
Changes in the Care Activity in Addiction Centers with Dual Pathology Patients during the COVID-19 Pandemic

 , ,
, ,
Abstract
:1. Introduction
- (a)
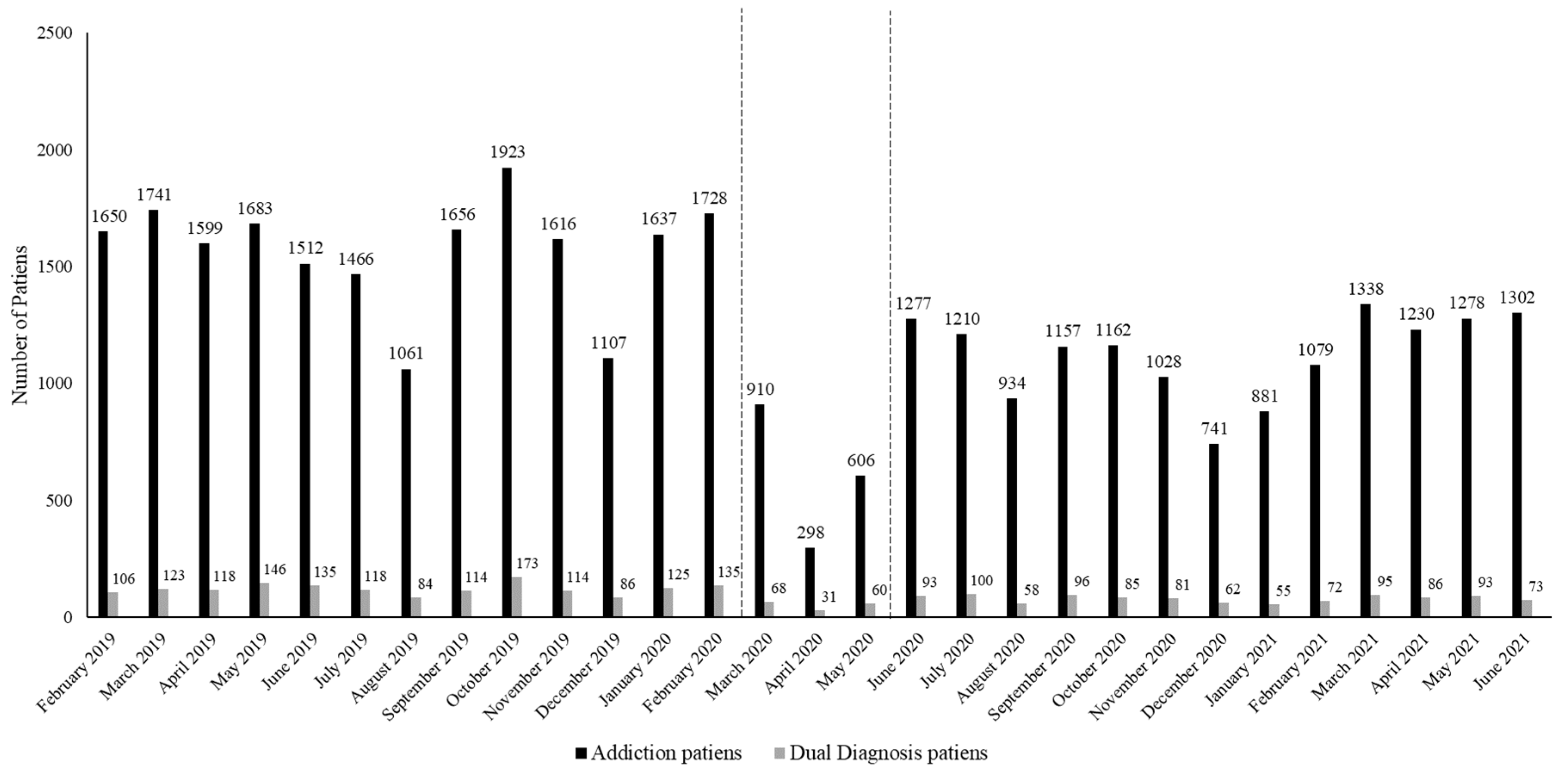
- The evolution of admissions to treatment decreased during confinement;
- (b)
- Patients with dual pathology who attend addiction care centers presented changes in their sociodemographic, consumption, and diagnosis profiles during the pandemic compared to the previous period;
- (c)
- Care indicators related to therapeutic appointments, toxicological tests, and treatment abandonment changed during the pandemic compared to the previous period.
2. Material and Methods
2.1. Design
2.2. Participants
2.3. Procedure
2.4. Ethics and Approvals
2.5. Statistical Analysis
3. Results
3.1. Evolution of Treatment Admissions between 1 February 2019 and 30 June 2021
3.2. Sociodemographic Characteristics, Consumption Patterns, and Comorbid Diagnoses
3.3. Care Provision Indicators
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chiappini, S.; Guirguis, A.; John, A.; Corkery, J.M.; Schifano, F. COVID-19: The Hidden Impact on Mental Health and Drug Addiction. Front. Psychiatry 2020, 11, 767. [Google Scholar] [CrossRef]
- Da, B.L.; Im, G.Y.; Schiano, T.D. COVID-19 Hangover: A Rising Tide of Alcohol Use Disorder and Alcohol-Associated Liver Disease. Hepatology 2020, 72, 1102–1108. [Google Scholar] [CrossRef] [PubMed]
- Ornell, F.; Moura, H.F.; Scherer, J.N.; Pechansky, F.; Kessler, F.H.P.; von Diemen, L. The COVID-19 Pandemic and Its Impact on Substance Use: Implications for Prevention and Treatment. Psychiatry Res. 2020, 289, 113096. [Google Scholar] [CrossRef] [PubMed]
- García-Rivera, B.R.; García-Alcaraz, J.L.; Mendoza-Martínez, I.A.; Olguin-Tiznado, J.E.; García-Alcaráz, P.; Aranibar, M.F.; Camargo-Wilson, C. Influence of COVID-19 Pandemic Uncertainty in Negative Emotional States and Resilience as Mediators against Suicide Ideation, Drug Addiction and Alcoholism. Int. J. Environ. Res. Public Health 2021, 18, 12891. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.Z.; Ahmed, O.; Aibao, Z.; Hanbin, S.; Siyu, L.; Ahmad, A. Epidemic of COVID-19 in China and Associated Psychological Problems. Asian J. Psychiatry 2020, 51, 102092. [Google Scholar] [CrossRef]
- Erquicia, J.; Valls, L.; Barja, A.; Gil, S.; Miquel, J.; Leal-Blanquet, J.; Schmidt, C.; Checa, J.; Vega, D. Emotional Impact of the COVID-19 Pandemic on Healthcare Workers in One of the Most Important Infection Outbreaks in Europe. Clin. Med. 2020, 155, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Yang, L.; Zhang, C.; Xiang, Y.-T.; Liu, Z.; Hu, S.; Zhang, B. Online Mental Health Services in China during the COVID-19 Outbreak. Lancet Psychiatry 2020, 7, e17–e18. [Google Scholar] [CrossRef]
- Nicolini, H. Depresión y Ansiedad En Los Tiempos de La Pandemia de COVID-19. Cirugía Cirujanos 2020, 88, 542–547. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, M.D.; Mamun, M.A. COVID-19 Suicidal Behavior among Couples and Suicide Pacts: Case Study Evidence from Press Reports. Psychiatry Res. 2020, 289, 113105. [Google Scholar] [CrossRef]
- Allen, B.; El Shahawy, O.; Rogers, E.S.; Hochman, S.; Khan, M.R.; Krawczyk, N. Association of Substance Use Disorders and Drug Overdose with Adverse COVID-19 Outcomes in New York City: January–October 2020. J. Public Health 2020, 43, 462–465. [Google Scholar] [CrossRef]
- Dubey, M.J.; Ghosh, R.; Chatterjee, S.; Biswas, P.; Chatterjee, S.; Dubey, S. COVID-19 and Addiction. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 817–823. [Google Scholar] [CrossRef] [PubMed]
- Wildberger, J.; Wenzel, K.; Fishman, M. Assessing Clinical Impacts and Attitudes Related to COVID-19 among Residential Substance Use Disorder Patients. Subst. Abus. 2022, 43, 756–762. [Google Scholar] [CrossRef] [PubMed]
- Finlay, I.; Gilmore, I. COVID-19 and Alcohol—A Dangerous Cocktail. BMJ 2020, 369, m1987. [Google Scholar] [CrossRef] [PubMed]
- The Nielsen Company. Rebalancing the “COVID-19 Effect” on Alcohol Sales. Available online: https://nielseniq.com/global/en/insights/analysis/2020/rebalancing-the-covid-19-effect-on-alcohol-sales/ (accessed on 3 May 2021).
- MacKillop, J.; Cooper, A.; Costello, J. National Retail Sales of Alcohol and Cannabis during the COVID-19 Pandemic in Canada. JAMA Netw. Open 2021, 4, e2133076. [Google Scholar] [CrossRef]
- Pollard, M.S.; Tucker, J.S.; Green, H.D. Changes in Adult Alcohol Use and Consequences during the COVID-19 Pandemic in the US. JAMA Netw. Open 2020, 3, e2022942. [Google Scholar] [CrossRef]
- Rolland, B.; Haesebaert, F.; Zante, E.; Benyamina, A.; Haesebaert, J.; Franck, N. Global Changes and Factors of Increase in Caloric/Salty Food, Screen, and Substance Use, during the Early COVID-19 Containment Phase in France: A General Population Online Survey. JMIR Public Health Surveill. 2020, 6, e19630. [Google Scholar] [CrossRef]
- Been, F.; Emke, E.; Matias, J.; Baz-Lomba, J.A.; Boogaerts, T.; Castiglioni, S.; Campos-Mañas, M.; Celma, A.; Covaci, A.; de Voogt, P.; et al. Changes in Drug Use in European Cities during Early COVID-19 Lockdowns—A Snapshot from Wastewater Analysis. Environ. Int. 2021, 153, 106540. [Google Scholar] [CrossRef]
- Chappuy, M.; Peyrat, M.; Lejeune, O.; Duvernay, N.; David, B.; Joubert, P.; Lack, P. Drug Consumption during Prolonged Lockdown due to COVID-19 as Observed in French Addiction Center. Therapies 2021, 76, 379–382. [Google Scholar] [CrossRef]
- Gili, A.; Bacci, M.; Aroni, K.; Nicoletti, A.; Gambelunghe, A.; Mercurio, I.; Gambelunghe, C. Changes in Drug Use Patterns during the COVID-19 Pandemic in Italy: Monitoring a Vulnerable Group by Hair Analysis. Int. J. Environ. Res. Public Health 2021, 18, 1967. [Google Scholar] [CrossRef]
- Schmidt, R.A.; Genois, R.; Jin, J.; Vigo, D.; Rehm, J.; Rush, B. The Early Impact of COVID-19 on the Incidence, Prevalence, and Severity of Alcohol Use and Other Drugs: A Systematic Review. Drug Alcohol Depend. 2021, 228, 109065. [Google Scholar] [CrossRef]
- Slavova, S.; Rock, P.; Bush, H.M.; Quesinberry, D.; Walsh, S.L. Signal of Increased Opioid Overdose during COVID-19 from Emergency Medical Services Data. Drug Alcohol Depend. 2020, 214, 108176. [Google Scholar] [CrossRef] [PubMed]
- Imtiaz, S.; Nafeh, F.; Russell, C.; Ali, F.; Elton-Marshall, T.; Rehm, J. The Impact of the Novel Coronavirus Disease (COVID-19) Pandemic on Drug Overdose-Related Deaths in the United States and Canada: A Systematic Review of Observational Studies and Analysis of Public Health Surveillance Data. Subst. Abus. Treat. Prev. Policy 2021, 16, 1–14. [Google Scholar] [CrossRef]
- Kilian, C.; Rehm, J.; Allebeck, P.; Braddick, F.; Gual, A.; Barták, M.; Bloomfield, K.; Gil, A.; Neufeld, M.; O’Donnell, A.; et al. Alcohol Consumption during the COVID-19 Pandemic in Europe: A Large-Scale Cross-Sectional Study in 21 Countries. Addiction 2021, 116, 3369–3380. [Google Scholar] [CrossRef]
- Mark, T.L.; Gibbons, B.; Barnosky, A.; Padwa, H.; Joshi, V. Changes in Admissions to Specialty Addiction Treatment Facilities in California During the COVID-19 Pandemic. JAMA Netw. Open 2021, 4, e2117029. [Google Scholar] [CrossRef] [PubMed]
- Aguilar, L.; Vicente-Hernández, B.; Remón-Gallo, D.; García-Ullán, L.; Valriberas-Herrero, I.; Maciá-Casas, A.; Pérez-Madruga, A.; Garzón, M.Á.; Álvarez-Navares, A.; Roncero, C. A Real-World Ten-Week Follow-up of the COVID Outbreak in an Outpatient Drug Clinic in Salamanca (Spain). J. Subst. Abus. Treat. 2021, 125, 108303. [Google Scholar] [CrossRef] [PubMed]
- Milani, R.M.; Keller, A.; Roush, S. Dual Diagnosis Anonymous (DDA) and the Transition to Online Support During COVID-19. J. Concurr. Disord. 2021. [Google Scholar] [CrossRef]
- Arya, S.; Gupta, R. COVID-19 outbreak: Challenges for Addiction services in India. Asian J. Psychiatry 2020, 51, 102086. [Google Scholar] [CrossRef]
- Green, T.C.; Bratberg, J.; Finnell, D.S. Opioid use disorder and the COVID 19 pandemic: A call to sustain regulatory easements and further expand access to treatment. Subst. Abus. 2020, 41, 147–149. [Google Scholar] [CrossRef]
- Cance, J.D.; Doyle, E. Changes in Outpatient Buprenorphine Dispensing During the COVID-19 Pandemic. JAMA 2020, 324, 2442–2444. [Google Scholar] [CrossRef]
- Huskamp, H.A.; Busch, A.B.; Uscher-Pines, L.; Barnett, M.L.; Riedel, L.; Mehrotra, A. Treatment of Opioid Use Disorder Among Commercially Insured Patients in the Context of the COVID-19 Pandemic. JAMA 2020, 324, 2440–2442. [Google Scholar] [CrossRef]
- Torrens-Mèlich, M. Dual pathology: Current situation and future challenges. Adicciones 2008, 20, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Tirado-Muñoz, J.; Farré, A.; Mestre-Pintó, J.; Szerman, N.; Torrens, M. Dual pathology in depression: Recommendations in treatment. Adicciones 2017, 30, 66–76. [Google Scholar] [CrossRef]
- Sivertsen, K.; Sørly, R.; Mydland, T.; Ekberg, J.I. Perspectives on Challenges and Opportunities in Norwegian Peer Recovery Services for People Living with Dual Diagnosis During a Pandemic. J. Patient Exp. 2021, 8, 237437352199695. [Google Scholar] [CrossRef] [PubMed]
- Daigre, C.; Grau-López, L.; Palma-Álvarez, R.F.; Perea-Ortueta, M.; Sorribes-Puertas, M.; Serrano-Pérez, P.; Quesada, M.; Segura, L.; Coronado, M.; Ramos-Quiroga, J.A.; et al. A Multicenter Study on the Impact of Gender, Age, and Dual Diagnosis on Substance Consumption and Mental Health Status in Outpatients Treated for Substance Use Disorders during COVID-19 Lockdown. J. Dual Diagn. 2022, 18, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Grau-López, L.; Daigre, C.; Palma-Álvarez, R.F.; Sorribes-Puertas, M.; Serrano-Pérez, P.; Quesada-Franco, M.; Segura, L.; Coronado, M.; Ramos-Quiroga, J.A.; Colom, J. COVID-19 Lockdown and Consumption Patterns among Substance Use Disorder Outpatients: A Multicentre Study. Eur. Addict. Res. 2022, 28, 243–254. [Google Scholar] [CrossRef]
- Sher, L. Dual disorders and suicide during and following the COVID-19 pandemic. Acta Neuropsychiatr. 2021, 33, 49–50. [Google Scholar] [CrossRef]
- Rao, R.; Mueller, C.; Broadbent, M. Dual diagnosis in older drinkers during the COVID-19 pandemic. Adv. Dual Diagn. 2021, 14, 70–79. [Google Scholar] [CrossRef]
- Gastón-Guerrero, A. Dual pathology: Drug dependence and depression. Apunt. Psicol. 2021, 38, 13–22. [Google Scholar]
- Ries, R.K. Serial, parallel and integrated models of dual diagnosis treatment. J. Health Care Poor Underserved 1992, 3, 173–180. [Google Scholar] [CrossRef]
- Arenas, F.; Ariza, M.J. Protocolo de Actuación Conjunta Entre Unidades de Salud Mental Comunitaria y Centros de Tratamiento Ambulatorio de Drogodependencias; Servicio Andaluz de Salud: Seville, Spain, 2012. [Google Scholar]
- European Monitoring Centre for Drugs and Drug Addiction. Treatment Demand Indicator (TDI) Standard Protocol 3.0: Guidelines for Reporting Data on People Entering Drug Treatment in European Countries; EMCDDA: Lisbon, Portugal, 2012.
- Dacosta-Sánchez, D.; Díaz-Batanero, C.; Fernández-Calderón, F.; Lozano, O.M. Impact of cluster B personality disorders in drugs therapeutic community treatment outcomes: A study based on Real World Data. J. Clin. Med. 2021, 10, 2572. [Google Scholar] [CrossRef]
- Roncero, C.; Vicente-Hernández, B.; Casado-Espada, N.M.; Aguilar, L.; Gamonal-Limcaoco, S.; Garzón, M.A.; Martínez-González, F.; Llanes-Álvarez, C.; Martínez, R.; Franco-Martín, M.; et al. The Impact of COVID-19 Pandemic on the Castile and Leon Addiction Treatment Network: A Real-Word Experience. Front. Psychiatry 2020, 11, 575755. [Google Scholar] [CrossRef] [PubMed]
- di Lorenzo, R.; Frattini, N.; Dragone, D.; Farina, R.; Luisi, F.; Ferrari, S.; Bandiera, G.; Rovesti, S.; Ferri, P. Psychiatric Emergencies During the COVID-19 Pandemic: A 6-Month Observational Study. Neuropsychiatr. Dis. Treat. 2021, 17, 1763–1778. [Google Scholar] [CrossRef] [PubMed]
- Harris, M.T.H.; Peterkin, A.; Bach, P.; Englander, H.; Lapidus, E.; Rolley, T.; Weimer, M.B.; Weinstein, Z.M. Adapting inpatient addiction medicine addiction consult services during the COVID-19 pandemic. Addict. Sci. Clin. Pract. 2021, 16, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Manthey, J.; Kilian, C.; Carr, S.; Bartak, M.; Bloomfield, K.; Braddick, F.; Rehm, J. Use of alcohol, tobacco, cannabis, and other substances during the first wave of the SARS-CoV-2 pandemic in Europe: A survey on 36,000 European substance users. Subst. Abus. Treat. Prev. Policy 2021, 16, 1–11. [Google Scholar] [CrossRef]
- Bonati, M.; Campi, R.; Segre, G. Psychological impact of the quarantine during the COVID-19 pandemic on the general European adult population: A systematic review of the evidence. Epidemiol. Psychiatr. Sci. 2022, 31, e27. [Google Scholar] [CrossRef]
- Preti, E.; di Pierro, R.; Fanti, E.; Madeddu, F.; Calati, R. Personality disorders in time of pandemic. Curr. Psychiatry Rep. 2020, 22, 1–9. [Google Scholar] [CrossRef]
- Patel, R.; Irving, J.; Brinn, A.; Broadbent, M.; Shetty, H.; McGuire, P. Impact of the COVID-19 pandemic on remote mental healthcare and prescribing in psychiatry: An electronic health record study. BMJ Open 2021, 11, e046365. [Google Scholar] [CrossRef]
- Mancheño-Barba, J.J.; Navas-León, S.; Gutiérrez-López, M.L.; Rosa-Cáceres, A.D.L.; Cáceres-Pachón, P. Analysis of the profiles of patients with dual pathology attending addiction centers, mental health centers, and a coordinated service. Ann. Psychol. 2019, 35, 233–241. [Google Scholar] [CrossRef] [Green Version]
- Mancheño-Barba, J.J.; Navas-León, S.; Fernández-Calderón, F.; Gutiérrez, M.; Sánchez-García, M.; Díaz-Batanero, C.; Lozano, O.M. Coordinated treatment between addiction and mental health centers vs uncoordinated treatment for patients with dual pathology: Greater dropout, but less deterioration of functional disability. Actas Españolas Psiquiatr. 2021, 49, 71–80. [Google Scholar]

{kind=link}
| Admission Period | Statistics (d.f.) | p | Effect Size | |||
|---|---|---|---|---|---|---|
| 19 February–20 February | March–20 May | 20 June–21 June | ||||
| No. of patients | 1577 (56.6%) | 159 (5.7%) | 1049 (37.7%) | |||
| % Patients (out of total patients) | 7.2 | 8.1 | 6.7 | χ2 (4) = 6.646 | 0.036 * | V = 0.013 |
| Readmissions | 67.4% | 74.8% | 63.2% | χ2 (4) = 10.549 | 0.005 ** | V = 0.062 |
| Sociodemographic variables | ||||||
| Admission age (Mean, SD) | 40.36 (11.536) | 39.25 (11.698) | 40.58 (11.920) | H (2) = 1.482 | 0.477 | ε2 = 0.001 |
| Gender (%) | ||||||
| Male | 75.8 | 72.5 | 73.8 | χ2 (2) = 1.796 | 0.407 | V = 0.025 |
| Female | 24.2 | 27.5 | 26.2 | |||
| Educational level (%) | ||||||
| No education | 17.0 | 14.1 | 14.6 | χ2 (8) = 13.402 | 0.099 | V = 0.049 |
| Primary | 39.1 | 37.8 | 35.3 | |||
| Secondary | 22.3 | 22.4 | 25.6 | |||
| Baccalaureate/Degree | 14.9 | 20.5 | 17.8 | |||
| Higher | 6.7 | 5.1 | 6.8 | |||
| Employment status (%) | ||||||
| Employed | 22.7 | 18.5 | 23.3 | χ2 (8) = 6.830 | 0.555 | V = 0.035 |
| Unemployed | 44.9 | 45.9 | 44.8 | |||
| Retired | 24.7 | 26.1 | 25.1 | |||
| Student | 3.5 | 6.4 | 3.6 | |||
| Others | 4.2 | 3.2 | 3.1 | |||
| Main referral source (%) | ||||||
| Legal Services | 3.1 | 4.4 | 2.5 | χ2 (10) = 7.263 | 0.700 | V = 0.036 |
| Own initiative | 41.9 | 48.1 | 42.2 | |||
| Family members | 13.2 | 8.9 | 12.8 | |||
| Health Services | 14.4 | 13.9 | 15.7 | |||
| Social Services | 23.3 | 22.2 | 22.7 | |||
| Others | 4.1 | 2.5 | ||||
| Variables related to consumption | ||||||
| Age of onset of consumption (Mean, SD) | 19.64 (10.91) | 20.81 (14.28) | 19.74 (11.29) | H (2) = 0.739 | 0.691 | ε2 = 0.000 |
| Admission drug (%) | ||||||
| Alcohol | 36.4 | 34.4 | 39.3 | 2.930 | 0.231 | V = 0.032 |
| Cocaine | 34.1 | 30.6 | 33.4 | 0.819 | 0.664 | V = 0.017 |
| Cannabis | 23.4 | 20.2 | 4.447 | 0.108 | V = 0.040 | |
| Opioids | 18.3 | 21.3 | 12.5 | 18.840 | 0.000 ** | V = 0.082 |
| Hypnosedatives | 2.9 | 4.4 | 3.5 | 1.455 | 0.483 | V = 0.023 |
| Pathological gambling | 4.7 | 1.9 | 4.7 | 2.759 | 0.252 | V = 0.031 |
| Other drugs used prior to admission (%) | ||||||
| Alcohol | 55.6 | 55.0 | 58.0 | χ2 (2) = 1.522 | 0.467 | V = 0.023 |
| Cocaine | 36.8 | 35.0 | 39.4 | χ2 (2) = 2.284 | 0.319 | V = 0.029 |
| Cannabis | 39.9 | 40.6 | 37.4 | χ2 (2) = 1.901 | 0.387 | V = 0.026 |
| Opioids | 18.6 | 22.5 | 13.7 | χ2 (2) = 14.231 | 0.001 ** | V = 0.071 |
| Hypnosedatives | 8.1 | 6.3 | 7.9 | χ2 (2) = 0.653 | 0.721 | V = 0.015 |
| Frequency of consumption in the 30 days prior to admission (%) | ||||||
| Every day | 44.1 | 45.2 | 42.4 | χ2 (10) = 12.011 | 0.284 | V = 0.048 |
| 4–6 days/week | 7.4 | 5.1 | 9.1 | |||
| 2–3 days/week | 13.9 | 12.7 | 14.1 | |||
| 1 day/week | 5.5 | 10.8 | 5.9 | |||
| Less 1 day/week | 7.8 | 6.4 | 8.2 | |||
| Did not consume | 21.3 | 19.7 | 20.4 | |||
| Variables related to the diagnosis of comorbid mental disorders | ||||||
| F 20. Schizophrenia, schizotypal disorders, and delusional disorders | 16.2 | 16.4 | 16.2 | 0.004 | 0.998 | V = 0.001 |
| F 30–39. Mood disorders | 17.4 | 13.8 | 16.9 | 1.297 | 0.523 | V = 0.022 |
| F 40–49. Neurotic, secondary to stressful situations, and somatoform disorders | 31.9 | 34.0 | 32.6 | 0.362 | 0.834 | V = 0.011 |
| F 41. Mixed Anxiety-Depressive Disorder | 16.8 | 20.1 | 17.6 | 1.241 | 0.538 | V = 0.021 |
| F 90. Hyperkinetic disorders | 4.6 | 3.8 | 3.3 | 2.480 | 0.289 | V = 0.030 |
| Mental retardation | 1.3 | 1.9 | 1.5 | 0.409 | 0.815 | V = 0.012 |
| Adult personality and behavioral disorders (%) | ||||||
| Any personality disorder (F 60–F 60.9) | 24.4 | 24.5 | 20.2 | 6.421 | 0.040 * | V = 0.048 |
| F 60.0 and 60.1. Paranoid or schizoid personality disorder | 2.0 | 2.5 | 1.3 | 2.220 | 0.330 | V = 0.028 |
| F 60.2–60.4. Antisocial, borderline, histrionic or narcissistic disorder | 12.6 | 8.8 | 10.9 | 3.268 | 0.195 | V = 0.034 |
| F 60.5–60.7. Avoidance, dependence, or obsessive-compulsive disorder. | 1.2 | 1.3 | 1.0 | 0.394 | 0.821 | V = 0.012 |
| F 60.9. Unspecified Personality disorder | 8.8 | 11.9 | 7.2 | 4.688 | 0.096 | V = 0.041 |
| Patients without specified ICD-10 diagnosis | 13.1 | 10.7 | 16.4 | 7.441 | 0.024 * | V = 0.052 |
| Admission Period | Statistics (d.f.) | p | Effect Size | ||||
|---|---|---|---|---|---|---|---|
| 19 February–20 February | March–20 May | 20 June–21 June | |||||
| Appointments (mean, SD) | |||||||
| Scheduled monthly | 1.12 (2.22) | 0.64 (0.74) | 1.28 (2.32) | H (2) = 62.655 | 0.000 ** | ε2 = 0.023 | |
| Percentage attendance | 0.76 (0.23) | 0.88 (0.25) | 0.77 (0.25) | H (2) = 92.348 | 0.000 ** | ε2 = 0.033 | |
| Toxicological controls (mean, SD) | |||||||
| Alcohol | % Patients tested | 7.7 | 0 | 10.4 | χ2 (2) = 7.701 | 0.021 ** | V = 0.086 |
| Average per patient | 4.91 (4.88) | 0 | 5.72 (14.82) | H (2) = 0.631 | 0.427 | ε2 = 0.000 | |
| Positive ratio | 0.14 (8.75) | 0 | 0.19 (0.35) | H (2) = 3.565 | 0.168 | ε2 = 0.001 | |
| Cocaine | % Patients tested | 53.6 | 24.5 | 45.4 | χ2 (2) = 18.174 | 0.000 ** | V = 0.139 |
| Average per patient | 6.51 (12.75) | 0.8 (1.14) | 5.20 (5.83) | H (2) = 17.721 | 0.000 ** | ε2 = 0.006 | |
| Positive ratio | 0.38 (0.40) | 0.50 (0.58) | 0.37 (0.41) | H (2) = 0.287 | 0.866 | ε2 = 0.000 | |
| Cannabis | % Patients tested | 52.3 | 20.0 | 40.1 | χ2 (2) = 19.761 | 0.000 ** | V = 0.178 |
| Average per patient | 5.16 (6.16) | 1.87 (0.64) | 4.86 (4.59) | H (2) = 6.142 | 0.046 ** | ε2 = 0.002 | |
| Positive ratio | 0.64 (0.42) | 0.63 (0.52) | 0.53 (0.45) | H (2) = 3.437 | 0.179 | ε2 = 0.001 | |
| Opioids | % Patients tested | 45.7 | 14.7 | 37.4 | χ2 (2) = 13.031 | 0.001 ** | V = 0.169 |
| Average per patient | 4.75 (6.69) | 1.60 (0.89) | 5.04 (6.55) | H (2) = 2.825 | 0.243 | ε2 = 0.001 | |
| Positive ratio | 0.30 (0.41) | 0.75 (0.50) | 0.75 (0.29) | H (2) = 28.033 | 0.000 ** | ε2 = 0.010 | |
| Benzodiazepines | % Patients tested | 21.7 | 14.3 | 13.5 | χ2 (2) = 1.013 | 0.603 | V = 0.106 |
| Average per patient | 2.10 (2.18) | 0 | 2.20 (1.30) | H (2) = 2.827 | 0.243 | ε2 = 0.001 | |
| Positive ratio | 0.69 (0.46) | 0 | 0.40 (0.55) | H (2) = 1.296 | 0.255 | ε2 = 0.000 | |
| % Patients that dropped out of treatment | 40.1 | 34.4 | 13.3 | 215.46 | 0.000 | V = 0.280 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mancheño-Velasco, C.; Dacosta-Sánchez, D.; Blanc-Molina, A.; Narvaez-Camargo, M.; Lozano-Rojas, Ó.M. Changes in the Care Activity in Addiction Centers with Dual Pathology Patients during the COVID-19 Pandemic. J. Clin. Med. 2022, 11, 4341. https://doi.org/10.3390/jcm11154341
Mancheño-Velasco C, Dacosta-Sánchez D, Blanc-Molina A, Narvaez-Camargo M, Lozano-Rojas ÓM. Changes in the Care Activity in Addiction Centers with Dual Pathology Patients during the COVID-19 Pandemic. Journal of Clinical Medicine. 2022; 11(15):4341. https://doi.org/10.3390/jcm11154341
Chicago/Turabian StyleMancheño-Velasco, Cinta, Daniel Dacosta-Sánchez, Andrea Blanc-Molina, Marta Narvaez-Camargo, and Óscar Martín Lozano-Rojas. 2022. "Changes in the Care Activity in Addiction Centers with Dual Pathology Patients during the COVID-19 Pandemic" Journal of Clinical Medicine 11, no. 15: 4341. https://doi.org/10.3390/jcm11154341
APA StyleMancheño-Velasco, C., Dacosta-Sánchez, D., Blanc-Molina, A., Narvaez-Camargo, M., & Lozano-Rojas, Ó. M. (2022). Changes in the Care Activity in Addiction Centers with Dual Pathology Patients during the COVID-19 Pandemic. Journal of Clinical Medicine, 11(15), 4341. https://doi.org/10.3390/jcm11154341