
Trends in Sexually Transmitted Infections in United States Ambulatory Care Clinics from 2005–2016

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data
2.2. Measures/Outcomes
2.3. Statistical Analysis
3. Results
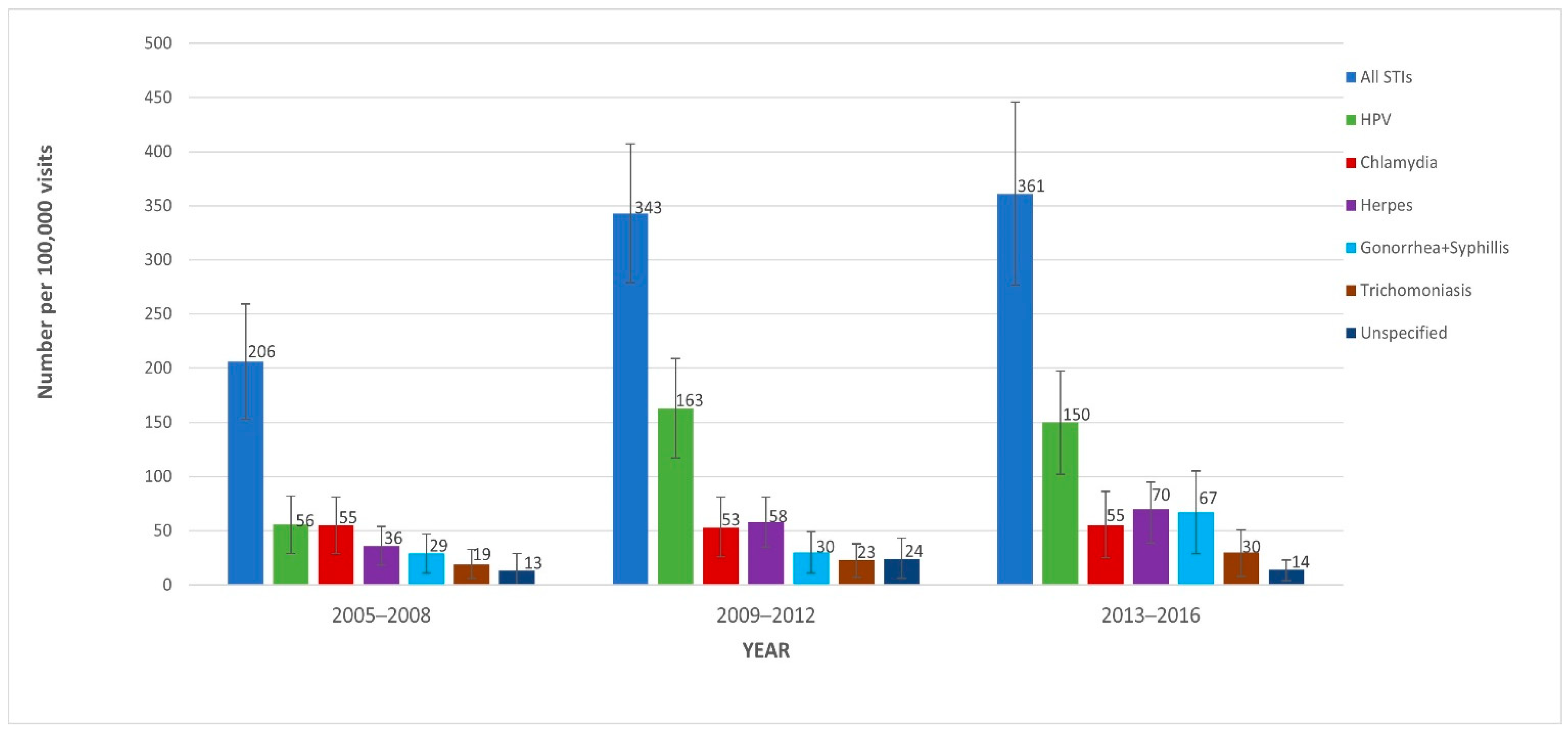
3.1. Trends of Non-HIV STI-Related Visits
3.2. Factors Associated with STI-Related Visits
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kreisel, K.M.; Spicknall, I.H.; Gargano, J.W.; Lewis, F.M.; Lewis, R.M.; Markowitz, L.E.; Roberts, H.; Johnson, A.S.; Song, R.; Cyr, S.B.S.; et al. Sexually Transmitted Infections Among US Women and Men: Prevalence and Incidence Estimates, 2018. Sex. Transm. Dis. 2021, 48, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Braun, D.L.; Marzel, A.; Steffens, D.; Schreiber, P.W.; Grube, C.; Scherrer, A.U.; Kouyos, R.D.; Günthard, H.F.; Anagnostopoulos, A.; Aubert, V.; et al. High Rates of Subsequent Asymptomatic Sexually Transmitted Infections and Risky Sexual Behavior in Patients Initially Presenting with Primary Human Immunodeficiency Virus-1 Infection. Clin. Infect. Dis. 2017, 66, 735–742. [Google Scholar] [CrossRef] [PubMed]
- Bowen, V.B.; Braxton, J.; Davis, D.W.; Flagg, E.W.; Grey, J.; Grier, L.; Harvey, A.; Kidd, S.; Kreisel, K.; Llata, E.; et al. Sexually Transmitted Sisease Surveillance 2018; Department of Health and Human Services: Atlanta, GA, USA, 2019. [CrossRef]
- CDC.gov. STD Facts-Human Papillomavirus (HPV). Available online: https://www.cdc.gov/STD/HPV/STDFACT-hpv.htm (accessed on 25 June 2021).
- Weinstock, H.S.; Kreisel, K.M.; Spicknall, I.H.; Chesson, H.W.; Miller, W.C. STI Prevalence, Incidence, and Costs in the United States: New Estimates, New Approach. Sex. Transm. Dis. 2021, 48, 207. [Google Scholar] [CrossRef] [PubMed]
- Kasting, M.L.; Shapiro, G.; Rosberger, Z.; Kahn, J.A.; Zimet, G.D. Tempest in a teapot: A systematic review of HPV vaccination and risk compensation research. Hum. Vaccines Immunother. 2016, 12, 1435–1450. [Google Scholar] [CrossRef] [Green Version]
- Holt, M.; Murphy, D.A. Individual Versus Community-Level Risk Compensation Following Preexposure Prophylaxis of HIV. Am. J. Public Health 2017, 107, 1568–1571. [Google Scholar] [CrossRef]
- Satterwhite, C.L.; Torrone, E.; Meites, E.; Dunne, E.F.; Mahajan, R.; Ocfemia, M.C.; Su, J.; Xu, F.; Weinstock, H. Sexually transmitted infections among US women and men: Prevalence and incidence estimates, 2008. Sex. Transm. Dis. 2013, 40, 187–193. [Google Scholar] [CrossRef]
- Guidance on Reporting Case Status for STD Case Reports. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/std/program/forms/Guidance-for-Case-Status-Variable_clearance_cleared.pdf (accessed on 9 June 2021).
- NAMCS/NHAMCS-Ambulatory Health Care Data Homepage. Available online: https://www.cdc.gov/nchs/ahcd/index.htm (accessed on 20 October 2020).
- National Center for Health Statistics. Using SAS with NAMCS Data. Available online: https://ftp.cdc.gov/pub/health_statistics/nchs/dataset_documentation/NAMCS/sas/readme2014-sas.txt (accessed on 21 April 2021).
- Healthcare Cost and Utilization Project (HCUP). Clinical Classifications Software (CCS) for ICD-9-CM Diagnoses. Available online: https://www.hcup-us.ahrq.gov/toolssoftware/ccs/ccs.jsp (accessed on 20 October 2020).
- Healthcare Cost and Utilization Project (HCUP). Clinical Classifications Software Refined (CCSR) for ICD-10-CM Diagnoses. Available online: https://www.hcup-us.ahrq.gov/toolssoftware/ccsr/ccs_refined.jsp (accessed on 20 April 2020).
- Understanding and Using NAMCS and NHAMCES Data. Data Tools and Basic Programming Techniques. Available online: https://www.cdc.gov/nchs/ppt/nchs2010/03_hsiao.pdf (accessed on 20 October 2020).
- Ware, C.E.; Ajabnoor, Y.; Mullins, P.M.; Mazer-Amirshahi, M.; Pines, J.M.; May, L. A retrospective cross-sectional study of patients treated in US EDs and ambulatory care clinics with sexually transmitted infections from 2001 to 2010. Am. J. Emerg. Med. 2016, 34, 1808–1811. [Google Scholar] [CrossRef]
- Nayyar, C.; Chander, R.; Gupta, P.; Sherwal, B.L. Evaluation of risk factors in patients attending STI clinic in a tertiary care hospital in North India. Indian J. Sex. Transm. Dis. AIDS 2015, 36, 48–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiv.gov. Who Is at Risk for HIV? Available online: https://www.hiv.gov/hiv-basics/overview/about-hiv-and-aids/who-is-at-risk-for-hiv (accessed on 20 October 2020).
- Peterman, T.A.; Newman, D.R.; Maddox, L.; Schmitt, K.; Shiver, S. High risk for HIV following syphilis diagnosis among men in Florida, 2000-2011. Public Health Rep. 2014, 129, 164–169. [Google Scholar] [CrossRef]
- Newman, D.R.; Rahman, M.M.; Brantley, A.; Peterman, T.A. Rates of New Human Immunodeficiency Virus (HIV) Diagnoses After Reported Sexually Transmitted Infection in Women in Louisiana, 2000–2015: Implications for HIV Prevention. Clin. Infect. Dis. 2020, 70, 1115–1120. [Google Scholar] [CrossRef]
- Barbee, L.A.; Khosropour, C.M.; Dombrowksi, J.C.; Golden, M.R. New Human Immunodeficiency Virus Diagnosis Independently Associated with Rectal Gonorrhea and Chlamydia in Men Who Have Sex with Men. Sex. Transm. Dis. 2017, 44, 385–389. [Google Scholar] [CrossRef]
- Kojima, N.; Davey, D.J.; Klausner, J.D. Pre-exposure prophylaxis for HIV infection and new sexually transmitted infections among men who have sex with men. AIDS 2016, 30, 2251–2252. [Google Scholar] [CrossRef] [PubMed]
- Buchacz, K.; Patel, P.; Taylor, M.; Kerndt, P.R.; Byers, R.H.; Holmberg, S.D.; Klausner, J.D. Syphilis increases HIV viral load and decreases CD4 cell counts in HIV-infected patients with new syphilis infections. AIDS 2004, 18, 2075–2079. [Google Scholar] [CrossRef]
- Cohen, M.S.; Hoffman, I.F.; Royce, R.A.; Kazembe, P.; Dyer, J.R.; Daly, C.C.; Zimba, D.; Vernazza, P.L.; Maida, M.; Fiscus, S.A.; et al. Reduction of concentration of HIV-1 in semen after treatment of urethritis: Implications for prevention of sexual transmission of HIV-1. Lancet 1997, 349, 1868–1873. [Google Scholar] [CrossRef]
- Scott-Sheldon, L.A.J.; Chan, P.A. Increasing Sexually Transmitted Infections in the U.S.: A Call for Action for Research, Clinical, and Public Health Practice. Arch. Sex. Behav. 2020, 49, 13–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Traeger, M.W.; Cornelisse, V.J.; Asselin, J.; Price, B.; Roth, N.J.; Willcox, J.; Tee, B.K.; Fairley, C.K.; Chang, C.C.; Armishaw, J.; et al. Association of HIV Preexposure Prophylaxis with Incidence of Sexually Transmitted Infections Among Individuals at High Risk of HIV Infection. JAMA 2019, 321, 1380–1390. [Google Scholar] [CrossRef] [PubMed]
- Traeger, M.W.; Schroeder, S.E.; Wright, E.J.; Hellard, M.E.; Cornelisse, V.J.; Doyle, J.S.; Stoové, M.A. Effects of Pre-exposure Prophylaxis for the Prevention of Human Immunodeficiency Virus Infection on Sexual Risk Behavior in Men Who Have Sex with Men: A Systematic Review and Meta-analysis. Clin. Infect. Dis. 2018, 67, 676–686. [Google Scholar] [CrossRef] [PubMed]
- Gardasil Vaccine Safety|FDA. Available online: https://www.fda.gov/vaccines-blood-biologics/safety-availability-biologics/gardasil-vaccine-safety (accessed on 17 May 2021).
- Stokley, S.; Jeyarakah, J.; Yankey, D.; Cano, M.; Gee, J.; Roark, J.; Curtis, R.C.; Markowitz, L. Human papillomavirus vaccination coverage among adolescents, 2007-2013, and postlicensure vaccine safety monitoring, 2006–2014—United States. MMWR Morb. Mortal. Wkly. Rep. 2014, 63, 620–624. [Google Scholar] [PubMed]
- Lei, J.; Ploner, A.; Elfström, K.M.; Wang, J.; Roth, A.; Fang, F.; Sundström, K.; Dillner, J.; Sparén, P. HPV Vaccination and the Risk of Invasive Cervical Cancer. N. Engl. J. Med. 2020, 383, 1340–1348. [Google Scholar] [CrossRef] [PubMed]
- Rosenblum, H.G.; Lewis, R.M.; Gargano, J.W.; Querec, T.D.; Unger, E.R.; Markowitz, L.E. Declines in Prevalence of Human Papillomavirus Vaccine-Type Infection Among Females after Introduction of Vaccine-United States, 2003–2018. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 415–420. [Google Scholar] [CrossRef]
- Cancer Trends Progress Report; Cervical Cancer Screening. Available online: https://progressreport.cancer.gov/detection/cervical_cancer (accessed on 15 October 2021).
- Fergus, S.; Zimmerman, M.A.; Caldwell, C.H. Growth trajectories of sexual risk behavior in adolescence and young adulthood. Am. J. Public Health 2007, 97, 1096–1101. [Google Scholar] [CrossRef] [PubMed]
- Garcia, M.R.; Wray, A.A. Sexually Transmitted Infections. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Guaschino, S. Complications of sexually transmitted diseases: Clinical course and treatment. Ann. Ist. Super. Sanita 2000, 36, 431–435. [Google Scholar] [PubMed]
- Sexually Transmitted Disease Surveillance 2019. Available online: https://www.cdc.gov/std/statistics/2019/tables.htm (accessed on 3 October 2021).


{kind=link}
| STI | Diagnosis Codes from HCUP’s CCSR and CCS | |
|---|---|---|
| ICD-9-CM | ICD-10-CM | |
| Chlamydia | 076x, 078.88, 079.98, 079.88, 099.1, 099.41, 099.5x | A55x, A56x, A71x, A74x |
| Gonorrhea | 098x | A54x |
| Syphilis | 090x–097x | A51x–A53x |
| HPV | 078.11, 795.05, 795.09, 795.15, 795.19, 796.75, 796.79 | A63.0, R85.81x, R85.82x, R87.81x, R87.82x |
| Trichomoniasis | 131x | A59x |
| Chancroid | 099.0 | A57x |
| Genital herpes | 054.1x | A60x |
| Unspecified STI | 099.9 | A64 |
| Reiter’s disease | 099.3 | M02.3 |
| Granuloma inguinale | 099.2 | A58 |
| Year (N = Unweighted # of Visits) | 2005–2008 (N = 110) | 2009–2012 (N = 241) | 2013–2016 (N = 246) | p-Value |
|---|---|---|---|---|
| Weighted number of visits | 4,419,914 | 7,604,358 | 7,502,703 | N/A |
| Weighted proportion of visits N% (95% CI:) | ||||
| Age categories | <0.01 | |||
| 15–24 years | 35.3 (24.2–46.5) | 30.0 (22.0–379) | 13.9 (7.7–20.2) | |
| 25–44 years | 36.2 (26.0–45.5) | 50.9 (43.5–58.3) | 65.1 (55.6–74.7) | |
| 45–64 years | 28.4 (17.9–38.9) | 19.1 (13.2–25.0) | 20.9 (12.2–29.6) | |
| Sex | 0.44 | |||
| Female | 74.8 (64.7–84.8) | 64.0 (54.6–73.3) | 56.0 (44.1–68.0) | |
| Male | 25.2 (15.2–35.3) * | 36.0 (26.7–45.4) | 44.0 (32.0–55.9) | |
| Race | 0.03 | |||
| White | 66.9 (55.6–78.1) | 69.6 (60.4–79.3) | 71.3 (61.7–80.9) | |
| Black | 27.0 (15.5–38.5) | 27.4 (18.0–36.8) | 22.1 (13.3–30.8) | |
| Other | 6.1 (0.9–11.4) * | 2.8 (0.4–5.1) * | 6.7 (1.4–11.9) * | |
| Ethnicity | <0.01 | |||
| Hispanic | 13.6 (6.9–20.2) * | 13.6 (7.1–20.2) | 19.9 (11.4–28.3) | |
| Not Hispanic | 86.4 (79.8–93.0) | 86.4 (79.8–92.9) | 80.1 (71.7–88.6) | |
| Insurance | <0.01 | |||
| Private | 68.3 (53.6–83.0) | 62.9 (51.8–74.0) | 60.3 (48.8–71.8) | |
| Medicare/Medicaid | 17.3 (5.0–29.6) | 22.4 (14.2–30.5) | 25.0 (14.4–35.6) | |
| others/missing | 14.3 (3.9–24.7) | 14.7 (5.1–24.3) | 14.7 (6.1–23.3) | |
| Region | 0.37 | |||
| Northeast | 12.8 (5.7–20.0) | 15.3 (9.0–21.7) | 17.3 (7.9–26.7) | |
| Midwest | 19.7 (8.5–30.9) | 13.3 (8.1–18.6) | 19.2 (11.3–27.1) | |
| South | 47.5 (33.3–61.7) | 54.9 (45.5–64.4) | 35.7 (24.6–46.7) | |
| West | 20.0 (10.3–29.6) | 16.4 (10.0–228) | 27.8 (16.0–39.6) | |
| HIV diagnosis | 1.0 (0.0–3.3) * | 3.8 (0.0–8.5) * | 3.7 (0.4–7.0) * | 0.66 |
| Variables | Adjusted Odds-Ratio (95% CI) |
|---|---|
| Year of diagnosis (ref: 2005–2008) | |
| 2009–2012 | 1.66 (1.20–2.30) |
| 2013–2016 | 1.77 (1.26–2.47) |
| Patient age categories (ref: 45–65 years) | |
| 15–24 years | 4.45 (3.19–6.20) |
| 25–44 years | 3.59 (2.71–4.77) |
| Sex (ref: Male) | |
| Female | 0.94 (0.72–1.22) |
| Race (ref: White) | |
| Black | 2.41 (1.78–3.25) |
| Other | 1.08 (0.63–1.84) |
| Patient ethnicity (ref: Non-Hispanic or Latino) | |
| Hispanic or Latino | 1.31 (0.97–1.78) |
| Insurance (ref: Medicaid/Medicare) | |
| Private | 0.87 (0.63–1.19) |
| Others | 0.89 (0.53–1.49) |
| Region (ref: Midwest) | |
| Northeast | 0.93 (0.62–1.38) |
| South | 1.22 (0.90–1.64) |
| West | 1.12 (0.76–1.67) |
| HIV vs. Non-HIV | 10.6 (5.50–20.27) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Unigwe, I.; Yang, S.; Song, H.J.; Lo-Ciganic, W.-H.; Hincapie-Castillo, J.; Cook, R.L.; Park, H. Trends in Sexually Transmitted Infections in United States Ambulatory Care Clinics from 2005–2016. J. Clin. Med. 2022, 11, 71. https://doi.org/10.3390/jcm11010071
Unigwe I, Yang S, Song HJ, Lo-Ciganic W-H, Hincapie-Castillo J, Cook RL, Park H. Trends in Sexually Transmitted Infections in United States Ambulatory Care Clinics from 2005–2016. Journal of Clinical Medicine. 2022; 11(1):71. https://doi.org/10.3390/jcm11010071
Chicago/Turabian StyleUnigwe, Ikenna, Seonkyeong Yang, Hyun Jin Song, Wei-Hsuan Lo-Ciganic, Juan Hincapie-Castillo, Robert L. Cook, and Haesuk Park. 2022. "Trends in Sexually Transmitted Infections in United States Ambulatory Care Clinics from 2005–2016" Journal of Clinical Medicine 11, no. 1: 71. https://doi.org/10.3390/jcm11010071
APA StyleUnigwe, I., Yang, S., Song, H. J., Lo-Ciganic, W.-H., Hincapie-Castillo, J., Cook, R. L., & Park, H. (2022). Trends in Sexually Transmitted Infections in United States Ambulatory Care Clinics from 2005–2016. Journal of Clinical Medicine, 11(1), 71. https://doi.org/10.3390/jcm11010071