
Use of the Thyromental Height Test for Prediction of Difficult Laryngoscopy: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Information Sources and Search Strategy
2.4. Selection Process
2.5. Data Collection Process and Data Items
2.6. Study Risk of Bias Assessment
2.7. Diagnostic Accuracy Measures
2.8. Synthesis Methods
2.9. Publication Bias Assessment
3. Results
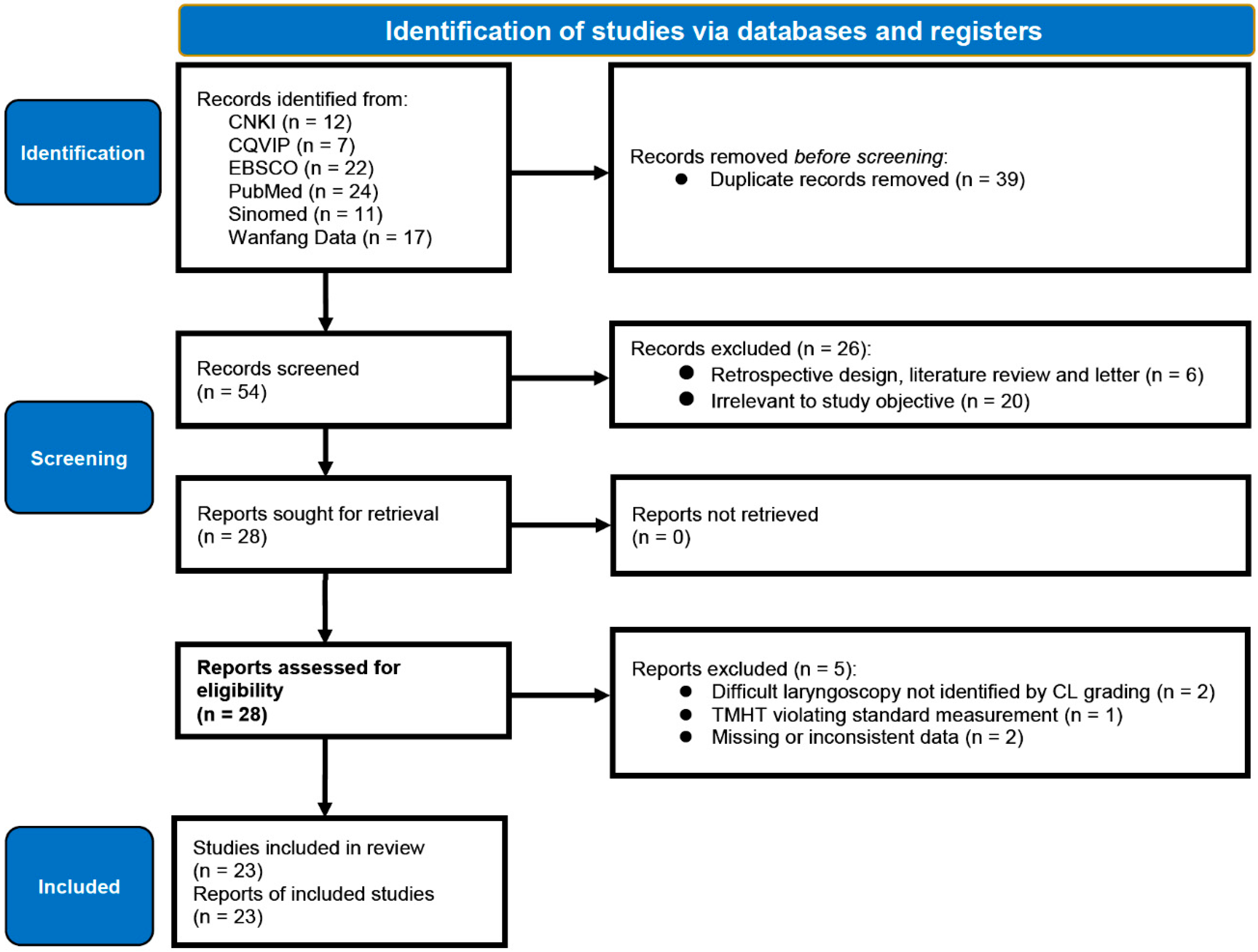
3.1. Study Selection
3.2. Study Characteristics
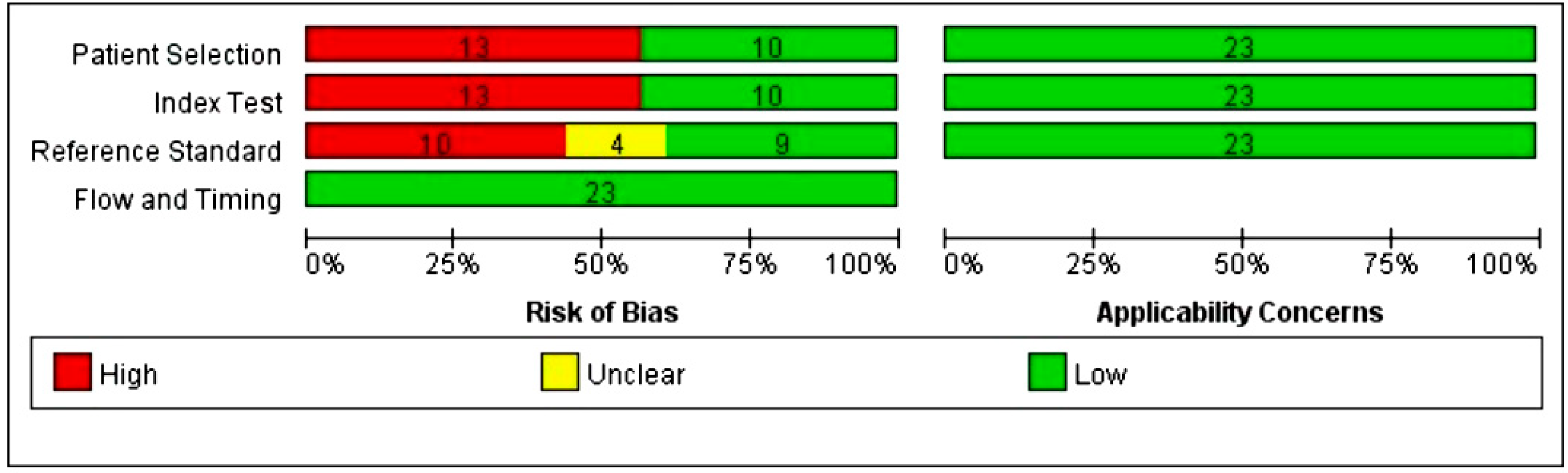
3.3. Risk of Bias in Studies
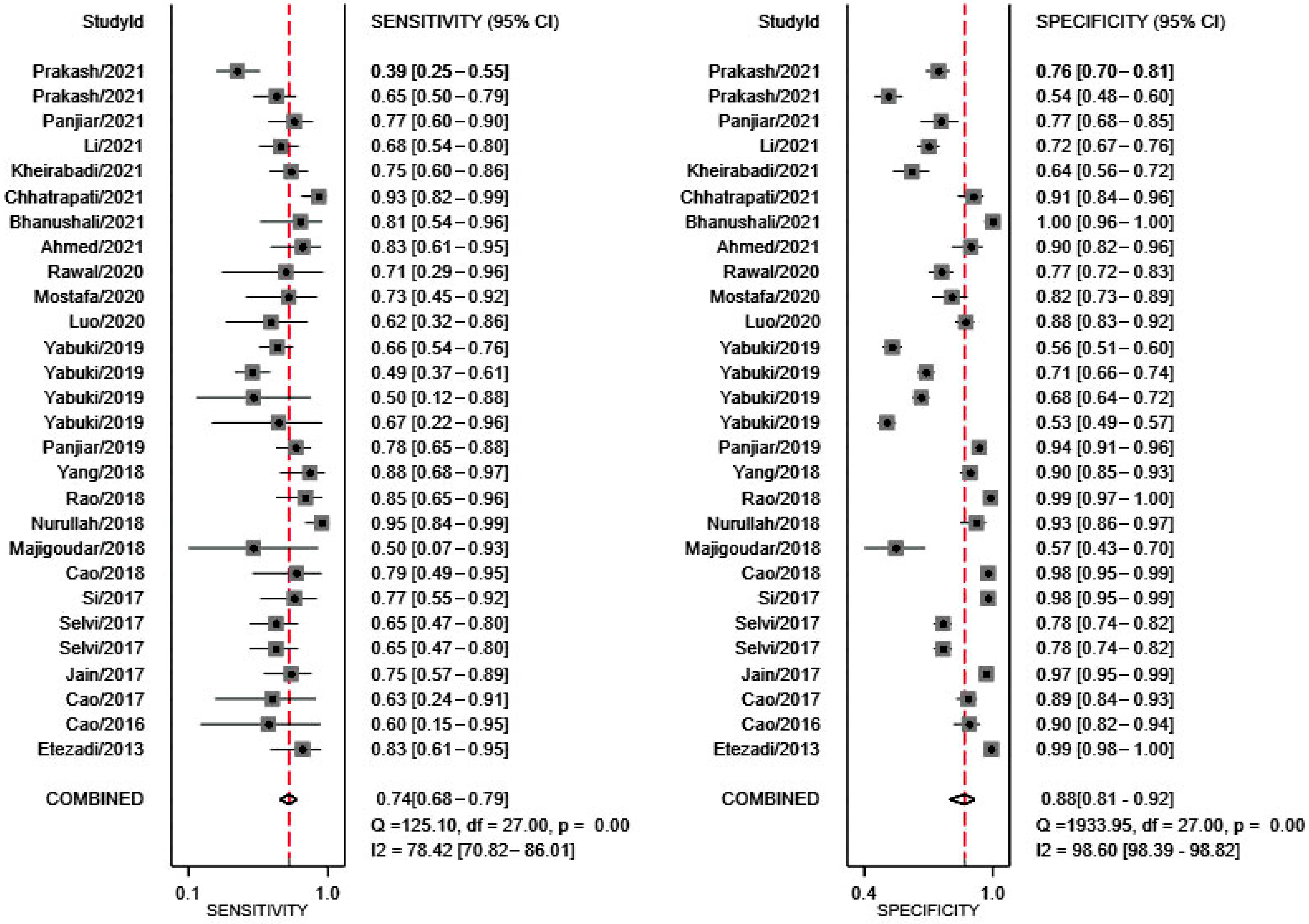
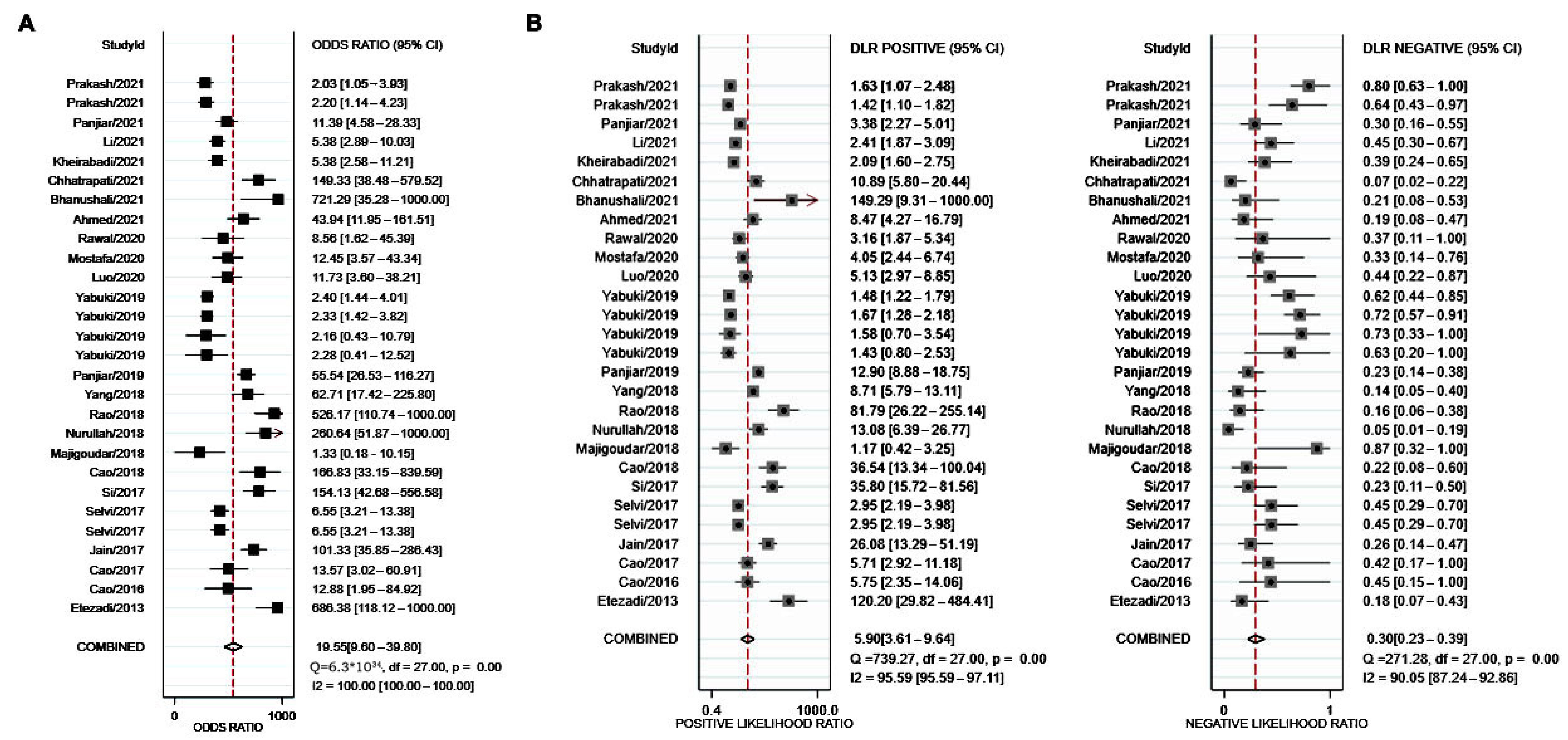
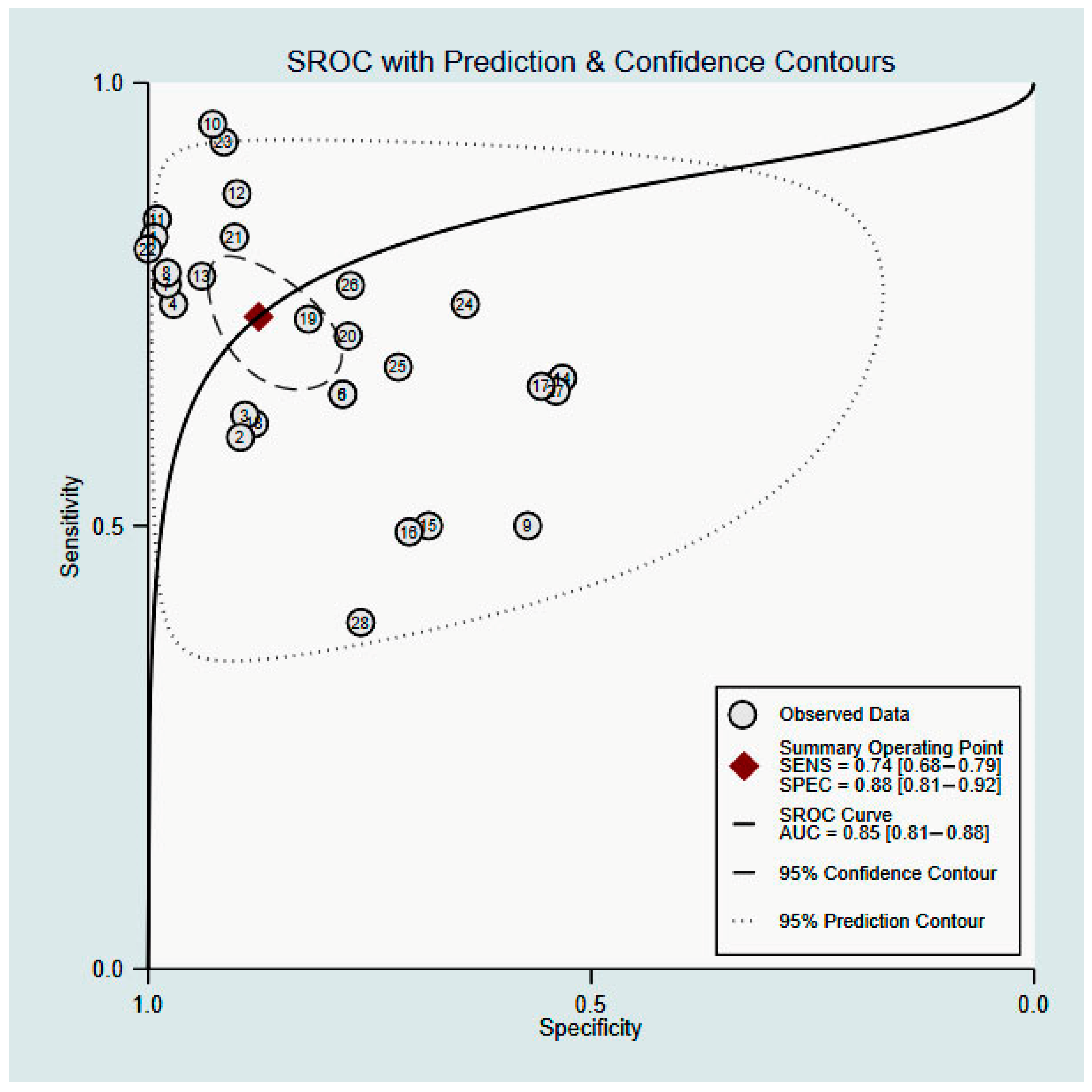
3.4. Results of Syntheses
3.5. Reporting Biases
4. Discussion
5. Limitations and Implications
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Apfelbaum, J.L.; Hagberg, C.A.; Connis, R.T.; Abdelmalak, B.B.; Agarkar, M.; Dutton, R.P.; Fiadjoe, J.E.; Greif, R.; Klock, P.A.; Mercier, D.; et al. 2022 American Society of Anesthesiologists Practice Guidelines for Management of the Difficult Airway. Anesthesiology 2022, 136, 31–81. [Google Scholar] [CrossRef] [PubMed]
- Honarmand, A.; Safavi, M.; Ansari, N. A comparison of between hyomental distance ratios, ratio of height to thyromental, modified Mallamapati classification test and upper lip bite test in predicting difficult laryngoscopy of patients undergoing general anesthesia. Adv. Biomed. Res. 2014, 3, 166. [Google Scholar] [PubMed]
- Apfelbaum, J.L.; Hagberg, C.A.; Caplan, R.A.; Blitt, C.D.; Connis, R.T.; Nickinovich, D.G.; Hagberg, C.A.; Caplan, R.A.; Benumof, J.L.; Berry, F.A.; et al. American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Practice guidelines for management of the difficult airway: An updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology 2013, 118, 251–270. [Google Scholar] [PubMed] [Green Version]
- Chhina, A.K.; Jain, R.; Gautam, P.L.; Garg, J.; Singh, N.; Grewal, A. Formulation of a multivariate predictive model for difficult intubation: A double blinded prospective study. J. Anaesthesiol. Clin. Pharmacol. 2018, 34, 62–67. [Google Scholar] [PubMed]
- Roth, D.; Pace, N.L.; Lee, A.; Hovhannisyan, K.; Warenits, A.M.; Arrich, J.; Herkner, H. Bedside tests for predicting difficult airways: An abridged Cochrane diagnostic test accuracy systematic review. Anaesthesia 2019, 74, 915–928. [Google Scholar] [CrossRef] [Green Version]
- Vannucci, A.; Cavallone, L.F. Bedside predictors of difficult intubation: A systematic review. Minerva Anestesiol. 2016, 82, 69–83. [Google Scholar]
- Detsky, M.E.; Jivraj, N.; Adhikari, N.K.; Friedrich, J.O.; Pinto, R.; Simel, D.L.; Wijeysundera, D.N.; Scales, D.C. Will This Patient Be Difficult to Intubate? The Rational Clinical Examination Systematic Review. JAMA 2019, 321, 493–503. [Google Scholar] [CrossRef]
- Yıldırım, İ.; İnal, M.T.; Memiş, D.; Turan, F.N. Determining the Efficiency of Different Preoperative Difficult Intubation Tests on Patients Undergoing Caesarean Section. Balkan Med. J. 2017, 34, 436–443. [Google Scholar] [CrossRef]
- Nørskov, A.K. Preoperative airway assessment—Experience gained from a multicentre cluster randomised trial and the Danish Anaesthesia Database. Dan. Med. J. 2016, 63, B5241. [Google Scholar]
- Dawood, A.S.; Talib, B.Z.; Sabri, I.S. Prediction of difficult intubation by using upper lip bite, thyromental distance and Mallampati score in comparison to Cormack and Lehane classification system. Wiad Lek. 2021, 74, 2305–2314. [Google Scholar] [CrossRef]
- Etezadi, F.; Ahangari, A.; Shokri, H.; Najafi, A.; Khajavi, M.R.; Daghigh, M.; Moharari, R.S. Thyromental height: A new clinical test for prediction of difficult laryngoscopy. Anesth. Analg. 2013, 117, 1347–1351. [Google Scholar] [CrossRef]
- Jain, N.; Das, S.; Kanchi, M. Thyromental height test for prediction of difficult laryngoscopy in patients undergoing coronary artery bypass graft surgical procedure. Ann. Card Anaesth. 2017, 20, 207–211. [Google Scholar]
- Selvi, O.; Kahraman, T.; Senturk, O.; Tulgar, S.; Serifsoy, E.; Ozer, Z. Evaluation of the reliability of preoperative descriptive airway assessment tests in prediction of the Cormack-Lehane score: A prospective randomized clinical study. J. Clin. Anesth. 2017, 36, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Majigoudar, S.S.; Revappa, K.B. Comparison of thyromental height test (TMH) with modified mallampati test and thyromental distance for prediction of difficult laryngoscopy: A prospective study. Indian J. Clin. Anaesth. 2017, 4, 238–241. [Google Scholar]
- Nurullah, M.; Alam, M.S.; Hossen, M.; Shahnawaz, M. Prediction of difficult airway by thyromental height test-a comparison with modified mallampati test. Bangladesh J. Med. Sci. 2018, 17, 455–461. [Google Scholar] [CrossRef]
- Rao, K.V.N.; Dhatchinamoorthi, D.; Nandhakumar, A.; Selvarajan, N.; Akula, H.R.; Thiruvenkatarajan, V. Validity of thyromental height test as a predictor of difficult laryngoscopy: A prospective evaluation comparing modified Mallampati score, interincisor gap, thyromental distance, neck circumference, and neck extension. Indian J. Anaesth. 2018, 62, 603–608. [Google Scholar] [PubMed]
- Panjiar, P.; Kochhar, A.; Bhat, K.M.; Bhat, M.A. Comparison of thyromental height test with ratio of height to thyromental distance, thyromental distance, and modified Mallampati test in predicting difficult laryngoscopy: A prospective study. J. Anaesthesiol. Clin. Pharmacol. 2019, 35, 390–395. [Google Scholar] [CrossRef]
- Yabuki, S.; Iwaoka, S.; Murakami, M.; Miura, H. Reliability of the thyromental height test for prediction of difficult visualisation of the larynx: A prospective external validation. Indian J. Anaesth. 2019, 63, 270–276. [Google Scholar] [CrossRef]
- Mostafa, M.; Saeed, M.; Hasanin, A.; Badawy, S.; Khaled, D. Accuracy of thyromental height test for predicting difficult intubation in elderly. J. Anesth. 2020, 34, 217–223. [Google Scholar] [CrossRef]
- Rawal, P.; Shrestha, S.M. The Evaluation of Thyromental Height Test as a Single, Accurate Predictor of Difficult Laryngoscopy. J. Nepal Health Res. Counc. 2020, 18, 271–276. [Google Scholar] [CrossRef]
- Carvalho, C.C.; Santos Neto, J.M.; Orange, F.A. Predictive performance of thyromental height for difficult laryngoscopies in adults: A systematic review and meta-analysis. Braz. J. Anesthesiol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.M.; Zaky, M.N.; El-Mekawy, N.M.; Ollaek, M.A.; Sami, W.M.; Mohamed, D.M. Evaluation of thyromental height test in prediction of difficult airway in obese surgical patients: An observational study. Indian J. Anaesth. 2021, 65, 880–885. [Google Scholar] [CrossRef] [PubMed]
- Bhanushali, A.; Date, A. Evaluation of upper lip bite test and thyromental height test for prediction of difficult laryngoscopy: A prospective observational study. Airway 2021, 4, 185–190. [Google Scholar]
- Chhatrapati, S.; Bloria, S.; Singh, N.; Paul, S.; Luthra, A.; Kataria, K.K.; Vithani, S.; Omar, S.; Nayanar, V.K.N. Comparison of modified Mallampati test and thyromental height test for preoperative airway assessment: A prospective observational study. Indian Anaesth. Forum 2021, 22, 47–52. [Google Scholar]
- Kheirabadi, D.; Honarmand, A.; Rasouli, M.R.; Safavi, M.R.; Maracy, M.R. Comparison of airway assessment tests for prediction of difficult intubation in obese patients: Importance of thyromental height and upper lip bite test. Minerva Anestesiol. 2021, 88, 114–120. [Google Scholar] [CrossRef]
- Panjiar, P.; Bhat, K.M.; Yousuf, I.; Kochhar, A.; Ralli, T. Study comparing different airway assessment tests in predicting difficult laryngoscopy: A prospective study in geriatric patients. Indian J. Anaesth. 2021, 65, 309–315. [Google Scholar] [CrossRef]
- Prakash, S.; Mullick, P.; Singh, R. Evaluation of thyromental height as a predictor of difficult laryngoscopy and difficult intubation: A cross-sectional observational study. Braz. J. Anesthesiol. 2021. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.; QUADAS-2 Group. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- The Cochrane Collaboration. Review Manager (RevMan), Version 5.4.1; The Cochrane Collaboration: London, UK, 2020. [Google Scholar]
- StataCorp LLC. StataCorp, Stata Statistical Software: Release 16; StataCorp LLC: College Station, TX, USA, 2019. [Google Scholar]
- Yang, Y.; Chen, M.; Shi, J.; Mo, H.Z.; Wu, Y.M.; Zou, X.H. Accuracy of modified thyromental height in predicting difficult laryngoscopy. Chin. J. Anesth. 2018, 38, 466–469. [Google Scholar]
- Si, Y.N.; Wang, X.L.; Shi, L. Comparison of predictive capability of different methods for difficult laryngoscopy. J. Clin. Anesthesiol. 2017, 33, 11–14. (In Chinese) [Google Scholar]
- Cao, J. Analysis of the effectiveness of different methods for predicting difficult airway laryngoscope intubation. Med. Inform. 2018, 31, 186–188. (In Chinese) [Google Scholar]
- Luo, J.Y.; Yang, Q.; He, F.F.; Liu, L.Y.; Ou-Yang, J. Accuracy of modified thyromental height test in predicting difficult laryngoscopy. J. Reg. Anat. Oper. Surg. 2020, 29, 836–839. (In Chinese) [Google Scholar]
- Li, M. The Effectiveness of Ultrasound Measurement of Upper Airway Anatomical Parameters in Predicting Difficult Airway. Master’s Thesis, China National Knowledge, Online. 2021. [Google Scholar] [CrossRef]
- Cao, Y.H.; Zhao, Y.X.; Chi, P. The value of thyromental height in predicting of difficult laryngoscopy. Beijing Med. J. 2016, 38, 880–882. [Google Scholar]
- Cao, Y.H.; Chi, P.; He, H.L. Diagnostic accuracy of ratio of height to thyromental distance for difficult laryngoscopy in Chinese population. Chin. J. Clin. 2017, 45, 81–83. (In Chinese) [Google Scholar]
- Carsetti, A.; Sorbello, M.; Adrario, E.; Donati, A.; Falcetta, S. Airway Ultrasound as Predictor of Difficult Direct Laryngoscopy: A Systematic Review and Meta-analysis. Anesth. Analg. 2022, 134, 740–750. [Google Scholar] [CrossRef]
- Lee, A.; Fan, L.T.; Gin, T.; Karmakar, M.K.; Ngan Kee, W.D. A systematic review (meta-analysis) of the accuracy of the Mallampati tests to predict the difficult airway. Anesth. Analg. 2006, 102, 1867–1878. [Google Scholar] [CrossRef]
- Faramarzi, E.; Soleimanpour, H.; Khan, Z.H.; Mahmoodpoor, A.; Sanaie, S. Upper lip bite test for prediction of difficult airway: A systematic review. Pak. J. Med. Sci. 2018, 34, 1019–1023. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Years | Countries | Mean Age; Years | Male; % | Female; % | Mean Height; cm | Mean Weight; kg | Mean BMI | Total Sample Size | DL; n (%) | Thresholds; cm |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Etezadi | 2013 | Iran | 44.5 | 47.5 | 52.5 | 166.1 | 72.0 | 25.8 | 314 | 23 (7.3) | 5 |
| Cao | 2016 | China | 43.0 | 56.7 | 43.3 | NA | NA | 24.2 | 120 | 5 (4.2) | 5 |
| Cao | 2017 | China | 42.0 | 58.0 | 42.0 | NA | NA | 25.2 | 200 | 8 (4) | 5 |
| Jain | 2017 | India | 56.7 | NA | NA | 162.6 | 65.3 | 24.7 | 345 | 32 (9.3) | 5 |
| Selvi | 2017 | Turkey | 48.5 | 51.0 | 49.0 | NA | 77.7 | NA | 451 | 37 (8.2) | 5 |
| 4.35 | |||||||||||
| Si | 2017 | China | 51.4 | NA | NA | 165.0 | NA | 25.8 | 300 | 22 (7.3) | 4.9 |
| Cao | 2018 | China | 44.6 | 56.0 | 44.0 | NA | 61.3 | NA | 200 | 24 (12) | 4.9 |
| Majigoudar | 2018 | India | 39.8 | 53.3 | 46.7 | NA | NA | 21.3 | 60 | 4 (6.7) | 5 |
| Nurullah | 2018 | Bangladesh | 45.4 | 50.4 | 49.6 | NA | NA | NA | 139 | 43 (31) | 5 |
| Rao | 2018 | Australia | 43.4 | 47.2 | 52.8 | 162.6 | 62.0 | 23.4 | 316 | 26 (8.2) | 5 |
| Yang | 2018 | China | 47.0 | 43.3 | 56.7 | 161.0 | NA | 23.0 | 263 | 24 (10) | 3.92 |
| Panjiar | 2019 | India | 37.2 | 43.6 | 56.4 | 158.4 | 61.1 | 24.5 | 550 | 55 (10) | 5 |
| Yabuki | 2019 | Japan | 50.2 | 18.0 | 82.0 | 159.6 | 58.6 | 22.9 | 609 | 6 (1) | 5 with BURP |
| 5.4 with BURP | |||||||||||
| 73 (12) | 5 without BURP | ||||||||||
| 5.4 without BURP | |||||||||||
| Luo | 2020 | China | 49.9 | 38.4 | 61.6 | 160.6 | 62.4 | NA | 263 | 13 (4.9) | 3.9 |
| Mostafa | 2020 | Egypt | 68.0 | 57.0 | 43.0 | NA | NA | 27.1 | 120 | 15 (12) | 5.7 |
| Rawal | 2020 | Nepal | 35.8 | 44.3 | 55.7 | 158.0 | 60.9 | 24.1 | 246 | 7 (2.8) | 5 |
| Ahmed | 2021 | Egypt | 38.3 | 78.1 | 21.9 | NA | NA | 43.7 | 105 | 23 (21.9) | 4.7 |
| Bhanushali | 2021 | India | 51.7 | 40.4 | 59.6 | 162.4 | NA | NA | 109 | 16 (14.7) | 5 |
| Chhatrapati | 2021 | India | 36.8 | 53.3 | 46.7 | NA | 55.2 | NA | 150 | 50 (30) | 5 |
| Kheirabadi | 2021 | Iran | 41.3 | 32.1 | 67.9 | NA | NA | 35.7 | 196 | 48 (24.5) | 4.8 |
| Li | 2021 | China | NA | 52.0 | 48.0 | NA | NA | NA | 400 | 53 (13.25) | 4.805 |
| Panjiar | 2021 | India | 69.4 | 48.4 | 58.6 | 154.1 | 54.2 | 23.1 | 140 | 35 (25) | 5.5 |
| Prakash | 2021 | India | 40.9 | 60.7 | 39.3 | 162.4 | 60.3 | 22.9 | 300 | 46 (15.3) | 5 |
| 4.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, W.; Tian, T.; Li, X.; Jiang, T.; Xue, F. Use of the Thyromental Height Test for Prediction of Difficult Laryngoscopy: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 4906. https://doi.org/10.3390/jcm11164906
Chen W, Tian T, Li X, Jiang T, Xue F. Use of the Thyromental Height Test for Prediction of Difficult Laryngoscopy: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(16):4906. https://doi.org/10.3390/jcm11164906
Chicago/Turabian StyleChen, Wenxuan, Tian Tian, Xintao Li, Tianyu Jiang, and Fushan Xue. 2022. "Use of the Thyromental Height Test for Prediction of Difficult Laryngoscopy: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 16: 4906. https://doi.org/10.3390/jcm11164906
APA StyleChen, W., Tian, T., Li, X., Jiang, T., & Xue, F. (2022). Use of the Thyromental Height Test for Prediction of Difficult Laryngoscopy: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 11(16), 4906. https://doi.org/10.3390/jcm11164906