
Microbial Spectrum and Antibiotic Resistance in Patients Suffering from Penetrating Crohn’s Disease

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
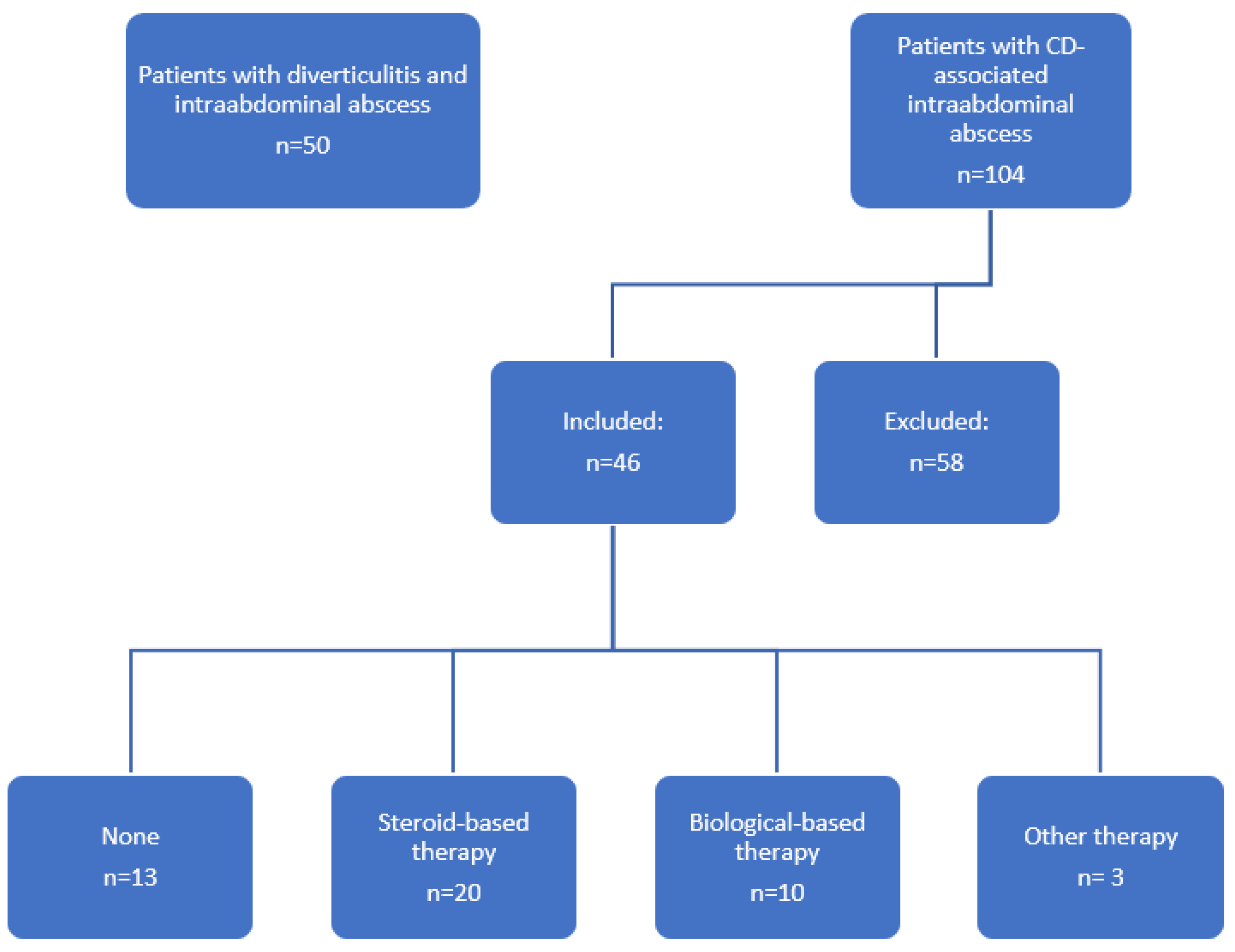
2.1. Study Population
2.2. Microbial Diagnostic
2.3. Subgroup Analysis
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
3.1. Patient Characteristics
3.2. Microbial Outcome
3.3. Microbial Spectrum and Influence of Immunosuppressive Therapy
3.4. Empiric Antibiotic Therapy and Resistance Profile
3.5. Local Epidemiological Data and Antibiotic Resistances
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Baumgart, D.C.; Sandborn, W.J. Crohn’s disease. Lancet 2012, 380, 1590–1605. [Google Scholar] [CrossRef] [Green Version]
- Gecse, K.; Khanna, R.; Stoker, J.; Jenkins, J.T.; Gabe, S.; Hahnloser, D.; D’Haens, G. Fistulizing Crohn’s disease: Diagnosis and management. United Eur. Gastroenterol. J. 2013, 1, 206–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keighley, M.R.; Eastwood, D.; Ambrose, N.S.; Allan, R.N.; Burdon, D.W. Incidence and microbiology of abdominal and pelvic abscess in Crohn’s disease. Gastroenterology 1982, 83, 1271–1275. [Google Scholar] [CrossRef]
- Yamaguchi, A.; Matsui, T.; Sakurai, T.; Ueki, T.; Nakabayashi, S.; Yao, T.; Futami, K.; Arima, S.; Ono, H. The clinical characteristics and outcome of intraabdominal abscess in Crohn’s disease. J. Gastroenterol. 2004, 39, 441–448. [Google Scholar] [CrossRef]
- de Groof, E.J.; Carbonnel, F.; Buskens, C.J.; Bemelman, W.A. Abdominal abscess in Crohn’s disease: Multidisciplinary management. Dig. Dis. 2014, 32 (Suppl. S1), 103–109. [Google Scholar] [CrossRef] [PubMed]
- De Simone, B.; Davies, J.; Chouillard, E.; Di Saverio, S.; Hoentjen, F.; Tarasconi, A.; Sartelli, M.; Biffl, W.L.; Ansaloni, L.; Coccolini, F.; et al. WSES-AAST guidelines: Management of inflammatory bowel disease in the emergency setting. World J. Emerg. Surg. 2021, 16, 23. [Google Scholar] [CrossRef]
- Feagins, L.A.; Holubar, S.D.; Kane, S.V.; Spechler, S.J. Current strategies in the management of intra-abdominal abscesses in Crohn’s disease. Clin. Gastroenterol. Hepatol. 2011, 9, 842–850. [Google Scholar] [CrossRef]
- Thompson, D.T.; Hrabe, J.E. Intra-abdominal and Anorectal Abscesses. Gastroenterol. Clin. N. Am. 2021, 50, 475–488. [Google Scholar] [CrossRef]
- Lichtenstein, G.R.; Loftus, E.V.; Isaacs, K.L.; Regueiro, M.D.; Gerson, L.B.; Sands, B.E. ACG Clinical Guideline: Management of Crohn’s Disease in Adults. Am. J. Gastroenterol. 2018, 113, 481–517. [Google Scholar] [CrossRef]
- Martins, R.; Carmona, C.; George, B.; Epstein, J.; Guideline, C. Management of Crohn’s disease: Summary of updated NICE guidance. BMJ 2019, 367, l5940. [Google Scholar] [CrossRef]
- Bemelman, W.A.; Warusavitarne, J.; Sampietro, G.M.; Serclova, Z.; Zmora, O.; Luglio, G.; de Buck van Overstraeten, A.; Burke, J.P.; Buskens, C.J.; Colombo, F.; et al. ECCO-ESCP Consensus on Surgery for Crohn’s Disease. J. Crohn’s Colitis 2018, 12, 1–16. [Google Scholar] [CrossRef]
- Celentano, V.; Giglio, M.C.; Pellino, G.; Rottoli, M.; Sampietro, G.; Spinelli, A.; Selvaggi, F.; on behalf of the Italian Society of Colorectal Surgery SICCR. High complication rate in Crohn’s disease surgery following percutaneous drainage of intra-abdominal abscess: A multicentre study. Int. J. Colorectal Dis. 2022, 37, 1421–1428. [Google Scholar] [CrossRef] [PubMed]
- Clancy, C.; Boland, T.; Deasy, J.; McNamara, D.; Burke, J.P. A Meta-analysis of Percutaneous Drainage Versus Surgery as the Initial Treatment of Crohn’s Disease-related Intra-abdominal Abscess. J. Crohn’s Colitis 2016, 10, 202–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collard, M.K.; Benoist, S.; Maggiori, L.; Zerbib, P.; Lefevre, J.H.; Denost, Q.; Germain, A.; Cotte, E.; Beyer-Berjot, L.; Corte, H.; et al. A Reappraisal of Outcome of Elective Surgery After Successful Non-Operative Management of an Intra-Abdominal Abscess Complicating Ileocolonic Crohn’s Disease: A Subgroup Analysis of a Nationwide Prospective Cohort. J. Crohn’s Colitis 2021, 15, 409–418. [Google Scholar] [CrossRef] [PubMed]
- Park, S.K.; Kim, K.J.; Lee, S.O.; Yang, D.H.; Jung, K.W.; Duk Ye, B.; Byeon, J.S.; Myung, S.J.; Yang, S.K.; Kim, J.H.; et al. Ciprofloxacin usage and bacterial resistance patterns in Crohn’s disease patients with abscesses. J. Clin. Gastroenterol. 2014, 48, 703–707. [Google Scholar] [CrossRef]
- Reuken, P.A.; Kruis, W.; Maaser, C.; Teich, N.; Buning, J.; Preiss, J.C.; Schmelz, R.; Bruns, T.; Fichtner-Feigl, S.; Stallmach, A.; et al. Microbial Spectrum of Intra-Abdominal Abscesses in Perforating Crohn’s Disease: Results from a Prospective German Registry. J. Crohn’s Colitis 2018, 12, 695–701. [Google Scholar] [CrossRef] [Green Version]
- Satsangi, J.; Silverberg, M.S.; Vermeire, S.; Colombel, J.F. The Montreal classification of inflammatory bowel disease: Controversies, consensus, and implications. Gut 2006, 55, 749–753. [Google Scholar] [CrossRef] [Green Version]
- Miller, J.M.; Binnicker, M.J.; Campbell, S.; Carroll, K.C.; Chapin, K.C.; Gilligan, P.H.; Gonzalez, M.D.; Jerris, R.C.; Kehl, S.C.; Patel, R.; et al. A Guide to Utilization of the Microbiology Laboratory for Diagnosis of Infectious Diseases: 2018 Update by the Infectious Diseases Society of America and the American Society for Microbiology. Clin. Infect. Dis. 2018, 67, e1–e94. [Google Scholar] [CrossRef]
- Nitzan, O.; Elias, M.; Peretz, A.; Saliba, W. Role of antibiotics for treatment of inflammatory bowel disease. World J. Gastroenterol. 2016, 22, 1078–1087. [Google Scholar] [CrossRef]
- Bermejo, F.; Garrido, E.; Chaparro, M.; Gordillo, J.; Manosa, M.; Algaba, A.; Lopez-Sanroman, A.; Gisbert, J.P.; Garcia-Planella, E.; Guerra, I.; et al. Efficacy of different therapeutic options for spontaneous abdominal abscesses in Crohn’s disease: Are antibiotics enough? Inflamm. Bowel Dis. 2012, 18, 1509–1514. [Google Scholar] [CrossRef]
- Gutierrez, A.; Lee, H.; Sands, B.E. Outcome of surgical versus percutaneous drainage of abdominal and pelvic abscesses in Crohn’s disease. Am. J. Gastroenterol. 2006, 101, 2283–2289. [Google Scholar] [CrossRef] [PubMed]
- Garcia, J.C.; Persky, S.E.; Bonis, P.A.; Topazian, M. Abscesses in Crohn’s disease: Outcome of medical versus surgical treatment. J. Clin. Gastroenterol. 2001, 32, 409–412. [Google Scholar] [CrossRef] [PubMed]
- Gervais, D.A.; Hahn, P.F.; O’Neill, M.J.; Mueller, P.R. Percutaneous abscess drainage in Crohn disease: Technical success and short- and long-term outcomes during 14 years. Radiology 2002, 222, 645–651. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Kim, Y.H.; Kim, J.H.; Chang, D.K.; Son, H.J.; Rhee, P.L.; Kim, J.J.; Paik, S.W.; Rhee, J.C. Nonsurgical treatment of abdominal or pelvic abscess in consecutive patients with Crohn’s disease. Dig. Liver Dis. 2006, 38, 659–664. [Google Scholar] [CrossRef]
- Alharbi, O.; Almadi, M.A.; Azzam, N.; Aljebreen, A.M.; AlAmeel, T.; Schreiber, S.; Mosli, M.H. Clinical characteristics, natural history, and outcomes of Crohn’s-related intra-abdominal collections. Saudi J. Gastroenterol. 2021, 27, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Graham, E.; Rao, K.; Cinti, S. Medical Versus Interventional Treatment of Intra-Abdominal Abscess in Patients With Crohn Disease. Infect. Dis. 2017, 10, 1179916117701736. [Google Scholar] [CrossRef] [Green Version]
- Jeong, S.H.; Choi, J.S.; Kim, J.W.; Kim, H.M.; Kim, H.S.; Im, J.P.; Kim, J.S.; Kim, Y.S.; Cheon, J.H.; Kim, W.H.; et al. Clinical Features of Intra-Abdominal Abscess and Intestinal Free-Wall Perforation in Korean Patients with Crohn’s Disease: Results from the CONNECT Study. J. Clin. Med. 2020, 10, 116. [Google Scholar] [CrossRef]
- Nguyen, D.L.; Nguyen, E.T.; Bechtold, M.L. Outcomes of initial medical compared with surgical strategies in the management of intra-abdominal abscesses in patients with Crohn’s disease: A meta-analysis. Eur. J. Gastroenterol. Hepatol. 2015, 27, 235–241. [Google Scholar] [CrossRef]
- Nguyen, D.L.; Sandborn, W.J.; Loftus, E.V., Jr.; Larson, D.W.; Fletcher, J.G.; Becker, B.; Mandrekar, J.; Harmsen, W.S.; Bruining, D.H. Similar outcomes of surgical and medical treatment of intra-abdominal abscesses in patients with Crohn’s disease. Clin Gastroenterol. Hepatol. 2012, 10, 400–404. [Google Scholar] [CrossRef]
- Patil, S.A.; Cross, R.K. Medical versus surgical management of penetrating Crohn’s disease: The current situation and future perspectives. Expert Rev. Gastroenterol. Hepatol. 2017, 11, 843–848. [Google Scholar] [CrossRef]
- Waked, B.; Holvoet, T.; Geldof, J.; Baert, F.; Pattyn, P.; Lobaton, T.; Hindryckx, P. Conservative management of spontaneous intra-abdominal abscess in Crohn’s disease: Outcome and prognostic factors. J. Dig. Dis. 2021, 22, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Versporten, A.; Zarb, P.; Caniaux, I.; Gros, M.F.; Drapier, N.; Miller, M.; Jarlier, V.; Nathwani, D.; Goossens, H.; Global, P.P.S.n. Antimicrobial consumption and resistance in adult hospital inpatients in 53 countries: Results of an internet-based global point prevalence survey. Lancet Glob. Health 2018, 6, e619–e629. [Google Scholar] [CrossRef] [Green Version]
- Cassier, P.; Lallechère, S.; Aho, S.; Astruc, K.; Neuwirth, C.; Piroth, L.; Chavanet, P. Cephalosporin and fluoroquinolone combinations are highly associated with CTX-M β-lactamase-producing Escherichia coli: A case-control study in a French teaching hospital. Clin. Microbiol. Infect. 2011, 17, 1746–1751. [Google Scholar] [CrossRef] [Green Version]
- Sankar, A.; Swanson, K.M.; Zhou, J.; Jena, A.B.; Ross, J.S.; Shah, N.D.; Karaca-Mandic, P. Association of Fluoroquinolone Prescribing Rates With Black Box Warnings from the US Food and Drug Administration. JAMA Netw. Open 2021, 4, e2136662. [Google Scholar] [CrossRef] [PubMed]
- Ledder, O.; Turner, D. Antibiotics in IBD: Still a Role in the Biological Era? Inflamm. Bowel Dis. 2018, 24, 1676–1688. [Google Scholar] [CrossRef]
- Li, G.; Ren, J.; Wu, Q.; Hu, D.; Wang, G.; Wu, X.; Liu, S.; Wu, Y.; Gu, G.; Li, J. Bacteriology of Spontaneous Intra-Abdominal Abscess in Patients with Crohn Disease in China: Risk of Extended-Spectrum Beta-Lactamase-Producing Bacteria. Surg. Infect. 2015, 16, 461–465. [Google Scholar] [CrossRef] [PubMed]
- Labricciosa, F.M.; Sartelli, M.; Abbo, L.M.; Barbadoro, P.; Ansaloni, L.; Coccolini, F.; Catena, F. Epidemiology and Risk Factors for Isolation of Multi-Drug-Resistant Organisms in Patients with Complicated Intra-Abdominal Infections. Surg. Infect. 2018, 19, 264–272. [Google Scholar] [CrossRef]
- Reuken, P.A.; Torres, D.; Baier, M.; Loffler, B.; Lubbert, C.; Lippmann, N.; Stallmach, A.; Bruns, T. Risk Factors for Multi-Drug Resistant Pathogens and Failure of Empiric First-Line Therapy in Acute Cholangitis. PLoS ONE 2017, 12, e0169900. [Google Scholar] [CrossRef] [Green Version]
- Andreassen, A.E.S.; Jacobsen, C.M.; de Blasio, B.; White, R.; Kristiansen, I.S.; Elstrom, P. The impact of methicillin-resistant S. aureus on length of stay, readmissions and costs: A register based case-control study of patients hospitalized in Norway. Antimicrob. Resist. Infect. Control 2017, 6, 74. [Google Scholar] [CrossRef] [Green Version]
- Zilberberg, M.D.; Nathanson, B.H.; Sulham, K.; Fan, W.; Shorr, A.F. Carbapenem resistance, inappropriate empiric treatment and outcomes among patients hospitalized with Enterobacteriaceae urinary tract infection, pneumonia and sepsis. BMC Infect. Dis. 2017, 17, 279. [Google Scholar] [CrossRef]
- de Kraker, M.E.; Wolkewitz, M.; Davey, P.G.; Koller, W.; Berger, J.; Nagler, J.; Icket, C.; Kalenic, S.; Horvatic, J.; Seifert, H.; et al. Burden of antimicrobial resistance in European hospitals: Excess mortality and length of hospital stay associated with bloodstream infections due to Escherichia coli resistant to third-generation cephalosporins. J. Antimicrob. Chemother. 2011, 66, 398–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Kraker, M.E.; Davey, P.G.; Grundmann, H.; BURDEN Study Group. Mortality and hospital stay associated with resistant Staphylococcus aureus and Escherichia coli bacteremia: Estimating the burden of antibiotic resistance in Europe. PLoS Med. 2011, 8, e1001104. [Google Scholar] [CrossRef] [Green Version]
- van Hecke, O.; Wang, K.; Lee, J.J.; Roberts, N.W.; Butler, C.C. Implications of Antibiotic Resistance for Patients’ Recovery From Common Infections in the Community: A Systematic Review and Meta-analysis. Clin. Infect. Dis. 2017, 65, 371–382. [Google Scholar] [CrossRef] [PubMed]
- Surat, G.; Meyer-Sautter, P.; Rusch, J.; Braun-Feldweg, J.; Germer, C.T.; Lock, J.F. Comparison of Duration and Empiric Antibiotic Choice of Post-Operative Treatment in Abdominal Sepsis. Surg. Infect. 2022, 23, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Surat, G.; Meyer-Sautter, P.; Rusch, J.; Braun-Feldweg, J.; Markus, C.K.; Germer, C.T.; Lock, J.F. Cefazolin Might Be Adequate for Perioperative Antibiotic Prophylaxis in Intra-Abdominal Infections without Sepsis: A Quality Improvement Study. Antibiotics 2022, 11, 501. [Google Scholar] [CrossRef]
- Forster, J.; Schulze, P.; Burger, C.; Krone, M.; Vogel, U.; Surat, G. Combined Training Intervention Targeting Medical and Nursing Staff Reduces Ciprofloxacin Use and Events of Urinary Tract Infection. Adv. Urol. 2022, 2022, 2474242. [Google Scholar] [CrossRef]
- Surat, G.; Vogel, U.; Wiegering, A.; Germer, C.T.; Lock, J.F. Defining the Scope of Antimicrobial Stewardship Interventions on the Prescription Quality of Antibiotics for Surgical Intra-Abdominal Infections. Antibiotics 2021, 10, 73. [Google Scholar] [CrossRef]
- Steinbach, C.L.; Topper, C.; Adam, T.; Kees, M.G. Spectrum adequacy of antibiotic regimens for secondary peritonitis: A retrospective analysis in intermediate and intensive care unit patients. Ann. Clin. Microbiol. Antimicrob. 2015, 14, 48. [Google Scholar] [CrossRef] [Green Version]
- Swenson, B.R.; Metzger, R.; Hedrick, T.L.; McElearney, S.T.; Evans, H.L.; Smith, R.L.; Chong, T.W.; Popovsky, K.A.; Pruett, T.L.; Sawyer, R.G. Choosing antibiotics for intra-abdominal infections: What do we mean by “high risk”? Surg. Infect. 2009, 10, 29–39. [Google Scholar] [CrossRef]
- Montravers, P.; Dupont, H.; Gauzit, R.; Veber, B.; Auboyer, C.; Blin, P.; Hennequin, C.; Martin, C. Candida as a risk factor for mortality in peritonitis. Crit. Care Med. 2006, 34, 646–652. [Google Scholar] [CrossRef]
- Kollef, M.; Micek, S.; Hampton, N.; Doherty, J.A.; Kumar, A. Septic shock attributed to Candida infection: Importance of empiric therapy and source control. Clin. Infect. Dis. 2012, 54, 1739–1746. [Google Scholar] [CrossRef] [PubMed]
- Garey, K.W.; Rege, M.; Pai, M.P.; Mingo, D.E.; Suda, K.J.; Turpin, R.S.; Bearden, D.T. Time to initiation of fluconazole therapy impacts mortality in patients with candidemia: A multi-institutional study. Clin. Infect. Dis. 2006, 43, 25–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Variable | Control (n = 50) | Crohn’s Disease (n = 46) | p |
|---|---|---|---|
| Age (year) | |||
| Median | 64.9 | 40.4 | <0.001 |
| (range) | (19.7–88.6) | (16.6–66.9) | |
| Sex (n,%) | |||
| Female | 25 (50.0) | 15 (32.6) | |
| Male | 25 (50.0) | 31 (67.4) | 0.100 |
| BMI (kg/m2) | |||
| Median | 28.0 | 23.6 | <0.001 |
| (range) | (17.5–47.1) | (13.6–37.0) | |
| CVRF (n,%) | 33 (66.0) | 22 (47.8) | 0.099 |
| COPD (n,%) | 8 (16.0) | 3 (6.5) | 0.203 |
| Diabetes (n,%) | 1 (2.0) | 3 (6.5) | 0.347 |
| Smoking | |||
| active (n,%) | 7 (14.0) | 10 (21.7) | |
| former (n,%) | 2 (4.0) | 1 (2.2) | 0.557 |
| ASA classification (n,%) | |||
| 1 | 1 (2.0) | 2 (4.3) | |
| 2 | 25 (50.0) | 28 (60.9) | |
| 3 | 22 (44.0) | 14 (30.4) | |
| 4 | 2 (4.0) | 2 (4.3) | 0.548 |
| Hb (g/dL) | |||
| median (range) | 12.9 (5.3–17.6) | 11.9 (6.6–19.8) | 0.530 |
| Albumin (g/L) | |||
| median (range) | 4.0 (2.2–5.0) | 3.7 (2.4–5.1) | 0.722 |
| Leukocytes (×1000/µL) | |||
| median (range) | 13.5 (4.5–30.2) | 12.8 (4.4–43.1) | 0.375 |
| CRP (mg/dL) | |||
| median (range) | 10.3 (0.1–38.2) | 6.0 (0.2–34.8) | 0.033 |
| Pathogen | Control (n = 50) | Crohn’s Disease (n = 46) | p |
|---|---|---|---|
| Negative (n,%) | 2 (4.0) | 10 (21.7) | 0.012 |
| Skin germs (n,%) | 0 (0) | 2 (4.3) | 0.227 |
| Viridans group streptococci (n,%) | 14 (28.0) | 15 (32.6) | 0.661 |
| Streptococcus groups A, B, C and G (n,%) | 2 (4.0) | 1 (2.2) | 1.000 |
| Staphylococcus spp. (n,%) | 4 (4.0) | 2 (4.3) | 1.000 |
| Anaerobic bacteria (n,%) | 31 (62.0) | 9 (19.6) | 0.001 |
| Enterobacterales (n,%) | 37 (74.0) | 20 (43.5) | 0.003 |
| Enterococcus spp. (n,%) | 15 (30.0) | 7 (15.2) | 0.096 |
| Non relevant (n,%) | 2 (4.0) | 4 (8.7) | 0.422 |
| Fungi (n,%) | 9 (18.0) | 10 (21.7) | 0.798 |
| Pathogen | No Immunosuppressive Therapy (n = 13) | Steroid-Based Immunosuppressive Therapy (n = 20) | Antibody-Based Immunosuppressive Therapy (n = 10) | p |
|---|---|---|---|---|
| Negative (n,%) | 1 (7.7) | 7 (35.0) | 2 (20.0) | 0.186 |
| Skin germs (n,%) | 2 (15.4) | 0 (0) | 0 (0) | 0.089 |
| Viridans group streptococci (n,%) | 5 (38.5) | 7 (35.0) | 3 (30.0) | 0.915 |
| Streptococcus groups A, B, C and G (n,%) | 1 (7.7) | 0 (0) | 0 (0) | 0.307 |
| Staphylococcus spp. (n,%) | 1 (7.7) | 1 (5.0) | 0 (0) | 0.682 |
| Anaerobic bacteria (n,%) | 2 (15.4) | 5 (25.0) | 1 (10.0) | 0.572 |
| Enterobacterales (n,%) | 7 (53.8) | 5 (25.0) | 6 (60.0) | 0.108 |
| Enterococcus spp. (n,%) | 2 (15.4) | 1 (5.0) | 2 (20.0) | 0.424 |
| Non relevant (n,%) | 0 (0) | 2 (10.0) | 0 (0.) | 0.299 |
| Fungi (n,%) | 2 (15.4) | 6 (30.0) | 1 (10.0) | 0.376 |
| Antibiotic Regime | Number (n) | Sensible | Intermediary | Resistant | No Therapy |
|---|---|---|---|---|---|
| Overall | 14 | 11 | 2 | 1 | 1 |
| CIP/MET | 5 | 5 | |||
| CEFT/MET | 3 | 3 | |||
| CEFU/MET | 2 | 1 | 1 | ||
| CEFA/MET | 1 | 1 | |||
| MERO | 1 | 1 | |||
| MET | 1 | 1 | |||
| PIP/TAZ | 1 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kusan, S.; Surat, G.; Kelm, M.; Anger, F.; Kim, M.; Germer, C.-T.; Schlegel, N.; Flemming, S. Microbial Spectrum and Antibiotic Resistance in Patients Suffering from Penetrating Crohn’s Disease. J. Clin. Med. 2022, 11, 4343. https://doi.org/10.3390/jcm11154343
Kusan S, Surat G, Kelm M, Anger F, Kim M, Germer C-T, Schlegel N, Flemming S. Microbial Spectrum and Antibiotic Resistance in Patients Suffering from Penetrating Crohn’s Disease. Journal of Clinical Medicine. 2022; 11(15):4343. https://doi.org/10.3390/jcm11154343
Chicago/Turabian StyleKusan, Simon, Güzin Surat, Matthias Kelm, Friedrich Anger, Mia Kim, Christoph-Thomas Germer, Nicolas Schlegel, and Sven Flemming. 2022. "Microbial Spectrum and Antibiotic Resistance in Patients Suffering from Penetrating Crohn’s Disease" Journal of Clinical Medicine 11, no. 15: 4343. https://doi.org/10.3390/jcm11154343
APA StyleKusan, S., Surat, G., Kelm, M., Anger, F., Kim, M., Germer, C.-T., Schlegel, N., & Flemming, S. (2022). Microbial Spectrum and Antibiotic Resistance in Patients Suffering from Penetrating Crohn’s Disease. Journal of Clinical Medicine, 11(15), 4343. https://doi.org/10.3390/jcm11154343