
Predictive Factors for Anastomotic Leakage after Laparoscopic and Open Total Gastrectomy: A Systematic Review

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Assessment of the Methodological Quality of Studies
3. Results
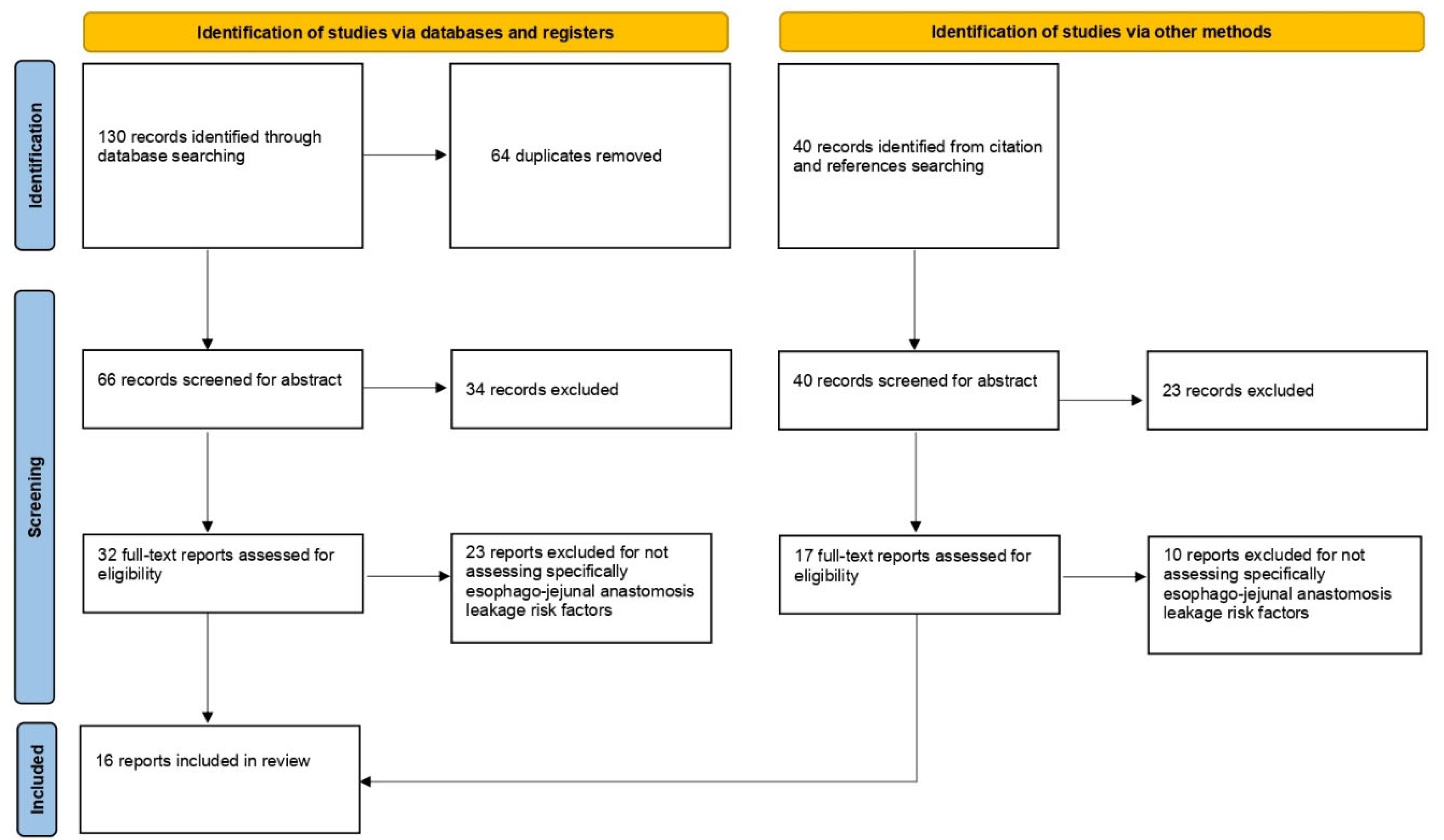
3.1. Search Strategy and Quality Assessment
3.2. Patients Related Factors
3.2.1. Age
3.2.2. Body Mass Index (BMI) and Obesity
3.2.3. Impaired Respiratory Function—American Society of Anesthesiology (ASA) Score
3.2.4. Preoperative Nutritional Status—Dysphagia and Gastric Stenosis
3.2.5. Alcohol Consumption, Diabetes and Chronic Renal Failure
3.2.6. Tumor Histology
3.3. Operative Factors
3.3.1. Laparoscopy

{kind=link}
| Reference | Year | Country | Period of Recruitment | Study Design | N | Minors Score |
|---|---|---|---|---|---|---|
| Barchi et al. [27] | 2019 | Brazil | 2009–2017 | Retrospective | 258 | 21 |
| Çetin et al. [28] | 2019 | Turkey | 2013–2016 | Retrospective | 80 | 18 |
| Deguchi et al. [18] | 2012 | Japan | 1999–2008 | Retrospective | 1640 | 10 |
| Kanaji et al. [13] | 2015 | Japan | 2008–2011 | Prospective | 185 | 17 |
| Kodera et al. [25] | 2019 | Japan | 2012–2013 | Retrospective | 1366 | 22 |
| Meyer et al. [21] | 2005 | Germany | 2002 | Prospective | 649 | 10 |
| Migita et al. [23] | 2012 | Japan | 2001–2011 | Retrospective | 327 | 12 |
| Oshi et al. [20] | 2018 | Japan | 2006–2014 | Retrospective | 131 | 18 |
| Rawicz et al. [24] | 2020 | Poland | 2016–2019 | Retrospective | 114 | 12 |
| Sakamoto et al. [26] | 2020 | Tokyo | 2012–2017 | Retrospective | 24,458 | 20 |
| Schietroma et al. [19] | 2013 | Italy | 2009–2012 | Prospective | 171 | 12 |
| Sierzega et al. [14] | 2010 | Poland | 1999–2004 | Retrospective | 690 | 12 |
| Sugiyama et al. [16] | 2017 | Japan | 2007–2014 | Retrospective | 215 | 16 |
| Takeuchi et al. [15] | 2016 | Japan | 2006–2015 | Retrospective | 65 | 12 |
| Trapani et al. [17] | 2020 | Italy | 2000–2018 | Retrospective | 1750 | 22 |
| Xing et al. [12] | 2021 | China | 2009–2019 | Retrospective | 390 | 18 |
| Reference | Surgical Approach | Surgery Intervention | Method of Esophagojejunostomy | Overall Leak Rate (%) | EJ Leakage Risk Factor Identified | Statistical Analysis |
|---|---|---|---|---|---|---|
| Barchi 2019 [27] | Open and laparoscopic | Completion gastrectomy: 50 Total gastrectomy: 208 | End-to-side circular stapler Laparoscopic: side-to-side endolinear stapler | 5.8 | Completion gastrectomy | Uni- and multivariate analysis |
| Cetin 2019 [28] | Open | Total gastrectomy: 80 | End-to-side circular stapler | 16.2 | Intraoperative time, additional organ resection | Uni- and multivariate analysis |
| Deguchi 2012 [18] | Open | Total gastrectomy: 1349 Proximal gastrectomy: 190 Completion gastrectomy: 101 | End-to-side circular stapler | 2.1 | Older pt (>65 years), pulmonary insufficiency, D2 or D2+ dissection, additional organ resection, omentum resection, thoracotomy, intraoperative blood transfusion, operative time and postoperative creatinine level | Uni- and multivariate analysis |
| Kanaji 2015 [13] | Open | Total gastrectomy: 185 | End-to-side circular stapler | 4.8 | Age ≥ 75, surgeon experienced <30 cases | Uni- and multivariate analysis |
| Kodera 2019 [25] | Open and laparoscopic | Total gastrectomy: 11,366 | x | OpenStageI: 3,6 Laparoscopic StageI: 5,4 Open Stage II–IV: 3.6 Laparoscopic StageII–IV: 5.7 | Laparoscopic approach | Comparison between matched cohorts |
| Meyer 2005 [21] | x | Total gastrectomy: 649 | Stapler Hand sewing | 5.5 | Preoperative dysphagia, gastric stenosis, positive (metastatic) lymph nodes, nicotine abuse, multivisceral resection | Uni- and multivariate analysis |
| Migita 2012 [23] | Open and laparoscopic | Total gastrectomy: 317 proximal gastrectomy: 10 | Circular stapler | 5.8 | HbA1c ≥ 7.0%, chronic renal failure, proximal gastrectomy, anastomotic troubles | Uni- and multivariate analysis |
| Oshi 2018 [20] | Laparoscopic | Total gastrectomy: 131 | End-to-side circular stapler OrVil | 9.9 | PNI 4 | Uni- and multivariate analysis |
| Rawicz 2020 [24] | Open and laparoscopic | Total gastrectomy and proximal gastrectomy: 114 | x | 4.6 | Mixed histological type of GC | Uni- and multivariate analysis |
| Sakamoto 2020 [26] | Open and laparoscopic | Total gastrectomy: 24,458 | x | Open 1,7; Laparoscopic: 2,9 | Laparoscopic approach | Comparison between matched cohorts |
| Schietroma 2013 [19] | Open | Total gastrectomy: 171 | Circular stapler Manual suture | 14.6 | Percentage of inspired oxygen, coexisting respiratory disease, ASA score ≥ 3, prolonged operative time | Uni- and multivariate analysis |
| Sierzega 2010 [14] | x | Total gastrectomy: 690 | Circular stapler | 5.9 | Splenectomy, pancreatectomy, age, ECOG 2–3 | Uni- and multivariate analysis |
| Sugiyama 2017 [16] | Laparoscopic | Total gastrectomy 215 | FE-EA 1 Circular stapler | FE-EA: 2.0; Circular stapler: 8.8 | BMI > 25, circular stapling anastomosis | Uni- and multivariate analysis |
| Takeuchi 2016 [15] | Open | Total gastrectomy: 75 | x | H-VFA 2: 23,1 L-VFA 3: 6,1 | H-VFA, age | Uni- and multivariate analysis |
| Trapani 2020 [17] | Open, laparoscopic and robotic | Total gastrectomy: 1750 | End to Side Side to side Partially Mechanical Totally Mechanical | 6.6 | Respiratory disease | Uni- and multivariate analysis |
| Xing 2021 [12] | Open and laparoscopic | Total gastrectomy: 390 | Circular stapler | 2.6 | Age > 65, Alcohol consumption of >2U/day | Uni- and multivariate analysis |
3.3.2. Anastomosis Type
3.3.3. Completion Gastrectomy
3.3.4. Additional Organ Resection—Extent of the Operation—Blood Loss
3.3.5. Intraoperative Time
3.3.6. Surgeon Experience
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sciuto, A.; Merola, G.; De Palma, G.D.; Sodo, M.; Pirozzi, F.; Bracale, U.M.; Bracale, U. Predictive factors for anastomotic leakage after laparoscopic colorectal surgery. World J. Gastroenterol. 2018, 24, 2247–2260. [Google Scholar] [CrossRef] [PubMed]
- Rahbari, N.N.; Weitz, J.; Hohenberger, W.; Heald, R.J.; Moran, B.; Ulrich, A.; Holm, T.; Wong, W.D.; Tiret, E.; Moriya, Y.; et al. Definition and grading of anastomotic leakage following anterior resection of the rectum: A proposal by the International Study Group of Rectal Cancer. Surgery 2010, 147, 339–351. [Google Scholar] [CrossRef] [PubMed]
- Milone, M.; Elmore, U.; Allaix, M.E.; Bianchi, P.P.; Biondi, A.; Boni, L.; Bracale, U.; Cassinotti, E.; Ceccarelli, G.; Corcione, F.; et al. Fashioning enterotomy closure after totally laparoscopic ileocolic anastomosis for right colon cancer: A multicenter experience. Surg. Endosc. 2020, 34, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Peel, A.L.; Taylor, E.W. Proposed definitions for the audit of postoperative infection: A discussion paper. Surgical Infection Study Group. Ann. R. Coll. Surg. Engl. 1991, 73, 385–388. [Google Scholar]
- Milone, M.; Elmore, U.; Musella, M.; Parise, P.; Zotti, M.C.; Bracale, U.; Di Lauro, K.; Manigrasso, M.; Milone, F.; Rosati, R. Safety and efficacy of laparoscopic wedge gastrectomy for large gastrointestinal stromal tumors. Eur. J. Surg. Oncol. 2017, 43, 796–800. [Google Scholar] [CrossRef] [PubMed]
- Bracale, U.; Pignata, G.; Lirici, M.M.; Hüscher, C.G.S.; Pugliese, R.; Sgroi, G.; Romano, G.; Spinoglio, G.; Gualtierotti, M.; Maglione, V.; et al. Guideline Committee Of The Italian Society Of Hospital Surgeons-ACOI and Italian Hi-Tech Surgical Club-IHTSC. Laparoscopic gastrectomies for cancer: The ACOI-IHTSC national guidelines. Minim. Invasive Ther. Allied Technol. 2012, 21, 313–319. [Google Scholar] [CrossRef]
- Bracale, U.; Corcione, F.; Pignata, G.; Andreuccetti, J.; Dolce, P.; Boni, L.; Cassinotti, E.; Olmi, S.; Uccelli, M.; Gualtierotti, M.; et al. Impact of neoadjuvant therapy followed by laparoscopic radical gastrectomy with D2 lymph node dissection in Western population: A multi-institutional propensity score-matched study. J. Surg. Oncol. 2021, 124, 1338–1346. [Google Scholar] [CrossRef]
- Inokuchi, M.; Otsuki, S.; Fujimori, Y.; Sato, Y.; Nakagawa, M.; Kojima, K. Systematic review of anastomotic complications of esophagojejunostomy after laparoscopic total gastrectomy. World J. Gastroenterol. 2015, 21, 9656–9665. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.M.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef] [PubMed]
- Xing, J.; Liu, M.; Qi, X.; Yu, J.; Fan, Y.; Xu, K.; Gao, P.; Tan, F.; Yao, Z.; Zhang, N.; et al. Risk factors for esophagojejunal anastomotic leakage after curative total gastrectomy combined with D2 lymph node dissection for gastric cancer. J. Int. Med. Res. 2021, 49, 3000605211000883. [Google Scholar] [CrossRef] [PubMed]
- Kanaji, S.; Ohyama, M.; Yasuda, T.; Sendo, H.; Suzuki, S.; Kawasaki, K.; Tanaka, K.; Fujino, Y.; Tominaga, M.; Kakeji, Y. Can the intraoperative leak test prevent postoperative leakage of esophagojejunal anastomosis after total gastrectomy? Surg. Today 2016, 46, 815–820. [Google Scholar] [CrossRef] [PubMed]
- Sierzega, M.; Kolodziejczyk, P.; Kulig, J.; Polish Gastric Cancer Study Group. Impact of anastomotic leakage on long-term survival after total gastrectomy for carcinoma of the stomach. Br. J. Surg. 2010, 97, 1035–1042. [Google Scholar] [CrossRef]
- Takeuchi, M.; Ishii, K.; Seki, H.; Yasui, N.; Sakata, M.; Shimada, A.; Matsumoto, H. Excessive visceral fat area as a risk factor for early postoperative complications of total gastrectomy for gastric cancer: A retrospective cohort study. BMC Surg. 2016, 16, 54. [Google Scholar] [CrossRef]
- Sugiyama, M.; Oki, E.; Ogaki, K.; Morita, M.; Sakaguchi, Y.; Koga, S.; Saeki, H.; Maehara, Y. Clinical Outcomes of Esophagojejunostomy in Totally Laparoscopic Total Gastrectomy: A Multicenter Study. Surg. Laparosc. Endosc. Percutan. Tech. 2017, 27, e87–e91. [Google Scholar] [CrossRef]
- Trapani, R.; Rausei, S.; Reddavid, R.; Degiuli, M.; ITALIAN RESEARCH GROUP FOR GASTRIC CANCER (GIRCG) Clinical Investigators. Risk factors for esophago-jejunal anastomosis leakage after total gastrectomy for cancer. A multicenter retrospective study of the Italian research group for gastric cancer. Eur. J. Surg. Oncol. 2020, 46, 2243–2247. [Google Scholar] [CrossRef]
- Deguchi, Y.; Fukagawa, T.; Morita, S.; Ohashi, M.; Saka, M.; Katai, H. Identification of risk factors for esophagojejunal anastomotic leakage after gastric surgery. World J. Surg. 2012, 36, 1617–1622. [Google Scholar] [CrossRef]
- Schietroma, M.; Cecilia, E.M.; Carlei, F.; Sista, F.; De Santis, G.; Piccione, F.; Amicucci, G. Prevention of anastomotic leakage after total gastrectomy with perioperative supplemental oxygen administration: A prospective randomized, double-blind, controlled, single-center trial. Ann. Surg. Oncol. 2013, 20, 1584–1590. [Google Scholar] [CrossRef]
- Oshi, M.; Kunisaki, C.; Miyamoto, H.; Kosaka, T.; Akiyama, H.; Endo, I. Risk Factors for Anastomotic Leakage of Esophagojejunostomy after Laparoscopy-Assisted Total Gastrectomy for Gastric Cancer. Dig. Surg. 2018, 35, 28–34. [Google Scholar] [CrossRef]
- Meyer, L.; Meyer, F.; Dralle, H.; Ernst, M.; Lippert, H.; Gastinger, I.; East German Study Group for Quality Control in Operative Medicine and Regional Development in Surgery. Insufficiency risk of esophagojejunal anastomosis after total abdominal gastrectomy for gastric carcinoma. Langenbeck’s Arch. Surg. 2005, 390, 510–516. [Google Scholar] [CrossRef] [PubMed]
- Tønnesen, H.; Schütten, B.T.; Jørgensen, B.B. Influence of alcohol on morbidity after colonic surgery. Dis. Colon Rectum 1987, 30, 549–551. [Google Scholar] [CrossRef] [PubMed]
- Migita, K.; Takayama, T.; Matsumoto, S.; Wakatsuki, K.; Enomoto, K.; Tanaka, T.; Ito, M.; Nakajima, Y. Risk factors for esophagojejunal anastomotic leakage after elective gastrectomy for gastric cancer. J. Gastrointest. Surg. 2012, 16, 1659–1665. [Google Scholar] [CrossRef] [PubMed]
- Rawicz-Pruszyński, K.; Sędłak, K.; Mlak, R.; Mielko, J.; Polkowski, W.P. Mixed Type Histology as a Predictive Factor for Esophagojejunostomy Leak in Advanced Gastric Cancer. Cancers 2020, 12, 1701. [Google Scholar] [CrossRef] [PubMed]
- Kodera, Y.; Yoshida, K.; Kumamaru, H.; Kakeji, Y.; Hiki, N.; Etoh, T.; Honda, M.; Miyata, H.; Yamashita, Y.; Seto, Y.; et al. Introducing laparoscopic total gastrectomy for gastric cancer in general practice: A retrospective cohort study based on a nationwide registry database in Japan. Gastric Cancer 2019, 22, 202–213. [Google Scholar] [CrossRef]
- Sakamoto, T.; Fujiogi, M.; Matsui, H.; Fushimi, K.; Yasunaga, H. Short-Term Outcomes of Laparoscopic and Open Total Gastrectomy for Gastric Cancer: A Nationwide Retrospective Cohort Analysis. Ann. Surg. Oncol. 2020, 27, 518–526. [Google Scholar] [CrossRef]
- Barchi, L.C.; Ramos, M.F.K.P.; Pereira, M.A.; Dias, A.R.; Ribeiro-Júnior, U.; Zilberstein, B.; Cecconello, I. Esophagojejunal anastomotic fistula: A major issue after radical total gastrectomy. Updates Surg. 2019, 71, 429–438. [Google Scholar] [CrossRef]
- Çetin, D.A.; Gündeş, E.; Çiyiltepe, H.; Aday, U.; Uzun, O.; Değer, K.C.; Duman, M. Risk factors and laboratory markers used to predict leakage in esophagojejunal anastomotic leakage after total gastrectomy. Turk. J. Surg. 2019, 35, 1–6. [Google Scholar] [CrossRef][Green Version]
- van der Wielen, N.; Straatman, J.; Daams, F.; Rosati, R.; Parise, P.; Weitz, J.; Reissfelder, C.; Diez Del Val, I.; Loureiro, C.; Parada-González, P.; et al. Open versus minimally invasive total gastrectomy after neoadjuvant chemotherapy: Results of a European randomized trial. Gastric Cancer 2021, 24, 258–271. [Google Scholar] [CrossRef]
- Isozaki, H.; Okajima, K.; Ichinona, T.; Hara, H.; Fujii, K.; Nomura, E. Risk factors of esophagojejunal anastomotic leakage after total gastrectomy for gastric cancer. Hepatogastroenterology 1997, 44, 1509–1512. [Google Scholar]
- Tonouchi, H.; Mohri, Y.; Tanaka, K.; Ohi, M.; Kobayashi, M.; Yamakado, K.; Kusunoki, M. Diagnostic sensitivity of contrast swallow for leakage after gastric resection. World J. Surg. 2007, 31, 128–131. [Google Scholar] [CrossRef] [PubMed]
- Lang, H.; Piso, P.; Stukenborg, C.; Raab, R.; Jähne, J. Management and results of proximal anastomotic leaks in a series of 1114 total gastrectomies for gastric carcinoma. Eur. J. Surg. Oncol. 2000, 26, 168–171. [Google Scholar] [CrossRef] [PubMed]
- Sauvanet, A.; Mariette, C.; Thomas, P.; Lozac’h, P.; Segol, P.; Tiret, E.; Delpero, J.-R.; Collet, D.; Leborgne, J.; Pradère, B.; et al. Mortality and morbidity after resection for adenocarcinoma of the gastroesophageal junction: Predictive factors. J. Am. Coll. Surg. 2005, 201, 253–262. [Google Scholar] [CrossRef]
- Carboni, F.; Valle, M.; Federici, O.; Levi Sandri, G.B.; Camperchioli, I.; Lapenta, R.; Assisi, D.; Garofalo, A. Esophagojejunal anastomosis leakage after total gastrectomy for esophagogastric junction adenocarcinoma: Options of treatment. J. Gastrointest. Oncol. 2016, 7, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, K.; Yanaga, K.; Kashiwagi, H.; Hanyuu, N.; Iwabuchi, S. Significance of intraoperative endoscopy in total gastrectomy for gastric cancer. Surg. Endosc. 2010, 24, 2633–2636. [Google Scholar] [CrossRef]
- Yan, Y.; Yang, A.; Lu, L.; Zhao, Z.; Li, C.; Li, W.; Chao, J.; Liu, T.; Fong, Y.; Fu, W.; et al. Impact of Neoadjuvant Therapy on Minimally Invasive Surgical Outcomes in Advanced Gastric Cancer: An International Propensity Score-Matched Study. Ann. Surg. Oncol. 2021, 28, 1428–1436. [Google Scholar] [CrossRef]
- Makuuchi, R.; Irino, T.; Tanizawa, Y.; Bando, E.; Kawamura, T.; Terashima, M. Esophagojejunal anastomotic leakage following gastrectomy for gastric cancer. Surg. Today 2019, 49, 187–196. [Google Scholar] [CrossRef]
- Mortensen, K.; Nilsson, M.; Slim, K.; Schäfer, M.; Mariette, C.; Braga, M.; Carli, F.; Demartines, N.; Griffin, S.M.; Lassen, K.; et al. Consensus guidelines for enhanced recovery after gastrectomy. Br. J. Surg. 2014, 101, 1209–1229. [Google Scholar] [CrossRef]
- Haga, Y.; Wada, Y.; Takeuchi, H.; Kimura, O.; Furuya, T.; Sameshima, H.; Ishikawa, M. Estimation of physiologic ability and surgical stress (E-PASS) for a surgical audit in elective digestive surgery. Surgery 2004, 135, 586–594. [Google Scholar] [CrossRef]
- Bozzetti, F.; on behalf of the SCRINIO Working Group. Screening the nutritional status in oncology: A preliminary report on 1000 outpatients. Support. Care Cancer 2009, 17, 279–284. [Google Scholar] [CrossRef]
- Rosania, R.; Chiapponi, C.; Malfertheiner, P.; Venerito, M. Nutrition in Patients with Gastric Cancer: An Update. Gastrointest. Tumors 2015, 2, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Gianotti, L.; Braga, M.; Nespoli, L.; Radaelli, G.; Beneduce, A.; Di Carlo, V. A randomized controlled trial of preoperative oral supplementation with a specialized diet in patients with gastrointestinal cancer. Gastroenterology 2002, 122, 1763–1770. [Google Scholar] [CrossRef]
- Rullier, E.; Laurent, C.; Garrelon, J.L.; Michel, P.; Saric, J.; Parneix, M. Risk factors for anastomotic leakage after resection of rectal cancer. Br. J. Surg. 1998, 85, 355–358. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, L.T.; Jørgensen, T.; Kirkeby, L.T.; Skovdal, J.; Vennits, B.; Wille-Jørgensen, P. Smoking and alcohol abuse are major risk factors for anastomotic leakage in colorectal surgery. Br. J. Surg. 1999, 86, 927–931. [Google Scholar] [CrossRef] [PubMed]
- Black, E.; Vibe-Petersen, J.; Jorgensen, L.N.; Madsen, S.M.; Agren, M.S.; Holstein, P.E.; Perrild, H.; Gottrup, F. Decrease of collagen deposition in wound repair in type 1 diabetes independent of glycemic control. Arch. Surg. 2003, 138, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Onodera, H.; Ikeuchi, D.; Nagayama, S.; Imamura, M. Weakness of anastomotic site in diabetic rats is caused by changes in the integrity of newly formed collagen. Dig. Surg. 2004, 21, 146–151. [Google Scholar] [CrossRef]
- Bracale, U.; Pacelli, F.; Milone, M.; Bracale, U.M.; Sodo, M.; Merola, G.; Troiani, T.; Di Salvo, E. Laparoscopic treatment of abdominal unicentric castleman’s disease: A case report and literature review. BMC Surg. 2017, 17, 38. [Google Scholar] [CrossRef]
- Azioni, G.; Bracale, U.; Scala, A.; Capobianco, F.; Barone, M.; Rosati, M.; Pignata, G. Laparoscopic ureteroneocystostomy and vesicopsoas hitch for infiltrative ureteral endometriosis. Minim. Invasive Ther. Allied Technol. 2010, 19, 292–297. [Google Scholar] [CrossRef]
- Etoh, T.; Honda, M.; Kumamaru, H.; Miyata, H.; Yoshida, K.; Kodera, Y.; Kakeji, Y.; Inomata, M.; Konno, H.; Seto, Y.; et al. Morbidity and mortality from a propensity score-matched, prospective cohort study of laparoscopic versus open total gastrectomy for gastric cancer: Data from a nationwide web-based database. Surg. Endosc. 2018, 32, 2766–2773. [Google Scholar] [CrossRef]
- Kawamura, H.; Ohno, Y.; Ichikawa, N.; Yoshida, T.; Homma, S.; Takahashi, M.; Taketomi, A. Anastomotic complications after laparoscopic total gastrectomy with esophagojejunostomy constructed by circular stapler (OrVil™) versus linear stapler (overlap method). Surg. Endosc. 2017, 31, 5175–5182. [Google Scholar] [CrossRef]
- Kosuga, T.; Hiki, N.; Nunobe, S.; Ohashi, M.; Kubota, T.; Kamiya, S.; Sano, T.; Yamaguchi, T. Does the Single-Stapling Technique for Circular-Stapled Esophagojejunostomy Reduce Anastomotic Complications After Laparoscopic Total Gastrectomy? Ann. Surg. Oncol. 2015, 22, 3606–3612. [Google Scholar] [CrossRef] [PubMed]
- Kodera, Y.; Sasako, M.; Yamamoto, S.; Sano, T.; Nashimoto, A.; Kurita, A. Identification of risk factors for the development of complications following extended and superextended lymphadenectomies for gastric cancer. Br. J. Surg. 2005, 92, 1103–1109. [Google Scholar] [CrossRef] [PubMed]
- Lo, C.H.; Chen, J.H.; Wu, C.W.; Lo, S.S.; Hsieh, M.C.; Lui, W.Y. Risk factors and management of intra-abdominal infection after extended radical gastrectomy. Am. J. Surg. 2008, 196, 741–745. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, K.; Shiraishi, N.; Adachi, Y.; Inomata, M.; Sato, K.; Kitano, S. Risk factors for complications following resection of large gastric cancer. Br. J. Surg. 2001, 88, 873–877. [Google Scholar] [CrossRef] [PubMed]
- Koliarakis, I.; Athanasakis, E.; Sgantzos, M.; Mariolis-Sapsakos, T.; Xynos, E.; Chrysos, E.; Souglakos, J.; Tsiaoussis, J. Intestinal Microbiota in Colorectal Cancer Surgery. Cancers 2020, 12, 3011. [Google Scholar] [CrossRef] [PubMed]
- Reddy, R.M.; Weir, W.B.; Barnett, S.; Heiden, B.T.; Orringer, M.B.; Lin, J.; Chan, A.C.; Carrott, P.W.; Lynch, W.R.; Beer, D.G.; et al. Increased Variance in Oral and Gastric Microbiome Correlates With Esophagectomy Anastomotic Leak. Ann. Thorac. Surg. 2018, 105, 865–870. [Google Scholar] [CrossRef]
- Schardey, H.M.; Joosten, U.; Finke, U.; Staubach, K.H.; Schauer, R.; Heiss, A.; Kooistra, A.; Rau, H.G.; Nibler, R.; Lüdeling, S.; et al. The prevention of anastomotic leakage after total gastrectomy with local decontamination. A prospective, randomized, double-blind, placebo-controlled multicenter trial. Ann. Surg. 1997, 225, 172–178. [Google Scholar] [CrossRef]
- Farran, L.; Llop, J.; Sans, M.; Kreisler, E.; Miró, M.; Galan, M.; Rafecas, A. Efficacy of enteral decontamination in the prevention of anastomotic dehiscence and pulmonary infection in esophagogastric surgery. Dis. Esophagus 2008, 21, 159–164. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bracale, U.; Peltrini, R.; De Luca, M.; Ilardi, M.; Di Nuzzo, M.M.; Sartori, A.; Sodo, M.; Danzi, M.; Corcione, F.; De Werra, C. Predictive Factors for Anastomotic Leakage after Laparoscopic and Open Total Gastrectomy: A Systematic Review. J. Clin. Med. 2022, 11, 5022. https://doi.org/10.3390/jcm11175022
Bracale U, Peltrini R, De Luca M, Ilardi M, Di Nuzzo MM, Sartori A, Sodo M, Danzi M, Corcione F, De Werra C. Predictive Factors for Anastomotic Leakage after Laparoscopic and Open Total Gastrectomy: A Systematic Review. Journal of Clinical Medicine. 2022; 11(17):5022. https://doi.org/10.3390/jcm11175022
Chicago/Turabian StyleBracale, Umberto, Roberto Peltrini, Marcello De Luca, Mariangela Ilardi, Maria Michela Di Nuzzo, Alberto Sartori, Maurizio Sodo, Michele Danzi, Francesco Corcione, and Carlo De Werra. 2022. "Predictive Factors for Anastomotic Leakage after Laparoscopic and Open Total Gastrectomy: A Systematic Review" Journal of Clinical Medicine 11, no. 17: 5022. https://doi.org/10.3390/jcm11175022
APA StyleBracale, U., Peltrini, R., De Luca, M., Ilardi, M., Di Nuzzo, M. M., Sartori, A., Sodo, M., Danzi, M., Corcione, F., & De Werra, C. (2022). Predictive Factors for Anastomotic Leakage after Laparoscopic and Open Total Gastrectomy: A Systematic Review. Journal of Clinical Medicine, 11(17), 5022. https://doi.org/10.3390/jcm11175022