
Virtual Therapeutic Garden: A Promising Method Supporting the Treatment of Depressive Symptoms in Late-Life: A Randomized Pilot Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Overview
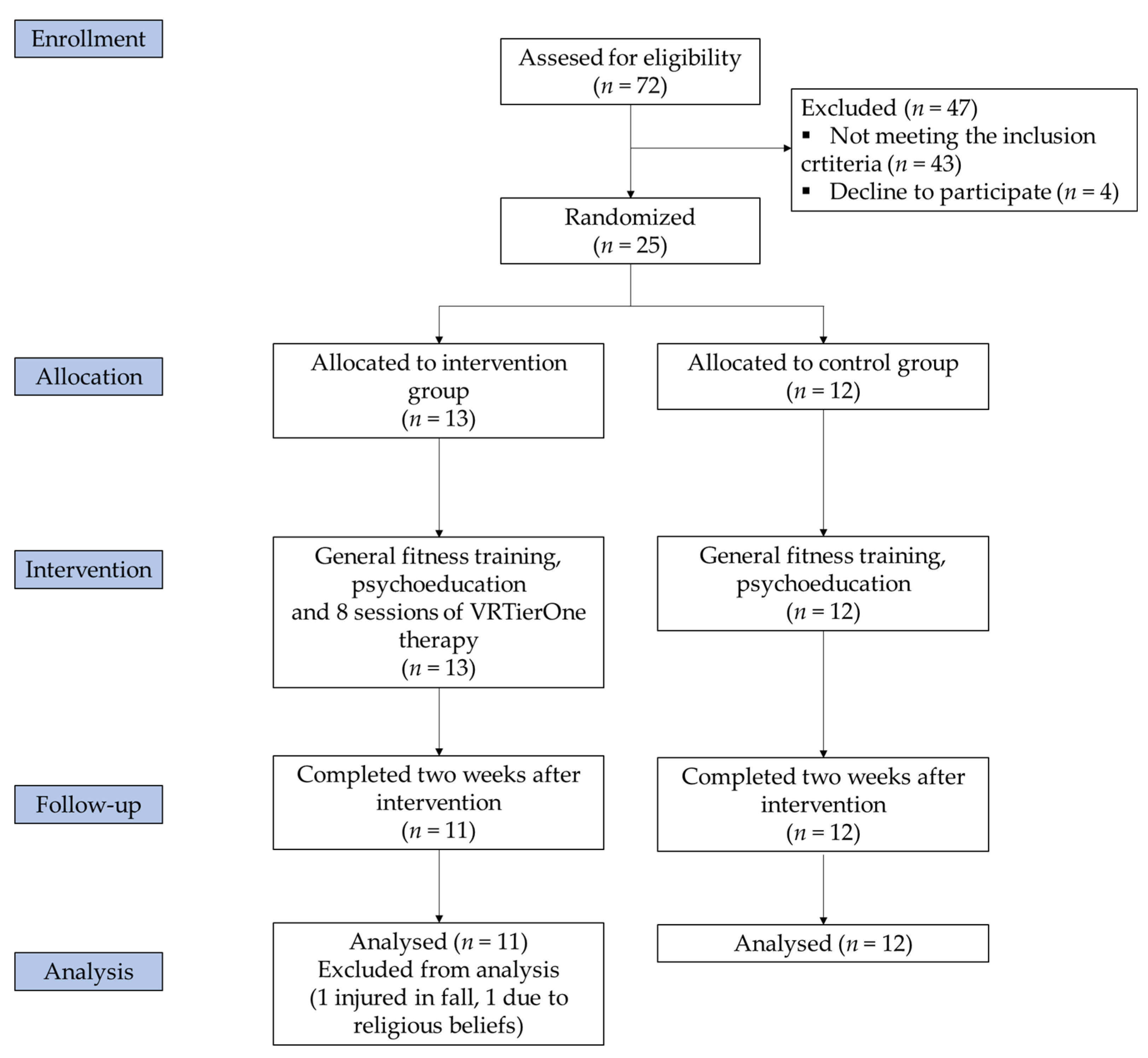
2.2. Participants
2.3. Outcome Measures
2.4. Interventions
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Luppa, M.; Sikorski, C.; Luck, T.; Ehreke, L.; Konnopka, A.; Wiese, B.; Weyerer, S.; König, H.-H.; Riedel-Heller, S.G. Age- and Gender-Specific Prevalence of Depression in Latest-Life—Systematic Review and Meta-Analysis. J. Affect Disord. 2012, 136, 212–221. [Google Scholar] [CrossRef]
- Anstey, K.J.; von Sanden, C.; Sargent-Cox, K.; Luszcz, M.A. Prevalence and Risk Factors for Depression in a Longitudinal, Population-Based Study Including Individuals in the Community and Residential Care. Am. J. Geriatr. Psychiatry 2007, 15, 497–505. [Google Scholar] [CrossRef]
- Verhaak, P.F.M.; Dekker, J.H.; de Waal, M.W.M.; van Marwijk, H.W.J.; Comijs, H.C. Depression, Disability and Somatic Diseases among Elderly. J. Affect Disord. 2014, 167, 187–191. [Google Scholar] [CrossRef]
- Schaakxs, R.; Comijs, H.C.; Lamers, F.; Kok, R.M.; Beekman, A.T.F.; Penninx, B.W.J.H. Associations between Age and the Course of Major Depressive Disorder: A 2-Year Longitudinal Cohort Study. Lancet Psychiatry 2018, 5, 581–590. [Google Scholar] [CrossRef]
- Morga, P.; Cieślik, B.; Sekułowicz, M.; Bujnowska-Fedak, M.; Drower, I.; Szczepańska-Gieracha, J. Low-Intensity Exercise as a Modifier of Depressive Symptoms and Self-Perceived Stress Level in Women with Metabolic Syndrome. J. Sports Sci. Med. 2021, 20, 221–226. [Google Scholar]
- Szczepańska-Gieracha, J.; Mazurek, J.; Serweta, A.; Boroń-Krupińska, K.; Kowalska, J.; Skrzek, A. Effectiveness Assessment of a Therapeutic Programme for Women with Overweight and Obesity: A Biopsychosocial Perspective. Fam. Med. Prim. Care Rev. 2019, 21, 381–386. [Google Scholar] [CrossRef]
- Fodor, L.A.; Coteț, C.D.; Cuijpers, P.; Szamoskozi, Ș.; David, D.; Cristea, I.A. The Effectiveness of Virtual Reality Based Interventions for Symptoms of Anxiety and Depression: A Meta-Analysis. Sci. Rep. 2018, 8, 10323. [Google Scholar] [CrossRef]
- Cieślik, B.; Mazurek, J.; Rutkowski, S.; Kiper, P.; Turolla, A.; Szczepańska-Gieracha, J. Virtual Reality in Psychiatric Disorders: A Systematic Review of Reviews. Complementary Ther. Med. 2020, 52, 102480. [Google Scholar] [CrossRef]
- Szczepańska-Gieracha, J.; Cieślik, B.; Rutkowski, S.; Kiper, P.; Turolla, A. What Can Virtual Reality Offer to Stroke Patients? A Narrative Review of the Literature. NeuroRehabilitation 2020, 47, 109–120. [Google Scholar] [CrossRef]
- Rutkowski, S.; Kiper, P.; Cacciante, L.; Cieślik, B.; Mazurek, J.; Turolla, A.; Szczepańska-Gieracha, J. Use of Virtual Reality-Based Training in Different Fields of Rehabilitation: A Systematic Review and Meta-Analysis. J. Rehabil. Med. 2020, 52, jrm00121. [Google Scholar] [CrossRef]
- Rutkowski, S. Management Challenges in Chronic Obstructive Pulmonary Disease in the COVID-19 Pandemic: Telehealth and Virtual Reality. J. Clin. Med. 2021, 10, 1261. [Google Scholar] [CrossRef] [PubMed]
- Askay, S.W.; Patterson, D.R.; Sharar, S.R. VIRTUAL REALITY HYPNOSIS. Contemp. Hypn. 2009, 26, 40–47. [Google Scholar] [CrossRef]
- Patterson, D.R.; Tininenko, J.R.; Schmidt, A.E.; Sharar, S.R. Virtual Reality Hypnosis: A Case Report. Int. J. Clin. Exp. Hypn. 2004, 52, 27–38. [Google Scholar] [CrossRef]
- Patterson, D.R.; Wiechman, S.A.; Jensen, M.; Sharar, S.R. Hypnosis Delivered through Immersive Virtual Reality for Burn Pain: A Clinical Case Series. Int. J. Clin. Exp. Hypn. 2006, 54, 130–142. [Google Scholar] [CrossRef]
- Austin, D.W.; Abbott, J.-A.M.; Carbis, C. The Use of Virtual Reality Hypnosis with Two Cases of Autism Spectrum Disorder: A Feasibility Study. Contemp. Hypn. 2008, 25, 102–109. [Google Scholar] [CrossRef]
- Gruzelier, J. Theta Synchronisation of Hippocampal and Long Distance Circuitry in the Brain: Implications for EEG-Neurofeedback and Hypnosis in the Treatment of PTSD; NATO Security through Science Series—E: Human and Societal Dynamics: Amsterdam, The Netherlands, 2006. [Google Scholar]
- Thompson, T.; Steffert, T.; Steed, A.; Gruzelier, J. A Randomized Controlled Trial of the Effects of Hypnosis with 3-D Virtual Reality Animation on Tiredness, Mood, and Salivary Cortisol. Int. J. Clin. Exp. Hypn. 2011, 59, 122–142. [Google Scholar] [CrossRef]
- Lynn, S.J.; Neufeld, V.; Maré, C. Direct Versus Indirect Suggestions: A Conceptual and Methodological Review. International Int. J. Clin. Exp. Hypn. 1993, 41, 124–152. [Google Scholar] [CrossRef] [PubMed]
- Lynn, S.J.; Sherman, S.J. The Clinical Importance of Sociocognitive Models of Hypnosis: Response Set Theory and Milton Erickson’s Strategic Interventions. Am. J. Clin. Hypn. 2000, 42, 294–315. [Google Scholar] [CrossRef]
- Short, D. Conversational Hypnosis: Conceptual and Technical Differences Relative to Traditional Hypnosis. Am. J. Clin. Hypn. 2018, 61, 125–139. [Google Scholar] [CrossRef] [PubMed]
- Matthews, W.J. Ericksonian Approaches to Hypnosis and Therapy: Where Are We Now? Int. J. Clin. Exp. Hypn. 2000, 48, 418–426; discussion 433–437. [Google Scholar] [CrossRef]
- Moss, D. The Most Beautiful Man: An Integration of Hypnosis and Biofeedback for Depression and Dissociation. Am. J. Clin. Hypn. 2019, 61, 322–334. [Google Scholar] [CrossRef]
- Larkin, D.M. Principles of Therapeutic Suggestions (Part I) and Clinical Applications of Therapeutic Suggestions (Part II). Explore N. Y. 2014, 10, 380–388. [Google Scholar] [CrossRef]
- Riva, G.; Baños, R.M.; Botella, C.; Wiederhold, B.K.; Gaggioli, A. Positive Technology: Using Interactive Technologies to Promote Positive Functioning. Cyberpsychology Behav. Soc. Netw. 2012, 15, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Gaggioli, A.; Villani, D.; Serino, S.; Banos, R.; Botella, C. Editorial: Positive Technology: Designing E-Experiences for Positive Change. Front. Psychol. 2019, 10. [Google Scholar] [CrossRef]
- Botella, C.; Riva, G.; Gaggioli, A.; Wiederhold, B.K.; Alcaniz, M.; Baños, R.M. The Present and Future of Positive Technologies. Cyberpsychology Behav. Soc. Netw. 2012, 15, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Julious, S.A. Sample Size of 12 per Group Rule of Thumb for a Pilot Study. Pharm. Stat. 2005, 4, 287–291. [Google Scholar] [CrossRef]
- Whitehead, A.L.; Julious, S.A.; Cooper, C.L.; Campbell, M.J. Estimating the Sample Size for a Pilot Randomised Trial to Minimise the Overall Trial Sample Size for the External Pilot and Main Trial for a Continuous Outcome Variable. Stat. Methods Med. Res. 2016, 25, 1057–1073. [Google Scholar] [CrossRef]
- Birckhead, B.; Khalil, C.; Liu, X.; Conovitz, S.; Rizzo, A.; Danovitch, I.; Bullock, K.; Spiegel, B. Recommendations for Methodology of Virtual Reality Clinical Trials in Health Care by an International Working Group: Iterative Study. JMIR Ment. Health 2019, 6, e11973. [Google Scholar] [CrossRef]
- Lopez, M.N.; Quan, N.M.; Carvajal, P.M. A Psychometric Study of the Geriatric Depression Scale. Eur. J. Psychol. Assess. 2010, 26, 55–60. [Google Scholar] [CrossRef]
- Plopa, M.; Makarowski, R. The Perception of Stress Questionnaire. Manual; Vizja Press & IT: Warsaw, Poland, 2010; ISBN 978-83-61086-79-6. [Google Scholar]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatry Scand 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The Validity of the Hospital Anxiety and Depression Scale. An Updated Literature Review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Smarr, K.L.; Keefer, A.L. Measures of Depression and Depressive Symptoms: Beck Depression Inventory-II (BDI-II), Center for Epidemiologic Studies Depression Scale (CES-D), Geriatric Depression Scale (GDS), Hospital Anxiety and Depression Scale (HADS), and Patient Health Questionnaire-9 (PHQ-9). Arthritis Care Res. 2011, 63, S454–S466. [Google Scholar] [CrossRef]
- Szczepańska-Gieracha, J.; Mazurek, J. The Role of Self-Efficacy in the Recovery Process of Stroke Survivors. Psychol. Res. Behav. Manag. 2020, 13, 897–906. [Google Scholar] [CrossRef] [PubMed]
- Levine, J.L.; Kurtz, R.M.; Lauter, J.L. Hypnosis and Its Effects on Left and Right Hemisphere Activity. Biol. Psychiatry 1984, 19, 1461–1475. [Google Scholar] [PubMed]
- Gabel, S. The Right Hemisphere in Imagery, Hypnosis, Rapid Eye Movement Sleep and Dreaming. Empirical Studies and Tentative Conclusions. J. Nerv. Ment. Dis. 1988, 176, 323–331. [Google Scholar] [CrossRef]
- Ahlskog, G. Clinical Hypnosis Today. Psychoanal. Rev. 2018, 105, 425–437. [Google Scholar] [CrossRef] [PubMed]
- Gruzelier, J.H. A Review of the Impact of Hypnosis, Relaxation, Guided Imagery and Individual Differences on Aspects of Immunity and Health. Stress 2002, 5, 147–163. [Google Scholar] [CrossRef]
- Szczepańska-Gieracha, J.; Jóźwik, S.; Cieślik, B.; Mazurek, J.; Gajda, R. Immersive Virtual Reality Therapy as a Support for Cardiac Rehabilitation: A Pilot Randomised Controlled Trial. Cyberpsychol. Behav. Soc. Netw. 2021. [Google Scholar] [CrossRef]
- Rutkowski, S.; Szczegielniak, J.; Szczepańska-Gieracha, J. Evaluation of the Efficacy of Immersive Virtual Reality Therapy as a Method Supporting Pulmonary Rehabilitation: A Randomized Controlled Trial. J. Clin. Med. 2021, 10, 352. [Google Scholar] [CrossRef]
- Li, J.; Theng, Y.-L.; Foo, S. Game-Based Digital Interventions for Depression Therapy: A Systematic Review and Meta-Analysis. Cyberpsychol. Behav. Soc. Netw. 2014, 17, 519–527. [Google Scholar] [CrossRef]
- Gamito, P.; Oliveira, J.; Rosa, P.; Morais, D.; Duarte, N.; Oliveira, S.; Saraiva, T. PTSD Elderly War Veterans: A Clinical Controlled Pilot Study. Cyberpsychol. Behav. Soc. Netw. 2010, 13, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, D.; Depp, C.A.; Vahia, I.V.; Reichstadt, J.; Palmer, B.W.; Kerr, J.; Norman, G.; Jeste, D.V. Exergames for Subsyndromal Depression in Older Adults: A Pilot Study of a Novel Intervention. Am. J. Geriatr. Psychiatry 2010, 18, 221–226. [Google Scholar] [CrossRef]
- Rendon, A.A.; Lohman, E.B.; Thorpe, D.; Johnson, E.G.; Medina, E.; Bradley, B. The Effect of Virtual Reality Gaming on Dynamic Balance in Older Adults. Age Ageing 2012, 41, 549–552. [Google Scholar] [CrossRef] [PubMed]
- Zeng, N.; Pope, Z.; Lee, J.E.; Gao, Z. Virtual Reality Exercise for Anxiety and Depression: A Preliminary Review of Current Research in an Emerging Field. J. Clin. Med. 2018, 7, 42. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Son, J.; Kim, J.; Yoon, B. Individualized Feedback-Based Virtual Reality Exercise Improves Older Women’s Self-Perceived Health: A Randomized Controlled Trial. Arch Gerontol. Geriatr. 2015, 61, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Monteiro-Junior, R.S.; Figueiredo, L.F.S.; Maciel-Pinheiro, P.T.; Abud, E.L.R.; Engedal, K.; Barca, M.L.; Nascimento, O.J.M.; Laks, J.; Deslandes, A.C. Virtual Reality-Based Physical Exercise With Exergames (PhysEx) Improves Mental and Physical Health of Institutionalized Older Adults. J. Am. Med. Dir. Assoc. 2017, 18, 454.e1–454.e9. [Google Scholar] [CrossRef]
- Baños, R.M.; Etchemendy, E.; Castilla, D.; García-Palacios, A.; Quero, S.; Botella, C. Positive Mood Induction Procedures for Virtual Environments Designed for Elderly People. Interact. Comput. 2012, 24, 131–138. [Google Scholar] [CrossRef]
- Riva, G.; Bernardelli, L.; Browning, M.H.E.M.; Castelnuovo, G.; Cavedoni, S.; Chirico, A.; Cipresso, P.; de Paula, D.M.B.; Di Lernia, D.; Fernández-Álvarez, J.; et al. COVID Feel Good—An Easy Self-Help Virtual Reality Protocol to Overcome the Psychological Burden of Coronavirus. Front. Psychiatry 2020, 11, 996. [Google Scholar] [CrossRef]
- Riva, G.; Bernardelli, L.; Castelnuovo, G.; Clementi, A.; Lernia, D.D.; Pedroli, E.; Malighetti, C.; Sforza, F.; Wiederhold, B.K.; Serino, S. A Free Weekly Self-Administered at-Home Virtual Reality Based Protocol for Overcoming the Psychological Burden of Coronavirus: A Pragmatic Waitlist-Controlled Trial Conducted During COVID-19 Lockdown in Italy with 2-Week Follow-Up. 2021. Available online: https://doi.org/10.31234/osf.io/ekz2u (accessed on 29 April 2021).
- Shah, L.B.I.; Torres, S.; Kannusamy, P.; Chng, C.M.L.; He, H.-G.; Klainin-Yobas, P. Efficacy of the Virtual Reality-Based Stress Management Program on Stress-Related Variables in People with Mood Disorders: The Feasibility Study. Arch. Psychiatry Nurs. 2015, 29, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Haro, M.V.; Modrego-Alarcón, M.; Hoffman, H.G.; López-Montoyo, A.; Navarro-Gil, M.; Montero-Marin, J.; García-Palacios, A.; Borao, L.; García-Campayo, J. Evaluation of a Mindfulness-Based Intervention With and Without Virtual Reality Dialectical Behavior Therapy® Mindfulness Skills Training for the Treatment of Generalized Anxiety Disorder in Primary Care: A Pilot Study. Front Psychol. 2019, 10, 55. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Overall (n = 23) | VR (n = 11) | Control (n = 12) | p-Value |
|---|---|---|---|---|
| Age, years | 70.73 (4.56) | 70.18 (4.87) | 71.25 (4.41) | 0.59 a |
| Body mass, kg | 73.14 (13.68) | 74.11 (10.46) | 72.25 (16.53) | 0.75 a |
| Height, cm | 160.04 (6.95) | 160.91 (8.44) | 159.25 (5.51) | 0.58 a |
| BMI, kg/cm2 | 28.47 (4.50) | 28.67 (3.74) | 28.29 (5.26) | 0.59 a |
| Normal (BMI 18.5–24.9), n (%) | 6 (26.09) | 2 (18.18) | 4 (33.33) | 0.41 b |
| Overweight (BMI 25–29.9), n (%) | 9 (39.13) | 5 (45.45) | 4 (33.33) | 0.55 b |
| Obese (BMI > 30), n (%) | 8 (34.78) | 4 (36.36) | 4 (33.33) | 0.88 b |
| Total cholesterol, mg/dL | 196.91 (42.78) | 201.18 (46.71) | 193.00 (40.52) | 0.66 a |
| HDL-C, mg/dL | 68.82 (16.85) | 67.27 (19.02) | 70.25 (15.30) | 0.68 a |
| LDL-C, mg/dL | 118.78 (33.46) | 125.90 (35.56) | 112.25 (31.50) | 0.34 a |
| Triglycerides, mg/dL | 116.00 (48.18) | 114.90 (36.46) | 117.00 (58.59) | 0.92 a |
| Fasting glucose, mg/dL | 103.61 (13.12) | 105.36 (16.56) | 102.01 (9.44) | 0.55 a |
| Resting SBP, mm Hg | 131.82 (13.87) | 133.27 (14.99) | 130.50 (13.28) | 0.64 a |
| Resting DBP, mm Hg | 74.86 (8.20) | 74.45 (8.10) | 75.25 (8.63) | 0.82 a |
| GDS | 12.26 (4.39) | 12.27 (4.45) | 12.25 (4.53) | 0.99 a |
| Current smoking, n (%) | 2 (8.69) | 1 (9.09) | 1 (8.33) | 0.95 b |
| Back pain, n (%) | 18 (78.26) | 8 (72.72) | 10 (83.33) | 0.54 b |
| Joints pain, n (%) | 21 (91.30) | 10 (90.90) | 11 (91.66) | 0.95 b |
| Other pain, n (%) | 13 (56.52) | 6 (54.54) | 7 (58.33) | 0.85 b |
| Marital status, married/single/widow (%) | 11/3/9 | 5/2/4 | 6/1/5 | 0.78 b |
| Education, low/medium/high (%) | 5/10/8 | 3/4/4 | 2/6/4 | 0.76 b |
| VR | Control | |||||||
|---|---|---|---|---|---|---|---|---|
| Pre-Intervention (n = 11) | Post-Intervention (n = 11) | After 2 Weeks (n = 11) | p-Value | Pre-Intervention (n = 12) | Post-Intervention (n = 12) | After 2-Weeks (n = 12) | p-Value | |
| GDS | 12.27 (4.45) | 8.27 * (3.60) | 7.27 * (2.57) | <0.001 | 12.25 (4.53) | 12.75 (4.82) | 11.83 (2.62) | 0.61 |
| Stress level | 61.45 (8.94) | 52.27 * (9.08) | 46.27 * (10.62) | <0.001 | 62.50 (9.53) | 63.50 (10.37) | 64.75 (11.46) | 0.38 |
| Emotional tension | 21.90 (4.67) | 20.09 (5.52) | 17.45 * (5.75) | 0.006 | 20.75 (2.70) | 21.25 (3.91) | 21.91 (4.27) | 0.36 |
| External stress | 19.36 (4.90) | 14.09 * (5.35 | 13.18 * (5.99) | <0.001 | 20.66 (4.29) | 20.91 (3.72) | 21.16 (4.74) | 0.74 |
| Intrapsychic stress | 20.18 (3.81) | 18.09 (2.11) | 15.63 * (3.23) | 0.003 | 21.08 (5.50) | 21.33 (4.18) | 21.66 (4.35) | 0.77 |
| HADS | 17.27 (5.36) | 13.00 * (3.25) | 11.27 * (3.13) | <0.001 | 17.66 (4.83) | 18.16 (4.52) | 18.00 (3.74) | 0.82 |
| HADS-Anxiety | 10.18 (3.78) | 7.36 * (2.33) | 5.81 * (2.60) | <0.001 | 9.83 (2.97) | 10.00 (2.69) | 10.41 (2.84) | 0.48 |
| HADS-Depression | 7.09 (2.02) | 5.63 (2.29) | 5.45 (2.33) | 0.07 | 7.83 (2.32) | 8.16 (2.51) | 7.58 (2.06) | 0.55 |
| VR (n = 11) | Control (n = 12) | MS | F | p | ƞp2 | |
|---|---|---|---|---|---|---|
| GDS | ||||||
| Pre vs. post | 4.00 (1.11–6.89); p = 0.001 | −0.50 (−3.27–2.27); p = 0.73 | ||||
| Pre vs. follow-up | 5.00 (2.11–7.89); p < 0.001 | 0.42 (−2.35–3.19); p = 0.41 | ||||
| Time * group | 39.47 | 8.31 | <0.001 | 0.28 | ||
| Stress level | ||||||
| Pre vs. post | 9.18 (2.65–15.71); p = 0.001 | −1.00 (−7.25–5.25); p = 0.59 | ||||
| Pre vs. follow-up | 15.18 (8.65–21.71); p < 0.001 | −2.25 (−8.50–4.00); p = 0.33 | ||||
| Time * group | 440.10 | 18.18 | <0.001 | 0.46 | ||
| Emotional tension | ||||||
| Pre vs. post | 1.82 (−1.42–5.06); p = 0.99 | −0.50 (−3.60–2.60); p = 0.94 | ||||
| Pre vs. follow-up | 4.45 (1.21–7.70); p = 0.001 | −1.17 (−4.27–1.94); p = 0.92 | ||||
| Time * group | 45.80 | 7.67 | 0.001 | 0.27 | ||
| External stress | ||||||
| Pre vs. post | 5.27 (2.16–8.39); p < 0.001 | −0.25 (−3.23–2.73); p = 0.98 | ||||
| Pre vs. follow-up | 6.18 (3.07–9.30); p < 0.001 | −0.50 (−3.48–2.48); p = 0.87 | ||||
| Time * group | 73.17 | 13.28 | <0.001 | 0.39 | ||
| Intrapsychic stress | ||||||
| Pre vs. post | 2.09 (−0.98–5.17); p = 0.60 | −0.25 (−3.19–2.69); p = 0.78 | ||||
| Pre vs. follow-up | 4.55 (1.47–7.62); p < 0.001 | −0.58 (−3.53–2.36); p = 0.54 | ||||
| Time * group | 37.84 | 7.05 | 0.002 | 0.25 | ||
| HADS | ||||||
| Pre vs. post | 4.27 (1.16–7.39); p = 0.001 | −0.50 (−3.48–2.48); p = 0.32 | ||||
| Pre vs. follow-up | 6.00 (2.89–9.11); p < 0.001 | −0.33 (−3.31–2.65); p = 0.75 | ||||
| Time * group | 62.49 | 11.35 | <0.001 | 0.35 | ||
| HADS-Anxiety | ||||||
| Pre vs. post | 2.82 (0.64–5.00); p = 0.003 | −0.17 (−2.26–1.92); p = 0.79 | ||||
| Pre vs. follow-up | 4.36 (2.18–6.55); p < 0.001 | −0.58 (−2.67–1.51); p = 0.54 | ||||
| Time * group | 35.61 | 13.18 | <0.001 | 0.39 | ||
| HADS-Depression | ||||||
| Pre vs. post | 1.45 (−0.32–3.23); p = 0.22 | −0.33 (−2.03–1.36); p = 0.87 | ||||
| Pre vs. follow-up | 1.64 (−0.18–3.41); p = 0.10 | 0.25 (−1.45–1.95); p = 0.85 | ||||
| Time * group | 5.05 | 2.83 | 0.070 | 0.12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szczepańska-Gieracha, J.; Cieślik, B.; Serweta, A.; Klajs, K. Virtual Therapeutic Garden: A Promising Method Supporting the Treatment of Depressive Symptoms in Late-Life: A Randomized Pilot Study. J. Clin. Med. 2021, 10, 1942. https://doi.org/10.3390/jcm10091942
Szczepańska-Gieracha J, Cieślik B, Serweta A, Klajs K. Virtual Therapeutic Garden: A Promising Method Supporting the Treatment of Depressive Symptoms in Late-Life: A Randomized Pilot Study. Journal of Clinical Medicine. 2021; 10(9):1942. https://doi.org/10.3390/jcm10091942
Chicago/Turabian StyleSzczepańska-Gieracha, Joanna, Błażej Cieślik, Anna Serweta, and Krzysztof Klajs. 2021. "Virtual Therapeutic Garden: A Promising Method Supporting the Treatment of Depressive Symptoms in Late-Life: A Randomized Pilot Study" Journal of Clinical Medicine 10, no. 9: 1942. https://doi.org/10.3390/jcm10091942
APA StyleSzczepańska-Gieracha, J., Cieślik, B., Serweta, A., & Klajs, K. (2021). Virtual Therapeutic Garden: A Promising Method Supporting the Treatment of Depressive Symptoms in Late-Life: A Randomized Pilot Study. Journal of Clinical Medicine, 10(9), 1942. https://doi.org/10.3390/jcm10091942