
Bing-Neel Syndrome, a Rare Presentation of Waldenström Macroglobulinemia—A Multicenter Report by the Polish Lymphoma Research Group

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Population and Outcome
2.3. Diagnosis of BNS
2.4. Response to Treatment
2.5. Statistical Analysis
3. Results
3.1. Patients
3.2. Diagnosis
3.3. Treatment
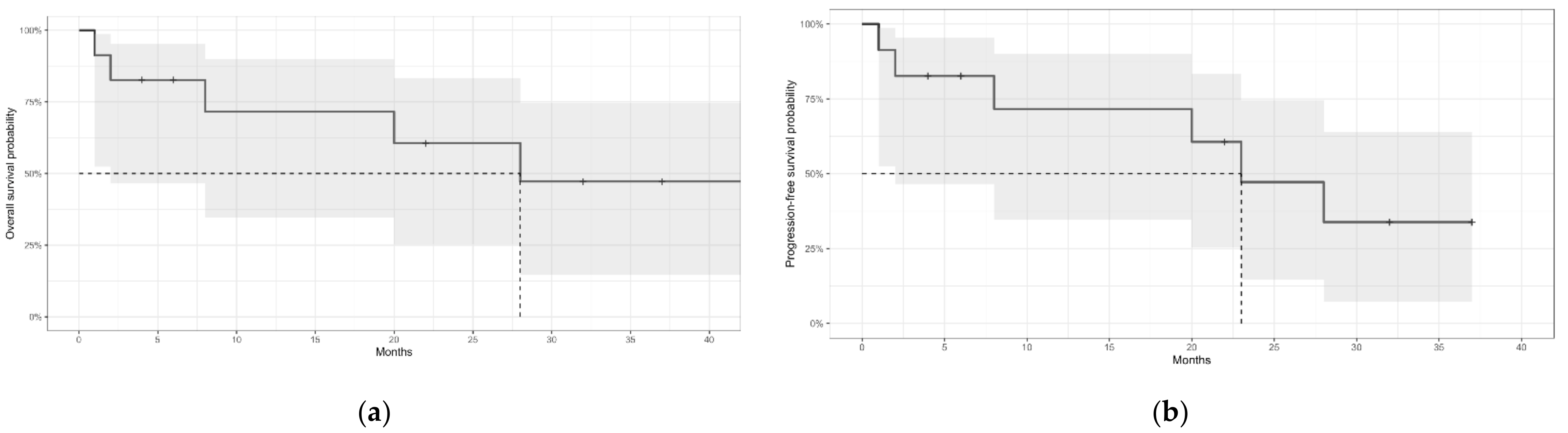
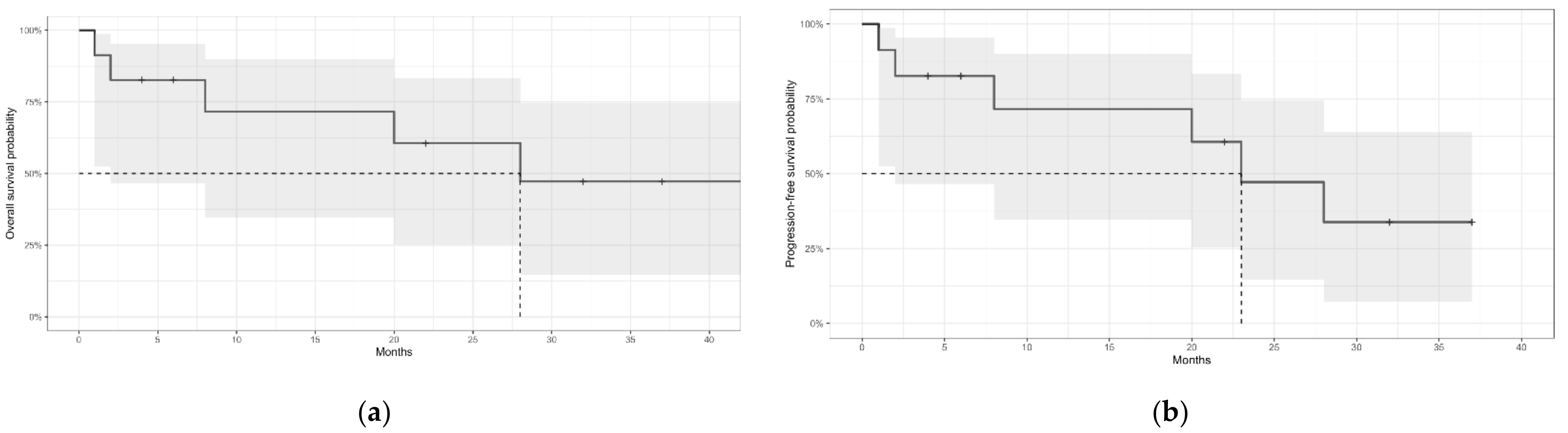
3.4. Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kastritis, E.; Leblond, V.; Dimopoulos, M.A.; Kimby, E.; Staber, P.; Kersten, M.J.; Tedeschi, A.; Buske, C.; ESMO Guidelines Committee. Waldenström’s macroglobulinaemia: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29 (Suppl. 4), iv41–iv50. [Google Scholar]
- Wang, H.; Chen, Y.; Li, F.; Delasalle, K.; Wang, J.; Alexanian, R.; Kwak, L.; Rustveld, L.; Du, X.L.; Wang, M. Temporal and geographic variations of Waldenstrom macroglobulinemia incidence: A large population-based study. Cancer 2012, 118, 3793–3800. [Google Scholar] [CrossRef]
- Kulkarni, M.T.; Treon, S.P.; Manning, R.; Xu, L.; Rinne, M.; Lee, E.Q.; Ghobrial, I.M.; Norden, A.; Kluk, M.J.; Nayak, L. Clinical Characteristics and Treatment Outcome of CNS Involvement (Bing-Neel Syndrome) in Waldenstrom’s Macroglobulinemia. Blood 2013, 122, 5090. [Google Scholar] [CrossRef]
- Minnema, M.C.; Kimby, E.; D’Sa, S.; Fornecker, L.M.; Poulain, S.; Snijders, T.J. Guideline for the diagnosis, treatment and response criteria for Bing-Neel syndrome. Haematologica 2017, 102, 43–51. [Google Scholar] [CrossRef] [Green Version]
- Varettoni, M.; Defrancesco, I.; Diamanti, L.; Marchioni, E.; Farina, L.M.; Pichiecchio, A. Bing-Neel Syndrome: Illustrative Cases and Comprehensive Review of the Literature. Mediterr. J. Hematol. Infect. Dis. 2017, 9, e2017061. [Google Scholar] [CrossRef] [Green Version]
- Vos, J.M.I.; Kersten, M.-J.; Kraan, W.; Groeneveld, O.N.; Linn, C.; Pals, S.T.; Minnema, M.C. Effective treatment of Bing-Neel Syndrome with oral fludarabine: A case series of four consecutive patients. Br. J. Haematol. 2016, 172, 461–464. [Google Scholar] [CrossRef]
- Varettoni, M.; Marchioni, E.; Bonfichi, M.; Picchiecchio, A.; Arcaini, L.; Arbasino, C.; Gotti, M.; Da Vià, K.; Delmonte, M.; Sciarra, R.; et al. Successful treatment with Rituximab and Bendamustine in a patient with newly diagnosed Waldenström’s Macroglobulinemia complicated by Bing-Neel syndrome. Am. J. Hematol. 2015, 90, E152–E153. [Google Scholar] [CrossRef] [Green Version]
- Simon, L.; Fitsiori, A.; Lemal, R.; Dupuis, J.; Carpentier, B.; Boudin, L.; Corby, A.; Aurran-Schleinitz, T.; Gastaud, L.; Talbot, A.; et al. Bing-Neel syndrome, a rare complication of Waldenström macroglobulinemia: Analysis of 44 cases and review of the literature. A study on behalf of the French Innovative Leukemia Organization (FILO). Haematologica 2015, 100, 1587–1594. [Google Scholar] [CrossRef] [Green Version]
- Castillo, J.J.; D’Sa, S.; Lunn, M.; Minnema, M.C.; Tedeschi, A.; Lansigan, F.; Palomba, M.L.; Varettoni, M.; Garcia-Sanz, R.; Nayak, L.; et al. Central nervous system involvement by Waldenström macroglobulinaemia (Bing-Neel syndrome): A multi-institutional retrospective study. Br. J. Haematol. 2016, 172, 709–715. [Google Scholar] [CrossRef] [Green Version]
- Castillo, J.J.; Itchaki, G.; Paludo, J.; Varettoni, M.; Buske, C.; Eyre, T.A.; Chavez, J.C.; Shain, K.H.; Issa, S.; Palomba, M.S.; et al. Ibrutinib for the treatment of Bing-Neel syndrome: A multicenter study. Blood 2019, 133, 299–305. [Google Scholar] [CrossRef] [Green Version]
- Simon, L.; Lemal, R.; Fornecker, L.M.; Tournilhac, O.; Leblond, V. High-dose therapy with autologous stem cells transplantation in Bing-Neel syndrome: A retrospective analysis of 14 cases. Am. J. Hematol. 2019, 94, E227–E229. [Google Scholar] [CrossRef] [PubMed]
- Giebel, S.; Basak, G.; Bieniaszewska, M.; Czerw, T.; Czyż, A.; Drozd-Sokołowska, J.; Dytfeld, D.; Giannopoulos, K.; Gil, L.; Helbig, G.; et al. Current status and achievements of Polish haemato-oncology. Acta Haematol. Pol. 2021, 52, 4–17. [Google Scholar] [CrossRef]
- Korfel, A.; Elter, T.; Thiel, E.; Hänel, M.; Möhle, R.; Schroers, R.; Reiser, M.; Dreyling, M.; Eucker, J.; Scholz, C.; et al. Phase II study of central nervous system (CNS)-directed chemotherapy including high-dose chemotherapy with autologous stem cell transplantation for CNS relapse of aggressive lymphomas. Haematologica 2013, 98, 364–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castillo, J.J.; Treon, S.P. How we manage Bing-Neel syndrome. Br. J. Haematol. 2019, 187, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Cabannes-Hamy, A.; Lemal, R.; Goldwirt, L.; Poulain, S.; Amorim, S.; Pérignon, R.; Berger, J.; Brice, P.; De Kerviler, E.; Bay, J.-O.; et al. Efficacy of ibrutinib in the treatment of Bing-Neel syndrome. Am. J. Hematol. 2016, 91, E17–E19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernard, S.; Goldwirt, L.; Amorim, S.; Brice, P.; Brière, J.; de Kerviler, E.; Mourah, S.; Sauvageon, H.; Thieblemont, C. Activity of ibrutinib in mantle cell lymphoma patients with central nervous system relapse. Blood 2015, 126, 1695–1698. [Google Scholar] [CrossRef]
- Mason, C.; Savona, S.; Rini, J.N.; Castillo, J.J.; Xu, L.; Hunter, Z.R.; Treon, S.P.; Allen, S.L. Ibrutinib penetrates the blood brain barrier and shows efficacy in the therapy of Bing Neel syndrome. Br. J. Haematol. 2017, 179, 339–341. [Google Scholar] [CrossRef]
- Hartsell, L.; Janes, A.; Larck, C.; Park, S.; Arnall, J.R. Ibrutinib for the treatment of Bing-Neel syndrome, a complication of Waldenström macroglobulinemia: Patient case report. J. Oncol. Pharm. Pract. 2019, 25, 1534–1539. [Google Scholar] [CrossRef] [PubMed]
- Boudin, L.; Patient, M.; Roméo, E.; Bladé, J.S.; de Jauréguiberry, J.P. Efficacy of ibrutinib as first-line treatment of tumoral Bing-Neel syndrome. Leuk. Lymphoma 2018, 59, 2746–2748. [Google Scholar] [CrossRef]
- Wong, J.; Cher, L.; Griffiths, J.; Cohen, A.; Huang, J.; Wang, L.; Gregory, G.; Opat, S. Efficacy of Zanubrutinib in the Treatment of Bing-Neel Syndrome. Hemasphere 2018, 30, e155. [Google Scholar] [CrossRef]
- Oyama, T.; Taoka, K.; Chiba, A.; Matsuda, K.; Maki, H.; Masamoto, Y.; Kurokawa, M. A Case of Bing-Neel Syndrome Successfully Treated with Tirabrutinib. Intern. Med. 2022, 2022, 9545-22. [Google Scholar] [CrossRef]
- Frustaci, A.M.; Rusconi, C.; Picardi, P.; Veronese, S.; Montillo, M.; Cairoli, R.; Tedeschi, A. Bing Neel Syndrome in a Previously Untreated Patient with Waldenström’s Macroglobulinemia: Contribution of MYD88 L265P Mutation on Cerebrospinal Fluid. Clin. Lymphoma Myeloma Leuk. 2016, 16, e7–e9. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Number of Patients | Median Age at BNS (Range) | Sex (Males) | Median Time from WM to BNS (Range) | Simultaneous Diagnosis | The Most Frequent Symptoms | Localization | First-Line Treatment | ORR to the First-Line Treatment | Overall Survival | Progression-Free Survival | Adverse Prognostic Factors | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Castillo et al. [9] | 34 | 62 (39–76) | 19 (56%) | 3 years (0–16) | 15% | Motor deficits of the limbs (35%); altered mental status (35%), cranial nerve symptoms (29%) | NR | HD-MTX-based (41%); Intrathecal-based (19%); HD-MTX + HD-AraC-based (16%) | 66% | 3-year: 59% (95% CI, 39–75%) | NR | Age > 65 years; PLT < 100 × 109/L; treatment for WM prior to BNS |
| Simon et al. [8] | 44 | 63 (47–84 ) | 35 (80%) | 8.9 years (0.8–25) (non-simultaneous diagnosis) | 36% | Balance disorder/ disturbed gait (48%); cranial nerve symptoms (36%); cognitive impairment (27%) | Diffuse-93%; Tumoral-9% | HD-MTX-based (41%); Intrathecal-based (9%); HD-MTX + HD-AraC-based (9%) | 70% | 5-year: 71%; 10-year 59% | Median 26 months | Not analyzed |
| Kulkarni et al. [3] | 13 | 60 (51–75) | NR | 6.3 years (0.3–11.9) | 0% | Seizures, hearing loss, cognitive impairment, gait instability, lower extremity weakness | NR | HD-MTX-based (62%); Intrathecal-based (23%); BR (8%) | 45% | Median not reached | NR | Not analyzed |
| Varettoni et al. [5] | 4 | 62 (38–68) | 3 (75%) | NR | 75% | Motor deficits (50%); ataxia (50%); cognitive impairment (25%); seizures (25%) | Diffuse-75%; Tumoral-25% | Intrathecal-based (75%); BR (75%) | 75% | NR | NR | Not analyzed |
| Patients treated with a specific therapy | ||||||||||||
| Vos et al. [6]—only patients treated with fludarabine | 4 | 60 (41–70) | 1 (25%) | simultaneous | 100% | Motor deficits (50%); cognitive impairment (50%); sensory deficits (25%); seizures (25%) | Diffuse-100% | Fludarabine-based (100%) | 100% | 2-year OS 100% | 2-year PFS 100% | Not analyzed |
| Castillo et al. [10]- only patients treated with ibrutinib | 28 | 65 (38–81) | 16 (57%) | 4.0 years (0–26.7) | NR | Motor deficits (46%); cognitive impairment (39%); sensory deficits (39%) | NR | Ibrutinib | 41% | 2-year Ibrutinib-OS 81% (95% CI, 49–94%) | 2-year EFS 80% | Not identified |
| Simon et al. [11]– only patients treated with auto-HCT | 14 | 61 (52–67) | 9 (64%) | NR | NR | NR | NR | HD-AraC-based (57%); HD-MTX-based (7%); HD-MTX + HD-AraC-based (7%) | NR | NR | NR | Not analyzed |
| N (%) | |
|---|---|
| Number of patients | 11 |
| Sex | |
| Female | 6 (55%) |
| Male | 5 (45%) |
| At WM diagnosis | |
| Age at WM diagnosis, median (range), years | 59 (32–65) |
| Previous MGUS | 1 (9%) |
| Performance status according to ECOG (missing: 2) | |
| 0 | 2 (22%) |
| 1 | 3 (33%) |
| 2 | 2 (22%) |
| 3 | 1 (11%) |
| 4 | 1 (11%) |
| IPSSWM (missing: 2) | |
| Low | 3 (33%) |
| Intermediate | 4 (44%) |
| High | 2 (22%) |
| At BNS diagnosis | |
| Age at BNS diagnosis, median (range), years | 61 (47–72) |
| Performance status according to ECOG (missing: 1) | |
| 0 | 0 (0%) |
| 1 | 3 (30%) |
| 2 | 2 (20%) |
| 3 | 3 (30%) |
| 4 | 2 (20%) |
| Time from WM diagnosis to BNS, median (range), years | 3.5 (0–17.2) |
| Simultaneous WM and BNS diagnosis | 1 (9%) |
| Diagnosis of BNS within 30 days from WM diagnosis | 2 (18%) |
| Number of lines of therapy for WM before BNS diagnosis, median (range) | 3 (0–7) |
| Previous treatment (any line) | |
| Chlorambucil | 2 (18%) |
| Fludarabine/cladribine | 5 (45%) |
| BR | 1 (9%) |
| DRC | 4 (36%) |
| BDR | 2 (18%) |
| Rituximab (missing: 1) | 5 (50%) |
| Auto-HCT for WM before BNS diagnosis | 1 (9%) |
| Status of WM at BNS diagnosis (missing: 1) | |
| OR | 1 (10%) |
| SD | 1 (10%) |
| PD | 3 (30%) |
| On treatment before response assessment | 3 (30%) |
| Untreated | 2 (20%) |
| Extramedullary WM disease (other than CNS), (missing: 1) | 4 (40%) |
| Peripheral neuropathy, (missing 1) | 6 (60%) |
| Laboratory parameters | |
| Hemoglobin, median (range), g/dL, (missing: 1) | 10.3 (8.3–14.8) |
| Platelets, median (range), ×109/L, (missing: 1) | 190 (15–288) |
| Neutrophils, median (range), ×109/L, (missing: 1) | 2.5 (0.4–4.9) |
| Lymphocytes, median (range), ×109/L, (missing: 1) | 1 (0.1–1.5) |
| IgM concentration, median (range), g/L, (missing: 1) | 10.2 (1.9–95.7) |
| IgG concentration, median (range), g/L, (missing: 2) | 7 (1.4–13) |
| FLC kappa/lambda ratio (missing: 1) | 2.01 (0.004–691) |
| N (%) | |
|---|---|
| Number of patients | 11 |
| Time from the symptoms onset to diagnosis, median (range), months (missing: 1) | 2.3 (0.5–63.9) |
| Symptoms | |
| Headaches | 4 (36%) |
| Gait disorders | 4 (36%) |
| Sensory symptoms | 3 (27%) |
| Cognitive deficits | 2(18%) |
| Dysarthria | 1 (9%) |
| Confusion | 1 (9%) |
| Depressed level of consciousness | 0 (0%) |
| Paresis | 3 (27%) |
| Seizures | 1 (9%) |
| Cranial nerve involvement (facial nerve) | 1 (9%) |
| Visual disturbances | 2 (18%) |
| Hearing impairment/hearing loss | 2 (18%) |
| Psychiatric symptoms | 1 (9%) |
| Diagnostic procedures | |
| MRI of the brain and spinal cord | 8 (73%) |
| Abnormal | 7/8 (88%) |
| CT of the brain | 1 (9%) |
| Cerebrospinal fluid | |
| Leukocytes in CSF, median (range), /mm3 (missing: 2) | 33 (3–214) |
| Protein in CSF, median (range), mg/dL (missing: 1) | 188 (32–1616) |
| Flow cytometry analysis of CSF (missing: 1) | 7 (70%) |
| Abnormal result | 7/7 (100%) |
| Protein electrophoresis of CSF | 2 (18%) |
| Abnormal | 1/2 (50%) |
| Immunofixation of CSF | 4 (36%) |
| IgM | 4/4 (100%) |
| Analysis of MYD88 L265P in CSF (missing: 1) | 3 (30%) |
| Detectable MYD88 L265P in CSF | 3/3 (100%) |
| Biopsy of a CNS lesion | 0 (0%) |
| Disease localization | |
| Disease localization (missing: 1) | |
| Meningeal involvement | 4 (40%) |
| Parenchymal involvement | 2 (20%) |
| Both meningeal and parenchymal | 4 (40%) |
| Encephalon involvement (missing: 1) | 5 (50%) |
| Spinal cord involvement (missing: 1) | 1 (10%) |
| Treatment of BNS | |
| The first line systemic therapy for BNS (N = 11) | |
| HD-MTX-based | 4 (36%) |
| HD-AraC-based | 2 (18%) |
| DRC | 3 (27%) |
| BR | 1 (9%) |
| VCD | 1 (9%) |
| Ibrutinib | 2 (18%) |
| 420 mg | 1 (9%) |
| 560 mg | 1 (9%) |
| Rituximab (in combination) | 6 (55%) |
| Radiotherapy | 1 (9%) |
| The 1st salvage systemic therapy for BNS (N = 2) | |
| HD-MTX/HD-AraC | 1 (50%) |
| HD-AraC-Temozolomid + auto-HCT | 1 (50%) |
| The 2nd salvage systemic therapy for BNS (N = 1) | |
| Ibrutinib (420 mg) | 1 (100%) |
| Intrathecal therapy | 7 (64%) |
| Plasmaphereses | 3 (27%) |
| Allo-HCT for BNS | 0 (0%) |
| Cumulative response to treatment | |
| CR | 2 (18%) |
| uCR | 2 (18%) |
| PR | 4 (36%) |
| NR | 0 (0%) |
| Early death during treatment | 1 (9%) |
| Not assessed | 2 (18%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drozd-Sokołowska, J.; Waszczuk-Gajda, A.; Witkowska, M.; Sienkiewicz, E.; Kopińska, A.; Kołkowska-Leśniak, A.; Barankiewicz, J.; Długosz-Danecka, M.; Smolewski, P.; Helbig, G.; et al. Bing-Neel Syndrome, a Rare Presentation of Waldenström Macroglobulinemia—A Multicenter Report by the Polish Lymphoma Research Group. J. Clin. Med. 2022, 11, 4447. https://doi.org/10.3390/jcm11154447
Drozd-Sokołowska J, Waszczuk-Gajda A, Witkowska M, Sienkiewicz E, Kopińska A, Kołkowska-Leśniak A, Barankiewicz J, Długosz-Danecka M, Smolewski P, Helbig G, et al. Bing-Neel Syndrome, a Rare Presentation of Waldenström Macroglobulinemia—A Multicenter Report by the Polish Lymphoma Research Group. Journal of Clinical Medicine. 2022; 11(15):4447. https://doi.org/10.3390/jcm11154447
Chicago/Turabian StyleDrozd-Sokołowska, Joanna, Anna Waszczuk-Gajda, Magdalena Witkowska, Elżbieta Sienkiewicz, Anna Kopińska, Agnieszka Kołkowska-Leśniak, Joanna Barankiewicz, Monika Długosz-Danecka, Piotr Smolewski, Grzegorz Helbig, and et al. 2022. "Bing-Neel Syndrome, a Rare Presentation of Waldenström Macroglobulinemia—A Multicenter Report by the Polish Lymphoma Research Group" Journal of Clinical Medicine 11, no. 15: 4447. https://doi.org/10.3390/jcm11154447
APA StyleDrozd-Sokołowska, J., Waszczuk-Gajda, A., Witkowska, M., Sienkiewicz, E., Kopińska, A., Kołkowska-Leśniak, A., Barankiewicz, J., Długosz-Danecka, M., Smolewski, P., Helbig, G., Lech-Marańda, E., Jurczak, W., Biecek, P., Giebel, S., Wiktor-Jędrzejczak, W., & Basak, G. (2022). Bing-Neel Syndrome, a Rare Presentation of Waldenström Macroglobulinemia—A Multicenter Report by the Polish Lymphoma Research Group. Journal of Clinical Medicine, 11(15), 4447. https://doi.org/10.3390/jcm11154447