
Assessment of the Patient’s Emotional Response with the RobHand Rehabilitation Platform: A Case Series Study

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. RobHand Rehabilitation Platform
2.2.1. Mechatronic Device
2.2.2. Passive Training Control
2.2.3. Software Environment
2.3. Self-Assessment Manikin Test
2.4. Experimental Setup and Protocol
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Forster, A.; Young, J. Stroke rehabilitation: Can we do better? Br. Med. J. 1992, 305, 1446–1447. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Rodriguez-Guerrero, C.; Knaepen, K.; Fraile-Marinero, J.C.; Perez-Turiel, J.; Gonzalez-de-Garibay, V.; Lefeber, D. Improving challenge/skill ratio in a multimodal interface by simultaneously adapting game difficulty and haptic assistance through psychophysiological and performance feedback. Front. Neurosci. 2017, 11, 242. [Google Scholar] [CrossRef]
- Guadagnoll, M.A.; Lee, T.D. Challenge Point: A Framework for Conceptualizing the Effects of Various Practice Conditions in Motor Learning. J. Mot. Behav. 2004, 36, 212–224. [Google Scholar] [CrossRef] [PubMed]
- Guerrero, C.R.; Marinero, J.C.F.; Turiel, J.P.; Muñoz, V. Using ‘human state aware’ robots to enhance physical human-robot interaction in a cooperative scenario. Comput. Methods Programs Biomed. 2019, 112, 250–259. [Google Scholar] [CrossRef] [PubMed]
- Coombes, S.A.; Cauraugh, J.H.; Janelle, C.M. Emotion and movement: Activation of defensive circuitry alters the magnitude of a sustained muscle contraction. Neurosci. Lett. 2006, 396, 192–196. [Google Scholar] [CrossRef]
- Yerkes, R.M.; Dodson, J.D. The Relation of Strength of Stimulus to Rapidity of Habit Formation. J. Comp. Neurol. Psychol. 1908, 18, 459–482. [Google Scholar] [CrossRef]
- Diamond, D.M.; Campbell, A.M.; Park, C.R.; Halonen, J.; Zoladz, P.R. The temporal dynamics model of emotional memory processing: A synthesis on the neurobiological basis of stress-induced amnesia, flashbulb and traumatic memories, and the Yerkes-Dodson law. Neural Plast. 2007, 2007, 60803. [Google Scholar] [CrossRef] [PubMed]
- Csikszentmihalyi, M.; Csikszentmihalyi, I.S. (Eds.) Optimal Experience: Psychological Studies of Flow in Consciousness; Cambridge University Press: New York, NY, USA, 1988. [Google Scholar]
- Holden, M.K. Virtual Environments for Motor Rehabilitation: Review. CyberPsychol. Behav. 2005, 8, 187–211. [Google Scholar] [CrossRef] [PubMed]
- Ostir, G.V.; Ivonne-Marie, B.; Ottenbacher, M.E.; Clow, A.; Ottenbacher, K.J. Associations between Positive Emotion and Recovery of Functional Status Following Stroke. Psychosom. Med. 2008, 70, 404–409. [Google Scholar] [CrossRef] [PubMed]
- Colombo, R.; Pisano, F.; Mazzone, A.; Delconte, C.; Micera, S.; Carrozza, M.C.; Dario, P.; Minuco, G. Design strategies to improve patient motivation during robot-aided rehabilitation. J. Neuroeng. Rehabil. 2007, 4, 3. [Google Scholar] [CrossRef] [PubMed]
- Maclean, N.; Pound, P.; Wolfe, C.; Rudd, A. The concept of patient motivation: A qualitative of stroke professionals’ attitudes. Stroke 2002, 33, 444–448. [Google Scholar] [CrossRef] [PubMed]
- Béjot, Y.; Bailly, H.; Graber, M.; Garnier, L.; Laville, A.; Dubourget, L.; Mielle, N.; Chevalier, C.; Durier, J.; Giroud, M. Impact of the ageing population on the burden of stroke: The dijon stroke registry. Neuroepidemiology 2019, 52, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Donnan, G.A.; Fisher, M.; Macleod, M.; Davis, S.M. Stroke. Lancet 2008, 371, 1612–1623. [Google Scholar] [CrossRef]
- Rechel, B.; Doyle, Y.; Grundy, E.; McKee, M. How can health systems respond to population ageing? In EU2009.C2. Policy Brief 10. Health Systems and Policy Analysis; WHO: Geneva, Switzerland, 2009; Volume 10, pp. 463–469. [Google Scholar]
- Mane, R.; Chouhan, T.; Guan, C. BCI for stroke rehabilitation: Motor and beyond. J. Neural Eng. 2020, 17, 041001. [Google Scholar] [CrossRef] [PubMed]
- Ekman, P. An Argument for Basic Emotions. Cogn. Emot. 1992, 6, 169–200. [Google Scholar] [CrossRef]
- Russell, J.A. A circumplex model of affect. J. Pers. Soc. Psychol. 1980, 39, 1161–1178. [Google Scholar] [CrossRef]
- Mihelj, M.; Novak, D.; Munih, M. Emotion-aware system for upper extremity rehabilitation. In Proceedings of the 2009 Virtual Rehabilitation International Conference, Haifa, Israel, 29 June 2009–2 July 2009; pp. 160–165. [Google Scholar]
- Mehrabian, A. Basic Dimensions for a General Psychological Theory: Implications for Personality, Social, Environmental, and Developmental Studies; Oelgeschlager, Gunn & Hain: Cambridge, UK, 1980. [Google Scholar]
- Bradley, M.M.; Lang, P.J. Measuring emotion: The self-assessment manikin and the semantic differential. J. Behav. Ther. Exp. Psychiat. 1994, 25, 49–59. [Google Scholar] [CrossRef]
- Villar, B.F.; Viñas, P.F.; Turiel, J.P.; Marinero, J.C.F.; Gordaliza, A. Influence on the user’s emotional state of the graphic complexity level in virtual therapies based on a robot-assisted neuro-rehabilitation platform. Comput. Methods Programs Biomed. 2020, 190, 105359. [Google Scholar] [CrossRef] [PubMed]
- Peter, C.; Herbon, A. Emotion representation and physiology assignments in digital systems. Interact. Comput. 2006, 18, 139–170. [Google Scholar] [CrossRef]
- Mandryk, R.L.; Atkins, M.S. A fuzzy physiological approach for continuously modeling emotion during interaction with play technologies. Int. J. Hum. Comput. Stud. 2007, 65, 329–347. [Google Scholar] [CrossRef]
- Bakker, I.; van der Voordt, T.; Vink, P.; de Boon, J. Pleasure, Arousal, Dominance: Mehrabian and Russell revisited. Curr. Psychol. 2014, 33, 405–421. [Google Scholar] [CrossRef]
- Russell, J.A.; Weiss, A.; Mendelsohn, G.A. Affect Grid: A Single-Item Scale of Pleasure and Arousal. J. Pers. Soc. Psychol. 1989, 57, 493–502. [Google Scholar] [CrossRef]
- Kreibig, S.D. Autonomic nervous system activity in emotion: A review. Biol. Psychol. 2010, 84, 394–421. [Google Scholar] [CrossRef] [PubMed]
- Ekman, P.; Levenson, R.W.; Friesen, W.V. Autonomic nervous system activity distinguishes among emotions. Science 1983, 221, 1208–1210. [Google Scholar] [CrossRef] [PubMed]
- Zhai, J.; Barreto, A.B.; Chin, C.; Li, C. Realization of stress detection using psychophysiological signals for improvement of human-computer interactions. In Proceedings of the IEEE Southeastcon, Ft. Lauderdale, FL, USA, 8–10 April 2005; pp. 415–420. [Google Scholar]
- Mower, E.; Feil-Seifer, D.J.; Matarić, M.J.; Narayanan, S. Investigating implicit cues for user state estimation in human-robot interaction using physiological measurements. In Proceedings of the 16th IEEE International Conference on Robot and Human Interactive Communication, Jeju, Korea, 26–29 August 2007; pp. 1125–1130. [Google Scholar]
- Liu, C.; Conn, K.; Sarkar, N.; Stone, W. Physiology-based affect recognition for computer-assisted intervention of children with Autism Spectrum Disorder. Int. J. Hum. Comput. Stud. 2008, 66, 662–677. [Google Scholar] [CrossRef]
- Gümüslü, E.; Barkana, D.E.; Köse, H. Emotion Recognition Using EEG and Physiological Data for Robot-Assisted Rehabilitation System. In Proceedings of the Companion Publication of the 2020 International Conference on Multimodal Interaction, New York, NY, USA, 25–29 October 2020; pp. 379–387. [Google Scholar]
- Choi, E.J.; Kim, D.K. Arousal and valence classification model based on long short-term memory and DEAP data for mental healthcare management. Healthc. Inform. Res. 2018, 24, 309–316. [Google Scholar] [CrossRef]
- Juan, V.M.; Cisnal, A.; Fraile, J.; Pérez-Turiel, J.; de la Fuente, E. Design and Characterization of a Lightweight Underactuated RACA Hand Exoskeleton for Neurorehabilitation. Rob. Auton. Syst. 2021, 143, 103828. [Google Scholar]
- Cisnal, A.; Perez-Turiel, J.; Fraile, J.C.; Sierra, D.; de la Fuente, E. RobHand: A Hand Exoskeleton with Real-Time EMG-Driven Embedded Control. Quantifying Hand Gesture Recognition Delays for Bilateral Rehabilitation. IEEE Access 2021, 9, 137809–137823. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing. Vienna, Australia. 2016. Available online: https://www.R-project.org/ (accessed on 28 June 2022).
- Subramanian, S.K.; Lourenço, C.B.; Chilingaryan, G.; Sveistrup, H.; Levin, M.F. Arm motor recovery using a virtual reality intervention in chronic stroke: Randomized control trial. Neurorehabil. Neural Repair 2013, 27, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Crosbie, J.H.; Lennon, S.; McGoldrick, M.C.; McNeill, M.D.; Burke, J.W.; McDonough, S.M. Virtual reality in the rehabilitation of the upper limb after hemiplegic stroke: A randomised pilot study. Screen 2008, 229, 235. [Google Scholar]
- Posner, J.; Russell, J.A.; Gerber, A.; Gorman, D.; Colibazzi, T.; Yu, S.; Wang, Z.; Kangarlu, A.; Zhu, H.; Peterson, B.S. The neurophysiological bases of emotion: An fMRI study of the affective circumplex using emotion-denoting words. Hum. Brain Mapp. 2009, 30, 883–895. [Google Scholar] [CrossRef] [PubMed]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dimension | Adjective Pairs |
|---|---|
| Valence | Unhappy–Happy Annoyed–Pleased Unsatisfied–Satisfied |
| Arousal | Relaxed–Stimulated Calm–Excited Sluggish–Frenzied |
| Dominance | Controlled–Controlling Influenced–Influential Cared for–In control |
| Patient | Sex | Age | Laterality Diagnosis |
|---|---|---|---|
| P1 | male | 61 | Left Ischemic stroke |
| P2 | male | 43 | Left Ischemic stroke |
| P3 | male | 22 | Right Ischemic stroke |
| P4 | female | 38 | Right Ischemic stroke |
| P5 | male | 53 | Right Ischemic stroke |
| Therapies | Movement-Based Exercises | Virtual Environment |
|---|---|---|
| (T1) | (a) | Virtual hand only |
| (T2) | (c) | Virtual hand only |
| (T3) | (b) | Virtual hand only |
| (T4) | (a) | Virtual kitchen |
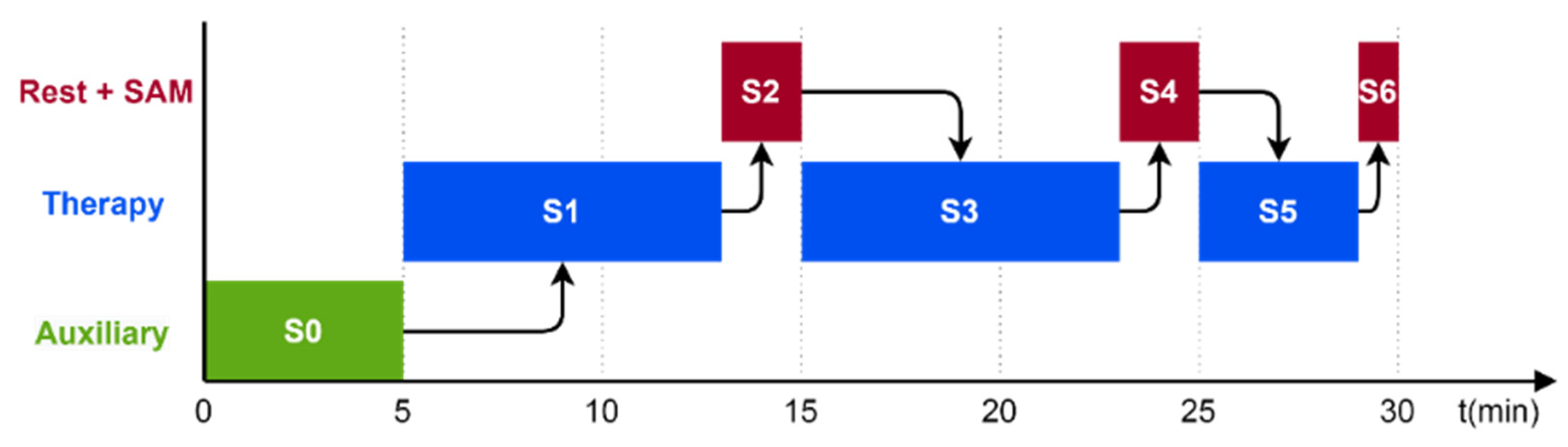
| Action | Duration | |
|---|---|---|
| Stage 0 (S0) | Placement of exoskeleton on the patients’ hand | 5 min |
| Stage 1 (S1) | Hand flexion/extension therapy (T1) and precision grips (T2) | 8 min |
| Stage 2 (S2) | Rest break and SAM test (SAM1) | 2 min |
| Stage 3 (S3) | Individual finger flexion/extension therapy (T3) | 8 min |
| Stage 4 (S4) | Rest break and SAM test (SAM2) | 2 min |
| Stage 5 (S5) | Squeeze oranges therapy (T4) | 4 min |
| Stage 6 (S6) | SAM test (SAM3) | 1 min |
| Total | 30 min |
| Df | Sum Sq. | Mean Sq. | F Value | Pr (>F) | Significance | |
|---|---|---|---|---|---|---|
| Valence | ||||||
| Phase | 2 | 3.56 | 1.7812 | 7.220 | 0.000845 | * |
| Test Stage | 2 | 1.60 | 0.8017 | 3.249 | 0.039960 | * |
| Residuals | 354 | 87.34 | 0.2467 | |||
| Arousal | ||||||
| Phase | 2 | 2.01 | 1.0028 | 4.409 | 0.0128 | * |
| Test Stage | 2 | 1.69 | 0.8457 | 3.718 | 0.0252 | * |
| Residuals | 354 | 80.52 | 0.2274 | |||
| Dominance | ||||||
| Phase | 2 | 2.99 | 1.4942 | 5.892 | 0.00304 | * |
| Test Stage | 2 | 2.65 | 1.3251 | 5.225 | 0.00580 | * |
| Residuals | 354 | 89.78 | 0.2536 | |||
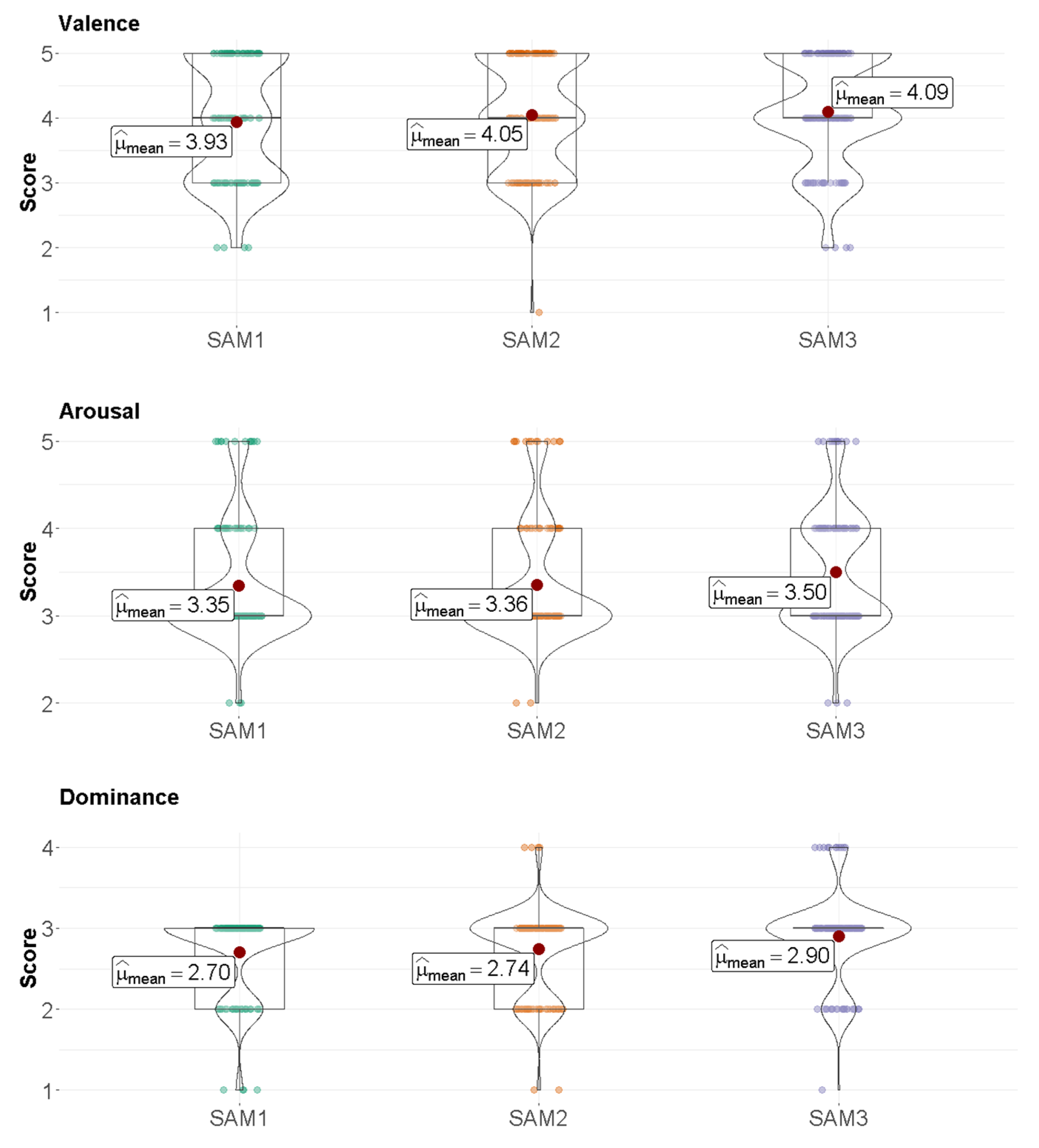
| Significance | Difference | Lower Limit | Upper Limit | p-Value | |
|---|---|---|---|---|---|
| Valence | |||||
| SAM1–SAM2 | 0.11570248 | −0.034488475 | 0.2658934 | 0.1666449 | |
| SAM1–SAM3 | * | 0.15702479 | 0.006833839 | 0.3072157 | 0.0380506 |
| SAM2–SAM3 | 0.04132231 | −0.108868641 | 0.1915133 | 0.7937554 | |
| Arousal | |||||
| SAM1–SAM2 | 0.008264463 | −0.135800455 | 0.1523294 | 0.9899934 | |
| SAM1–SAM3 | * | 0.148760331 | 0.004695413 | 0.2928252 | 0.0411630 |
| SAM2–SAM3 | 0.140495868 | −0.003569050 | 0.2845608 | 0.0577416 | |
| Dominance | |||||
| SAM1–SAM2 | 0.04132231 | −0.110641128 | 0.1932858 | 0.7980122 | |
| SAM1–SAM3 | * | 0.19834711 | 0.046383666 | 0.3503105 | 0.0064807 |
| SAM2–SAM3 | * | 0.15702479 | 0.005061352 | 0.3089882 | 0.0409853 |
| Significance | Difference | Lower Limit | Upper Limit | p-Value | |
|---|---|---|---|---|---|
| Valence | |||||
| Initial–Middle | * | −0.2655285 | −0.40773323 | −0.1233237 | 0.0000436 |
| Initial–Final | 0.1133333 | −0.04253927 | 0.2692059 | 0.2023516 | |
| Middle–Final | * | 0.3788618 | 0.21670056 | 0.5410230 | 0.0000002 |
| Arousal | |||||
| Initial–Middle | * | −0.40422764 | −0.5407669 | −0.2676884 | 0.0000000 |
| Initial–Final | * | −0.41777778 | −0.5674403 | −0.2681153 | 0.0000000 |
| Middle–Final | −0.01355014 | −0.1692507 | 0.1421505 | 0.9771383 | |
| Dominance | |||||
| Initial– Middle | 0.1248780 | −0.01930057 | 0.2690567 | 0.1045848 | |
| Initial–Final | * | 0.2422222 | 0.08418607 | 0.4002584 | 0.0010288 |
| Middle–Final | 0.1173442 | −0.04706790 | 0.2817562 | 0.2143593 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cisnal, A.; Moreno-SanJuan, V.; Fraile, J.C.; Turiel, J.P.; de-la-Fuente, E.; Sánchez-Brizuela, G. Assessment of the Patient’s Emotional Response with the RobHand Rehabilitation Platform: A Case Series Study. J. Clin. Med. 2022, 11, 4442. https://doi.org/10.3390/jcm11154442
Cisnal A, Moreno-SanJuan V, Fraile JC, Turiel JP, de-la-Fuente E, Sánchez-Brizuela G. Assessment of the Patient’s Emotional Response with the RobHand Rehabilitation Platform: A Case Series Study. Journal of Clinical Medicine. 2022; 11(15):4442. https://doi.org/10.3390/jcm11154442
Chicago/Turabian StyleCisnal, Ana, Victor Moreno-SanJuan, Juan Carlos Fraile, Javier P. Turiel, Eusebio de-la-Fuente, and Guillermo Sánchez-Brizuela. 2022. "Assessment of the Patient’s Emotional Response with the RobHand Rehabilitation Platform: A Case Series Study" Journal of Clinical Medicine 11, no. 15: 4442. https://doi.org/10.3390/jcm11154442
APA StyleCisnal, A., Moreno-SanJuan, V., Fraile, J. C., Turiel, J. P., de-la-Fuente, E., & Sánchez-Brizuela, G. (2022). Assessment of the Patient’s Emotional Response with the RobHand Rehabilitation Platform: A Case Series Study. Journal of Clinical Medicine, 11(15), 4442. https://doi.org/10.3390/jcm11154442