
Caries Decline in Preschool Children from Low Social Classes and with Migration Background in Hamburg, Germany: Outcome from Repeated Cross-Sectional Caries Epidemiological Studies


Abstract
:1. Introduction
2. Methods
3. Results
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Splieth, C.H.; Santamaria, R.M.; Basner, R.; Schüler, E.; Schmoeckel, J. 40-Year Longitudinal Caries Development in German Adolescents in the Light of New Caries Measures. Caries Res. 2019, 53, 609–616. [Google Scholar] [CrossRef] [PubMed]
- Schiffner, U. Prevalence of disease and care in children (12 years): Dental caries, erosions and molar-incisor-hypomineralisations. In Fifth German Oral Health Study; Jordan, A.R., Micheelis, W., Eds.; Deutscher Ärzteverlag: Cologne, Germany, 2016; Volume 35, pp. 231–268. [Google Scholar]
- Team DAJ. Epidemiologische Begleituntersuchungen zur Gruppenprophylaxe. 2016. Available online: https://www.daj.de/studien.29.0.html (accessed on 6 April 2022).
- Lagerweij, M.D.; van Loveren, C. Declining Caries Trends: Are We Satisfied? Curr. Oral Health Rep. 2015, 2, 212–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwendicke, F.; Dorfer, C.E.; Schlattmann, P.; Foster Page, L.; Thomson, W.M.; Paris, S. Socioeconomic inequality and caries: A systematic review and meta-analysis. J. Dent. Res. 2015, 94, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Cvikl, B.; Haubenberger-Praml, G.; Drabo, P.; Hagmann, M.; Gruber, R.; Moritz, A.; Nell, A. Migration background is associated with caries in Viennese school children, even if parents have received a higher education. BMC Oral. Health 2014, 14, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Julihn, A.; Ekbom, A.; Modéer, T. Migration background: A risk factor for caries development during adolescence. Eur. J. Oral. Sci. 2010, 118, 618–625. [Google Scholar] [CrossRef] [PubMed]
- Gülzow, H.J.; Gerritzen, T.H.; Ritter, H.J. Milchzahnkaries bei Großstadtkindern. Dtsch Zahnärztl 1980, 35, 297–300. [Google Scholar]
- Schiffner, U.; Gülzow, H.J. Kariesfrequenz und Kariesbefall Hamburger Kindergarten- und Tageskinder im Jahre 1987. Dtsch Zahnärztl 1988, 43, 1166–1171. [Google Scholar]
- Gülzow, H.J.; Burghardt, P.; Schiffner, U. Karies bei Hamburger Kindergartenkindern 1977–1993. Dtsch Zahnärztl 1996, 51, 354–365. [Google Scholar]
- Sabel, C. Karies bei Hamburger Kindern im Alter von 3 bis 6 Jahren im Jahr 2006 Med. Diss. Ph.D. Thesis, Staats-und Universitätsbibliothek Hamburg Carl von Ossietzky, Hamburg, Germany, 2012. [Google Scholar]
- Schulz, B.; Wolter, I.; Schiffner, U. Caries prevalence and caries experience among 3- to 6-year-old children in Hamburg, Germany. Oralprophylaxe Kinderzahnheilkunde 2022, 44, 34–39. [Google Scholar] [CrossRef]
- World Health Organization. Oral Health Surveys: Basic Methods, 5th ed.; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Marthaler, T.M. A standardized system of recording dental conditions. Helv. Odontol. Acta 1966, 10, 1–18. [Google Scholar] [PubMed]
- Bundesamt, S. Pressekonferenz “Leben in Deutschland—Ergebnisse des Mikrozensus 2005”. Available online: https://web.archive.org/web/20060630171741/http://www.destatis.de/presse/deutsch/pk/2006/Mikrozensus2005_Statement_Hahlen.pdf (accessed on 10 May 2022).
- Garbin, C.A.S.; Saliba, T.A.; Teruel, G.P.; Moimaz, S.A.S.; Garbin, A. Caries Experience in Preschool Children over a 10-year Period. Oral Health Prev. Dent. 2019, 17, 263–266. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, J.C.; D’Hoore, W.; Van Nieuwenhuysen, J.P. Caries decline in the primary dentition of Belgian children over 15 years. Community Dent. Oral Epidemiol. 2004, 32, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Koch, G.; Helkimo, A.N.; Ullbro, C. Caries prevalence and distribution in individuals aged 3–20 years in Jönköping, Sweden: Trends over 40 years. Eur. Arch. Paediatr. Dent. 2017, 18, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Sozialgesetzbuch (SGB V). 21 SGB V Verhütung von Zahnerkrankungen (Gruppenprophylaxe). Available online: https://www.sozialgesetzbuch-sgb.de/sgbv/21.html (accessed on 2 May 2022).
- Splieth, C.H.; Heyduck, C.; König, K.G. Gruppenprophylaxe nach dem Caries Decline. Oralprophylaxe & Kinderzahnheilkunde 2006, 28, 60–64. [Google Scholar]
- Robert-Koch-Institut. Gesundheit in Deutschland 2015—Interventionsebenen. Available online: https://www.gbe-bund.de/gbe/ergebnisse.prc_tab?fid=25658&suchstring=4.4.1&query_id=&sprache=D&fund_typ=TXT&methode=2&vt=1&verwandte=1&page_ret=0&seite=&p_lfd_nr=1&p_news=&p_sprachkz=D&p_uid=gast&p_aid=25137239&hlp_nr=3&p_janein=J (accessed on 2 May 2022).
- Gemeinsamer Bundesausschuss. Richtlinie über die Früherkennungsuntersuchungen auf Zahn-, Mund- und Kieferkrankheiten (in der Version mit Inkrafttreten vom 01.01.2004). Available online: https://www.g-ba.de/richtlinien/historie/45/ (accessed on 1 May 2022).
- Gemeinsamer Bundesausschuss. Richtlinie des Gemeinsamen Bundesausschusses über die Früherkennungsuntersuchungen auf Zahn-, Mund- und Kieferkrankheiten (Zahnärztliche Früherkennung gemäß § 26 Absatz 1 Satz 5 und Absatz 2 Satz 5 SGB V) (FU-RL). Available online: https://www.g-ba.de/richtlinien/29/ (accessed on 10 May 2022).

{kind=link}
{kind=link}
| 1977 | 1987 | 1993 | 2006 | 2016 | |
|---|---|---|---|---|---|
| n = 1508 | n = 1927 | n = 1956 | n = 1643 | n = 933 | |
| Prevalence (%) | |||||
| WHO criteria | 58.4 | 48.0 | 41.5 | 27.3 | 22.7 |
| Including IC | 91.0 | 74.4 | 52.4 | 50.8 | 44.4 |
| dmft | |||||
| WHO criteria | 2.6 | 2.5 | 2.1 | 1.1 | 0.8 |
| Including IC | 6.4 | 4.6 | 2.6 | 2.3 | 1.8 |
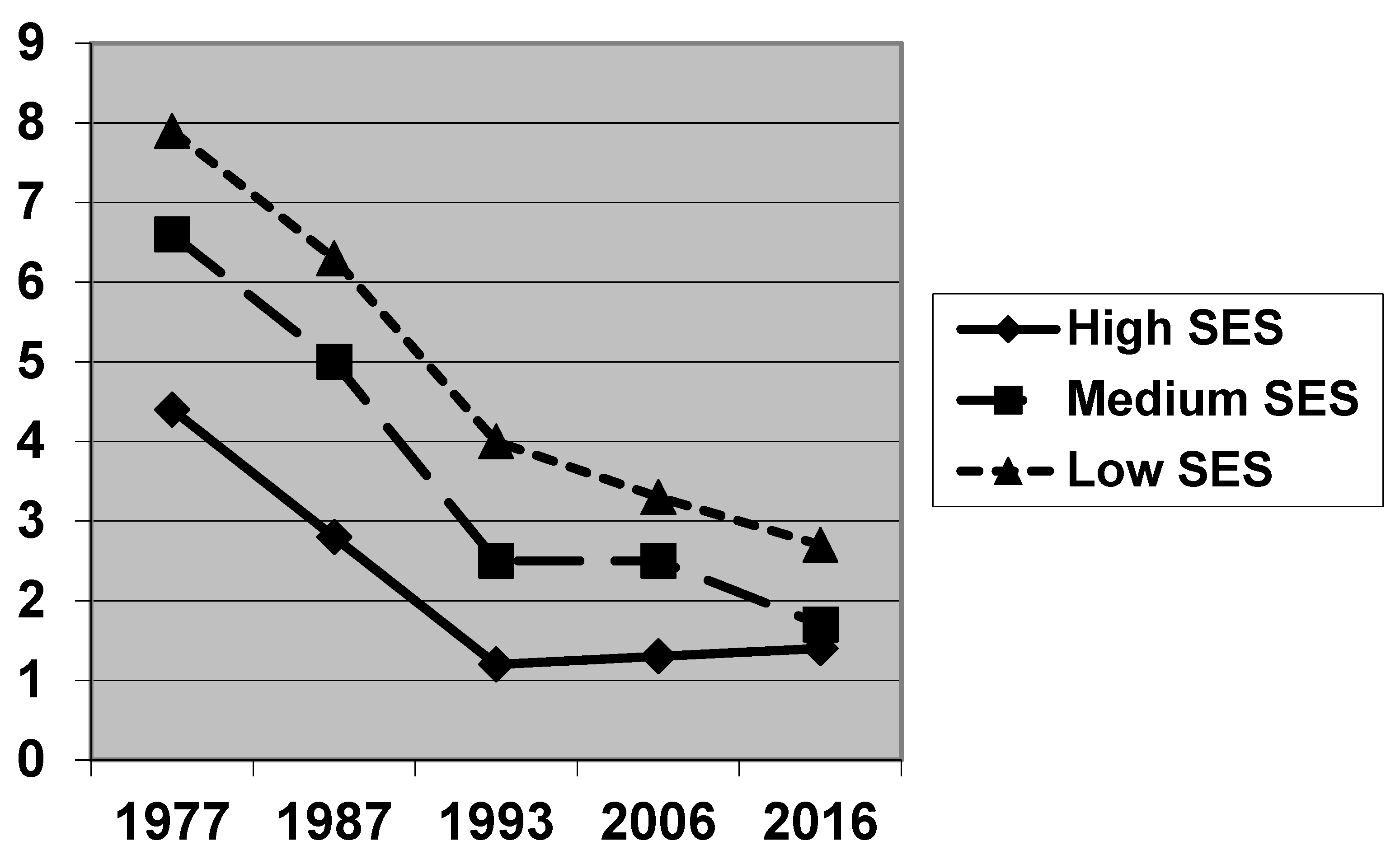
| 1977 | 1987 | 1993 | 2006 | 2016 | |
|---|---|---|---|---|---|
| Prevalence (WHO criteria) | |||||
| High SES | 45.7 | 28.7 | 21.1 | 19.3 | 14.7 |
| Middle SES | 60.9 | 51.8 | 41.5 | 28.2 | 26.2 |
| Low SES | 64.9 | 65.8 | 57.9 | 36.9 | 42.6 |
| p (Chi2-test) | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Prevalence (incl. IC) | |||||
| High SES | 82.4 | 59.4 | 33.6 | 39.4 | 40.9 |
| Middle SES | 92.2 | 77.2 | 50.5 | 52.7 | 42.4 |
| Low SES | 96.4 | 88.2 | 71.3 | 63.6 | 51.9 |
| p (Chi2-test) | <0.001 | <0.001 | <0.001 | <0.001 | 0.114 |
| dmft (WHO criteria) | |||||
| High SES | 1.6 | 1.2 | 0.7 | 0.6 | 0.4 |
| Middle SES | 2.8 | 2.7 | 2.0 | 1.2 | 0.8 |
| Low SES | 3.3 | 3.5 | 3.2 | 1.8 | 1.9 |
| p (KW-test) | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| dmft (incl. IC) | |||||
| High SES | 4.4 | 2.8 | 1.2 | 1.3 | 1.4 |
| Middle SES | 6.6 | 5.0 | 2.5 | 2.5 | 1.7 |
| Low SES | 7.9 | 6.3 | 4.0 | 3.3 | 2.7 |
| p (KW-test) | <0.001 | <0.001 | <0.001 | <0.001 | <0.011 |
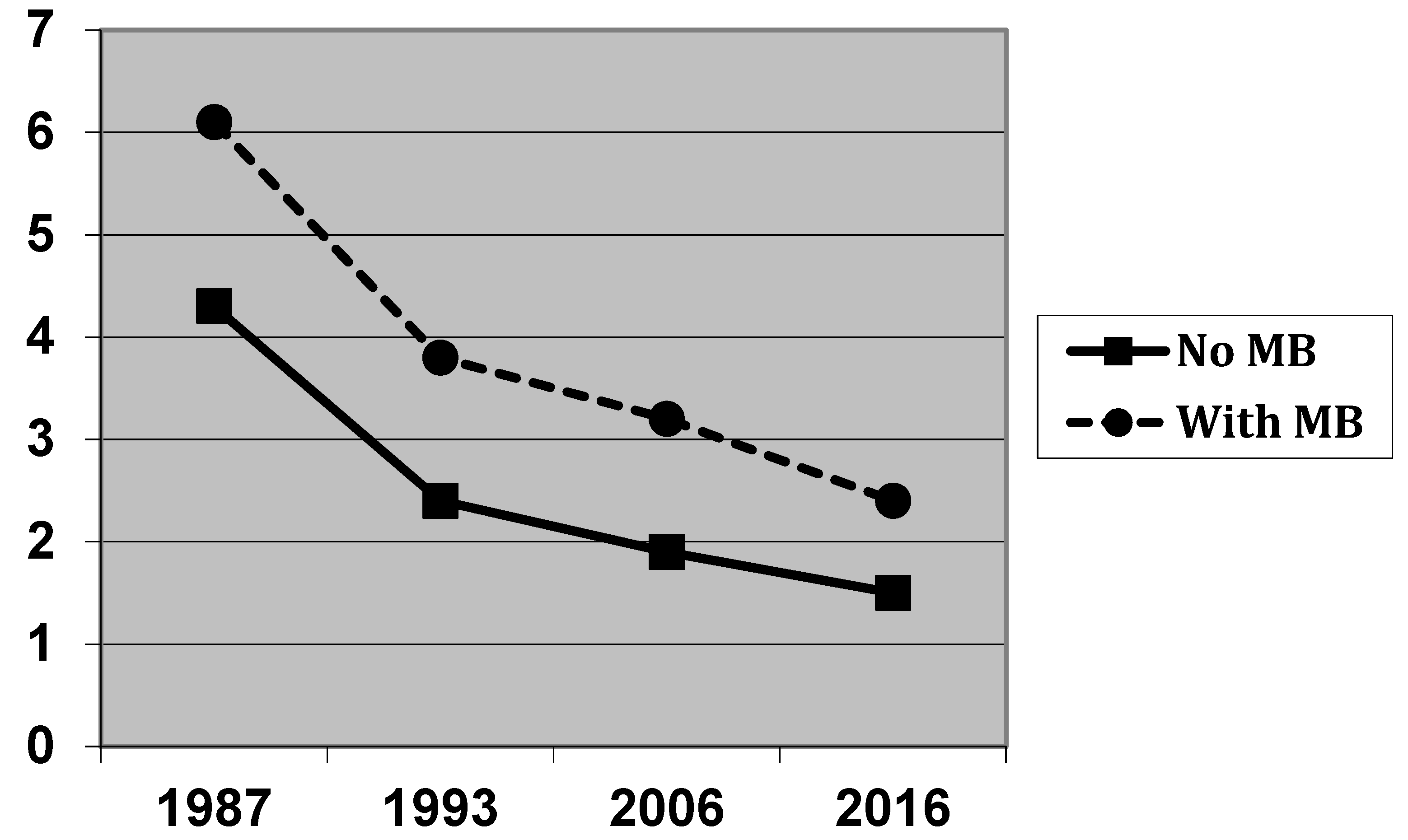
| 1987 | 1993 | 2006 | 2016 | |
|---|---|---|---|---|
| Prevalence (WHO criteria) | ||||
| No MB | 45.2 | 37.9 | 22.0 | 17.8 |
| With MB | 61.9 | 55.8 | 38.7 | 35.5 |
| p (Chi2-test) | <0.001 | <0.001 | <0.001 | <0.001 |
| Prevalence (incl. IC) | ||||
| No MB | 72.0 | 48.7 | 44.9 | 40.5 |
| With MB | 85.5 | 67.3 | 62.3 | 53.5 |
| p (Chi2-test) | <0.001 | <0.001 | <0.001 | 0.003 |
| dmft (WHO criteria) | ||||
| No MB | 2.3 | 1.8 | 0.9 | 0.5 |
| With MB | 3.4 | 2.9 | 1.7 | 1.3 |
| p (MW-test) | <0.001 | <0.001 | <0.001 | <0.001 |
| dmft (incl. IC) | ||||
| No MB | 4.3 | 2.4 | 1.9 | 1.5 |
| With MB | 6.1 | 3.8 | 3.2 | 2.4 |
| p (MW-test) | <0.001 | <0.001 | <0.001 | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schiffner, U. Caries Decline in Preschool Children from Low Social Classes and with Migration Background in Hamburg, Germany: Outcome from Repeated Cross-Sectional Caries Epidemiological Studies. J. Clin. Med. 2022, 11, 4251. https://doi.org/10.3390/jcm11154251
Schiffner U. Caries Decline in Preschool Children from Low Social Classes and with Migration Background in Hamburg, Germany: Outcome from Repeated Cross-Sectional Caries Epidemiological Studies. Journal of Clinical Medicine. 2022; 11(15):4251. https://doi.org/10.3390/jcm11154251
Chicago/Turabian StyleSchiffner, Ulrich. 2022. "Caries Decline in Preschool Children from Low Social Classes and with Migration Background in Hamburg, Germany: Outcome from Repeated Cross-Sectional Caries Epidemiological Studies" Journal of Clinical Medicine 11, no. 15: 4251. https://doi.org/10.3390/jcm11154251
APA StyleSchiffner, U. (2022). Caries Decline in Preschool Children from Low Social Classes and with Migration Background in Hamburg, Germany: Outcome from Repeated Cross-Sectional Caries Epidemiological Studies. Journal of Clinical Medicine, 11(15), 4251. https://doi.org/10.3390/jcm11154251