
High Definition Three-Dimensional Exoscope (VITOM 3D) in E.N.T. Surgery: A Systematic Review of Current Experience

 ,
, 

 , , ,
, , ,  ,
, 
 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol Data Extraction and Outcomes
2.2. Electronic Database Search
2.3. Eligibility Criteria
- Original articles;
- The article was published in English;
- The studies included clinically confirmed E.N.T. disorders treated with 4k exoscope-assisted surgery;
- The studies reported detailed information on 4k exoscope-assisted surgery as high-definition images of the surgical field, improved vision and depth perception, different treatment modalities, and patient’s comorbidities.
- 5.
- Editorials, letters to the editor, or reviews;
- 6.
- Studies that included animal samples.
2.4. Synthesis of Results
2.5. Statistical Analysis
3. Results
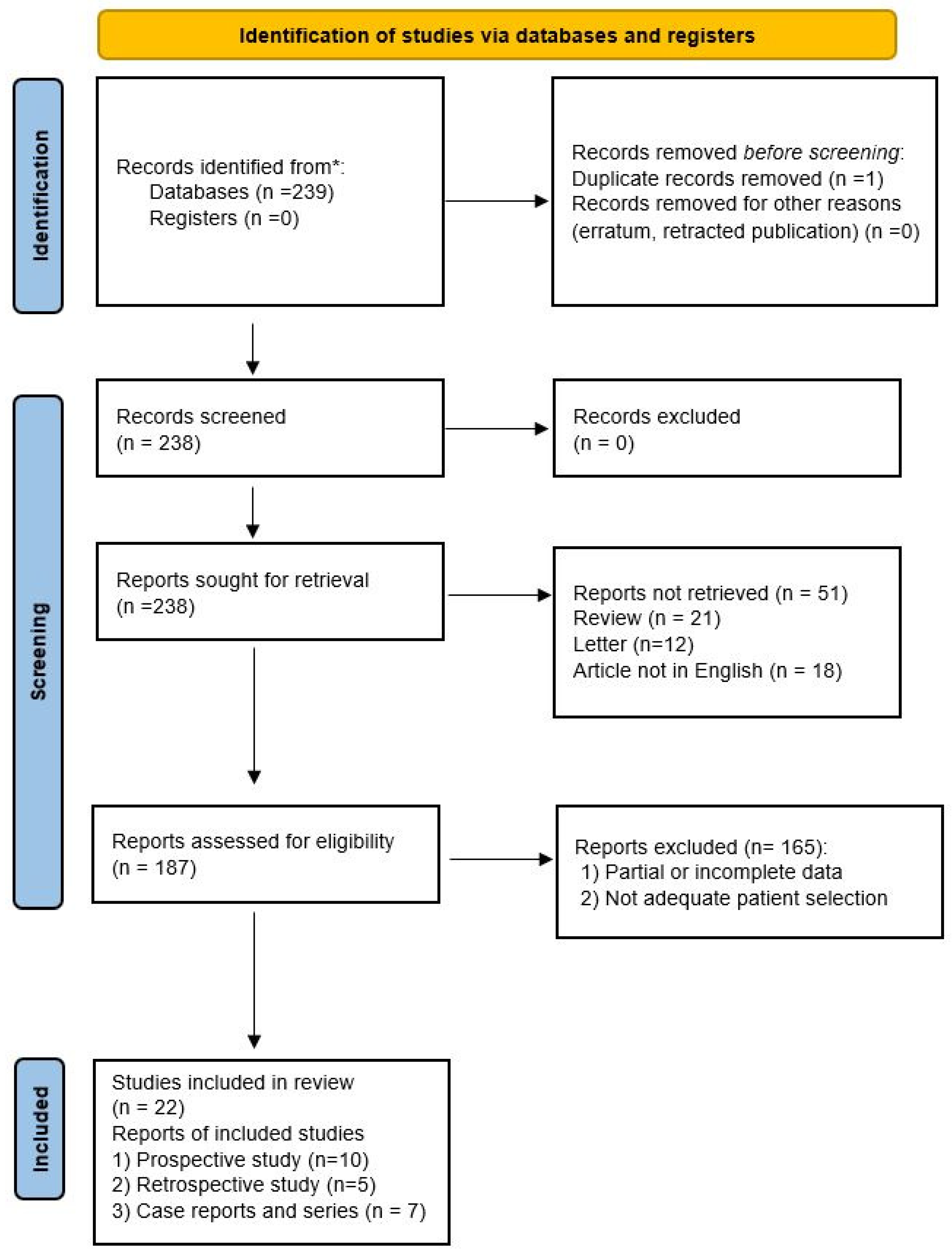
3.1. Paper Retrieval
3.2. Study Features
3.3. Patients’ Features, Comorbidities, and Treatment
3.4. Surgical Times and Cost Effectiveness in Comparision of Techniques
3.5. Lateral Skull Base and Ear Surgery
3.6. Nasal and Paranasal Surgery
3.7. Exoscope Application in Head and Neck Surgery
3.7.1. Oral Surgery
3.7.2. Laryngeal Surgery
3.7.3. Parotid Gland Surgery
3.7.4. Submandibular Gland Surgery
3.8. Reconstructive Approaches
3.9. Study Limitations
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Colombo, G.; Ferreli, F.; Di Bari, M.; Cugini, G.; Miceli, S.; De Virgilio, A.; Spriano, G.; Poletti, A. Introducing the High-definition 3D exoscope in ear surgery: Preliminary analysis of advantages and limits compared with operative microscope. Eur. Arch. Otorhinolaryngol. 2021, 278, 4217–4223. [Google Scholar] [CrossRef] [PubMed]
- De Virgilio, A.; Costantino, A.; Ms, T.M.; Conti, V.; Pirola, F.; Russo, E.; Mercante, G.; Spriano, G. Pre-Clinical Experience with the VITOM 3D and the ARTip Cruise System for Micro-Laryngeal Surgery. Laryngoscope 2021, 131, 136–138. [Google Scholar] [CrossRef] [PubMed]
- Ridge, S.E.; Shetty, K.R.; Lee, D.J. Heads-up Surgery: Endoscopes and Exoscopes for Otology and Neurotology in the Era of the COVID-19 Pandemic. Otolaryngol. Clin. N. Am. 2021, 54, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Bartkowiak, E.; Łuczewski, Ł.; Chou, J.T.-T.; Wierzbicka, M. Is the 3D exoscope better than the surgical microscope in parotid surgery: A prospective, randomized single-center study. Eur. Arch. Otorhinolaryngol. 2022, 279, 1029–1034. [Google Scholar] [CrossRef] [PubMed]
- Crosetti, E.; Arrigoni, G.; Manca, A.; Caracciolo, A.; Bertotto, I.; Succo, G. 3D Exoscopic Surgery (3Des) for Transoral Oropharyngectomy. Front. Oncol. 2020, 10, 16. [Google Scholar] [CrossRef]
- Boscolo-Rizzo, P.; Zanelli, E.; Giudici, F.; Boscolo-Nata, F.; Cristalli, G.; Deganello, A.; Tomasoni, M.; Piazza, C.; Bossi, P.; Spinato, G.; et al. Prognostic value of H-index in patients surgically treated for squamous cell carcinoma of the larynx. Laryngoscope Investig. Otolaryngol. 2021, 6, 729–737. [Google Scholar] [CrossRef]
- Saraniti, C.; Speciale, R.; Gallina, S.; Salvago, P. Prognostic role of resection margin in open oncologic laryngeal surgery: Survival analysis of a cohort of 139 patients affected by squamous cell carcinoma. Braz. J. Otorhinolaryngol. 2019, 85, 603–610. [Google Scholar] [CrossRef]
- Juul, M.L.; Wagner, N. Objective and subjective outcome in 42 patients after treatment of sialolithiasis by transoral incision of Warthon’s duct: A retrospective middle-term follow-up study. Eur. Arch. Otorhinolaryngol. 2014, 271, 3059–3066. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (prisma-p) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [Green Version]
- Campbell, M.; McKenzie, J.E.; Sowden, A.; Katikireddi, S.V.; Brennan, S.E.; Ellis, S.; Hartmann-Boyce, J.; Ryan, R.; Shepperd, S.; Thomas, J.; et al. Synthesis without meta-analysis (SWiM) in systematic reviews: Reporting guideline. BMJ 2020, 368, l6890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M.; the QUADAS-2 Group. QUADAS-2: A revisedtool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Munn, Z.; Moola, S.; Lisy, K.; Riitano, D.; Tufanaru, C. Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data. Int. J. Evid. Based Healthc. 2015, 13, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Wierzbicka, M.; Szyfter, W.; Greczka, G.; Gawęcki, W. Otosurgery with the High-Definition Three-Dimensional (3D) Exoscope: Advantages and Disadvantages. J. Clin. Med. 2021, 10, 777. [Google Scholar] [CrossRef] [PubMed]
- Minoda, R.; Miwa, T. Non-microscopic Middle Ear Cholesteatoma Surgery: A Case Report of a Novel Head-Up Approach. Otol. Neurotol. 2019, 40, 777–781. [Google Scholar] [CrossRef]
- Ally, M.; Kullar, P.; Mochloulis, G.; Vijendren, A. Using a 4K three-dimensional exoscope system (Vitom 3D) for mastoid surgery during the coronavirus disease 2019 pandemic. J. Laryngol. Otol. 2021, 135, 273–275. [Google Scholar] [CrossRef]
- Smith, S.; Kozin, E.D.; Kanumuri, V.V.; Barber, S.R.; Backous, D.; Nogueira, J.F.; Lee, D.J. Initial Experience with 3-Dimensional Exoscope-Assisted Transmastoid and Lateral Skull Base Surgery. Otolaryngol. Neck Surg. 2019, 160, 364–367. [Google Scholar] [CrossRef]
- Rubini, A.; Di Gioia, S.; Marchioni, D. 3D exoscopic surgery of lateral skull base. Eur. Arch. Otorhinolaryngol. 2020, 277, 687–694. [Google Scholar] [CrossRef]
- Iwami, K.; Watanabe, T.; Osuka, K.; Ogawa, T.; Miyachi, S.; Fujimoto, Y. Combined Exoscopic and Endoscopic Technique for Craniofacial Resection. Curr. Oncol. 2021, 28, 3945–3958. [Google Scholar] [CrossRef]
- Tasca, I.; Compadretti, G.C.; Romano, C. High-definition video telescopic rhinoplasty. Video rinoplastica ad alta definizione. Acta Otorhinolaryngol. Ital. 2016, 36, 496–498. [Google Scholar] [CrossRef]
- Pirola, F.; De Virgilio, A.; Di Maria, A.; Russo, E.; Di Bari, M.; Costantino, A.; Ferreli, F.; Mercante, G.; Colombo, G.; Spriano, G.; et al. Applying the Exoscope to Lacrimal Surgery: Preliminary Experience. ORL J. Otorhinolaryngol. Relat. Spec. 2021, 83, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Bignami, M.; Arosio, A.D.; Dalfino, G.; Sileo, G.; Czaczkes, C.; Valenzise, V.; Zannella, S.; Demelas, L.; Castelnuovo, P.; Volpi, L. First Experience of ARTip Cruise VITOM-assisted OPF Removal of Frontal Fibro-osseous Lesion: Operative Video. Laryngoscope 2021, 131, 2219–2223. [Google Scholar] [CrossRef] [PubMed]
- Carlucci, C.; Fasanella, L.; Maccarini, A.R. Exolaryngoscopy: A new technique for laryngeal surgery. Acta Otorhinolaryngol. Ital. 2012, 32, 326–328. [Google Scholar] [PubMed]
- Cantarella, G.; Pignataro, L. A High-Definition 3-Dimensional Exoscope with the ARTip Cruise System as an Effective New Tool for Phonosurgery: A Preliminary Report. J. Voice 2021. [Google Scholar] [CrossRef] [PubMed]
- Carobbio, A.L.C.; Missale, F.; Fragale, M.; Mora, F.; Guastini, L.; Parrinello, G.; Canevari, F.R.M.; Peretti, G.; Mattos, L.S. Transoral laser microsurgery: Feasibility of a new exoscopic HD-3D system coupled with free beam or fiber laser. Lasers Med. Sci. 2021, 36, 1865–1872. [Google Scholar] [CrossRef]
- Mincione, A.; Lepera, D.; Rizzi, L. VITOM 3D System in Parotid Gland Surgery: Our Experience. J. Craniofacial Surg. 2021, 32, e138–e141. [Google Scholar] [CrossRef]
- Carta, F.; Mariani, C.; Marrosu, V.; Gerosa, C.; Puxeddu, R. Three-dimensional, high-definition exoscopic parotidectomy: A valid alternative to magnified-assisted surgery. Br. J. Oral Maxillofac. Surg. 2020, 58, 1128–1132. [Google Scholar] [CrossRef]
- Capaccio, P.; Di Pasquale, D.; Bresciani, L.; Torretta, S.; Pignataro, L. 3D video-assisted trans-oral removal of deep hilo-parenchymal sub-mandibular stones. Acta Otorhinolaryngol. Ital. 2019, 39, 367–373. [Google Scholar] [CrossRef] [Green Version]
- Ferreli, F.; Di Bari, M.; Mercante, G.; De Virgilio, A.; Spriano, G. 3D 4K VITOM-assisted transoral removal of distal stone in the Wharton’s duct. Am. J. Otolaryngol. 2021, 42, 102821. [Google Scholar] [CrossRef]
- De Virgilio, A.; Mercante, G.; Gaino, F.; Yiu, P.; Ms, T.M.; Malvezzi, L.; Colombo, G.; Pellini, R.; Spriano, G. Preliminary clinical experience with the 4 K3-dimensional microvideoscope (VITOM 3D) system for free flap head and neck reconstruction. Head Neck 2020, 42, 138–140. [Google Scholar] [CrossRef]
- De Virgilio, A.; Festa, B.M.; Costantino, A.; Mercante, G.; Spriano, G. High-definition 3D exoscope-assisted soft palate excision and reconstruction. Head Neck 2022, 44, 292–295. [Google Scholar] [CrossRef] [PubMed]
- Belykh, E.; George, L.; Zhao, X.; Carotenuto, A.; Moreira, L.B.; Yağmurlu, K.; Bozkurt, B.; Byvaltsev, V.A.; Nakaji, P.; Preul, M.C. Microvascular anastomosis under 3D exoscope or endoscope magnification: A proof-of-concept study. Surg. Neurol. Int. 2018, 9, 115. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors, Year, Reference | Study Design | Patients | Treatment | Results | Surgical Techniques: Comparison and Complications | Surgical Times, Cost Effectiveness |
|---|---|---|---|---|---|---|
| Colombo et al., 2021 [1] | Retrospective study | 13 | Ear surgery | There was no significant statistical difference between the two groups concerning ORst1 (p = 0.90), ORst2 (p = 0.76), and operation time (p = 0.59). The tympanoplasty with mastoidectomy median operation time was 163 min (IQ25–75: 144–210) in the exoscope group and 148 min (IQ25–75: 128–165) in the operative microscope group; no statistical difference was found between the two groups (p = 0.23). The operation time for binaural cochlear implant case number 12 was 152 min using the exoscope and 158 min using the operative microscope; for case number 13, the operation time was 174 min with the exoscope and 211 min with the operative microscope. | Easier positioning of the exoscope inside the operating room due to its weight being significantly lower than that of the operative microscope (0.7 kg vs. > 229 kg). It is easier to maneuver, and it occupies a smaller amount of space. Advantages include lightness, maneuverability, and compactness. It can be easily one-handedly rotated and moved in any direction, achieving even narrow view angles. The exoscope needs a large surgical corridor to guarantee good performance. The wider variety of visual angles in exoscope surgery makes it necessary to define a new anatomical point of view, with specific training. | The exoscope was cheaper than a modern operative microscope. No significant differences were reported in the surgical times in group comparison (p < 0.05). |
| De Virgilio et al., 2021 [2] | Prospective study | 10 | Micro-Laryngeal Surgery | The highest mean placement time in medical students and residents (81.29 s and 57.96 s, respectively) compared to E.N.T. staff members (45.10 s). Furthermore, among the outcomes, a level of satisfaction with the method was recorded in up to 90% of cases. | Maneuvering is intuitive thanks to manual movements via direct drag mode. Setup of the system is easy and fast thanks to the position preset, which memorizes standard robotic arm positions. It is, in fact, possible to save and recall previous positions without directly touching the robotic arm. | The mean times of the procedures were similar between the three groups (p < 0.05 for all). |
| Bartkowiak et al., 2021 [4] | Prospective study | 71 | Parotid surgery | A significantly higher percentage of patients in the exoscope group developed transient facial nerve paralysis (n = 9; 29% vs. n = 4, 10%). | A higher degree of movement freedom and excellent ergonomics with reduced fatigue. No exoscope-related complications were observed. | Both microscope and exoscope procedures had similar total operative times (>90 min). |
| Crosetti et al., 2020 [5] | Prospective study | 10 | Oropharyngeal surgery | Post-surgical pain was low; NRS: 1.2. One case of subcutaneous emphysema and one submental blood collection. | VITOM 3D proved to be a versatile and compact optical instrument, giving an excellent 3D image without oral cavity involvement. Only 2/41 ORL staff developed discomfort due to the 3D vision: headache and pain in the nose bridge. | The average cost of consumables (VITOM and joystick sterile coating) per procedure was €62 (€41 and €21, respectively). Effectiveness is comparable with TORS and microscopic transoral techniques, but with lower platform costs. |
| Wierzbicka et al., 2021 [14] | Prospective study | 60 | Otosurgery | The differences between the 3D exoscope and the microscope were not statistically significant (p = 0.488). | High-resolution 3D images, greater freedom for exoscope adjustment, and a comfortable surgical posture. In deeper areas of the middle ear, due to the surgical field narrowing, the exoscope provided worse visibility. | The average time for the procedure did not differ from the microscope for stapes (40 min). Contrasting field visualization depending on surgical steps. |
| Minoda et al., 2019 [15] | Case series | 2 | Middle ear cholesteatoma surgery | No residual cholesteatoma after 9 months postoperatively. | The higher magnification using the system caused a deterioration of the surgical images. Uncomfortable refocusing of the surgical 3D exoscope system. | It was quick and smooth, unlike the transition between microscope and endoscope. |
| Ally et al., 2021 [16] | Case report | 1 | Mastoid surgery | No postoperative complications. The patient was discharged on day 1 postoperatively because of comorbidities. At the 2-week follow-up, the graft had taken well, and there was no evidence of any remnant disease. | Head-up position procedure, more comfortable. Eight times the depth of field compared to the microscope and nearly twice the magnification. The light was too bright down the external auditory canal through a speculum. | The cost of the exoscopic platform (approximately £120,000) is comparable to the operating microscope and about 10 times lower than the da Vinci robotic surgical system. |
| Smith et al., 2019 [17] | Prospective study | 11 | Lateral skull base surgery | The exoscope was the sole visualization tool in 7 cases, with 4 including the use of an endoscope or microscope. There were no perioperative complications. Potential subjective advantages include superior ergonomics, compact size, and an equal visual experience for surgeons and observers. | New visualization system has a learning curve. Low lighting in small surgical corridors and pixilation at high magnification. | Surgeons became subjectively more comfortable and efficient with repeated exoscope usage. |
| Rubini et al., 2019 [18] | Retrospective study | 24 | Lateral skull base surgery | No intraoperative complication, while postoperatively, only one minor complication emerged. The facial and hearing function outcomes were fully comparable (p > 0.05). | The anatomical structures are more realistic, and the recognition and differentiation of the different structures are better with the 3D exoscopic view. The exoscope allowed a position with a horizontal view throughout the surgical operation. Surgeon experiences discomfort due to the use of fixed optics and limited movements. | The average operative time was 289 min in the exoscope group and 313 min in the microscope group. |
| Iwami et al., 2021 [19] | Retrospective study | 8 | Craniofacial Resection | The exoscope provided excellent 3D transcranial images in all the patients treated. The exoscopic transcranial approach was performed according to the same steps as the traditional C.F.R., which used a microscope. | Ability to be conveniently and rapidly interchanged with an endoscope improved ergonomics and shared operative view. Limited illumination and pixilation at high magnifications when using deep and narrow surgical corridors. | Lower costs, ease of portability, and educational benefits. |
| Tasca I. et al., 2016 [20] | Case report | 1 | Rhinoplasty | Visualization during interventions was improved, thereby allowing understanding of the procedures and enhancing the teaching environment. | High-definition images, whilst simultaneously maintaining the use of two operating hands. The operating field may always be centered on the screen even in cases of inevitable movements of anatomical structures during operating maneuvers, such as elevations of the tunnels or osteotomies. | Although several advantages were reported, the authors stated the system could not represent a substitute for traditional surgery. |
| Pirola et al., 2021 [21] | Retrospective study | 21 | Lacrimal surgery | At follow-up, 1/31 (3.2%) cases had persisting unilateral epiphora in the exo-endoscopic group, with 2/53 (3.8%) in the endoscopy-only group. No statistical differences among unsuccessful procedures (p = 0.896). | The concurrent picture in picture visualization has educational potential. Reduced stereoscopic effect, uncomfortable position, and increased eye strain due to watching a screen. | The mean procedure times were similar among the three groups enrolled (20.22 s, 21.92 s, and 22.59 s). |
| Bignami et al., 2021 [22] | Case report | 1 | Frontal Fibro-osseous removal | Effective removal of the lesion and good access to the whole frontal sinus, with proper control of critical areas. No complications. | High-quality recordings that are extremely useful for didactic purposes. Anatomical structures were enhanced and magnified for better appreciation. Additionally, the perspective is always the same as the main surgeon’s, which is an additional factor that might facilitate the transition from the role of assistant to first operator. “Head-up surgery” might be unfamiliar or difficult | The authors reported reduced operative time with consequent cost-effectiveness benefits. |
| Carlucci et al., 2012 [23] | Prospective study | 12 | Laryngeal surgery | Postoperative voice analysis showed a good result in the resolution of phonatory problems. Laryngeal biopsies were easy to obtain, as was the use of N.B.I. | Excellent visualization of laryngeal structures (especially Reinke’s edema), chordal cysts, N.B.I. usage, and proposed biopsies for neoformation. Limited sulcus visualization with the exoscope system. | - |
| Cantarella et al., 2021 [24] | Case series | 6 | Phonosurgery | Significant outcomes in dysphonia (p = 0.03), VHI-10 (p = 0.03), voice breathiness (p = 0.03), and maximal phonation time (p = 0.03). | Optimal depth of field. High illumination and definition of anatomical detail. The monitor needed to be oriented perpendicular to the surgeon’s view. No technical difficulty. | The time required to set up the equipment and perform the procedures was similar to the operative microscope. |
| Carobbio et al., 2021 [25] | Prospective study | 17 | Transoral microsurgery | Surgical times for both laryngeal and oropharyngeal/hypopharyngeal lesions (p = 0.17 and p = 0.59, respectively). | The smaller size of the viewing system allows for better ergonomics for both the first surgeon, the assistant, and the entire surgical team, improving the assistant’s maneuvers and teaching purposes. The 3D-HD exoscope has minimal image latency, especially observed during hand movements at high magnification. | Time-sensitive oncologic procedures such as transoral laser microsurgery or transoral resection of critical laryngotracheal stenosis could be carried out with the esoscopic system. |
| Mincione et al., 2021 [26] | Retrospective study | 9 | Parotid gland surgery | Superficial parotidectomy was performed in 5 cases (55.6%): type I–II in 2 cases (22.2%), type I and III in 1 case (11.1%). The postoperative period was uneventful for all patients, and no complications were reported. The mean operating time was 145 min (range 135–165 min). | Visualization, ergonomics, versatility, training, and education. Asthenopia and a long learning curve were reported. | - |
| Carta et al., 2020 [27] | Prospective study | 9 | Parotidectomy | No statistical significance in the range of postoperative transient facial nerve weakness of the present series (11.1%) and the range of the previous study (5.9%) (p = 0.532) in comparison. | The implementation of lighting and magnification of the surgical field and the capability for precise dissection of fine structures. Occurrence of fatigue, headache, dizziness, and eye strain during or after surgery due to the polarizing glasses needed to provide a 3D view for the length of the procedure. | The mean (range) time of surgery was 149.4 (115–210) min. No postoperative complications were experienced; the mean hospitalization time was 3.8 days. |
| Capaccio et al., 2011 [28] | Prospective study | 5 | Submandibular gland surgery | Successful stone removal and significant subjective improvement were achieved. One of the patients revealed a residual 3 mm asymptomatic Hilo-parenchymal stone, consequently removed. Wharton’s duct and the lingual nerve were identified and preserved in all cases. Only two patients required sialendoscopy to locate the stone more precisely. | A better view of the operating field by all members of the surgical team; clear anatomical delineation; and improved oral floor depth perception, lingual nerve, and Wharton’s duct. | No substantial difference between 2D and 3D endoscopic surgery in terms of blood loss and operative times. |
| Ferreli et al., 2020 [29] | Case report | 1 | Transoral surgery of calculus of Wharton’s duct | High-quality magnification of the oral pelvis, easy identification of the entrance of the left submandibular gland duct, and the calculus was obtained. No postoperative complications occurred. At 7 days postoperative follow-up, the patient had developed a neo-ostium 5 mm from the papilla. | The risk for iatrogenic lesions of the lingual nerve was reduced. However, it was possible to treat only palpable and anterior stones. | - |
| De Virgilio et al., 2020 [30] | Prospective study | 10 | Free flap head and neck reconstruction | The exoscope system provided sufficient access, reach, and visualization to perform successfully free flap harvesting and microvascular anastomosis. No significant complications. | Using the 3D glasses, both surgeons and nurses benefit from the same visualization throughout the entire procedure | - |
| De Virgilio et al., 2021 [31] | Case report | 1 | Soft palate excision and reconstruction | Exoscopic technology has been proven to benefit each step of head and neck demolition and reconstruction. The magnified surgical field obtained with the exoscopic technology permits higher surgical precision. | The necessity to wear 3D glasses can be bothersome for some operators because the lenses are dark, and the exoscope is used in half-light to enhance the visual quality of the screen. | The authors suggested conducting more specific studies to define the potential impact of the exoscope on setup and surgery time. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferlito, S.; La Mantia, I.; Caruso, S.; Cammaroto, G.; Chiesa-Estomba, C.M.; Iannella, G.; Nocera, F.; Ingrassia, A.; Cocuzza, S.; Vicini, C.; et al. High Definition Three-Dimensional Exoscope (VITOM 3D) in E.N.T. Surgery: A Systematic Review of Current Experience. J. Clin. Med. 2022, 11, 3639. https://doi.org/10.3390/jcm11133639
Ferlito S, La Mantia I, Caruso S, Cammaroto G, Chiesa-Estomba CM, Iannella G, Nocera F, Ingrassia A, Cocuzza S, Vicini C, et al. High Definition Three-Dimensional Exoscope (VITOM 3D) in E.N.T. Surgery: A Systematic Review of Current Experience. Journal of Clinical Medicine. 2022; 11(13):3639. https://doi.org/10.3390/jcm11133639
Chicago/Turabian StyleFerlito, Salvatore, Ignazio La Mantia, Sebastiano Caruso, Giovanni Cammaroto, Carlos Miguel Chiesa-Estomba, Giannicola Iannella, Francesco Nocera, Angelo Ingrassia, Salvatore Cocuzza, Claudio Vicini, and et al. 2022. "High Definition Three-Dimensional Exoscope (VITOM 3D) in E.N.T. Surgery: A Systematic Review of Current Experience" Journal of Clinical Medicine 11, no. 13: 3639. https://doi.org/10.3390/jcm11133639
APA StyleFerlito, S., La Mantia, I., Caruso, S., Cammaroto, G., Chiesa-Estomba, C. M., Iannella, G., Nocera, F., Ingrassia, A., Cocuzza, S., Vicini, C., Hans, S., Lechien, J. R., & Maniaci, A. (2022). High Definition Three-Dimensional Exoscope (VITOM 3D) in E.N.T. Surgery: A Systematic Review of Current Experience. Journal of Clinical Medicine, 11(13), 3639. https://doi.org/10.3390/jcm11133639