
Predicting, Recognizing, and Treating Right Heart Failure in Patients Undergoing Durable LVAD Therapy


Abstract
:1. Introduction
2. Right Heart Function in LVADs
2.1. Anatomy and Function of the Right Heart
2.2. Influence of VAD on Right Heart Function
3. Diagnosis and Recognition of Right Heart Failure
3.1. Definitions of Early and Late Right Heart Failure
3.2. Risk Models
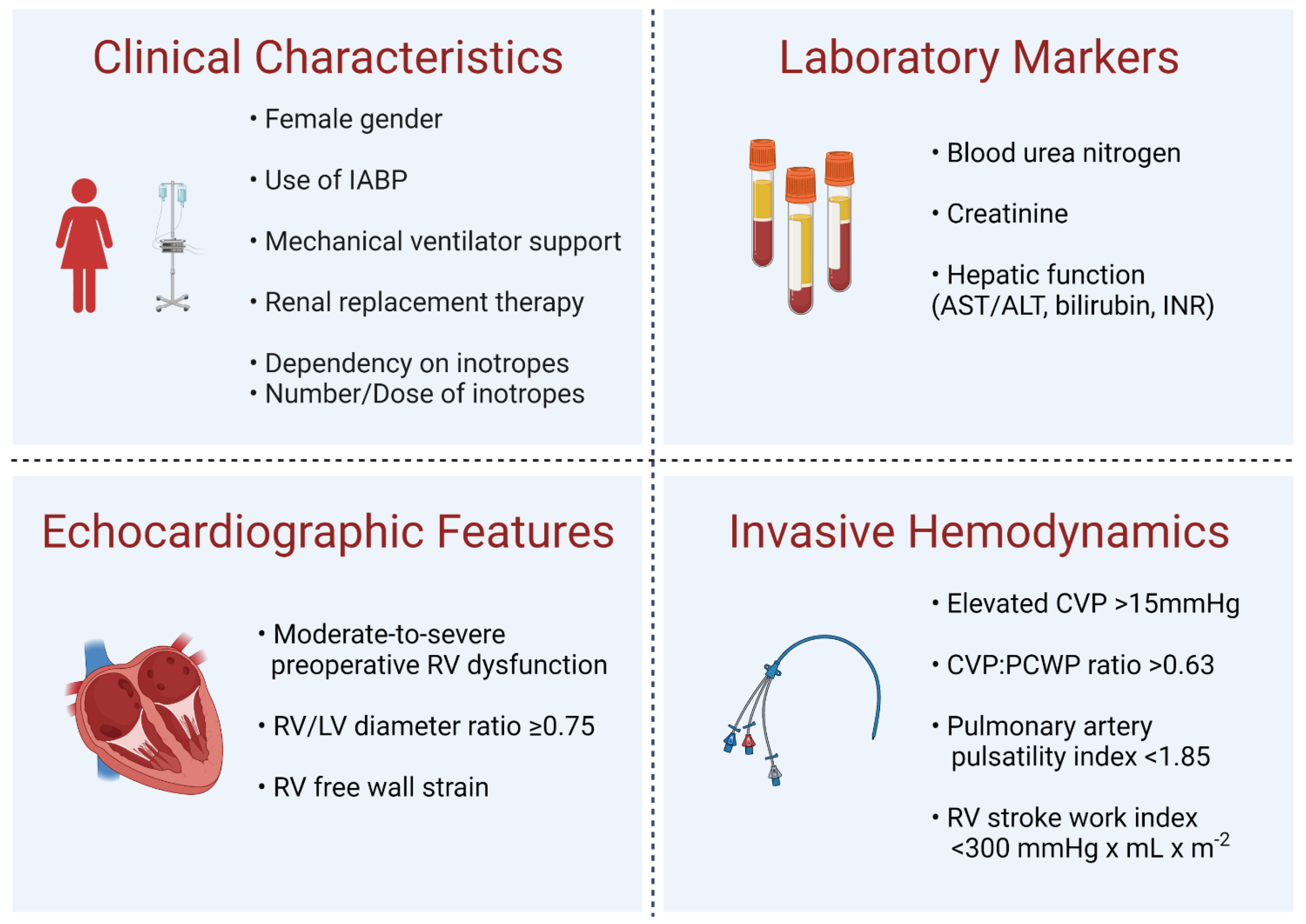
3.3. Risk Factors
4. Management of Right Heart Failure
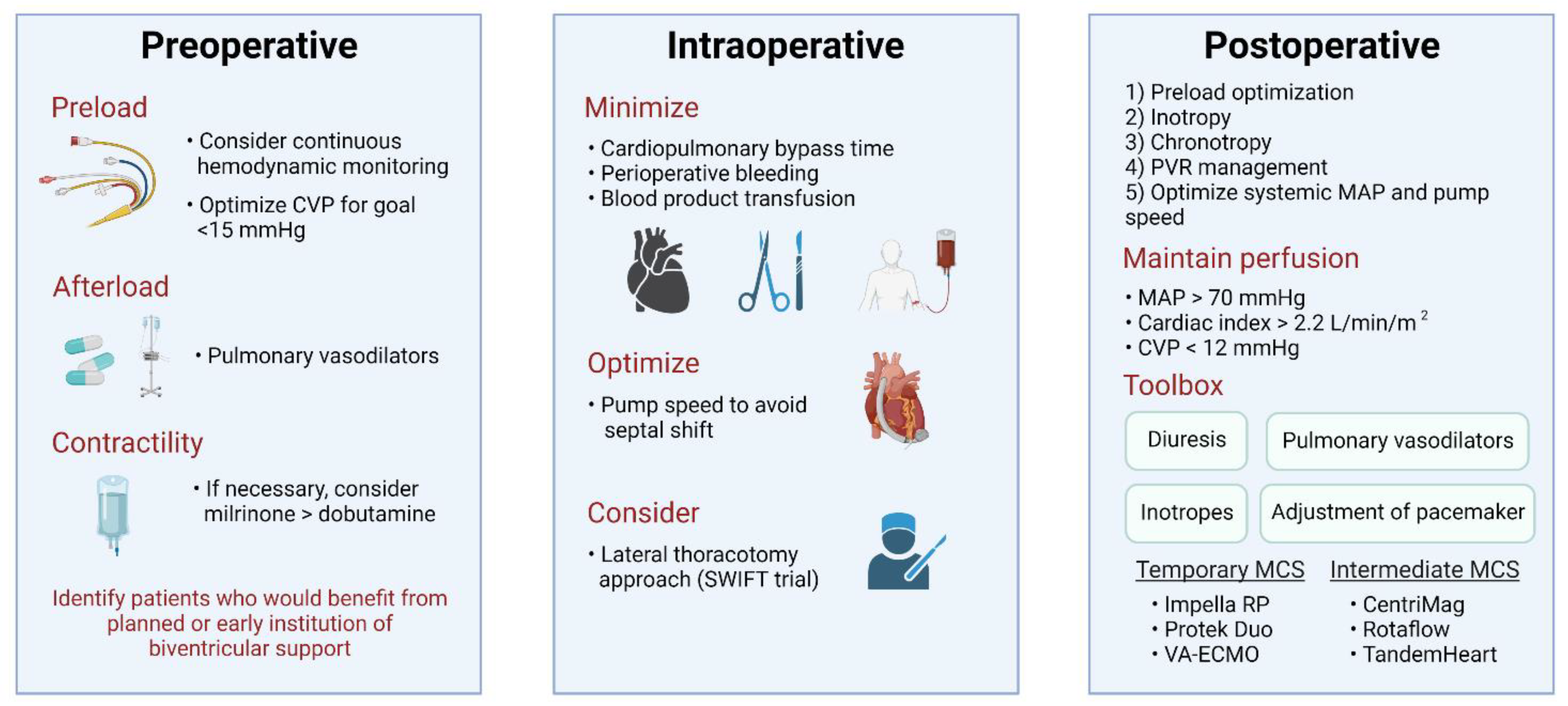
4.1. Preoperative Medical Management
4.2. Intraoperative Management
4.3. Postoperative Management
4.4. Mechanical Support
5. Future Directions and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Mehra, M.R.; Cleveland, J.C.; Uriel, N.; Cowger, J.A.; Hall, S.; Horstmanshof, D.; Naka, Y.; Salerno, C.T.; Chuang, J.; Williams, C.; et al. Primary Results of Long-Term Outcomes in the MOMENTUM 3 Pivotal Trial and Continued Access Protocol Study Phase: A Study of 2200 HeartMate 3 Left Ventricular Assist Device Implants. Eur. J. Heart Fail. 2021, 23, 1392–1400. [Google Scholar] [CrossRef] [PubMed]
- Mehra, M.R.; Goldstein, D.J.; Uriel, N.; Cleveland, J.C.; Yuzefpolskaya, M.; Salerno, C.; Walsh, M.N.; Milano, C.A.; Patel, C.B.; Ewald, G.A.; et al. Two-Year Outcomes with a Magnetically Levitated Cardiac Pump in Heart Failure. N. Engl. J. Med. 2018, 378, 1386–1395. [Google Scholar] [CrossRef] [PubMed]
- Soliman, O.I.I.; Akin, S.; Muslem, R.; Boersma, E.; Manintveld, O.C.; Krabatsch, T.; Gummert, J.F.; de By, T.M.M.H.; Bogers, A.J.J.C.; Zijlstra, F.; et al. Derivation and Validation of a Novel Right-Sided Heart Failure Model After Implantation of Continuous Flow Left Ventricular Assist Devices: The EUROMACS (European Registry for Patients with Mechanical Circulatory Support) Right-Sided Heart Failure Risk Score. Circulation 2018, 137, 891–906. [Google Scholar] [CrossRef] [PubMed]
- Loghmanpour, N.A.; Kormos, R.L.; Kanwar, M.K.; Teuteberg, J.J.; Murali, S.; Antaki, J.F. A Bayesian Model to Predict Right Ventricular Failure Following Left Ventricular Assist Device Therapy. JACC Heart Fail. 2016, 4, 711–721. [Google Scholar] [CrossRef]
- Kalogeropoulos, A.P.; Kelkar, A.; Weinberger, J.F.; Morris, A.A.; Georgiopoulou, V.V.; Markham, D.W.; Butler, J.; Vega, J.D.; Smith, A.L. Validation of Clinical Scores for Right Ventricular Failure Prediction after Implantation of Continuous-Flow Left Ventricular Assist Devices. J. Heart Lung Transplant. 2015, 34, 1595–1603. [Google Scholar] [CrossRef]
- Kormos, R.L.; Teuteberg, J.J.; Pagani, F.D.; Russell, S.D.; John, R.; Miller, L.W.; Massey, T.; Milano, C.A.; Moazami, N.; Sundareswaran, K.S.; et al. Right Ventricular Failure in Patients with the HeartMate II Continuous-Flow Left Ventricular Assist Device: Incidence, Risk Factors, and Effect on Outcomes. J. Thorac. Cardiovasc. Surg. 2010, 139, 1316–1324. [Google Scholar] [CrossRef] [Green Version]
- Dang, N.C.; Topkara, V.K.; Mercando, M.; Kay, J.; Kruger, K.H.; Aboodi, M.S.; Oz, M.C.; Naka, Y. Right Heart Failure After Left Ventricular Assist Device Implantation in Patients With Chronic Congestive Heart Failure. J. Heart Lung Transplant. 2006, 25, 1–6. [Google Scholar] [CrossRef]
- Rich, J.D.; Gosev, I.; Patel, C.B.; Joseph, S.; Katz, J.N.; Eckman, P.M.; Lee, S.; Sundareswaran, K.; Kilic, A.; Bethea, B.; et al. The Incidence, Risk Factors, and Outcomes Associated with Late Right-Sided Heart Failure in Patients Supported with an Axial-Flow Left Ventricular Assist Device. J. Heart Lung Transplant. 2017, 36, 50–58. [Google Scholar] [CrossRef] [Green Version]
- Takeda, K.; Naka, Y.; Yang, J.A.; Uriel, N.; Colombo, P.C.; Jorde, U.P.; Takayama, H. Outcome of Unplanned Right Ventricular Assist Device Support for Severe Right Heart Failure after Implantable Left Ventricular Assist Device Insertion. J. Heart Lung Transplant. Off. Publ. Int. Soc. Heart Transplant. 2014, 33, 141–148. [Google Scholar] [CrossRef]
- Takeda, K.; Takayama, H.; Colombo, P.C.; Yuzefpolskaya, M.; Fukuhara, S.; Han, J.; Kurlansky, P.; Mancini, D.M.; Naka, Y. Incidence and Clinical Significance of Late Right Heart Failure during Continuous-Flow Left Ventricular Assist Device Support. J. Heart Lung Transplant. 2015, 34, 1024–1032. [Google Scholar] [CrossRef] [Green Version]
- Estep, J.D.; Soltesz, E.; Cogswell, R. The New Heart Transplant Allocation System: Early Observations and Mechanical Circulatory Support Considerations. J. Thorac. Cardiovasc. Surg. 2021, 161, 1839–1846. [Google Scholar] [CrossRef] [PubMed]
- Hanff, T.C.; Harhay, M.O.; Kimmel, S.E.; Molina, M.; Mazurek, J.A.; Goldberg, L.R.; Birati, E.Y. Trends in Mechanical Support Use as a Bridge to Adult Heart Transplant Under New Allocation Rules. JAMA Cardiol. 2020, 5, 728–729. [Google Scholar] [CrossRef] [PubMed]
- James, T.N. Anatomy of the Crista Supraventricularis: Its Importance for Understanding Right Ventricular Function, Right Ventricular Infarction and Related Conditions. J. Am. Coll. Cardiol. 1985, 6, 1083–1095. [Google Scholar] [CrossRef] [Green Version]
- Konstam, M.A.; Kiernan, M.S.; Bernstein, D.; Bozkurt, B.; Jacob, M.; Kapur, N.K.; Kociol, R.D.; Lewis, E.F.; Mehra, M.R.; Pagani, F.D.; et al. Evaluation and Management of Right-Sided Heart Failure: A Scientific Statement from the American Heart Association. Circulation 2018, 137, e578–e622. [Google Scholar] [CrossRef]
- Lampert, B.C.; Teuteberg, J.J. Right Ventricular Failure after Left Ventricular Assist Devices. J. Heart Lung Transplant. Off. Publ. Int. Soc. Heart Transplant. 2015, 34, 1123–1130. [Google Scholar] [CrossRef] [Green Version]
- El Hajj, M.C.; Viray, M.C.; Tedford, R.J. Right Heart Failure: A Hemodynamic Review. Cardiol. Clin. 2020, 38, 161–173. [Google Scholar] [CrossRef]
- Haddad, F.; Hunt, S.A.; Rosenthal, D.N.; Murphy, D.J. Right Ventricular Function in Cardiovascular Disease, Part I. Circulation 2008, 117, 1436–1448. [Google Scholar] [CrossRef]
- Tedford, R.J. Determinants of Right Ventricular Afterload (2013 Grover Conference Series). Pulm. Circ. 2014, 4, 211–219. [Google Scholar] [CrossRef] [Green Version]
- Nakagawa, A.; Yasumura, Y.; Yoshida, C.; Okumura, T.; Tateishi, J.; Yoshida, J.; Abe, H.; Tamaki, S.; Yano, M.; Hayashi, T.; et al. Prognostic Importance of Right Ventricular-Vascular Uncoupling in Acute Decompensated Heart Failure With Preserved Ejection Fraction. Circ. Cardiovasc. Imaging 2020, 13, e011430. [Google Scholar] [CrossRef]
- Wright, S.P.; Groves, L.; Vishram-Nielsen, J.K.K.; Karvasarski, E.; Valle, F.H.; Alba, A.C.; Mak, S. Elevated Pulmonary Arterial Elastance and Right Ventricular Uncoupling Are Associated with Greater Mortality in Advanced Heart Failure. J. Heart Lung Transplant. 2020, 39, 657–665. [Google Scholar] [CrossRef]
- Bellavia, D.; Iacovoni, A.; Scardulla, C.; Moja, L.; Pilato, M.; Kushwaha, S.S.; Senni, M.; Clemenza, F.; Agnese, V.; Falletta, C.; et al. Prediction of Right Ventricular Failure after Ventricular Assist Device Implant: Systematic Review and Meta-Analysis of Observational Studies. Eur. J. Heart Fail. 2017, 19, 926–946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayek, S.; Sims, D.B.; Markham, D.W.; Butler, J.; Kalogeropoulos, A.P. Assessment of Right Ventricular Function in Left Ventricular Assist Device Candidates. Circ. Cardiovasc. Imaging 2014, 7, 379–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raina, A.; Vaidya, A.; Gertz, Z.M.; Chambers, S.; Forfia, P.R. Marked Changes in Right Ventricular Contractile Pattern after Cardiothoracic Surgery: Implications for Post-Surgical Assessment of Right Ventricular Function. J. Heart Lung Transplant. 2013, 32, 777–783. [Google Scholar] [CrossRef] [PubMed]
- Cogswell, R.; John, R.; Shaffer, A. Right Ventricular Failure After Left Ventricular Assist Device. Cardiol. Clin. 2020, 38, 219–225. [Google Scholar] [CrossRef]
- Houston, B.A.; Kalathiya, R.J.; Hsu, S.; Loungani, R.; Davis, M.E.; Coffin, S.T.; Haglund, N.; Maltais, S.; Keebler, M.E.; Leary, P.J.; et al. Right Ventricular Afterload Sensitivity Dramatically Increases after Left Ventricular Assist Device Implantation: A Multi-Center Hemodynamic Analysis. J. Heart Lung Transplant. Off. Publ. Int. Soc. Heart Transplant. 2016, 35, 868–876. [Google Scholar] [CrossRef] [Green Version]
- Shore, S.; Hanff, T.C.; Mazurek, J.A.; Seigerman, M.; Zhang, R.; Grandin, E.W.; Vorovich, E.; Mather, P.; Olt, C.; Howard, J.; et al. The Effect of Transfusion of Blood Products on Ventricular Assist Device Support Outcomes. ESC Heart Fail. 2020, 7, 3573–3581. [Google Scholar] [CrossRef]
- Gulati, G.; Ruthazer, R.; Denofrio, D.; Vest, A.R.; Kent, D.; Kiernan, M.S. Understanding Longitudinal Changes in Pulmonary Vascular Resistance After Left Ventricular Assist Device Implantation. J. Card. Fail. 2021, 27, 552–559. [Google Scholar] [CrossRef]
- Birati, E.Y.; Mazurek, J.A. Changes in Pulmonary Vascular Resistance after Left Ventricular Assist Device Implantation: “The Post-VAD Residual”. J. Card. Fail. 2021, 27, 618–619. [Google Scholar] [CrossRef]
- Matthews, J.C.; Koelling, T.M.; Pagani, F.D.; Aaronson, K.D. The Right Ventricular Failure Risk Score: A Pre-Operative Tool for Assessing the Risk of Right Ventricular Failure in Left Ventricular Assist Device Candidates. J. Am. Coll. Cardiol. 2008, 51, 2163–2172. [Google Scholar] [CrossRef] [Green Version]
- Fitzpatrick, J.R.; Frederick, J.R.; Hsu, V.M.; Kozin, E.D.; O’Hara, M.L.; Howell, E.; Dougherty, D.; McCormick, R.C.; Laporte, C.A.; Cohen, J.E.; et al. Risk Score Derived from Pre-Operative Data Analysis Predicts the Need for Biventricular Mechanical Circulatory Support. J. Heart Lung Transplant. 2008, 27, 1286–1292. [Google Scholar] [CrossRef] [Green Version]
- Drakos, S.G.; Janicki, L.; Horne, B.D.; Kfoury, A.G.; Reid, B.B.; Clayson, S.; Horton, K.; Haddad, F.; Li, D.Y.; Renlund, D.G.; et al. Risk Factors Predictive of Right Ventricular Failure After Left Ventricular Assist Device Implantation. Am. J. Cardiol. 2010, 105, 1030–1035. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Simon, M.A.; Bonde, P.; Harris, B.U.; Teuteberg, J.J.; Kormos, R.L.; Antaki, J.F. Decision Tree for Adjuvant Right Ventricular Support in Patients Receiving a Left Ventricular Assist Device. J. Heart Lung Transplant. 2012, 31, 140–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atluri, P.; Goldstone, A.B.; Fairman, A.S.; MacArthur, J.W.; Shudo, Y.; Cohen, J.E.; Acker, A.L.; Hiesinger, W.; Howard, J.L.; Acker, M.A.; et al. Predicting Right Ventricular Failure in the Modern, Continuous Flow Left Ventricular Assist Device Era. Ann. Thorac. Surg. 2013, 96, 857–864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehra, M.R.; Uriel, N.; Naka, Y.; Cleveland, J.C.; Yuzefpolskaya, M.; Salerno, C.T.; Walsh, M.N.; Milano, C.A.; Patel, C.B.; Hutchins, S.W.; et al. A Fully Magnetically Levitated Left Ventricular Assist Device—Final Report. N. Engl. J. Med. 2019, 380, 1618–1627. [Google Scholar] [CrossRef]
- Lenderman, J.C. Intermacs Appendices—School of Medicine—Interagency Registry for Mechanically Assisted Circulatory Support|UAB. Available online: https://www.uab.edu/medicine/intermacs/intermacs-documents (accessed on 7 August 2021).
- Frankfurter, C.; Molinero, M.; Vishram-Nielsen, J.K.K.; Foroutan, F.; Mak, S.; Rao, V.; Billia, F.; Orchanian-Cheff, A.; Alba, A.C. Predicting the Risk of Right Ventricular Failure in Patients Undergoing Left Ventricular Assist Device Implantation. Circ. Heart Fail. 2020, 13, e006994. [Google Scholar] [CrossRef]
- Benjamin, M.M.; Sundararajan, S.; Sulaiman, S.; Miles, B.; Walker, R.J.; Durham, L.; Kohmoto, T.; Joyce, D.L.; Ishizawar, D.; Gaglianello, N.; et al. Association of Preoperative Duration of Inotropy on Prevalence of Right Ventricular Failure Following LVAD Implantation. ESC Heart Fail. 2020, 7, 1949–1955. [Google Scholar] [CrossRef]
- Stricagnoli, M.; Sciaccaluga, C.; Mandoli, G.E.; Rizzo, L.; Sisti, N.; Aboumarie, H.S.; Benfari, G.; Maritan, L.; Tsioulpas, C.; Bernazzali, S.; et al. Clinical, Echocardiographic and Hemodynamic Predictors of Right Heart Failure after LVAD Placement. Int. J. Cardiovasc. Imaging 2022, 38, 561–570. [Google Scholar] [CrossRef]
- Grant, A.D.M.; Smedira, N.G.; Starling, R.C.; Marwick, T.H. Independent and Incremental Role of Quantitative Right Ventricular Evaluation for the Prediction of Right Ventricular Failure after Left Ventricular Assist Device Implantation. J. Am. Coll. Cardiol. 2012, 60, 521–528. [Google Scholar] [CrossRef] [Green Version]
- Kato, T.S.; Farr, M.; Schulze, P.C.; Maurer, M.; Shahzad, K.; Iwata, S.; Homma, S.; Jorde, U.; Takayama, H.; Naka, Y.; et al. Usefulness of Two-Dimensional Echocardiographic Parameters of the Left Side of the Heart to Predict Right Ventricular Failure after Left Ventricular Assist Device Implantation. Am. J. Cardiol. 2012, 109, 246–251. [Google Scholar] [CrossRef]
- Chriqui, L.-E.; Monney, P.; Kirsch, M.; Tozzi, P. Prediction of Right Ventricular Failure after Left Ventricular Assist Device Implantation in Patients with Heart Failure: A Meta-Analysis Comparing Echocardiographic Parameters. Interact. Cardiovasc. Thorac. Surg. 2021, 33, 784–792. [Google Scholar] [CrossRef]
- Kato, T.S.; Jiang, J.; Schulze, P.C.; Jorde, U.; Uriel, N.; Kitada, S.; Takayama, H.; Naka, Y.; Mancini, D.; Gillam, L.; et al. Serial Echocardiography Using Tissue Doppler and Speckle Tracking Imaging to Monitor Right Ventricular Failure before and after Left Ventricular Assist Device Surgery. JACC Heart Fail. 2013, 1, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Vivo, R.P.; Cordero-Reyes, A.M.; Qamar, U.; Garikipati, S.; Trevino, A.R.; Aldeiri, M.; Loebe, M.; Bruckner, B.A.; Torre-Amione, G.; Bhimaraj, A.; et al. Increased Right-to-Left Ventricle Diameter Ratio Is a Strong Predictor of Right Ventricular Failure after Left Ventricular Assist Device. J. Heart Lung Transplant. 2013, 32, 792–799. [Google Scholar] [CrossRef] [PubMed]
- Kukucka, M.; Stepanenko, A.; Potapov, E.; Krabatsch, T.; Redlin, M.; Mladenow, A.; Kuppe, H.; Hetzer, R.; Habazettl, H. Right-to-Left Ventricular End-Diastolic Diameter Ratio and Prediction of Right Ventricular Failure with Continuous-Flow Left Ventricular Assist Devices. J. Heart Lung Transplant. Off. Publ. Int. Soc. Heart Transplant. 2011, 30, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Dufendach, K.A.; Zhu, T.; Diaz Castrillon, C.; Hong, Y.; Countouris, M.E.; Hickey, G.; Keebler, M.; Thoma, F.W.; Kilic, A. Pre-Implant Right Ventricular Free Wall Strain Predicts Post-LVAD Right Heart Failure. J. Card. Surg. 2021, 36, 1996–2003. [Google Scholar] [CrossRef]
- Liang, L.W.; Jamil, A.; Mazurek, J.A.; Urgo, K.A.; Wald, J.; Birati, E.Y.; Han, Y. Right Ventricular Global Longitudinal Strain as a Predictor of Acute and Early Right Heart Failure Post Left Ventricular Assist Device Implantation. ASAIO J. Am. Soc. Artif. Intern. Organs 1992 2022, 68, 333–339. [Google Scholar] [CrossRef]
- Dandel, M.; Potapov, E.; Krabatsch, T.; Stepanenko, A.; Löw, A.; Vierecke, J.; Knosalla, C.; Hetzer, R. Load Dependency of Right Ventricular Performance Is a Major Factor to Be Considered in Decision Making Before Ventricular Assist Device Implantation. Circulation 2013, 128, S14–S23. [Google Scholar] [CrossRef] [Green Version]
- Morine, K.J.; Kiernan, M.S.; Pham, D.T.; Paruchuri, V.; Denofrio, D.; Kapur, N.K. Pulmonary Artery Pulsatility Index Is Associated With Right Ventricular Failure After Left Ventricular Assist Device Surgery. J. Card. Fail. 2016, 22, 110–116. [Google Scholar] [CrossRef]
- Kang, G.; Ha, R.; Banerjee, D. Pulmonary Artery Pulsatility Index Predicts Right Ventricular Failure after Left Ventricular Assist Device Implantation. J. Heart Lung Transplant. Off. Publ. Int. Soc. Heart Transplant. 2016, 35, 67–73. [Google Scholar] [CrossRef]
- Grandin, E.W.; Zamani, P.; Mazurek, J.A.; Troutman, G.S.; Birati, E.Y.; Vorovich, E.; Chirinos, J.A.; Tedford, R.J.; Margulies, K.B.; Atluri, P.; et al. Right Ventricular Response to Pulsatile Load Is Associated with Early Right Heart Failure and Mortality after Left Ventricular Assist Device. J. Heart Lung Transplant. 2017, 36, 97–105. [Google Scholar] [CrossRef]
- Argenziano, M.; Choudhri, A.F.; Moazami, N.; Rose, E.A.; Smith, C.R.; Levin, H.R.; Smerling, A.J.; Oz, M.C. Randomized, Double-Blind Trial of Inhaled Nitric Oxide in LVAD Recipients with Pulmonary Hypertension. Ann. Thorac. Surg. 1998, 65, 340–345. [Google Scholar] [CrossRef]
- Lovich, M.A.; Pezone, M.J.; Wakim, M.G.; Denton, R.J.; Maslov, M.Y.; Murray, M.R.; Tsukada, H.; Agnihotri, A.K.; Roscigno, R.F.; Gamero, L.G.; et al. Inhaled Nitric Oxide Augments Left Ventricular Assist Device Capacity by Ameliorating Secondary Right Ventricular Failure. ASAIO J. Am. Soc. Artif. Intern. Organs 1992 2015, 61, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Khazanie, P.; Hammill, B.G.; Patel, C.B.; Kiernan, M.S.; Cooper, L.B.; Arnold, S.V.; Fendler, T.J.; Spertus, J.A.; Curtis, L.H.; Hernandez, A.F. Use of Heart Failure Medical Therapies Among Patients With Left Ventricular Assist Devices: Insights From INTERMACS. J. Card. Fail. 2016, 22, 672–679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gulati, G.; Grandin, E.W.; Kennedy, K.; Cabezas, F.; DeNofrio, D.D.; Kociol, R.; Rame, J.E.; Pagani, F.D.; Kirklin, J.K.; Kormos, R.L.; et al. Preimplant Phosphodiesterase-5 Inhibitor Use Is Associated With Higher Rates of Severe Early Right Heart Failure After Left Ventricular Assist Device Implantation. Circ. Heart Fail. 2019, 12, e005537. [Google Scholar] [CrossRef] [PubMed]
- Turner, K.R. Right Ventricular Failure After Left Ventricular Assist Device Placement-The Beginning of the End or Just Another Challenge? J. Cardiothorac. Vasc. Anesth. 2019, 33, 1105–1121. [Google Scholar] [CrossRef] [PubMed]
- McGee, E.; Danter, M.; Strueber, M.; Mahr, C.; Mokadam, N.A.; Wieselthaler, G.; Klein, L.; Lee, S.; Boeve, T.; Maltais, S.; et al. Evaluation of a Lateral Thoracotomy Implant Approach for a Centrifugal-Flow Left Ventricular Assist Device: The LATERAL Clinical Trial. J. Heart Lung Transplant. 2019, 38, 344–351. [Google Scholar] [CrossRef]
- Abbott Medical Devices. In Implantation of the HeartMate 3 in Subjects with Heart Failure Using Surgical Techniques Other than Full Median Sternotomy; 2021. Available online: https://clinicaltrials.gov (accessed on 12 February 2022).
- Fujita, T.; Kobayashi, J.; Hata, H.; Seguchi, O.; Murata, Y.; Yanase, M.; Nakatani, T. Right Heart Failure and Benefits of Adjuvant Tricuspid Valve Repair in Patients Undergoing Left Ventricular Assist Device Implantation. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2014, 46, 802–807. [Google Scholar] [CrossRef] [Green Version]
- Piacentino, V.; Ganapathi, A.M.; Stafford-Smith, M.; Hsieh, M.K.; Patel, C.B.; Simeone, A.A.; Rogers, J.G.; Milano, C.A. Utility of Concomitant Tricuspid Valve Procedures for Patients Undergoing Implantation of a Continuous-Flow Left Ventricular Device. J. Thorac. Cardiovasc. Surg. 2012, 144, 1217–1221. [Google Scholar] [CrossRef] [Green Version]
- Piacentino, V.; Troupes, C.D.; Ganapathi, A.M.; Blue, L.J.; Mackensen, G.B.; Swaminathan, M.; Felker, G.M.; Stafford-Smith, M.; Lodge, A.J.; Rogers, J.G.; et al. Clinical Impact of Concomitant Tricuspid Valve Procedures During Left Ventricular Assist Device Implantation. Ann. Thorac. Surg. 2011, 92, 1414–1419. [Google Scholar] [CrossRef]
- Song, H.K.; Gelow, J.M.; Mudd, J.; Chien, C.; Tibayan, F.A.; Hollifield, K.; Naftel, D.; Kirklin, J. Limited Utility of Tricuspid Valve Repair at the Time of Left Ventricular Assist Device Implantation. Ann. Thorac. Surg. 2016, 101, 2168–2174. [Google Scholar] [CrossRef] [Green Version]
- Robertson, J.O.; Grau-Sepulveda, M.V.; Okada, S.; O’Brien, S.M.; Matthew Brennan, J.; Shah, A.S.; Itoh, A.; Damiano, R.J.; Prasad, S.; Silvestry, S.C. Concomitant Tricuspid Valve Surgery during Implantation of Continuous-Flow Left Ventricular Assist Devices: A Society of Thoracic Surgeons Database Analysis. J. Heart Lung Transplant. 2014, 33, 609–617. [Google Scholar] [CrossRef]
- Barac, Y.D.; Nicoara, A.; Bishawi, M.; Schroder, J.N.; Daneshmand, M.A.; Hashmi, N.K.; Velazquez, E.; Rogers, J.G.; Patel, C.B.; Milano, C.A. Durability and Efficacy of Tricuspid Valve Repair in Patients Undergoing Left Ventricular Assist Device Implantation. JACC Heart Fail. 2020, 8, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Zhigalov, K.; Szczechowicz, M.; Mashhour, A.; Kadyraliev, B.K.; Mkalaluh, S.; Easo, J.; Ennker, J.; Eichstaedt, H.C.; Weymann, A. Left Ventricular Assist Device Implantation with Concomitant Tricuspid Valve Repair: Is There Really a Benefit? J. Thorac. Dis. 2019, 11, S902–S912. [Google Scholar] [CrossRef] [PubMed]
- Fujino, T.; Imamura, T.; Nitta, D.; Kim, G.; Smith, B.; Kalantari, S.; Nguyen, A.; Chung, B.; Narang, N.; Holzhauser, L.; et al. Effect of Concomitant Tricuspid Valve Surgery With Left Ventricular Assist Device Implantation. Ann. Thorac. Surg. 2020, 110, 918–924. [Google Scholar] [CrossRef]
- Xanthopoulos, A.; Wolski, K.; Wang, Q.; Blackstone, E.H.; Randhawa, V.K.; Soltesz, E.G.; Young, J.B.; Nissen, S.E.; Estep, J.D.; Triposkiadis, F.; et al. Postimplant Phosphodiesterase-5 Inhibitor Use in Centrifugal Flow Left Ventricular Assist Devices. JACC Heart Fail. 2022, 10, 89–100. [Google Scholar] [CrossRef] [PubMed]
- Imamura, T.; Chung, B.; Nguyen, A.; Rodgers, D.; Sayer, G.; Adatya, S.; Sarswat, N.; Kim, G.; Raikhelkar, J.; Ota, T.; et al. Decoupling between Diastolic Pulmonary Artery Pressure and Pulmonary Capillary Wedge Pressure as a Prognostic Factor After Continuous Flow Ventricular Assist Device Implantation. Circ. Heart Fail. 2017, 10, e003882. [Google Scholar] [CrossRef] [Green Version]
- Imamura, T.; Narang, N.; Kim, G.; Raikhelkar, J.; Chung, B.; Nguyen, A.; Holzhauser, L.; Rodgers, D.; Kalantari, S.; Smith, B.; et al. Decoupling between Diastolic Pulmonary Artery and Pulmonary Capillary Wedge Pressures Is Associated With Right Ventricular Dysfunction and Hemocompatibility-Related Adverse Events in Patients With Left Ventricular Assist Devices. J. Am. Heart Assoc. 2020, 9, e014801. [Google Scholar] [CrossRef]
- Morgan, J.A.; John, R.; Lee, B.J.; Oz, M.C.; Naka, Y. Is Severe Right Ventricular Failure in Left Ventricular Assist Device Recipients a Risk Factor for Unsuccessful Bridging to Transplant and Post-Transplant Mortality. Ann. Thorac. Surg. 2004, 77, 859–863. [Google Scholar] [CrossRef]
- Fitzpatrick, J.R.; Frederick, J.R.; Hiesinger, W.; Hsu, V.M.; McCormick, R.C.; Kozin, E.D.; Laporte, C.M.; O’Hara, M.L.; Howell, E.; Dougherty, D.; et al. Early Planned Institution of Biventricular Mechanical Circulatory Support Results in Improved Outcomes Compared with Delayed Conversion of a Left Ventricular Assist Device to a Biventricular Assist Device. J. Thorac. Cardiovasc. Surg. 2009, 137, 971–977. [Google Scholar] [CrossRef] [Green Version]
- Kapur, N.K.; Esposito, M.L.; Bader, Y.; Morine, K.J.; Kiernan, M.S.; Pham, D.T.; Burkhoff, D. Mechanical Circulatory Support Devices for Acute Right Ventricular Failure. Circulation 2017, 136, 314–326. [Google Scholar] [CrossRef] [Green Version]
- Lo Coco, V.; De Piero, M.E.; Massimi, G.; Chiarini, G.; Raffa, G.M.; Kowalewski, M.; Maessen, J.; Lorusso, R. Right Ventricular Failure after Left Ventricular Assist Device Implantation: A Review of the Literature. J. Thorac. Dis. 2021, 13, 1256–1269. [Google Scholar] [CrossRef]
- Anderson, M.B.; Goldstein, J.; Milano, C.; Morris, L.D.; Kormos, R.L.; Bhama, J.; Kapur, N.K.; Bansal, A.; Garcia, J.; Baker, J.N.; et al. Benefits of a Novel Percutaneous Ventricular Assist Device for Right Heart Failure: The Prospective RECOVER RIGHT Study of the Impella RP Device. J. Heart Lung Transplant. Off. Publ. Int. Soc. Heart Transplant. 2015, 34, 1549–1560. [Google Scholar] [CrossRef] [PubMed]
- Ravichandran, A.K.; Baran, D.A.; Stelling, K.; Cowger, J.A.; Salerno, C.T. Outcomes with the Tandem Protek Duo Dual-Lumen Percutaneous Right Ventricular Assist Device. ASAIO J. Am. Soc. Artif. Intern. Organs 1992 2018, 64, 570–572. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, B.; Coats, A.J.; Tsutsui, H.; Abdelhamid, M.; Adamopoulos, S.; Albert, N.; Anker, S.D.; Atherton, J.; Böhm, M.; Butler, J.; et al. Universal Definition and Classification of Heart Failure: A Report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure. J. Card. Fail. 2021, 27, 387–413. [Google Scholar] [CrossRef]
- Boyle, A.J.; Ascheim, D.D.; Russo, M.J.; Kormos, R.L.; John, R.; Naka, Y.; Gelijns, A.C.; Hong, K.N.; Teuteberg, J.J. Clinical Outcomes for Continuous-Flow Left Ventricular Assist Device Patients Stratified by Pre-Operative INTERMACS Classification. J. Heart Lung Transplant. Off. Publ. Int. Soc. Heart Transplant. 2011, 30, 402–407. [Google Scholar] [CrossRef]
- Jorde, U.P.; Kushwaha, S.S.; Tatooles, A.J.; Naka, Y.; Bhat, G.; Long, J.W.; Horstmanshof, D.A.; Kormos, R.L.; Teuteberg, J.J.; Slaughter, M.S.; et al. Results of the Destination Therapy Post-Food and Drug Administration Approval Study with a Continuous Flow Left Ventricular Assist Device: A Prospective Study Using the INTERMACS Registry (Interagency Registry for Mechanically Assisted Circulatory Support). J. Am. Coll. Cardiol. 2014, 63, 1751–1757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uriel, N.; Burkhoff, D.; Kim, G.; Silverstein, T.; Juricek, C.; Kaye, D.M.; Sayer, G. Oral Milrinone for the Treatment of Chronic Severe Right Ventricular Failure in Left Ventricular Assist Device Patients. Circ. Heart Fail. 2021, 14, e007286. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Author | Year | Definition | Severity Distinction |
| Early Right Heart Failure | |||
| Matthews et al. [29] | 2008 | Need for IV inotropes >14 days, inhaled nitric oxide ≥48 h, right-sided circulatory support (ECMO or RVAD) or hospital discharge with IV inotrope | |
| Fitzpatrick et al. [30] | 2008 | Need for RVAD support | |
| Kormos et al. [6] | 2010 | Need for RVAD or continuous inotropic support ≥14 days following implantation | |
| Drakos et al. [31] | 2010 | Need for RVAD implantation, inhaled nitric oxide ≥48 h, or need for IV inotropes >14 consecutive days | |
| Wang et al. [32] | 2012 | Need for RVAD support | |
| Atluri et al. [33] | 2013 | Need for RVAD support | |
| INTERMACS [35] | 2014 | Elevated CVP (RAP > 16 mmHg, dilated IVC on echocardiogram, or elevated jugular venous pulse) + manifestations of elevated CVP (peripheral edema, ascites/hepatomegaly, lab evidence of worsening hepatic or renal dysfunction) | Mild: within 7 days Moderate: 7–14 days Severe: >14 days or need for RVAD |
| Soliman et al. [3] | 2018 | Short- or long-term right-sided circulatory support, continuous inotropic support ≥14 days, or inhaled nitric oxide ventilation ≥48 h | Severe |
| Rich et al. [8] | 2017 | RV dysfunction associated with signs/symptoms of RHF * that warrant RVAD, use of inotropes >14 consecutive days, or need to reinitiate inotropes between 14 and 30 days post-implant | |
| Mehra et al. (MOMENTUM 3) [34] | 2019 | Signs/symptoms of persistent RV dysfunction * requiring RVAD, inhaled nitric oxide, or inotropes >7 days anytime following LVAD implantation | |
| Late Right Heart Failure | |||
| Kormos et al. [6] | 2010 | Inotropic support starting >14 days post-implantation | |
| Takeda et al. [10] | 2015 | Right heart failure requiring rehospitalization following index hospitalization in addition to medical/surgical management (i.e., augmented diuretics, inotropes, and RVAD implantation) | |
| Rich et al. [8] | 2017 | RV dysfunction associated with signs/symptoms of RHF * that warrant readmission with initiation of inotropes >30 days following discharge from index hospitalization | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, T.S.; Cevasco, M.; Birati, E.Y.; Mazurek, J.A. Predicting, Recognizing, and Treating Right Heart Failure in Patients Undergoing Durable LVAD Therapy. J. Clin. Med. 2022, 11, 2984. https://doi.org/10.3390/jcm11112984
Wang TS, Cevasco M, Birati EY, Mazurek JA. Predicting, Recognizing, and Treating Right Heart Failure in Patients Undergoing Durable LVAD Therapy. Journal of Clinical Medicine. 2022; 11(11):2984. https://doi.org/10.3390/jcm11112984
Chicago/Turabian StyleWang, Teresa S., Marisa Cevasco, Edo Y. Birati, and Jeremy A. Mazurek. 2022. "Predicting, Recognizing, and Treating Right Heart Failure in Patients Undergoing Durable LVAD Therapy" Journal of Clinical Medicine 11, no. 11: 2984. https://doi.org/10.3390/jcm11112984
APA StyleWang, T. S., Cevasco, M., Birati, E. Y., & Mazurek, J. A. (2022). Predicting, Recognizing, and Treating Right Heart Failure in Patients Undergoing Durable LVAD Therapy. Journal of Clinical Medicine, 11(11), 2984. https://doi.org/10.3390/jcm11112984