
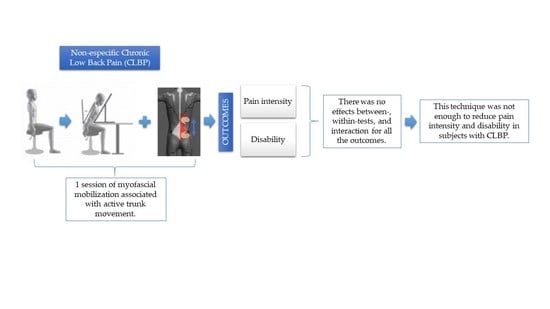
Can a Single Trial of a Thoracolumbar Myofascial Release Technique Reduce Pain and Disability in Chronic Low Back Pain? A Randomized Balanced Crossover Study

 ,
,  ,
,  , ,
, ,  ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Populations
2.3. Sample Size Calculation
2.4. Outcome Measures
2.5. Intervention
2.5.1. Control
2.5.2. Experimental
2.5.3. Placebo
2.6. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Boff, T.A.; Pasinato, F.; Ben, Â.J.; Bosmans, J.E.; van Tulder, M.; Carregaro, R.L. Effectiveness of Spinal Manipulation and Myofascial Release Compared with Spinal Manipulation Alone on Health-Related Outcomes in Individuals with Non-Specific Low Back Pain: Randomized Controlled Trial. Physiotherapy 2020, 107, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Global Burden of Disease Study 2013 Collaborators. Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 301 Acute and Chronic Diseases and Injuries in 188 Countries, 1990–2013: A Systematic Analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 743–800. [Google Scholar] [CrossRef]
- Ajimsha, M.S.; Daniel, B.; Chithra, S. Effectiveness of Myofascial Release in the Management of Chronic Low Back Pain in Nursing Professionals. J. Bodyw. Mov. Ther. 2014, 18, 273–281. [Google Scholar] [CrossRef]
- Arguisuelas, M.D.; Lisón, J.F.; Sánchez-Zuriaga, D.; Martínez-Hurtado, I.; Doménech-Fernández, J. Effects of Myofascial Release in Non-Specific Chronic Low Back Pain: A Randomized Clinical Trial. Spine 2017, 42, 627–634. [Google Scholar] [CrossRef] [PubMed]
- Arguisuelas, M.D.; Lisón, J.F.; Coloma, P.S. Clinical Biomechanics Effects of Myofascial Release in Erector Spinae Myoelectric Activity and Lumbar Spine Kinematics in Non-Specific Chronic Low Back Pain: Randomized. Clin. Biomech. 2019, 63, 27–33. [Google Scholar] [CrossRef]
- Casato, G.; Stecco, C.; Busin, R. Role of Fasciae in Nonspecific Low Back Pain. Eur. J. Transl. Myol. 2019, 29, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Mense, S. Innervation of the Thoracolumbar Fascia. Eur. J. Transl. Myol. 2019, 29, 151–158. [Google Scholar] [CrossRef]
- Schilder, A.; Hoheisel, U.; Magerl, W.; Benrath, J.; Klein, T.; Treede, R.D. Sensory Findings after Stimulation of the Thoracolumbar Fascia with Hypertonic Saline Suggest Its Contribution to Low Back Pain. Pain 2014, 155, 222–231. [Google Scholar] [CrossRef]
- Ajimsha, M.S.; Al-Mudahka, N.R.; Al-Madzhar, J.A. Effectiveness of Myofascial Release: Systematic Review of Randomized Controlled Trials. J. Bodyw. Mov. Ther. 2015, 19, 102–112. [Google Scholar] [CrossRef]
- Akhtar, M.W.; Karimi, H.; Gilani, S.A. Effectiveness of Core Stabilization Exercises and Routine Exercise Therapy in Management of Pain in Chronic Nonspecific Low Back Pain: A Randomized Controlled Clinical Trial. Pak. J. Med. Sci. 2017, 33, 1002–1006. [Google Scholar] [CrossRef]
- Searle, A.; Spink, M.; Ho, A.; Chuter, V. Exercise Interventions for the Treatment of Chronic Low Back Pain: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Clin. Rehabil. 2015, 29, 1155–1167. [Google Scholar] [CrossRef] [PubMed]
- van Middelkoop, M.; Rubinstein, S.M.; Verhagen, A.P.; Ostelo, R.W.; Koes, B.W.; van Tulder, M.W. Exercise Therapy for Chronic Nonspecific Low-Back Pain. Best Pract. Res. Clin. Rheumatol. 2010, 24, 193–204. [Google Scholar] [CrossRef] [PubMed]
- van Middelkoop, M.; Rubinstein, S.M.; Kuijpers, T.; Verhagen, A.P.; Ostelo, R.; Koes, B.W.; van Tulder, M.W. A Systematic Review on the Effectiveness of Physical and Rehabilitation Interventions for Chronic Non-Specific Low Back Pain. Eur. Spine J. 2011, 20, 19–39. [Google Scholar] [CrossRef]
- Wang, X.Q.; Zheng, J.J.; Yu, Z.W.; Bi, X.; Lou, S.J.; Liu, J.; Cai, B.; Hua, Y.H.; Wu, M.; Wei, M.L.; et al. A Meta-Analysis of Core Stability Exercise versus General Exercise for Chronic Low Back Pain. PLoS ONE 2012, 7, e52082. [Google Scholar] [CrossRef]
- Bialosky, J.E.; Bishop, M.D.; Penza, C.W. Placebo Mechanisms of Manual Therapy: A Sheep in Wolf’s Clothing? J. Orthop. Sports Phys. Ther. 2017, 47, 301–304. [Google Scholar] [CrossRef]
- McGlone, F.; Wessberg, J.; Olausson, H. Discriminative and Affective Touch: Sensing and Feeling. Neuron 2014, 82, 737–755. [Google Scholar] [CrossRef]
- Wilke, J.; Schleip, R.; Klingler, W.; Stecco, C. The Lumbodorsal Fascia as a Potential Source of Low Back Pain: A Narrative Review. BioMed Res. Int. 2017, 2017, 5349620. [Google Scholar] [CrossRef]
- Bishop, M.D.; Torres-Cueco, R.; Gay, C.W.; Lluch-Girbés, E.; Beneciuk, J.M.; Bialosky, J.E. What Effect Can Manual Therapy Have on a Patient’s Pain Experience? Pain Manag. 2015, 5, 455–464. [Google Scholar] [CrossRef]
- De Coninck, K.; Hambly, K.; Dickinson, J.W.; Passfield, L. Measuring the Morphological Characteristics of Thoracolumbar Fascia in Ultrasound Images: An Inter-Rater Reliability Study. BMC Musculoskelet. Disord. 2018, 19, 180. [Google Scholar] [CrossRef]
- Krause, F.; Wilke, J.; Vogt, L.; Banzer, W. Intermuscular Force Transmission along Myofascial Chains: A Systematic Review. J. Anat. 2016, 228, 910–918. [Google Scholar] [CrossRef] [PubMed]
- Wilke, J.; Krause, F.; Vogt, L.; Banzer, W. What Is Evidence-Based about Myofascial Chains: A Systematic Review. Arch. Phys. Med. Rehabil. 2016, 97, 454–461. [Google Scholar] [CrossRef]
- Wilke, J.; Niederer, D.; Vogt, L.; Banzer, W. Remote Effects of Lower Limb Stretching: Preliminary Evidence for Myofascial Connectivity? J. Sports Sci. 2016, 34, 2145–2148. [Google Scholar] [CrossRef]
- Bordoni, B.; Marelli, F.; Morabito, B.; Sacconi, B. The Indeterminable Resilience of the Fascial System. J. Integr. Med. 2017, 15, 337–343. [Google Scholar] [CrossRef]
- Langevin, H.M.; Fox, J.R.; Koptiuch, C.; Badger, G.J.; Greenan-Naumann, A.C.; Bouffard, N.A.; Konofagou, E.E.; Lee, W.N.; Triano, J.J.; Henry, S.M. Reduced Thoracolumbar Fascia Shear Strain in Human Chronic Low Back Pain. BMC Musculoskelet. Disord. 2011, 12, 203. [Google Scholar] [CrossRef] [PubMed]
- Findley, T.; Chaudhry, H.; Stecco, A.; Roman, M. Fascia Research—A Narrative Review. J. Bodyw. Mov. Ther. 2012, 16, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Fritz, J.M.; Beneciuk, J.M.; George, S.Z. Relationship between Categorization with the STarT Back Screening Tool and Prognosis for People Receiving Physical Therapy for Low Back Pain. Phys. Ther. 2011, 91, 722–732. [Google Scholar] [CrossRef] [PubMed]
- Lauridsen, H.H.; Hartvigsen, J.; Manniche, C.; Korsholm, L.; Grunnet-Nilsson, N. Responsiveness and Minimal Clinically Important Difference for Pain and Disability Instruments in Low Back Pain Patients. BMC Musculoskelet. Disord. 2006, 7, 82. [Google Scholar] [CrossRef]
- WHO. WHO Guidelines on Physical Activity and Sedentary Behaviour; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Department of Health and Human Services. Executive Summary Physical Activity Guidelines for Americans, 2nd ed.; U.S. Department of Health and Human Services: Washington, DC, USA, 2019; pp. 1–7. [Google Scholar]
- Bhadauria, E.A.; Gurudut, P. Comparative Effectiveness of Lumbar Stabilization, Dynamic Strengthening, and Pilates on Chronic Low Back Pain: Randomized Clinical Trial. J. Exerc. Rehabil. 2017, 13, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Childs, J.D.; Piva, S.R.; Fritz, J.M. Responsiveness of the Numeric Pain Rating Scale in Patients with Low Back Pain. Spine 2005, 30, 1331–1334. [Google Scholar] [CrossRef]
- Antonaci, F.; Sand, T.; Lucas, G.A. Pressure Algometry in Healthy Subjects: Inter-Examiner Variability. Scand. J. Rehabil. Med. 1998, 30, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Pöntinen, P.J. Reliability, Validity, Reproducibility of Algometry in Diagnosis of Active and Latent Tender Spots and Trigger Points. J. Musculoskelet. Pain 1998, 6, 61–71. [Google Scholar] [CrossRef]
- Frank, L.; McLaughlin, P.; Vaughan, B. The Repeatability of Pressure Algometry in Asymptomatic Individuals over Consecutive Days. Int. J. Osteopath. Med. 2013, 16, 143–152. [Google Scholar] [CrossRef]
- Vigatto, R.; Alexandre, N.M.C.; Filho, H.R.C. Development of a Brazilian Portuguese Version of the Oswestry Disability Index. Spine 2007, 32, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Johnsen, L.G.; Hellum, C.; Nygaard, Ø.P.; Storheim, K.; Brox, J.I.; Rossvoll, I.; Leivseth, G.; Grotle, M. Comparison of the SF6D, the EQ5D, and the Oswestry Disability Index in Patients with Chronic Low Back Pain and Degenerative Disc Disease. BMC Musculoskelet. Disord. 2013, 14, 148. [Google Scholar] [CrossRef]
- Saltychev, M.; Mattie, R.; McCormick, Z.; Bärlund, E.; Laimi, K. Psychometric Properties of the Oswestry Disability Index. Int. J. Rehabil. Res. 2017, 40, 202–208. [Google Scholar] [CrossRef]
- Chaitow, L. What’s in a Name: Myofascial Release or Myofascial Induction? J. Bodyw. Mov. Ther. 2017, 21, 749–751. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Jiménez, E.M.; Becerro-de-Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; Rodríguez-Sanz, D.; Díaz-Velázquez, J.I.; Casado-Hernández, I.; Mazoteras-Pardo, V.; López-López, D. Acute Effects of Myofascial Induction Technique in Plantar Fascia Complex in Patients with Myofascial Pain Syndrome on Postural Sway and Plantar Pressures: A Quasi-Experimental Study. Phys. Ther. Sport 2020, 43, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Farrar, J.T.; Young, J.P.; LaMoreaux, L.; Werth, J.L.; Poole, R.M. Clinical Importance of Changes in Chronic Pain Intensity Measured on an 11-Point Numerical Pain Rating Scale. Pain 2001, 94, 149–158. [Google Scholar] [CrossRef]
- Kovacs, F.M.; Abraira, V.; Royuela, A.; Corcoll, J.; Alegre, L.; Cano, A.; Muriel, A.; Zamora, J.; Gil Del Real, M.T.; Gestoso, M.; et al. Minimal Clinically Important Change for Pain Intensity and Disability in Patients with Nonspecific Low Back Pain. Spine 2007, 32, 2915–2920. [Google Scholar] [CrossRef] [PubMed]
- Voogt, L.; de Vries, J.; Meeus, M.; Struyf, F.; Meuffels, D.; Nijs, J. Analgesic Effects of Manual Therapy in Patients with Musculoskeletal Pain: A Systematic Review. Man. Ther. 2015, 20, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Fischer, A.A. Pressure Algometry over Normal Muscles. Standard Values, Validity and Reproducibility of Pressure Threshold. Pain 1987, 30, 115–126. [Google Scholar] [CrossRef]
- Zügel, M.; Maganaris, C.N.; Wilke, J.; Jurkat-Rott, K.; Klingler, W.; Wearing, S.C.; Findley, T.; Barbe, M.F.; Steinacker, J.M.; Vleeming, A.; et al. Fascial Tissue Research in Sports Medicine: From Molecules to Tissue Adaptation, Injury and Diagnostics: Consensus Statement. Br. J. Sports Med. 2018, 52, 1497. [Google Scholar] [CrossRef]
- Magnusson, S.P.; Langberg, H.; Kjaer, M. The Pathogenesis of Tendinopathy: Balancing the Response to Loading. Nat. Rev. Rheumatol. 2010, 6, 262–268. [Google Scholar] [CrossRef]
- Mertens, P.; Blond, S.; David, R.; Rigoard, P. Anatomy, Physiology and Neurobiology of the Nociception: A Focus on Low Back Pain (Part A). Neurochirurgie 2015, 61, S22–S34. [Google Scholar] [CrossRef]
- Puentedura, E.J.; Flynn, T. Combining Manual Therapy with Pain Neuroscience Education in the Treatment of Chronic Low Back Pain: A Narrative Review of the Literature. Physiother. Theory Pract. 2016, 32, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Wallwork, S.B.; Bellan, V.; Catley, M.J.; Moseley, G.L. Neural Representations and the Cortical Body Matrix: Implications for Sports Medicine and Future Directions. Br. J. Sports Med. 2016, 50, 990–996. [Google Scholar] [CrossRef]
- Cholewicki, J.; Breen, A.; Popovich, J.M.; Peter Reeves, N.; Sahrmann, S.A.; Van Dillen, L.R.; Vleeming, A.; Hodges, P.W. Can Biomechanics Research Lead to More Effective Treatment of Low Back Pain? A Point-Counterpoint Debate. J. Orthop. Sports Phys. Ther. 2019, 49, 425–436. [Google Scholar] [CrossRef] [PubMed]
- Bittencourt, N.F.N.; Meeuwisse, W.H.; Mendonça, L.D.; Nettel-Aguirre, A.; Ocarino, J.M.; Fonseca, S.T. Complex Systems Approach for Sports Injuries: Moving from Risk Factor Identification to Injury Pattern Recognition—Narrative Review and New Concept. Br. J. Sports Med. 2016, 50, 1309–1314. [Google Scholar] [CrossRef]
- Huysmans, E.; Ickmans, K.; Van Dyck, D.; Nijs, J.; Gidron, Y.; Roussel, N.; Polli, A.; Moens, M.; Goudman, L.; De Kooning, M. Association Between Symptoms of Central Sensitization and Cognitive Behavioral Factors in People With Chronic Nonspecific Low Back Pain: A Cross-Sectional Study. J. Manip. Physiol. Ther. 2018, 41, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Wiech, K.; Ploner, M.; Tracey, I. Neurocognitive Aspects of Pain Perception. Trends Cogn. Sci. 2008, 12, 306–313. [Google Scholar] [CrossRef]
- Louw, A.; Puentedura, E.J.; Diener, I.; Zimney, K.J.; Cox, T. Pain Neuroscience Education: Which Pain Neuroscience Education Metaphor Worked Best? South. African J. Physiother. 2019, 75, 1329. [Google Scholar] [CrossRef] [PubMed]
- Wood, L.; Hendrick, P.A. A Systematic Review and Meta-Analysis of Pain Neuroscience Education for Chronic Low Back Pain: Short-and Long-Term Outcomes of Pain and Disability. Eur. J. Pain 2019, 23, 234–249. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Characteristics | Subjects (n = 41) Mean (95% CI *) or % |
|---|---|
| Age (years) | 36 (22–50) |
| Gender, women (%) | 60.98 |
| Sedentary (%) | 56.09 |
| NRPS 1 baseline (0–10) | 3.68 (1.39–5.97) |
| PPT 2 (N/cm2) | 34 (16.57–51.43) |
| FTF 3 (cm) | 13 (2–24) |
SBST 4—prognosis (%)
| 56.1 24.4 19.5 |
| Outcomes | Control Mean (95% CI) | Placebo Mean (95% CI) | Experimental Mean (95% CI) | Between-Tests | Within-Tests | Interaction | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| p | F | η2 | Power | p | F | η2 | Power | p | F | η2 | Power | ||||
| PPT (N/cm2) PT | 37.25 (32.63–41.86) | 29.37 (23.93–34.81) | 30.38 (24.70–36.06) | 0.40 | 0.90 | 0.47 | 0.99 | 0.56 | 0.34 | 0.25 | 0.90 | 0.06 | 2.80 | 0.73 | 1.00 |
| PPT (N/cm2) FU | 36.11 (30.90–41.31) | 31.82 (26.12–37.52) | 34.66 (28.01–41.32) | ||||||||||||
| NPRS (score) PT | 3.41 (2.69–4.12) | 3.80 (3.06–4.53) | 3.00 (2.30–3.69) | 0.06 | 2.79 | 0.73 | 1.00 | 0.80 | 0.06 | 0.05 | 0.25 | 0.61 | 0.48 | 0.32 | 0.97 |
| NPRS (score) FU | 3.43 (2.76–4.09) | 3.48 (2.73–4.22) | 3.14 (2.38–3.89) | ||||||||||||
| ODI (%) PT | 15.82 (12.91–18.74) | 17.51(14.42–20.59) | 19.26 (16.29–22.23) | 0.007 | 5.01 | 0.83 | 1.00 | 0.73 | 0.11 | 0.07 | 0.31 | 0.97 | 0.02 | 0.02 | 0.11 |
| ODI (%) FU | 18.04 (15.00–21.09) | 17.70 (14.65–20.76) | 19.29 (16.22–22.36) | ||||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paulo, L.R.; Lacerda, A.C.R.; Martins, F.L.M.; Fernandes, J.S.C.; Vieira, L.S.; Guimarães, C.Q.; Ballesteros, S.d.S.G.; Anjos, M.T.S.d.; Tavares, P.A.; Fonseca, S.F.d.; et al. Can a Single Trial of a Thoracolumbar Myofascial Release Technique Reduce Pain and Disability in Chronic Low Back Pain? A Randomized Balanced Crossover Study. J. Clin. Med. 2021, 10, 2006. https://doi.org/10.3390/jcm10092006
Paulo LR, Lacerda ACR, Martins FLM, Fernandes JSC, Vieira LS, Guimarães CQ, Ballesteros SdSG, Anjos MTSd, Tavares PA, Fonseca SFd, et al. Can a Single Trial of a Thoracolumbar Myofascial Release Technique Reduce Pain and Disability in Chronic Low Back Pain? A Randomized Balanced Crossover Study. Journal of Clinical Medicine. 2021; 10(9):2006. https://doi.org/10.3390/jcm10092006
Chicago/Turabian StylePaulo, Luana Rocha, Ana Cristina Rodrigues Lacerda, Fábio Luiz Mendonça Martins, José Sebastião Cunha Fernandes, Leonardo Sette Vieira, Cristiano Queiroz Guimarães, Sílvia de Simoni Guedes Ballesteros, Marco Túlio Saldanha dos Anjos, Patrícia Aparecida Tavares, Sueli Ferreira da Fonseca, and et al. 2021. "Can a Single Trial of a Thoracolumbar Myofascial Release Technique Reduce Pain and Disability in Chronic Low Back Pain? A Randomized Balanced Crossover Study" Journal of Clinical Medicine 10, no. 9: 2006. https://doi.org/10.3390/jcm10092006
APA StylePaulo, L. R., Lacerda, A. C. R., Martins, F. L. M., Fernandes, J. S. C., Vieira, L. S., Guimarães, C. Q., Ballesteros, S. d. S. G., Anjos, M. T. S. d., Tavares, P. A., Fonseca, S. F. d., Oliveira, M. X., Bernardo-Filho, M., Sá-Caputo, D. d. C. d., Mendonça, V. A., & Taiar, R. (2021). Can a Single Trial of a Thoracolumbar Myofascial Release Technique Reduce Pain and Disability in Chronic Low Back Pain? A Randomized Balanced Crossover Study. Journal of Clinical Medicine, 10(9), 2006. https://doi.org/10.3390/jcm10092006