRef]
- Frankfurt, S.; Frazier, P.; Syed, M.; Jung, K.R. Using Group-Based Trajectory and Growth Mixture Modeling to Identify Classes of Change Trajectories. Couns. Psychol. 2016, 44, 622–660. [Google Scholar] [CrossRef]
- Nagin, D.S.; Odgers, C.L. Group-Based Trajectory Modeling in Clinical Research. Annu. Rev. Clin. Psychol. 2010, 6, 109–138. [Google Scholar] [CrossRef]
- Song, M. Trajectory analysis in obesity epidemiology: A promising life course approach. Curr. Opin. Endocr. Metab. Res. 2019, 4, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of Postnatal Depression: Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef]
- Cox, J.; Holden, J. Perinatal Mental Health: A Guide to the Edinburgh Postnatal Depression Scale (EPDS); Royal College of Psychiatrists: London, UK, 2003. [Google Scholar]
- Levis, B.; Negeri, Z.; Sun, Y.; Benedetti, A.; Thombs, B.D. Accuracy of the Edinburgh Postnatal Depression Scale (EPDS) for screening to detect major depression among pregnant and postpartum women: Systematic review and meta-analysis of individual participant data. BMJ 2020, 371, m4022. [Google Scholar] [CrossRef]
- O’Connor, E.; Rossom, R.C.; Henninger, M.; Groom, H.C.; Burda, B.U. Primary Care Screening for and Treatment of Depression in Pregnant and Postpartum Women: Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2016, 315, 388–406. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Guo, X.; Lau, Y.; Chan, K.S.; Yin, L.; Chen, J. Psychometric evaluation of the Mainland Chinese version of the Edinburgh Postnatal Depression Scale. Int. J. Nurs. Stud. 2009, 46, 813–823. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Zheng, X. The relationship between social support and postnatal depression of primiparous women. Chin. J. Nurs. 2001, 36, 731–733. [Google Scholar]
- Arrandale, V.; Koehoorn, M.; MacNab, Y.; Kennedy, S.M. How to Use SAS® Proc Traj and SAS® Proc Glimmix in Respiratory Epidemiology; University of British Columbia: Vancouver, BC, USA, 2006. [Google Scholar] [CrossRef]
- Jones, B.L.; Nagin, D.S. Proc TRAJ: A SAS Procedure for Group-Based Modeling of Longitudinal Data. In Proceedings of the 135st APHA Annual Meeting and Exposition 2007, Washington, DC, USA, 3–7 November 2007. [Google Scholar]
- Twisk, J.; Hoekstra, T. Classifying developmental trajectories over time should be done with great caution: A comparison between methods. J. Clin. Epidemiol. 2012, 65, 1078–1087. [Google Scholar] [CrossRef]
- Niyonkuru, C.; Wagner, A.K.; Ozawa, H.; Amin, K.; Goyal, A.; Fabio, A. Group-Based Trajectory Analysis Applications for Prognostic Biomarker Model Development in Severe TBI: A Practical Example. J. Neurotrauma 2013, 30, 938–945. [Google Scholar] [CrossRef]
- Jamshidian, M.; Jalal, S. Tests of Homoscedasticity, Normality, and Missing Completely at Random for Incomplete Multivariate Data. Psychometrika 2010, 75, 649–674. [Google Scholar] [CrossRef] [PubMed]
- Nagin, D. Group-Based Modeling of Development; Harvard University Press: Cambridge, MA, USA, 2005; Volume 4159, p. 9780674041318. [Google Scholar] [CrossRef]
- Wagner, A.K.; Amin, K.B.; Niyonkuru, C.; A Postal, B.; McCullough, E.H.; Ozawa, H.; Dixon, C.E.; Bayir, H.; Clark, R.S.; Kochanek, P.; et al. CSF Bcl-2 and cytochrome C temporal profiles in outcome prediction for adults with severe TBI. J. Cereb. Blood Flow Metab. 2011, 31, 1886–1896. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.K.; McCullough, E.H.; Niyonkuru, C.; Ozawa, H.; Loucks, T.; Dobos, J.A.; Brett, C.A.; Santarsieri, M.; Dixon, C.E.; Berga, S.L.; et al. Acute Serum Hormone Levels: Characterization and Prognosis after Severe Traumatic Brain Injury. J. Neurotrauma 2011, 28, 871–888. [Google Scholar] [CrossRef]
- Gavin, N.I.; Gaynes, B.N.; Lohr, K.N.; Meltzer-Brody, S.; Gartlehner, G.; Swinson, T. Perinatal depression: A systematic review of prevalence and incidence. Obstet. Gynecol. 2005, 106 Pt 1, 1071–1083. [Google Scholar] [CrossRef] [PubMed]
- Hewitt, C.; Gilbody, S.; Brealey, S.; Paulden, M.; Palmer, S.; Mann, R.; Green, J.; Morrell, J.; Barkham, M.; Light, K.; et al. Methods to identify postnatal depression in primary care: An integrated evidence synthesis and value of information analysis. Health Technol. Assess. 2009, 13, 147–230. [Google Scholar] [CrossRef]
- Siu, A.L.; Bibbins-Domingo, K.; Grossman, D.C.; Baumann, L.C.; Davidson, K.; Ebell, M.; García, F.A.R.; Gillman, M.; Herzstein, J.; Kemper, A.R.; et al. Screening for Depression in Adults: US Preventive Services Task Force Recommendation Statement. JAMA 2016, 315, 380–387. [Google Scholar] [CrossRef]
- Health NCCfM. Antenatal and Postnatal Mental Health: Clinical Management and Service Guidance; British Psychological Society: Leicester, UK, 2014. [Google Scholar]
- Gong, W.; Jin, X.; Cheng, K.K.; Caine, E.D.; Lehman, R.; Xu, D.R. Chinese Women’s Acceptance and Uptake of Referral after Screening for Perinatal Depression. Int. J. Environ. Res. Public Health 2020, 17, 8686. [Google Scholar] [CrossRef]
- Tully, K.P.; Stuebe, A.M.; Verbiest, S.B. The fourth trimester: A critical transition period with unmet maternal health needs. Am. J. Obstet. Gynecol. 2017, 217, 37–41. [Google Scholar] [CrossRef]
- Xiong, J.; Fang, Q.; Chen, J.; Li, Y.; Li, H.; Li, W.; Zheng, X. States Transitions Inference of Postpartum Depression Based on Multi-State Markov Model. Int. J. Environ. Res. Public Health 2021, 18, 7449. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Watts, K.; Morrell, J. Chinese primiparous women’s experience of the traditional postnatal practice of “Doing the month”: A descriptive method study. Jpn. J. Nurs. Sci. 2018, 16, 253–262. [Google Scholar] [CrossRef]
- van de Schoot, R.; Sijbrandij, M.; Winter, S.D.; Depaoli, S.; Vermunt, J.K. The GRoLTS-Checklist: Guidelines for Reporting on Latent Trajectory Studies. Struct. Equ. Model. A Multidiscip. J. 2016, 24, 451–467. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Missing Data Points | Samples Available for Analysis (%) |
|---|---|
| 1 | 131 (30.1) |
| 0 | 304 (69.9) |
| Total | 435 (100.00) |
| Variables | Total (n = 435) |
|---|---|
| Childbirth age, mean (SD) | 25.56 (3.34) |
| Marriage, n (%) | |
| Married | 435 (100%) |
| Education, n (%) | |
| Middle school or lower | 109 (25.06%) |
| High school | 123 (28.28%) |
| University or higher | 203 (46.67%) |
| Occupation, n (%) | |
| Professional | 19 (4.37%) |
| Skilled | 32 (7.36%) |
| Unskilled | 260 (59.78%) |
| Unemployed | 124 (28.51%) |
| Family income (per month, person) ※, n (%) | |
| <3000 yuan (USD 420) | 92 (21.15%) |
| 3001–5000 yuan (USD 420–700) | 202 (46.44%) |
| >5000 yuan (USD 700) | 141 (32.41%) |
| Childbirth mode, n (%) | |
| Natural childbirth | 285 (65.52%) |
| Assisted childbirth * | 67 (15.40%) |
| C-section | 83 (19.08%) |
| Attending parenting training, n (%) | |
| Yes | 230 (52.87%) |
| No | 205 (47.13%) |
| Baby gender, n (%) | |
| Girl | 176 (40.46%) |
| Boy | 259 (59.54%) |
| Baby health, mean (SD) | 81.94 (15.09) |
| Baby fussiness, mean (SD) | 66.19 (21.54) |
| Emotional support, mean (SD) | 10.34 (2.74) |
| Material support, mean (SD) | 10.12 (3.28) |
| Informational support, mean (SD) | 6.94 (3.21) |
| Evaluation of support, mean (SD) | 8.55 (2.99) |
| Number of Groups | Polynomial Order | BIC | Bayes Factor |
|---|---|---|---|
| 1 | 3 | −4658.88 | |
| 2 | 3 3 | −4299.13 | >1000 |
| 3 | 3 3 3 | −4192.20 | >1000 |
| 4 | 3 3 3 3 | −4130.93 | >1000 |
| 5 | 3 3 2 3 2 | −4136.80 | 0.0028 |
| Group 1 (n = 76) | Group 2 (n = 139) | Group 3 (n = 138) | Group 4 (n = 82) | |
|---|---|---|---|---|
| AvePP | 0.94 | 0.91 | 0.91 | 0.96 |
| 0.18 | 0.32 | 0.32 | 0.19 | |
| 0.18 | 0.32 | 0.31 | 0.19 | |
| | | 0.01 | 0.00 | 0.01 | 0.00 |
| 69.02 | 20.83 | 23.45 | 93.66 |
| Major PPD Status Group (Group 4) | Minor PPD Status Group (Group 3) | |||||
|---|---|---|---|---|---|---|
| Variables | OR | 95% CI | p Value | OR | 95% CI | p Value |
| Emotional support | 0.63 | (0.55, 0.73) | <0.001 | 0.57 | (0.50, 0.65) | <0.001 |
| Material support | 0.77 | (0.69, 0.86) | <0.001 | 0.75 | (0.68, 0.83) | <0.001 |
| Informational support | 0.73 | (0.66, 0.82) | <0.001 | 0.69 | (0.62, 0.76) | <0.001 |
| Evaluation of support | 0.48 | (0.41, 0.56) | <0.001 | 0.61 | (0.54, 0.69) | <0.001 |
| Attending parenting training | 0.08 | (0.04, 0.18) | <0.001 | 0.14 | (0.07, 0.26) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiong, J.; Fang, Q.; Huang, L.; Yan, X.; Zheng, X. Group-Based Trajectory Analysis for Postpartum Depression Symptoms among Chinese Primiparous Women. J. Clin. Med. 2022, 11, 6249. https://doi.org/10.3390/jcm11216249
Xiong J, Fang Q, Huang L, Yan X, Zheng X. Group-Based Trajectory Analysis for Postpartum Depression Symptoms among Chinese Primiparous Women. Journal of Clinical Medicine. 2022; 11(21):6249. https://doi.org/10.3390/jcm11216249
Chicago/Turabian StyleXiong, Juan, Qiyu Fang, Lingling Huang, Xinyi Yan, and Xujuan Zheng. 2022. "Group-Based Trajectory Analysis for Postpartum Depression Symptoms among Chinese Primiparous Women" Journal of Clinical Medicine 11, no. 21: 6249. https://doi.org/10.3390/jcm11216249
APA StyleXiong, J., Fang, Q., Huang, L., Yan, X., & Zheng, X. (2022). Group-Based Trajectory Analysis for Postpartum Depression Symptoms among Chinese Primiparous Women. Journal of Clinical Medicine, 11(21), 6249. https://doi.org/10.3390/jcm11216249