
Uterine Factor Infertility, a Systematic Review

 , , ,
, , ,  ,
,
Abstract
1. Introduction
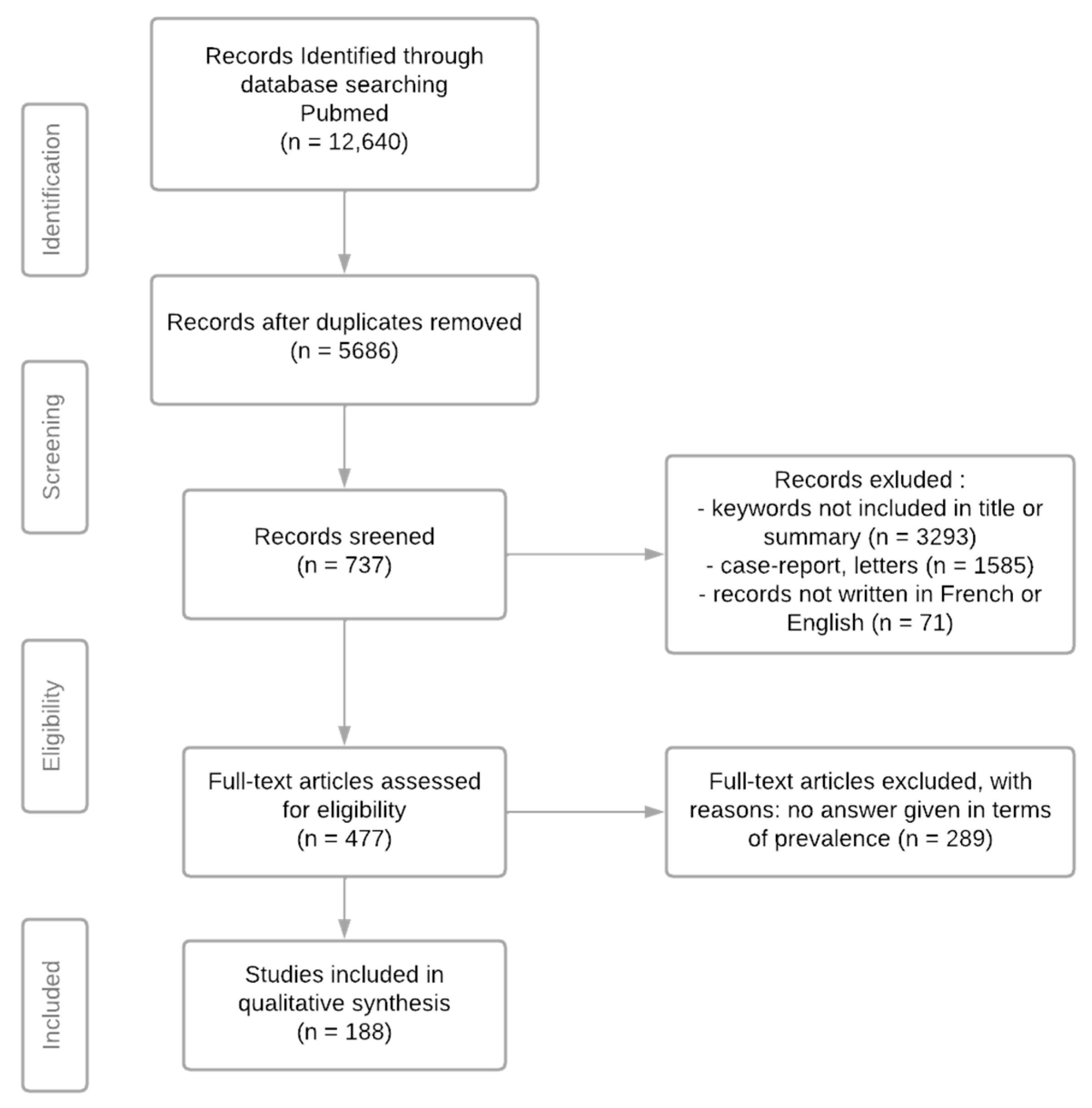
2. Materials and Methods
- -
- Congenital: uterine agenesis (MRKH syndrome, complete androgen insensitivity syndrome (CAIS));
- -
- Acquired: hemostasis hysterectomy (postpartum hysterectomy), hysterectomy for benign conditions (polymyomatous uterus, endometriosis, adenomyosis, functional menorrhagia, pelvic statics disorder), carcinological hysterectomy (ovarian, endometrial or cervical cancer).
- -
- Congenital: uterine malformations, Distilbene® uterus;
- -
- Acquired: uterine irradiation, adenomyosis, synechiae and Asherman’s syndrome, myomas, polyps.
- -
- “uterine factor infertility”;
- -
- “uterus transplantation”;
- -
- “adenomyosis [and] infertility”;
- -
- “uterus agenesis [and/or] MRKH syndroma [and/or] complete androgen insensitivity syndroma [and] infertility”;
- -
- “hysterectomy [and] prevalence [and/or] incidence”;
- -
- “uterus malformation [and/or] hypoplastic uterus [and/or] uterus septa [and/or] DES uterus [and] infertility”;
- -
- “uterine myomas [and] infertility”;
- -
- “uterine polyp [and] infertility”;
- -
- “uterine synechia [and] infertility”;
- -
- “uterus radiation [and] infertility”.
3. Results
3.1. Uterine Factor Infertility: General Data
3.2. Uterine Agenesia
3.3. Hysterectomies
3.4. Uterine Malformations
3.5. Radiation-Induced Uterine Condition
3.6. Adenomyosis
3.7. Synechiae and Asherman Syndrome
3.8. Uterine Myomas
3.9. Uterine Polyps
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Assistance Médicale à la Procréation (AMP). Inserm-La Science Pour la Santé n.d. Available online: https://www.inserm.fr/information-en-sante/dossiers-information/assistance-medicale-procreation-amp (accessed on 7 August 2019).
- Akhter, S.; Alam, H.; Khanam, N.N.; Zabin, F. Characteristics of infertile couples. Mymensingh Med. J. 2011, 20, 121–127. [Google Scholar] [PubMed]
- Elhussein, O.G.; Ahmed, M.A.; Suliman, S.O.; Yahya, L.I.; Adam, I. Epidemiology of infertility and characteristics of infertile couples requesting assisted reproduction in a low-resource setting in Africa, Sudan. Fertil. Res. Pract. 2019, 5, 7. [Google Scholar] [CrossRef] [PubMed]
- Ümit, G.; Izetbegovic, S.; Admir, R.; Spahovic, H.; Cihan, G. Causes of Sterility in Bosnia-Herzegovina Population. Mater. Socio-Med. 2015, 27, 185–187. [Google Scholar] [CrossRef]
- Brännström, M.; Johannesson, L.; Dahm-Kähler, P.; Enskog, A.; Mölne, J.; Kvarnström, N.; Diaz-Garcia, C.; Hanafy, A.; Lundmark, C.; Marcickiewicz, J.; et al. First clinical uterus transplantation trial: A six-month report. Fertil. Steril. 2014, 101, 1228–1236. [Google Scholar] [CrossRef]
- Hur, C.; Rehmer, J.; Flyckt, R.; Falcone, T. Uterine Factor Infertility: A Clinical Review. Clin. Obstet. Gynecol. 2019, 62, 257–270. [Google Scholar] [CrossRef]
- Hatasaka, H. Clinical Management of the Uterine Factor in Infertility. Clin. Obstet. Gynecol. 2011, 54, 696–709. [Google Scholar] [CrossRef]
- Taylor, E.; Gomel, V. The uterus and fertility. Fertil. Steril. 2008, 89, 1–16. [Google Scholar] [CrossRef]
- Jones, B.P.; Kasaven, L.; Vali, S.; Saso, S.; Jalmbrant, M.; Bracewell-Milnes, T.; Thum, M.-Y.; Quiroga, I.; Friend, P.; Diaz-Garcia, C.; et al. Uterine Transplantation: Review of Livebirths and Reproductive Implications. Transplantation 2021, 105, 1695–1707. [Google Scholar] [CrossRef]
- Jones, B.P.; Kasaven, L.S.; Chan, M.; Vali, S.; Saso, S.; Bracewell-Milnes, T.; Thum, M.-Y.; Nicopoullos, J.; Diaz-Garcia, C.; Quiroga, I.; et al. Uterine Transplantation in 2021: Recent Developments and the Future. Clin. Obstet. Gynecol. 2022, 65, 4–14. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- NewCastleOttawaScale. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 22 July 2022).
- Benbella, A.; Aboulmakarim, S.; Hardizi, H.; Zaidouni, A.; Bezad, R. Infertility in the Moroccan population: An etiological study in the reproductive health centre in Rabat. Pan Afr. Med. J. 2018, 30. [Google Scholar] [CrossRef]
- Masoumi, S.Z.; Parsa, P.; Darvish, N.; Mokhtari, S.; Yavangi, M.; Roshanaei, G. An epidemiologic survey on the causes of infertility in patients referred to infertility center in Fatemieh Hospital in Hamadan. Iran. J. Reprod. Med. 2015, 13, 513–516. [Google Scholar] [PubMed]
- Meng, Q.; Ren, A.; Zhang, L.; Liu, J.; Li, Z.; Yang, Y.; Li, R.; Ma, L. Incidence of infertility and risk factors of impaired fecundity among newly married couples in a Chinese population. Reprod. Biomed. Online 2015, 30, 92–100. [Google Scholar] [CrossRef]
- Herlin, M.; Bjørn, A.-M.B.; Rasmussen, M.; Trolle, B.; Petersen, M.B. Prevalence and patient characteristics of Mayer–Rokitansky–Küster–Hauser syndrome: A nationwide registry-based study. Hum. Reprod. 2016, 31, 2384–2390. [Google Scholar] [CrossRef]
- Hughes, I.A.; Davies, J.D.; Bunch, T.I.; Pasterski, V.; Mastroyannopoulou, K.; MacDougall, J. Androgen insensitivity syndrome. Lancet Lond. Engl. 2012, 380, 1419–1428. [Google Scholar] [CrossRef]
- Boehmer, A.L.; Brinkmann, O.; Brüggenwirth, H.; van Assendelft, C.; Otten, B.J.; Verleun-Mooijman, M.C.; Niermeijer, M.F.; Brunner, H.G.; Rouwé, C.W.; Waelkens, J.J.; et al. Genotype versus phenotype in families with androgen insensitivity syndrome. J. Clin. Endocrinol. Metab. 2001, 86, 4151–4160. [Google Scholar] [CrossRef] [PubMed]
- Sarpel, U.; Palmer, S.K.; Dolgin, S.E. The incidence of complete androgen insensitivity in girls with inguinal hernias and assessment of screening by vaginal length measurement. J. Pediatr. Surg. 2005, 40, 133–136, discussion 136–137. [Google Scholar] [CrossRef]
- Cooper, R.; Lawlor, D.A.; Hardy, R.; Ebrahim, S.; Leon, D.A.; Wadsworth, M.E.J.; Kuh, D. Socio-economic position across the life course and hysterectomy in three British cohorts: A cross-cohort comparative study. BJOG Int. J. Obstet. Gynaecol. 2005, 112, 1126–1133. [Google Scholar] [CrossRef]
- Desai, S.; Campbell, O.M.; Sinha, T.; Mahal, A.; Cousens, S. Incidence and determinants of hysterectomy in a low-income setting in Gujarat, India. Health Policy Plan. 2017, 32, 68–78. [Google Scholar] [CrossRef]
- Hammer, A.; Kahlert, J.; Gravitt, P.E.; Rositch, A.F. Hysterectomy-corrected cervical cancer mortality rates in Denmark during 2002–2015: A registry-based cohort study. Acta Obstet. Gynecol. Scand. 2019, 98, 1063–1069. [Google Scholar] [CrossRef]
- Hammer, A.; Kahlert, J.; Rositch, A.; Pedersen, L.; Gravitt, P.; Blaakaer, J.; Soegaard, M. The temporal and age-dependent patterns of hysterectomy-corrected cervical cancer incidence rates in Denmark: A population-based cohort study. Acta Obstet. Gynecol. Scand. 2017, 96, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Hill, E.L.; Graham, M.L.; Shelley, J.M. Hysterectomy trends in Australia-between 2000/01 and 2004/05. Aust. N. Z. J. Obstet. Gynaecol. 2010, 50, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Babalola, E.O.; Bharucha, A.E.; Schleck, C.D.; Gebhart, J.B.; Zinsmeister, A.R.; Melton, L.J. Decreasing utilization of hysterectomy. Am. J. Obstet. Gynecol. 2007, 196, 214.e1–214.e7. [Google Scholar] [CrossRef][Green Version]
- Merrill, R.M. Prevalence Corrected Hysterectomy Rates and Probabilities in Utah. Ann. Epidemiol. 2001, 11, 127–135. [Google Scholar] [CrossRef]
- Redburn, J.C.; Murphy, M.F.G. Hysterectomy prevalence and adjusted cervical and uterine cancer rates in England and Wales. BJOG Int. J. Obstet. Gynaecol. 2001, 108, 388–395. [Google Scholar] [CrossRef] [PubMed]
- Wilson, L.F.; Pandeya, N.; Mishra, G.D. Hysterectomy trends in Australia, 2000–2001 to 2013–2014: Joinpoint regression analysis. Acta Obstet. Gynecol. Scand. 2017, 96, 1170–1179. [Google Scholar] [CrossRef] [PubMed]
- Beckmann, K.; Iosifidis, P.; Shorne, L.; Gilchrist, S.; Roder, D. Effects of variations in hysterectomy status on population coverage by cervical screening. Aust. N. Z. J. Public Health 2003, 27, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Bower, J.K.; Schreiner, P.J.; Sternfeld, B.; Lewis, C.E. Black–White Differences in Hysterectomy Prevalence: The CARDIA Study. Am. J. Public Health 2009, 99, 300–307. [Google Scholar] [CrossRef]
- Desai, S.; Shuka, A.; Nambiar, D.; Ved, R. Patterns of hysterectomy in India: A national and state-level analysis of the Fourth National Family Health Survey (2015–2016). BJOG: Int. J. Obstet. Gynaecol. 2019, 126, 72–80. [Google Scholar] [CrossRef]
- Gartner, D.R.; Delamater, P.L.; Hummer, R.A.; Lund, J.L.; Pence, B.W.; Robinson, W.R. Integrating Surveillance Data to Estimate Race/Ethnicity-specific Hysterectomy Inequalities Among Reproductive-aged Women: Who’s at Risk? Epidemiology 2020, 31, 385–392. [Google Scholar] [CrossRef]
- Liu, F.; Pan, Y.; Liang, Y.; Zhang, C.; Deng, Q.; Li, X.; Liu, M.; He, Z.; Liu, Y.; Li, J.; et al. The epidemiological profile of hysterectomy in rural Chinese women: A population-based study. BMJ Open 2017, 7, e015351. [Google Scholar] [CrossRef] [PubMed]
- Merrill, R.M. Hysterectomy Surveillance in the United States, 1997 through 2005. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2008, 14, CR24–CR31. [Google Scholar]
- Merrill, R.M.; Layman, A.B.; Oderda, G.; Asche, C. Risk Estimates of Hysterectomy and Selected Conditions Commonly Treated with Hysterectomy. Ann. Epidemiol. 2008, 18, 253–260. [Google Scholar] [CrossRef]
- Rositch, A.F.; Nowak, R.G.; Gravitt, P.E. Increased Age and Race-Specific Incidence of Cervical Cancer After Correction for Hysterectomy Prevalence in the United States From 2000 to 2009. Cancer 2014, 120, 2032–2038. [Google Scholar] [CrossRef] [PubMed]
- Ruiz de Azua Unzurrunzaga, G.; Brewster, D.H.; Wild, S.H.; Sivalingam, V.N. Declining hysterectomy prevalence and the estimated impact on uterine cancer incidence in Scotland. Cancer Epidemiol. 2019, 59, 227–231. [Google Scholar] [CrossRef]
- Shekhar, C.; Paswan, B.; Singh, A. Prevalence, sociodemographic determinants and self-reported reasons for hysterectomy in India. Reprod. Health 2019, 16, 118. [Google Scholar] [CrossRef] [PubMed]
- Temkin, S.M.; Kohn, E.C.; Penberthy, L.; Cronin, K.A.; Rubinsak, L.; Dickie, L.A.; Minasian, L.; Noone, A.-M. Hysterectomy-corrected rates of endometrial cancer among women younger than age 50 in the United States. Cancer Causes Control 2018, 29, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Meher, T.; Sahoo, H. Regional pattern of hysterectomy among women in India: Evidence from a recent large scale survey. Women Health 2020, 60, 585–600. [Google Scholar] [CrossRef]
- Meher, T.; Sahoo, H. Changing trends in the preference of health care facility and reasons for hysterectomy in India. Health Care Women Int. 2020, 41, 802–816. [Google Scholar] [CrossRef]
- Prusty, R.K.; Choithani, C.; Gupta, S.D. Predictors of hysterectomy among married women 15–49 years in India. Reprod. Health 2018, 15, 3. [Google Scholar] [CrossRef]
- Lai, J.C.-Y.; Huang, N.; Huang, S.-M.; Hu, H.-Y.; Wang, C.-W.; Chou, Y.-J.; Wang, K.-L. Decreasing trend of hysterectomy in Taiwan: A population-based study, 1997–2010. Taiwan J. Obstet. Gynecol. 2015, 54, 512–518. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Ding, T.; Luo, A.; Lu, Y.; Ma, D.; Wang, S. Comparison of surgical indications for hysterectomy by age and approach in 4653 Chinese women. Front. Med. 2014, 8, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Chen, I.; Wise, M.R.; Dunn, S.; Anderson, G.; Degani, N.; Lefebvre, G.; Bierman, A.S. Social and Geographic Determinants of Hysterectomy in Ontario: A Population-Based Retrospective Cross-Sectional Analysis. J. Obstet. Gynaecol. Can. 2017, 39, 861–869. [Google Scholar] [CrossRef]
- Parazzini, F.; Ricci, E.; Bulfoni, G.; Cipriani, S.; Chiaffarino, F.; Malvezzi, M.; Frigerio, L. Hysterectomy rates for benign conditions are declining in Lombardy, Italy: 1996–2010. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 178, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Sebitloane, M.H.; Moodley, J. Moodley Emergency peripartum hysterectomy. East Afr. Med. J. 2001, 78, 70–74. [Google Scholar] [CrossRef][Green Version]
- Heitkamp, A.; Seinstra, J.; Akker, T.; Vollmer, L.; Gebhardt, S.; Roosmalen, J.; Vries, J.I.; Theron, G. A district-wide population-based descriptive study of emergency peripartum hysterectomy in a middle-income country. Int. J. Gynecol. Obstet. 2019, 146, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Abasiattai, A.M.; Umoiyoho, A.J.; Utuk, N.M.; Inyang-Etoh, E.C.; Asuquo, O.P. Emergency peripartum hysterectomy in a tertiary hospital in southern Nigeria. Pan Afr. Med. J. 2013, 15. [Google Scholar] [CrossRef]
- Okogbenin, S.; Gharoro, E.; Otoide, V.; Okonta, P. Obstetric hysterectomy: Fifteen years’ experience in a Nigerian tertiary centre. J. Obstet. Gynaecol. 2003, 23, 356–359. [Google Scholar] [CrossRef]
- Akintayo, A.A.; Olagbuji, B.N.; Aderoba, A.K.; Akadiri, O.; Olofinbiyi, B.A.; Bakare, B. Emergency Peripartum Hysterectomy: A Multicenter Study of Incidence, Indications and Outcomes in Southwestern Nigeria. Matern. Child Health J. 2016, 20, 1230–1236. [Google Scholar] [CrossRef]
- Olamijulo, J.A.; Abiara, O.E.; Olaleye, O.O.; Ogedengbe, O.K.; Giwa-Osagie, F.; Oluwole, O.O. Emergency obstetric hysterectomy in a Nigerian teaching hospital: A ten-year review. Niger. Q. J. Hosp. Med. 2013, 23, 69–74. [Google Scholar]
- Mathe, J.K. Obstetric hysterectomy in rural Democratic Republic of the Congo: An analysis of 40 cases at Katwa Hospital. Afr. J. Reprod. Health 2008, 12, 60–66. [Google Scholar] [PubMed]
- Ezechi, O.; Kalu, B.; Njokanma, F.; Nwokoro, C.; Okeke, G. Emergency peripartum hysterectomy in a Nigerian hospital: A 20-year review. J. Obstet. Gynaecol. 2004, 24, 372–373. [Google Scholar] [CrossRef] [PubMed]
- Badejoko, O.O.; Awowole, I.O.; Ijarotimi, A.O.; Badejoko, B.O.; Loto, O.M.; Ogunniyi, S.O. Obstetric hysterectomy: Trend and outcome in Ile-Ife, Nigeria. J. Obstet. Gynaecol. 2013, 33, 581–584. [Google Scholar] [CrossRef] [PubMed]
- Bassey, G.; Akani, C.I. Emergency peripartum hysterectomy in a low resource setting: A 5-year analysis. Niger. J. Med. J. Natl. Assoc. Resid. Dr. Niger. 2014, 23, 170–175. [Google Scholar]
- Rabiu, K.A.; Akinlusi, F.M.; Adewunmi, A.A.; Akinola, O.I. Emergency peripartum hysterectomy in a tertiary hospital in Lagos, Nigeria: A five-year review. Trop. Doct. 2010, 40. [Google Scholar] [CrossRef]
- Okusanya Peripartum Hysterectomy in A Nigerian University Hospital: An Assessment of Severe Maternal Outcomes with the Maternal Severity Index Model. Available online: https://www.npmj.org/article.asp?issn=1117-1936;year=2016;volume=23;issue=2;spage=62;epage=66;aulast=Okusanya (accessed on 18 February 2021).
- Umezurike, C.C.; Feyi-Waboso, P.A.; Adisa, C.A. Peripartum hysterectomy in Aba southeastern Nigeria. Aust. N. Z. J. Obstet. Gynaecol. 2008, 48, 580–582. [Google Scholar] [CrossRef]
- Obiechina, N.J.A.; Eleje, G.U.; Ezebialu, I.U.; Okeke, C.A.F.; Mbamara, S.U. Emergency peripartum hysterectomy in Nnewi, Nigeria: A 10-year review. Niger. J. Clin. Pract. 2012, 15, 168. [Google Scholar] [CrossRef]
- Wandabwa, J.; Businge, C.; Longo-Mbenza, B.; Mdaka, M.; Kiondo, P. Peripartum hysterectomy: Two years experience at Nelson Mandela Academic hospital, Mthatha, Eastern Cape South Africa. Afr. Health Sci. 2013, 13, 469–474. [Google Scholar] [CrossRef]
- Nayama, M.; Moulaye, A.-A.; Djibrill, B.; Garba, M.; Idi, N.; Boukerrou, M. Les hystérectomies d’hémostase en pays sous-équipé: Un geste vital. Étude prospective dans une maternité de référence au Niger. Gynécologie Obs. Fertil. 2006, 34, 900–905. [Google Scholar] [CrossRef]
- Pembe, A.B.; Wangwe, P.J.T.; Massawe, S.N. Emergency peripartum hysterectomies at Muhimbili National Hospital, Tanzania: Review of cases from 2003 to 2007. Tanzan. J. Health Res. 2012, 14. [Google Scholar] [CrossRef]
- Baskett, T. Emergency obstetric hysterectomy. J. Obstet. Gynaecol. 2003, 23, 353–355. [Google Scholar] [CrossRef] [PubMed]
- Bateman, B.T.; Mhyre, J.M.; Callaghan, W.M.; Kuklina, E.V. Peripartum hysterectomy in the United States: Nationwide 14 year experience. Am. J. Obstet. Gynecol. 2012, 206, 63.e1–63.e8. [Google Scholar] [CrossRef] [PubMed]
- Bodelon, C.; Bernabe-Ortiz, A.; Schiff, M.A.; Reed, S.D. Factors Associated With Peripartum Hysterectomy. Obstet. Gynecol. 2009, 114, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Forna, F.; Miles, A.M.; Jamieson, D.J. Emergency peripartum hysterectomy: A comparison of cesarean and postpartum hysterectomy. Am. J. Obstet. Gynecol. 2004, 190, 1440–1444. [Google Scholar] [CrossRef]
- Glaze, S.; Ekwalanga, P.; Roberts, G.; Lange, I.; Birch, C.; Rosengarten, A.; Jarrell, J.; Ross, S. Peripartum Hysterectomy 1999 to 2006. Obstet. Gynecol. 2008, 111, 732–738. [Google Scholar] [CrossRef] [PubMed]
- Govindappagari, S.; Wright, J.D.; Ananth, C.V.; Huang, Y.; D’Alton, M.E.; Friedman, A.M. Risk for Peripartum Hysterectomy and Center Hysterectomy and Delivery Volume. Obstet. Gynecol. 2016, 128, 1215–1224. [Google Scholar] [CrossRef]
- Ibrahim, M.; Ziegler, C.; Klam, S.L.; Wieczorek, P.; Abenhaim, H.A. Incidence, Indications, and Predictors of Adverse Outcomes of Postpartum Hysterectomies: 20-Year Experience in a Tertiary Care Centre. J. Obstet. Gynaecol. Can. 2014, 36, 14–20. [Google Scholar] [CrossRef]
- Owolabi, M.S.; Blake, R.E.; Mayor, M.T.; Adegbulugbe, H.A. Incidence and determinants of peripartum hysterectomy in the metropolitan area of the District of Columbia. J. Reprod. Med. 2013, 58, 167–172. [Google Scholar]
- Kastner, E. Emergency peripartum hysterectomy: Experience at a community teaching hospital. Obstet. Gynecol. 2002, 99, 971–975. [Google Scholar] [CrossRef]
- Hernandez, J.; Wendel, G.; Sheffield, J. Trends in Emergency Peripartum Hysterectomy at a Single Institution: 1988–2009. Am. J. Perinatol. 2012, 30, 365–370. [Google Scholar] [CrossRef]
- Bakshi, S.; Meyer, B.A. Indications for and outcomes of emergency peripartum hysterectomy. A five-year review. J. Reprod. Med. 2000, 45, 733–737. [Google Scholar] [PubMed]
- Yamamoto, H.; Sagae, S.; Nishikawa, S.; Kudo, R. Emergency Postpartum Hysterectomy in Obstetric Practice. J. Obstet. Gynaecol. Res. 2000, 26, 341–345. [Google Scholar] [CrossRef] [PubMed]
- Jin, R.; Guo, Y.; Chen, Y. Risk factors associated with emergency peripartum hysterectomy. Chin. Med. J. 2014, 127, 900–904. [Google Scholar] [PubMed]
- Erman Akar, M.; Saygili Yilmaz, E.; Yuksel, B.; Yilmaz, Z. Emergency peripartum hysterectomy. Eur. J. Obstet. Gynecol. Reprod. Biol. 2004, 113, 178–181. [Google Scholar] [CrossRef]
- Özden, S.; Yildirim, G.; Basaran, T.; Gurbuz, B.; Dayicioglu, V. Analysis of 59 cases of emergent peripartum hysterectomies during a 13-year period. Arch. Gynecol. Obstet. 2005, 271, 363–367. [Google Scholar] [CrossRef]
- Begum, M.; Alsafi, F.; ElFarra, J.; Tamim, H.M.; Le, T. Emergency Peripartum Hysterectomy in a Tertiary Care Hospital in Saudi Arabia. J. Obstet. Gynaecol. India 2014, 64, 321–327. [Google Scholar] [CrossRef]
- Chibber, R.; Al-Hijji, J.; Fouda, M.; Al-Saleh, E.; Al-Adwani, A.R.; Mohammed, A.T. A 26-Year Review of Emergency Peripartum Hysterectomy in a Tertiary Teaching Hospital in Kuwait–Years 1983–2011. Med. Princ. Pract. 2012, 21, 217–222. [Google Scholar] [CrossRef]
- Demirci, O.; Tuğrul, A.S.; Yılmaz, E.; Tosun, Ö.; Demirci, E.; Eren, Y.S. Emergency peripartum hysterectomy in a tertiary obstetric center: Nine years evaluation: Emergency peripartum hysterectomy. J. Obstet. Gynaecol. Res. 2011, 37, 1054–1060. [Google Scholar] [CrossRef]
- Kayabasoglu, F.; Guzin, K.; Aydogdu, S.; Sezginsoy, S.; Turkgeldi, L.; Gunduz, G. Emergency peripartum hysterectomy in a tertiary Istanbul hospital. Arch. Gynecol. Obstet. 2008, 278, 251–256. [Google Scholar] [CrossRef]
- Tapisiz, O.L.; Altinbas, S.K.; Yirci, B.; Cenksoy, P.; Kaya, A.E.; Dede, S.; Kandemir, O. Emergency peripartum hysterectomy in a tertiary hospital in Ankara, Turkey: A 5-year review. Arch. Gynecol. Obstet. 2012, 286, 1131–1134. [Google Scholar] [CrossRef]
- Wei, Q.; Zhang, W.; Chen, M.; Zhang, L.; He, G.; Liu, X. Peripartum hysterectomy in 38 hospitals in China: A population-based study. Arch. Gynecol. Obstet. 2014, 289, 549–553. [Google Scholar] [CrossRef] [PubMed]
- Danisman, N.; Baser, E.; Togrul, C.; Kaymak, O.; Tandogan, M.; Gungor, T. Emergency peripartum hysterectomy: Experience of a major referral hospital in Ankara, Turkey. J. Obstet. Gynaecol. 2015, 35, 19–21. [Google Scholar] [CrossRef] [PubMed]
- Sahin, S.; Guzin, K.; Eroğlu, M.; Kayabasoglu, F.; Yaşartekin, M.S. Emergency peripartum hysterectomy: Our 12-year experience. Arch. Gynecol. Obstet. 2014, 289, 953–958. [Google Scholar] [CrossRef] [PubMed]
- Temizkan, O.; Angın, D.; Karakuş, R.; Şanverdi, İ.; Polat, M.; Karateke, A. Changing trends in emergency peripartum hysterectomy in a tertiary obstetric center in Turkey during 2000–2013. J. Turk. Ger. Gynecol. Assoc. 2016, 17, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Orbach, A.; Levy, A.; Wiznitzer, A.; Mazor, M.; Holcberg, G.; Sheiner, E. Peripartum cesarean hysterectomy: Critical analysis of risk factors and trends over the years. J. Matern.-Fetal Neonatal Med. 2011, 24, 480–484. [Google Scholar] [CrossRef] [PubMed]
- Rahman, J.; Al-Ali, M.; Qutub, H.O.; Al-Suleiman, S.S.; Al-Jama, F.E.; Rahman, M.S. Emergency obstetric hysterectomy in a university hospital: A 25-year review. J. Obstet. Gynaecol. 2008, 28, 69–72. [Google Scholar] [CrossRef]
- Zhang, Y.; Yan, J.; Han, Q.; Yang, T.; Cai, L.; Fu, Y.; Cai, X.; Guo, M. Emergency obstetric hysterectomy for life-threatening postpartum hemorrhage. Medicine 2017, 96, e8443. [Google Scholar] [CrossRef]
- Katchy, K.C.; Ziad, F.; Nashmi, N.A.; Diejomaoh, M.F.E. Emergency obstetric hysterectomy in Kuwait: A clinico pathological analysis. Arch. Gynecol. Obstet. 2006, 273, 360–365. [Google Scholar] [CrossRef]
- Tahmina, S.; Daniel, M.; Gunasegaran, P. Emergency Peripartum Hysterectomy: A 14-Year Experience at a Tertiary Care Centre in India. J. Clin. Diagn. Res. JCDR 2017, 11, QC08–QC11. [Google Scholar] [CrossRef]
- Chawla, J.; Arora, D.; Paul, M.; Ajmani, S.N. Emergency Obstetric Hysterectomy: A Retrospective Study from a Teaching Hospital in North India over Eight Years. Oman Med. J. 2015, 30, 181–186. [Google Scholar] [CrossRef]
- Kovavisarach, E. Obstetric hysterectomy: A 14-year experience of Rajavithi Hospital 1989–2002. J. Med. Assoc. Thail. 2006, 89, 1817–1821. [Google Scholar]
- Tahaoglu, A.E.; Balsak, D.; Togrul, C.; Obut, M.; Tosun, O.; Cavus, Y.; Bademkiran, H.; Budak, S. Emergency peripartum hysterectomy: Our experience. Ir. J. Med. Sci. 2016, 185, 833–838. [Google Scholar] [CrossRef] [PubMed]
- El-Jallad, M.F.; Zayed, F.; Al-Rimawi, H.S. Emergency peripartum hysterectomy in Northern Jordan: Indications and obstetric outcome (an 8-year review). Arch. Gynecol. Obstet. 2004, 270, 271–273. [Google Scholar] [CrossRef]
- Jou, H.-J.; Hung, H.-W.; Ling, P.-Y.; Chen, S.-M.; Wu, S.-C. Peripartum hysterectomy in Taiwan. Int. J. Gynecol. Obstet. 2008, 101, 269–272. [Google Scholar] [CrossRef] [PubMed]
- Saeed, F.; Khalid, R.; Khan, A.; Masheer, S.; Rizvi, J.H. Peripartum hysterectomy: A ten-year experience at a tertiary care hospital in a developing country. Trop. Doct. 2010, 40, 18–21. [Google Scholar] [CrossRef]
- Nawal, R.; Nooren, M. Obstetric hysterectomy: A life saving emergency. Indian J. Med. Sci. 2013, 67, 99. [Google Scholar] [CrossRef]
- Kara, M. Emergency peripartum hysterectomy cases in Agri: A 6-year review. Clin. Exp. Obstet. Gynecol. 2012, 39, 202–204. [Google Scholar]
- Pradhan, M.; Shao, Y. Emergency Peripartum Hysterectomy as Postpartum Hemorrhage Treatment: Incidence, Risk factors, and Complications. JNMA J. Nepal Med. Assoc. 2014, 52, 668–676. [Google Scholar] [CrossRef]
- Bai, S.W.; Lee, H.J.; Cho, J.S.; Park, Y.W.; Kim, S.K.; Park, K.H. Peripartum hysterectomy and associated factors. J. Reprod. Med. 2003, 48, 148–152. [Google Scholar]
- Korejo, R.; Nasir, A.; Yasmin, H.; Bhutta, S. Emergency Obstetric Hysterectomy. J. Pak. Med. Assoc. 2012, 62, 4. [Google Scholar]
- Uysal, D.; Cokmez, H.; Aydin, C.; Ciftpinar, T. Emergency peripartum hysterectomy: A retrospective study in a tertiary care hospital in Turkey from 2007 to 2015. J. Pak. Med. Assoc. 2018, 68, 3. [Google Scholar]
- Nisar, N.; Sohoo, N.A. Emergency peripartum hysterectomy: Frequency, indications and maternal outcome. J. Ayub Med. Coll. Abbottabad JAMC 2009, 21, 48–51. [Google Scholar] [PubMed]
- Sakinci, M.; Kuru, O.; Tosun, M.; Karagoz, A.; Celik, H.; Bildircin, F.D.; Malatyalioglu, E. Clinical analysis of emergency peripartum hysterectomies in a tertiary center. Clin. Exp. Obstet. Gynecol. 2014, 41, 654–658. [Google Scholar] [CrossRef]
- Zeteroglu, S.; Ustun, Y.; Engin-Ustun, Y.; Sahin, G.; Kamacı, M. Peripartum hysterectomy in a teaching hospital in the eastern region of Turkey. Eur. J. Obstet. Gynecol. Reprod. Biol. 2005, 120, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Özcan, H.Ç.; Uğur, M.G.; Balat, Ö.; Bayramoğlu Tepe, N.; Sucu, S. Emergency peripartum hysterectomy: Single center ten-year experience. J. Matern. Fetal Neonatal Med. 2017, 30, 2778–2783. [Google Scholar] [CrossRef] [PubMed]
- Sharma, B.; Sikka, P.; Jain, V.; Jain, K.; Bagga, R.; Suri, V. Peripartum hysterectomy in a tertiary care hospital: Epidemiology and outcomes. J. Anaesthesiol. Clin. Pharmacol. 2017, 33, 324–328. [Google Scholar] [CrossRef] [PubMed]
- Yucel, O.; Ozdemir, I.; Yucel, N.; Somunkiran, A. Emergency peripartum hysterectomy: A 9-year review. Arch. Gynecol. Obstet. 2006, 274, 84–87. [Google Scholar] [CrossRef]
- Engelsen, I.B.; Albrechtsen, S.; Iversen, O.E. Peripartum hysterectomy-incidence and maternal morbidity. Acta Obstet. Gynecol. Scand. 2001, 80, 409–412. [Google Scholar] [CrossRef]
- Sakse, A.; Weber, T.; Nickelsen, C.; Secher, N.J. Peripartum hysterectomy in Denmark 1995–2004. Acta Obstet. Gynecol. Scand. 2007, 86, 1472–1475. [Google Scholar] [CrossRef]
- Tadesse, W.; Farah, N.; Hogan, J.; D’arcy, T.; Kennelly, M.; Turner, M.J. Peripartum hysterectomy in the first decade of the 21st century. J. Obstet. Gynaecol. 2011, 31, 320–321. [Google Scholar] [CrossRef]
- Campbell, S.M.; Corcoran, P.; Manning, E.; Greene, R.A. Peripartum hysterectomy incidence, risk factors and clinical characteristics in Ireland. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 207, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Kwee, A.; Bots, M.L.; Visser, G.H.A.; Bruinse, H.W. Emergency peripartum hysterectomy: A prospective study in The Netherlands. Eur. J. Obstet. Gynecol. Reprod. Biol. 2006, 124, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Langdana, F.; Geary, M.; Haw, W.; Keane, D. Peripartum hysterectomy in the 1990s: Any new lessons? J. Obstet. Gynaecol. 2001, 21, 121–123. [Google Scholar] [CrossRef]
- Roopnarinesingh, R.; Fay, L.; Mckenna, P. A 27-year review of obstetric hysterectomy. J. Obstet. Gynaecol. 2003, 23, 252–254. [Google Scholar] [CrossRef] [PubMed]
- Vandenberghe, G.; Guisset, M.; Janssens, I.; Leeuw, V.V.; Roelens, K.; Hanssens, M.; Russo, E.; Van Keirsbilck, J.; Englert, Y.; Verstraelen, H. A nationwide population-based cohort study of peripartum hysterectomy and arterial embolisation in Belgium: Results from the Belgian Obstetric Surveillance System. BMJ Open 2017, 7, e016208. [Google Scholar] [CrossRef] [PubMed]
- Yoong, W.; Massiah, N.; Oluwu, A. Obstetric hysterectomy: Changing trends over 20 years in a multiethnic high risk population. Arch. Gynecol. Obstet. 2006, 274, 37–40. [Google Scholar] [CrossRef]
- Flood, K.M.; Said, S.; Geary, M.; Robson, M.; Fitzpatrick, C.; Malone, F.D. Changing trends in peripartum hysterectomy over the last 4 decades. Am. J. Obstet. Gynecol. 2009, 200, 632.e1–632.e6. [Google Scholar] [CrossRef]
- Jakobsson, M.; Tapper, A.-M.; Colmorn, L.B.; Lindqvist, P.G.; Klungsøyr, K.; Krebs, L.; Børdahl, P.E.; Gottvall, K.; Källén, K.; Bjarnadóttir, R.I.; et al. Emergency peripartum hysterectomy: Results from the prospective Nordic Obstetric Surveillance Study (NOSS). Acta Obstet. Gynecol. Scand. 2015, 94, 745–754. [Google Scholar] [CrossRef]
- Smith, J.; Mousa, H.A. Peripartum hysterectomy for primary postpartum haemorrhage: Incidence and maternal morbidity. J. Obstet. Gynaecol. 2007, 27, 44–47. [Google Scholar] [CrossRef]
- Eniola, O.A.; Bewley, S.; Waterstone, M.; Hooper, R.; Wolfe, C.D.A. Obstetric hysterectomy in a population of South East England. J. Obstet. Gynaecol. 2006, 26, 104–109. [Google Scholar] [CrossRef]
- Kallianidis, A.F.; Maraschini, A.; Danis, J.; Colmorn, L.B.; Deneux-Tharaux, C.; Donati, S.; Gissler, M.; Jakobsson, M.; Knight, M.; Kristufkova, A.; et al. Epidemiological analysis of peripartum hysterectomy across nine European countries. Acta Obstet. Gynecol. Scand. 2020, 99, 1364–1373. [Google Scholar] [CrossRef] [PubMed]
- Selo-Ojeme, D.O.; Bhattacharjee, P.; Izuwa-Njoku, N.F.; Kadir, R.A. Emergency peripartum hysterectomy in a tertiary London hospital. Arch. Gynecol. Obstet. 2005, 271, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Sheiner, E.; Levy, A.; Katz, M.; Mazor, M. Identifying risk factors for peripartum cesarean hysterectomy. A population-based study. J. Reprod. Med. 2003, 48, 622–626. [Google Scholar] [PubMed]
- Wenham, J.; Matijevic, R. Post-partum hysterectomies: Revisited. J. Perinat. Med. 2001, 29. [Google Scholar] [CrossRef] [PubMed]
- Lone, F.; Sultan, A.H.; Thakar, R.; Beggs, A. Risk factors and management patterns for emergency obstetric hysterectomy over 2 decades. Int. J. Gynecol. Obstet. 2010, 109, 12–15. [Google Scholar] [CrossRef]
- Parazzini, F.; Ricci, E.; Cipriani, S.; Chiaffarino, F.; Bortolus, R.; Chiantera, V.; Bulfoni, G. Temporal trends and determinants of peripartum hysterectomy in Lombardy, Northern Italy, 1996–2010. Arch. Gynecol. Obstet. 2013, 287, 223–228. [Google Scholar] [CrossRef]
- Varras, M.; Krivis, C.; Plis, C.; Tsoukalos, G. Emergency obstetric hysterectomy at two tertiary centers: A clinical analysis of 11 years experience. Clin. Exp. Obstet. Gynecol. 2010, 37, 117–119. [Google Scholar]
- Habek, D.; Bečareviç, R. Emergency Peripartum Hysterectomy in a Tertiary Obstetric Center: 8-Year Evaluation. Fetal Diagn. Ther. 2007, 22, 139–142. [Google Scholar] [CrossRef]
- Ossola, M.W.; Somigliana, E.; Mauro, M.; Acaia, B.; Benaglia, L.; Fedele, L. Risk factors for emergency postpartum hysterectomy: The neglected role of previous surgically induced abortions. Acta Obstet. Gynecol. Scand. 2011, 90, 1450–1453. [Google Scholar] [CrossRef]
- Christopoulos, P.; Hassiakos, D.; Tsitoura, A.; Panoulis, K.; Papadias, K.; Vitoratos, N. Obstetric hysterectomy: A review of cases over 16 years. J. Obstet. Gynaecol. 2011, 31, 139–141. [Google Scholar] [CrossRef]
- Jones, B.; Zhang, E.; Alzouebi, A.; Robbins, T.; Paterson-Brown, S.; Prior, T.; Kumar, S. Maternal and perinatal outcomes following peripartum hysterectomy from a single tertiary centre. Aust. N. Z. J. Obstet. Gynaecol. 2013, 53, 561–565. [Google Scholar] [CrossRef] [PubMed]
- Stivanello, E.; Knight, M.; Dallolio, L.; Frammartino, B.; Rizzo, N.; Fantini, M.P. Peripartum hysterectomy and cesarean delivery: A population-based study. Acta Obstet. Gynecol. Scand. 2010, 89, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Macharey, G.; Ulander, V.-M.; Kostev, K.; Väisänen-Tommiska, M.; Ziller, V. Emergency peripartum hysterectomy and risk factors by mode of delivery and obstetric history: A 10-year review from Helsinki University Central Hospital. J. Perinat. Med. 2015, 43, 721–728. [Google Scholar] [CrossRef]
- Maraschini, A.; Lega, I.; D’Aloja, P.; Buoncristiano, M.; Dell’Oro, S.; Donati, S. Women undergoing peripartum hysterectomy due to obstetric hemorrhage: A prospective population-based study. Acta Obstet. Gynecol. Scand. 2020, 99, 274–282. [Google Scholar] [CrossRef] [PubMed]
- de Gregorio, A.; Friedl, T.W.P.; Scholz, C.; Janni, W.; Ebner, F.; de Gregorio, N. Emergency peripartal hysterectomy–a single-center analysis of the last 13 years at a tertiary perinatal care unit. J. Perinat. Med. 2019, 47, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Daskalakis, G.; Anastasakis, E.; Papantoniou, N.; Mesogitis, S.; Theodora, M.; Antsaklis, A. Emergency obstetric hysterectomy. Acta Obstet. Gynecol. Scand. 2007, 86, 223–227. [Google Scholar] [CrossRef]
- Roethlisberger, M.; Womastek, I.; Posch, M.; Husslein, P.; Pateisky, N.; Lehner, R. Early postpartum hysterectomy: Incidence and risk factors. Acta Obstet. Gynecol. Scand. 2010, 89, 1040–1044. [Google Scholar] [CrossRef]
- D’Arpe, S.; Franceschetti, S.; Corosu, R.; Palaia, I.; Di Donato, V.; Perniola, G.; Muzii, L.; Benedetti Panici, P. Emergency peripartum hysterectomy in a tertiary teaching hospital: A 14-year review. Arch. Gynecol. Obstet. 2015, 291, 841–847. [Google Scholar] [CrossRef]
- Gerli, S.; Favilli, A.; Bini, V.; Di Renzo, G.C. Postpartum hysterectomy: A regional multicentre analysis in Italy. J. Obstet. Gynaecol. 2010, 30, 829–832. [Google Scholar] [CrossRef]
- Wong, T.Y. Emergency peripartum hysterectomy: A 10-year review in a tertiary obstetric hospital. N. Z. Med. J. 2011, 124, 34–39. [Google Scholar]
- Cheng, H.C.; Pelecanos, A.; Sekar, R. Review of peripartum hysterectomy rates at a tertiary Australian hospital. Aust. N. Z. J. Obstet. Gynaecol. 2016, 56, 614–618. [Google Scholar] [CrossRef] [PubMed]
- Awan, N.; Bennett, M.J.; Walters, W.A.W. Emergency peripartum hysterectomy: A 10-year review at the Royal Hospital for Women, Sydney: Emergency peripartum hysterectomy. Aust. N. Z. J. Obstet. Gynaecol. 2011, 51, 210–215. [Google Scholar] [CrossRef]
- Lim, W.H.; Pavlov, T.; Dennis, A.E. Analysis of emergency peripartum hysterectomy in Northern Tasmania: Emergency peripartum hysterectomy. Aust. J. Rural Health 2014, 22, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Arulpragasam, K.; Hyanes, G.; Epee-Bekima, M. Emergency peripartum hysterectomy in a Western Australian population: Ten-year retrospective case-note analysis. Aust. N. Z. J. Obstet. Gynaecol. 2019, 59, 533–537. [Google Scholar] [CrossRef] [PubMed]
- Shamsa, A.; Harris, A.; Anpalagan, A. Peripartum hysterectomy in a tertiary hospital in Western Sydney. J. Obstet. Gynaecol. 2015, 35, 350–353. [Google Scholar] [CrossRef] [PubMed]
- Kellie, F.J.; Wandabwa, J.N.; Mousa, H.A.; Weeks, A.D. Mechanical and surgical interventions for treating primary postpartum haemorrhage. Cochrane Database Syst. Rev. 2020, 7, CD013663. [Google Scholar] [CrossRef]
- Garg, K.; Shih, K.; Iasonos, A. Endometrial Carcinomas in Women Aged 40 Years and Younger: Tumors Associated With Loss of DNA Mismatch Repair Proteins Comprise a Distinct Clinicopathologic Subset. Am. J. Surg. Pathol. 2009, 33, 9. [Google Scholar] [CrossRef]
- Esselen, K.M.; Vitonis, A.; Einarsson, J.; Muto, M.G.; Cohen, S. Health Care Disparities in Hysterectomy for Gynecologic Cancers: Data From the 2012 National Inpatient Sample. Obstet. Gynecol. 2015, 126, 1029–1039. [Google Scholar] [CrossRef]
- Merrill, R.M. Impact of Hysterectomy and Bilateral Oophorectomy on Race-Specific Rates of Corpus, Cervical, and Ovarian Cancers in the United States. Ann. Epidemiol. 2006, 16, 880–887. [Google Scholar] [CrossRef]
- Grimbizis, G.F.; Gordts, S.; Di Spiezio Sardo, A.; Brucker, S.; De Angelis, C.; Gergolet, M.; Li, T.-C.; Tanos, V.; Brolmann, H.; Gianaroli, L.; et al. The ESHRE/ESGE consensus on the classification of female genital tract congenital anomalies. Hum. Reprod. 2013, 28, 2032–2044. [Google Scholar] [CrossRef]
- Shuiqing, M.; Xuming, B.; Jinghe, L. Pregnancy and its outcome in women with malformed uterus. Chin. Med. Sci. J. Chung-Kuo Hsueh Ko Hsueh Tsa Chih 2002, 17, 242–245. [Google Scholar]
- Tur-Kaspa, I.; Gal, M.; Hartman, M.; Hartman, J.; Hartman, A. A prospective evaluation of uterine abnormalities by saline infusion sonohysterography in 1009 women with infertility or abnormal uterine bleeding. Fertil. Steril. 2006, 86, 1731–1735. [Google Scholar] [CrossRef] [PubMed]
- Prior, M.; Richardson, A.; Asif, S.; Polanski, L.; Parris-Larkin, M.; Chandler, J.; Fogg, L.; Jassal, P.; Thornton, J.G.; Raine-Fenning, N.J. Outcome of assisted reproduction in women with congenital uterine anomalies: A prospective observational study. Ultrasound Obstet. Gynecol. 2018, 51, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Ludwin, A.; Ludwin, I.; Neto, M.A.C.; Nastri, C.O.; Bhagavath, B.; Lindheim, S.R.; Martins, W.P. Septate uterus according to ESHRE/ESGE, ASRM and CUME definitions: Association with infertility and miscarriage, cost and warnings for women and healthcare systems. Ultrasound Obstet. Gynecol. 2019, 54, 800–814. [Google Scholar] [CrossRef]
- Saridogan, E.; Salman, M.; Direk, L.S.; Alchami, A. Reproductive Performance Following Hysteroscopic Surgery for Uterine Septum: Results from a Single Surgeon Data. J. Clin. Med. 2021, 10, 130. [Google Scholar] [CrossRef]
- Şükür, Y.E.; Yakıştıran, B.; Özmen, B.; Sönmezer, M.; Berker, B.; Atabekoğlu, C. Hysteroscopic Corrections for Complete Septate and T-Shaped Uteri Have Similar Surgical and Reproductive Outcome. Reprod. Sci. 2018, 25, 1649–1654. [Google Scholar] [CrossRef]
- Wang, X.; Hou, H.; Yu, Q. Fertility and pregnancy outcomes following hysteroscopic metroplasty of different sized uterine septa. Medicine 2019, 98, 30. [Google Scholar] [CrossRef]
- Larsen, E.C.; Schmiegelow, K.; Rechnitzer, C.; Loft, A.; Müller, J.; Andersen, A.N. Radiotherapy at a young age reduces uterine volume of childhood cancer survivors. Acta Obstet. Gynecol. Scand. 2004, 83, 96–102. [Google Scholar] [CrossRef]
- Sudour, H.; Chastagner, P.; Claude, L.; Desandes, E.; Klein, M.; Carrie, C.; Bernier, V. Fertility and Pregnancy Outcome After Abdominal Irradiation That Included or Excluded the Pelvis in Childhood Tumor Survivors. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, 867–873. [Google Scholar] [CrossRef]
- Kunz, G.; Beil, D.; Huppert, P.; Noe, M.; Kissler, S.; Leyendecker, G. Adenomyosis in endometriosis—prevalence and impact on fertility. Evidence from magnetic resonance imaging. Hum. Reprod. 2005, 20, 2309–2316. [Google Scholar] [CrossRef]
- Bourdon, M.; Santulli, P.; Oliveira, J.; Marcellin, L.; Maignien, C.; Melka, L.; Bordonne, C.; Millisher, A.-E.; Plu-Bureau, G.; Cormier, J.; et al. Focal adenomyosis is associated with primary infertility. Fertil. Steril. 2020, 114, 1271–1277. [Google Scholar] [CrossRef] [PubMed]
- Abu Hashim, H.; Elaraby, S.; Fouda, A.A.; Rakhawy, M.E. The prevalence of adenomyosis in an infertile population: A cross-sectional study. Reprod. Biomed. Online 2020, 40, 842–850. [Google Scholar] [CrossRef] [PubMed]
- Salzani, A.; Yela, D.A.; Gabiatti, J.R.E.; Bedone, A.J.; Monteiro, I.M.U. Prevalence of uterine synechia after abortion evacuation curettage. Sao Paulo Med. J. 2007, 125, 261–264. [Google Scholar] [CrossRef] [PubMed]
- Socolov, R.; Anton, E.; Butureanu, S.; Socolov, D. The endoscopic management of uterine synechiae. A clinical study of 78 cases. Chir. Buchar. Rom. 1990 2010, 105, 515–518. [Google Scholar]
- Kdous, M.; Hachicha, R.; Zhioua, F.; Ferchiou, M.; Chaker, A.; Meriah, S. Fertilité après cure hystéroscopique de synéchie. Gynécologie Obs. Fertil. 2003, 31, 422–428. [Google Scholar] [CrossRef]
- Walid, D.; Nadia, O.; Abdelwaheb, M.; Sonia, B.H.; Badreddine, B.; Rachida, S. Profil épidémiologique, diagnostic étiologique et pronostic des synéchies utérines: A propos de 86 cas. Tunis. Med. 2011, 90, 5. [Google Scholar]
- Johnson, G.; MacLehose, R.F.; Baird, D.D.; Laughlin-Tommaso, S.K.; Hartmann, K.E. Uterine leiomyomata and fecundability in the Right from the Start study. Hum. Reprod. Oxf. Engl. 2012, 27, 2991–2997. [Google Scholar] [CrossRef]
- Di Gregorio, A.; Maccario, S.; Raspollini, M. The role of laparoscopic myomectomy in women of reproductive age. Reprod. Biomed. Online 2002, 4, 55–58. [Google Scholar] [CrossRef]
- Nicolaus, K.; Bräuer, D.; Sczesny, R.; Lehmann, T.; Diebolder, H.; Runnebaum, I.B. Unexpected coexistent endometriosis in women with symptomatic uterine leiomyomas is independently associated with infertility, nulliparity and minor myoma size. Arch. Gynecol. Obstet. 2019, 300, 103–108. [Google Scholar] [CrossRef]
- Rovio, P.H.; Heinonen, P.K. Pregnancy outcomes after transvaginal myomectomy by colpotomy. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 161, 130–133. [Google Scholar] [CrossRef]
- Roy, K.K.; Singla, S.; Baruah, J.; Sharma, J.B.; Kumar, S.; Singh, N. Reproductive outcome following hysteroscopic myomectomy in patients with infertility and recurrent abortions. Arch. Gynecol. Obstet. 2010, 282, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Torre, A.; Paillusson, B.; Fain, V.; Labauge, P.; Pelage, J.P.; Fauconnier, A. Uterine artery embolization for severe symptomatic fibroids: Effects on fertility and symptoms. Hum. Reprod. 2014, 29, 490–501. [Google Scholar] [CrossRef] [PubMed]
- Torre, A.; Fauconnier, A.; Kahn, V.; Limot, O.; Bussierres, L.; Pelage, J.P. Fertility after uterine artery embolization for symptomatic multiple fibroids with no other infertility factors. Eur. Radiol. 2017, 27, 2850–2859. [Google Scholar] [CrossRef]
- Shokeir, T.A.; Shalan, H.M.; El-Shafei, M.M. Significance of endometrial polyps detected hysteroscopically in eumenorrheic infertile women. J. Obstet. Gynaecol. Res. 2004, 30, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Dahm-Kähler, P.; Diaz-Garcia, C.; Brännström, M. Human uterus transplantation in focus. Br. Med. Bull. 2016, 117, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Flyckt, R.; Davis, A.; Farrell, R.; Zimberg, S.; Tzakis, A.; Falcone, T. Uterine Transplantation: Surgical Innovation in the Treatment of Uterine Factor Infertility. J. Obstet. Gynaecol. Can. 2018, 40, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Johannesson, L.; Dahm-Kähler, P.; Eklind, S.; Brännström, M. The Future of Human Uterus Transplantation. Womens Health 2014, 10, 455–467. [Google Scholar] [CrossRef]
- Brännström, M.; Dahm Kähler, P.; Greite, R.; Mölne, J.; Díaz-García, C.; Tullius, S.G. Uterus Transplantation: A Rapidly Expanding Field. Transplantation 2018, 102, 569–577. [Google Scholar] [CrossRef]


{kind=link}
| Author | Publication Date | Population | Country | Couple’s Infertility (%) | Primary Infertility (%) | Secondary Infertility (%) | Male Infertility * (%) | Female Infertility * (%) | Mixed Infertility * (%) | Unexplained Infertility * (%) | Uterine Factor Infertility * (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Benbella et al. [13] | 2018 | Infertile population (1265 couples) | Morocco | 77.2 | 22.8 | 28.2 | 39.6 | 17.0 | 15.2 | 12.6 | |
| Elhussein et al. [3] | 2019 | Infertile population (800 couples) | Sudan | 68.9 | 31.1 | 35.5 | 42.8 | 18.4 | 3.4 | 2.1 | |
| Masoumi et al. [14] | 2015 | Infertile population (1200 couples) | Iran | 69.5 | 30.5 | 66.0 | 88.9 | 16.7 | |||
| Meng et al. [15] | 2015 | General population (2151 couples) | China | 13.6 | 14.0 | 11.2 | 17.0 | 40.0 | 26.0 | 17.0 | 12.1 |
| Author | Publication Date | Study Design | Country | Annual Incidence (Cases/100,000 Persons a Year) |
|---|---|---|---|---|
| Babalola et al. [25] | 2007 | Retrospective study | USA | 430 |
| Cooper et al. [20] | 2005 | Cross-sectional study | UK | 150 |
| Desai et al. [21] | 2017 | Cross-sectional study | India | 100 |
| Hammer et al. [22] | 2019 | Retrospective study | Denmark | 150 |
| Hammer et al. [23] | 2017 | Retrospective study | Denmark | 90 |
| Hill et al. [24] | 2010 | Cross-sectional study | Australia | 150 |
| Merrill et al. [26] | 2001 | Cross-sectional study | USA | 700 |
| Redburn et al. [27] | 2001 | Retrospective study | UK | 350 |
| Wilson et al. [28] | 2017 | Retrospective study | Australia | 70 |
| Author | Publication Date | Study Design | Country | Prevalence (%) |
|---|---|---|---|---|
| Beckmann et al. [29] | 2003 | Retrospective study | Australia | 7.90 |
| Bower et al. [30] | 2009 | Retrospective study | USA | 4.00 |
| Desai et al. [31] | 2019 | Cross-sectional study | India | 3.59 |
| Gartner et al. [32] | 2020 | Retrospective study | USA | 6.00 |
| Liu et al. [33] | 2017 | Cross-sectional study | China | 3.32 |
| Merrill et al. [34] | 2008 | Retrospective study | USA | 10.00 |
| Merrill et al. [35] | 2008 | Retrospective study | USA | 14.00 |
| Meher et al. [40] | 2020 | Retrospective study | India | 4.10 |
| Meher et al. [41] | 2020 | Retrospective study | India | 3.20 |
| Prusty et al. [42] | 2018 | Cross-sectional study | India | 1.70 |
| Rositch et al. [36] | 2014 | Retrospective study | USA | 10.00 |
| Ruiz de Azua Unzurrunzaga et al. [37] | 2019 | Retrospective study | Scotland | 10.00 |
| Shekhar et al. [38] | 2019 | Cross-sectional study | India | 4.80 |
| Temkin et al. [39] | 2018 | Retrospective study | USA | 10.00 |
| Author | Publication Date | Study Design | Country | Infertility’s Prevalence (%) |
|---|---|---|---|---|
| Di Gregorio et al. [171] | 2002 | Retrospective study | Italy | 70.00 |
| Nicolaus et al. [172] | 2019 | Retrospective study | USA | 15.70 |
| Rovio et al. [173] | 2012 | Retrospective study | Finland | 12.00 |
| Roy et al. [174] | 2010 | Retrospective study | India | 44.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sallée, C.; Margueritte, F.; Marquet, P.; Piver, P.; Aubard, Y.; Lavoué, V.; Dion, L.; Gauthier, T. Uterine Factor Infertility, a Systematic Review. J. Clin. Med. 2022, 11, 4907. https://doi.org/10.3390/jcm11164907
Sallée C, Margueritte F, Marquet P, Piver P, Aubard Y, Lavoué V, Dion L, Gauthier T. Uterine Factor Infertility, a Systematic Review. Journal of Clinical Medicine. 2022; 11(16):4907. https://doi.org/10.3390/jcm11164907
Chicago/Turabian StyleSallée, Camille, François Margueritte, Pierre Marquet, Pascal Piver, Yves Aubard, Vincent Lavoué, Ludivine Dion, and Tristan Gauthier. 2022. "Uterine Factor Infertility, a Systematic Review" Journal of Clinical Medicine 11, no. 16: 4907. https://doi.org/10.3390/jcm11164907
APA StyleSallée, C., Margueritte, F., Marquet, P., Piver, P., Aubard, Y., Lavoué, V., Dion, L., & Gauthier, T. (2022). Uterine Factor Infertility, a Systematic Review. Journal of Clinical Medicine, 11(16), 4907. https://doi.org/10.3390/jcm11164907