
The Role of Soluble Low-Density Lipoprotein Receptor-Related Protein-1 in Obstructive Sleep Apnoea


 ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Subjects
2.2. Sleep Studies
2.3. Biomarker Measurements
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Plasma sLRP-1 Levels between Control and OSA Groups
3.3. Association between Circulating sLRP-1 Levels and Clinical Variables
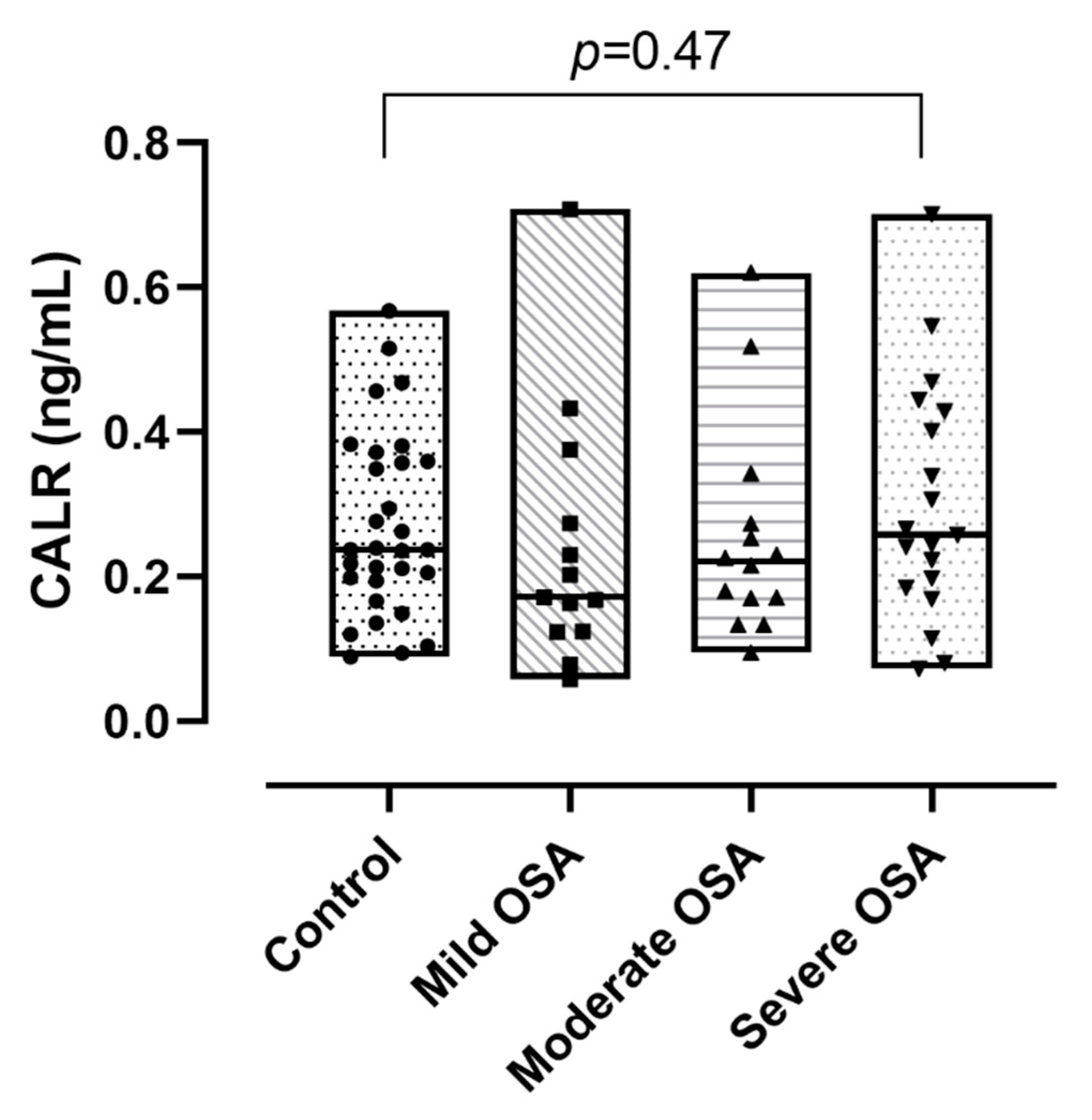
3.4. Circulating Calreticulin Levels
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Trzepizur, W.; Le Vaillant, M.; Meslier, N.; Pigeanne, T.; Masson, P.; Humeau, M.P.; Bizieux-Thaminy, A.; Goupil, F.; Chollet, S.; Ducluzeau, P.H.; et al. Independent association between nocturnal intermittent hypoxemia and metabolic dyslipidemia. Chest 2013, 143, 1584–1589. [Google Scholar] [CrossRef] [PubMed]
- Lévy, P.; Kohler, M.; McNicholas, W.T.; Barbé, F.; McEvoy, R.D.; Somers, V.K.; Lavie, L.; Pépin, J.-L. Obstructive sleep apnoea syndrome. Nat. Rev. Dis. Prim. 2015, 1, 15015. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Nanayakkara, A.; Jun, J.; Savransky, V.; Polotsky, V.Y. Effect of deficiency in SREBP cleavage-activating protein on lipid metabolism during intermittent hypoxia. Physiol. Genom. 2007, 31, 273–280. [Google Scholar] [CrossRef]
- Gileles-Hillel, A.; Kheirandish-Gozal, L.; Gozal, D. Biological plausibility linking sleep apnoea and metabolic dysfunction. Nat. Rev. Endocrinol. 2016, 12, 290–298. [Google Scholar] [CrossRef] [PubMed]
- Bartness, T.J.; Shrestha, Y.B.; Vaughan, C.H.; Schwartz, G.J.; Song, C.K. Sensory and sympathetic nervous system control of white adipose tissue lipolysis. Mol. Cell. Endocrinol. 2010, 318, 34–43. [Google Scholar] [CrossRef]
- Drager, L.F.; Li, J.; Shin, M.K.; Reinke, C.; Aggarwal, N.R.; Jun, J.C.; Bevans-Fonti, S.; Sztalryd, C.; O’Byrne, S.M.; Kroupa, O.; et al. Intermittent hypoxia inhibits clearance of triglyceride-rich lipoproteins and inactivates adipose lipoprotein lipase in a mouse model of sleep apnoea. Eur. Hear. J. 2012, 33, 783–790. [Google Scholar] [CrossRef]
- Drager, L.F.; Jun, J.; Polotsky, V.Y. Obstructive sleep apnea and dyslipidemia: Implications for atherosclerosis. Curr. Opin. Endocrinol. Diabetes Obes. 2010, 17, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Lillis, A.P.; Van Duyn, L.B.; Murphy-Ullrich, J.E.; Strickland, D.K. LDL Receptor-Related Protein 1: Unique Tissue-Specific Functions Revealed by Selective Gene Knockout Studies. Physiol. Rev. 2008, 88, 887–918. [Google Scholar] [CrossRef]
- Gorovoy, M.; Gaultier, A.; Campana, W.M.; Firestein, G.S.; Gonias, S.L. Inflammatory mediators promote production of shed LRP1/CD91, which regulates cell signaling and cytokine expression by macrophages. J. Leukoc. Biol. 2010, 88, 769–778. [Google Scholar] [CrossRef] [PubMed]
- Costales, P.; Castellano, J.; Revuelta-López, E.; Cal, R.; Aledo, R.; Llampayas, O.; Nasarre, L.; Juarez, C.; Badimon, L.; Llorente-Cortés, V. Lipopolysaccharide downregulates CD91/low-density lipoprotein receptor-related protein 1 expression through SREBP-1 overexpression in human macrophages. Atherosclerosis 2013, 227, 79–88. [Google Scholar] [CrossRef]
- Gonias, S.L.; Campana, W.M. LDL receptor-related protein-1: A regulator of inflammation in atherosclerosis, cancer, and injury to the nervous system. Am. J. Pathol. 2014, 184, 18–27. [Google Scholar] [CrossRef]
- Rohlmann, A.; Gotthardt, M.; Hammer, R.E.; Herz, J. Inducible inactivation of hepatic LRP gene by cre-mediated recombination confirms role of LRP in clearance of chylomicron remnants. J. Clin. Investig. 1998, 101, 689–695. [Google Scholar] [CrossRef] [PubMed]
- Van Den Biggelaar, M.; Madsen, J.J.; Faber, J.H.; Zuurveld, M.G.; van der Zwaan, C.; Olsen, O.H.; Stennicke, H.R.; Mertens, K.; Meijer, A.B. Factor VIII Interacts with the Endocytic Receptor Low-density Lipoprotein Receptor-related Protein 1 via an Extended Surface Comprising “Hot-Spot” Lysine Residues. J. Biol. Chem. 2015, 290, 16463–16476. [Google Scholar] [CrossRef] [PubMed]
- Gaultier, A.; Arandjelovic, S.; Niessen, S.; Overton, C.D.; Linton, M.F.; Fazio, S.; Campana, W.M.; Cravatt, B.F., III; Gonias, S.L. Regulation of tumor necrosis factor receptor-1 and the IKK-NF-κB pathway by LDL receptor–related protein explains the antiinflammatory activity of this receptor. Blood 2008, 111, 5316–5325. [Google Scholar] [CrossRef] [PubMed]
- Quinn, K.A.; Grimsley, P.G.; Dai, Y.P.; Tapner, M.; Chesterman, C.N.; Owensby, D.A. Soluble low density lipoprotein receptor-related protein (LRP) circulates in human plasma. J. Biol. Chem. 1997, 272, 23946–23951. [Google Scholar] [CrossRef] [PubMed]
- Kielbik, M.; Szulc-Kielbik, I.; Klink, M. Calreticulin—Multifunctional Chaperone in Immunogenic Cell Death: Potential Significance as a Prognostic Biomarker in Ovarian Cancer Patients. Cells 2021, 10, 130. [Google Scholar] [CrossRef] [PubMed]
- Ogden, C.A.; de Cathelineau, A.; Hoffmann, P.R.; Bratton, D.; Ghebrehiwet, B.; Fadok, V.A.; Henson, P.M. C1q and mannose binding lectin engagement of cell surface calreticulin and CD91 initiates macropinocytosis and uptake of apoptotic cells. J. Exp. Med. 2001, 194, 781–795. [Google Scholar] [CrossRef]
- Pákó, J.; Kunos, L.; Mészáros, M.; Tárnoki, D.L.; Tárnoki, Á.D.; Horváth, I.; Bikov, A. Decreased Levels of Anti-Aging Klotho in Obstructive Sleep Apnea. Rejuvenation Res. 2020, 23, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Kunos, L.; Horvath, P.; Kis, A.; Tarnoki, D.L.; Tarnoki, A.D.; Lazar, Z.; Bikov, A. Circulating Survivin Levels in Obstructive Sleep Apnoea. Lung 2018, 196, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Bikov, A.; Kunos, L.; Pállinger, É.; Lázár, Z.; Kis, A.; Horváth, G.; Losonczy, G.; Komlósi, Z.I. Diurnal variation of circulating microvesicles is associated with the severity of obstructive sleep apnoea. Sleep Breath. 2017, 21, 595–600. [Google Scholar] [CrossRef]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for scoring respiratory events in sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Qin, S.; Yin, J.; Huang, K. Free Fatty Acids Increase Intracellular Lipid Accumulation and Oxidative Stress by Modulating PPARα and SREBP-1c in L-02 Cells. Lipids 2016, 51, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Bertolio, R.; Napoletano, F.; Mano, M.; Maurer-Stroh, S.; Fantuz, M.; Zannini, A.; Bicciato, S.; Sorrentino, G.; Del Sal, G. Sterol regulatory element binding protein 1 couples mechanical cues and lipid metabolism. Nat. Commun. 2019, 10, 1326. [Google Scholar] [CrossRef] [PubMed]
- Costales, P.; Aledo, R.; Vérnia, S.; Das, A.; Shah, V.H.; Casado, M.; Badimon, L.; Llorente-Cortés, V. Selective role of sterol regulatory element binding protein isoforms in aggregated LDL-induced vascular low density lipoprotein receptor-related protein-1 expression. Atherosclerosis 2010, 213, 458–468. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.X.; He, L.Y.; Zhang, M.; Wang, F.; Liu, F.; Peng, W.X. 1,25-Dihydroxyvitamin D3 regulates expression of LRP1 and RAGE in vitro and in vivo, enhancing Aβ1-40 brain-to-blood efflux and peripheral uptake transport. Neuroscience 2016, 322, 28–38. [Google Scholar] [CrossRef]
- Zhao, Y.; Zeng, C.-Y.; Li, X.-H.; Yang, T.-T.; Kuang, X.; Du, J.-R. Klotho overexpression improves amyloid-β clearance and cognition in the APP/PS1 mouse model of Alzheimer’s disease. Aging Cell 2020, 19, 13239. [Google Scholar] [CrossRef]
- Bozkurt, N.C.; Cakal, E.; Sahin, M.; Ozkaya, E.C.; Firat, H.; Delibasi, T. The relation of serum 25-hydroxyvitamin-D levels with severity of obstructive sleep apnea and glucose metabolism abnormalities. Endocrine 2012, 41, 518–525. [Google Scholar] [CrossRef]
- Gabryelska, A.; Szmyd, B.; Szemraj, J.; Stawski, R.; Sochal, M.; Białasiewicz, P. Patients with obstructive sleep apnea present with chronic upregulation of serum HIF-1α protein. J. Clin. Sleep Med. 2020, 16, 1761–1768. [Google Scholar] [CrossRef]
- Gabryelska, A.; Szmyd, B.; Panek, M.; Szemraj, J.; Kuna, P.; Białasiewicz, P. Serum hypoxia-inducible factor-1α protein level as a diagnostic marker of obstructive sleep apnea. Pol. Arch. Intern. Med. 2020, 130, 158–160. [Google Scholar] [CrossRef]
- Lu, D.; Li, N.; Yao, X.; Zhou, L. Potential inflammatory markers in obstructive sleep apnea-hypopnea syndrome. Bosn. J. Basic Med. Sci. 2017, 17, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Gabryelska, A.; Sochal, M.; Turkiewicz, S.; Białasiewicz, P. Relationship between HIF-1 and Circadian Clock Proteins in Obstructive Sleep Apnea Patients-Preliminary Study. J. Clin. Med. 2020, 9, 1599. [Google Scholar] [CrossRef] [PubMed]
- Gabryelska, A.; Karuga, F.F.; Szmyd, B.; Białasiewicz, P. HIF-1α as a Mediator of Insulin Resistance, T2DM, and Its Complications: Potential Links With Obstructive Sleep Apnea. Front. Physiol. 2020, 11, 1035. [Google Scholar] [CrossRef] [PubMed]
- Castellano, J.; Aledo, R.; Sendra, J.; Costales, P.; Juan-Babot, O.; Badimon, L.; Llorente-Cortés, V. Hypoxia Stimulates Low-Density Lipoprotein Receptor–Related Protein-1 Expression Through Hypoxia-Inducible Factor-1α in Human Vascular Smooth Muscle Cells. Arter. Thromb. Vasc. Biol. 2011, 31, 1411–1420. [Google Scholar] [CrossRef]
- Li, P.; Wu, J.; Zhao, L.; Feng, X.W. Effects and relationship of intermittent hypoxia on serum lipid levels, hepatic low-density lipoprotein receptor-related protein 1, and hypoxia-inducible factor 1α. Sleep Breath. 2016, 20, 167–173. [Google Scholar] [CrossRef]
- Field, P.A.; Gibbons, G.F. Decreased hepatic expression of the low-density lipoprotein (LDL) receptor and LDL receptor-related protein in aging rats is associated with delayed clearance of chylomicrons from the circulation. Metabolism 2000, 49, 492–498. [Google Scholar] [CrossRef]
- Chen, J.; Pi, S.; Yu, C.; Shi, H.; Liu, Y.; Guo, X.; Zhou, L.; Li, Y.; He, H.; Xia, Y.; et al. sLRP1 (Soluble Low-Density Lipoprotein Receptor-Related Protein 1). Arter. Thromb. Vasc. Biol. 2020, 40, 166–179. [Google Scholar] [CrossRef]
- de Gonzalo-Calvo, D.; Cenarro, A.; Martínez-Bujidos, M.; Badimon, L.; Bayes-Genis, A.; Ordonez-Llanos, J.; Civeira, F.; Llorente-Cortés, V. Circulating soluble low-density lipoprotein receptor-related protein 1 (sLRP1) concentration is associated with hypercholesterolemia: A new potential biomarker for atherosclerosis. Int. J. Cardiol. 2015, 201, 20–29. [Google Scholar] [CrossRef]
- Brifault, C.; Gilder, A.S.; Laudati, E.; Banki, M.; Gonias, S.L. Shedding of membrane-associated LDL receptor-related protein-1 from microglia amplifies and sustains neuroinflammation. J. Biol. Chem. 2017, 292, 18699–18712. [Google Scholar] [CrossRef]
- Qian, Y.; Yi, H.; Zou, J.; Meng, L.; Tang, X.; Zhu, H.; Yu, D.; Zhou, H.; Su, K.; Guan, J.; et al. Independent Association between Sleep Fragmentation and Dyslipidemia in Patients with Obstructive Sleep Apnea. Sci. Rep. 2016, 6, 26089. [Google Scholar] [CrossRef]
- Liu, X.; Xu, F.; Fu, Y.; Liu, F.; Sun, S.; Wu, X. Calreticulin induces delayed cardioprotection through mitogen-activated protein kinases. Proteomics 2006, 6, 3792–3800. [Google Scholar] [CrossRef] [PubMed]
- Hirano, M.; Imagawa, A.; Totani, K. Stratified analysis of lectin-like chaperones in the folding disease-related metabolic syndrome rat model. Biochem. Biophys. Res. Commun. 2016, 478, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.; Xian, X.; Holland, W.L.; Tsai, S.; Herz, J. Low-Density Lipoprotein Receptor-Related Protein-1 Protects Against Hepatic Insulin Resistance and Hepatic Steatosis. EBioMedicine 2016, 7, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Gaultier, A.; Arandjelovic, S.; Li, X.; Janes, J.; Dragojlovic, N.; Zhou, G.P.; Dolkas, J.; Myers, R.R.; Gonias, S.L.; Campana, W.M. A shed form of LDL receptor-related protein-1 regulates peripheral nerve injury and neuropathic pain in rodents. J. Clin. Investig. 2008, 118, 161–172. [Google Scholar] [CrossRef]
- Scilabra, S.D.; Troeberg, L.; Yamamoto, K.; Emonard, H.; Thøgersen, I.; Enghild, J.J.; Strickland, D.K.; Nagase, H. Differential regulation of extracellular tissue inhibitor of metalloproteinases-3 levels by cell membrane-bound and shed low density lipoprotein receptor-related protein 1. J. Biol. Chem. 2013, 288, 332–342. [Google Scholar] [CrossRef]
- Overton, C.D.; Yancey, P.G.; Major, A.S.; Linton, M.F.; Fazio, S. Deletion of macrophage LDL receptor-related protein increases atherogenesis in the mouse. Circ. Res. 2007, 100, 670–677. [Google Scholar] [CrossRef]
- May, P.; Bock, H.H.; Nofer, J.R. Low density receptor-related protein 1 (LRP1) promotes anti-inflammatory phenotype in murine macrophages. Cell Tissue Res. 2013, 354, 887–889. [Google Scholar] [CrossRef]
- Meilinger, M.; Gschwentner, C.; Burger, I.; Haumer, M.; Wahrmann, M.; Szollar, L.; Nimpf, J.; Huettinger, M. Metabolism of activated complement component C3 is mediated by the low density lipoprotein receptor-related protein/alpha(2)-macroglobulin receptor. J. Biol. Chem. 1999, 274, 38091–38096. [Google Scholar] [CrossRef]
- Horvath, P.; Tarnoki, D.L.; Tarnoki, A.D.; Karlinger, K.; Lazar, Z.; Losonczy, G.; Kunos, L.; Bikov, A. Complement system activation in obstructive sleep apnea. J. Sleep Res. 2018, 27, e12674. [Google Scholar] [CrossRef] [PubMed]
- Saenko, E.L.; Yakhyaev, A.V.; Mikhailenko, I.; Strickland, D.K.; Sarafanov, A.G. Role of the Low Density Lipoprotein-related Protein Receptor in Mediation of Factor VIII Catabolism*. J. Biol. Chem. 1999, 274, 37685–37692. [Google Scholar] [CrossRef]
- Bovenschen, N.; Mertens, K.; Hu, L.; Havekes, L.M.; van Vlijmen, B.J. LDL receptor cooperates with LDL receptor-related protein in regulating plasma levels of coagulation factor VIII in vivo. Blood 2005, 106, 906–912. [Google Scholar] [CrossRef] [PubMed]
- Phillips, C.L.; McEwen, B.J.; Morel-Kopp, M.C.; Yee, B.J.; Sullivan, D.R.; Ward, C.M.; Tofler, G.H.; Grunstein, R.R. Effects of continuous positive airway pressure on coagulability in obstructive sleep apnoea: A randomised, placebo-controlled crossover study. Thorax 2012, 67, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Weiss, H.J.; Sussman, I.I.; Hoyer, L.W. Stabilization of factor VIII in plasma by the von Willebrand factor. Studies on posttransfusion and dissociated factor VIII and in patients with von Willebrand’s disease. J. Clin. Investig. 1977, 60, 390–404. [Google Scholar] [CrossRef] [PubMed]
- von Känel, R.; Malan, N.T.; Hamer, M.; Lambert, G.W.; Schlaich, M.; Reimann, M.; Malan, L. Three-year changes of prothrombotic factors in a cohort of South Africans with a high clinical suspicion of obstructive sleep apnea. Thromb. Haemost. 2016, 115, 63–72. [Google Scholar] [CrossRef]
- Rastegarlari, G.; Pegon, J.N.; Casari, C.; Odouard, S.; Navarrete, A.M.; Saint-Lu, N.; van Vlijmen, B.J.; Legendre, P.; Christophe, O.D.; Denis, C.V.; et al. Macrophage LRP1 contributes to the clearance of von Willebrand factor. Blood 2012, 119, 2126–2134. [Google Scholar] [CrossRef]
- Kounnas, M.Z.; Henkin, J.; Argraves, W.S.; Strickland, D.K. Low density lipoprotein receptor-related protein/alpha 2-macroglobulin receptor mediates cellular uptake of pro-urokinase. J. Biol. Chem. 1993, 268, 21862–21867. [Google Scholar] [CrossRef]
- Conese, M.; Nykjaer, A.; Petersen, C.M.; Cremona, O.; Pardi, R.; Andreasen, P.A.; Gliemann, J.; Christensen, E.I.; Blasi, F. alpha-2 Macroglobulin receptor/Ldl receptor-related protein(Lrp)-dependent internalization of the urokinase receptor. J. Cell Biol. 1995, 131, 1609–1622. [Google Scholar] [CrossRef]
- Punjabi, N.M.; Sorkin, J.D.; Katzel, L.I.; Goldberg, A.P.; Schwartz, A.R.; Smith, P.L. Sleep-disordered breathing and insulin resistance in middle-aged and overweight men. Am. J. Respir. Crit. Care. Med. 2002, 165, 677–682. [Google Scholar] [CrossRef]
- Wolk, R.; Shamsuzzaman, A.S.M.; Somers, V.K. Obesity, Sleep Apnea, and Hypertension. Hypertension 2003, 42, 1067–1074. [Google Scholar] [CrossRef]
- Esser, N.; Legrand-Poels, S.; Piette, J.; Scheen, A.J.; Paquot, N. Inflammation as a link between obesity, metabolic syndrome and type 2 diabetes. Diabetes Res. Clin. Pract. 2014, 105, 141–150. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control (n = 30) | OSA (n = 46) | p | |
|---|---|---|---|
| Age (years) | 43 (30–51) | 54 (46–62) | <0.001 |
| Males (n, %) | 23 | 67 | <0.001 |
| BMI (kg/m2) | 23.89 (20.96–26.99) | 29.89 (25.11–37.56) | <0.001 |
| Hypertension (%) | 30 | 67 | 0.001 |
| Diabetes (%) | 10 | 15 | 0.511 |
| Dyslipidaemia (%) | 27 | 30 | 0.723 |
| Cardiovascular disease (%) | 7 | 9 | 0.748 |
| Cardiac arrythmia (%) | 13 | 26 | 0.183 |
| Smokers (%) | 3 | 30 | 0.004 |
| SBP (mmHg) | 120.0 (110.0–128.8) | 135.5 (122.0–148.0) | <0.001 |
| DBP (mmHg) | 70.0 (66.3–80.0) | 84.0 (78.5–90.0) | <0.001 |
| CRP (mg/l) | 1.75 (0.84–2.50) | 3.20 (1.79–4.79) | 0.005 |
| Glucose (mmol/l) | 4.7 (4.3–5.2) | 5.1 (4.9–6.2) | 0.002 |
| Cholesterol (mmol/l) | 5.63 ± 1.03 | 5.59 ± 1.03 | 0.877 |
| HDL-C (mmol/l) | 1.59 (1.38–1.97) | 1.25 (1.06–1.47) | <0.001 |
| LDL-C (mmol/l) | 3.39 ± 0.83 | 3.58 ± 0.88 | 0.328 |
| Triglyceride (mmol/l) | 1.29 (0.93–1.56) | 1.64 (1.26–2.15) | 0.004 |
| Lipoprotein (a) (mmol/l) | 0.22 (0.08–0.58) | 0.35 (0.02–0.54) | 0.937 |
| ApoA1 (g/l) | 1.66 (1.50–1.73) | 1.46 (1.29–1.64) | 0.097 |
| ApoB (g/l) | 1.17 (1.09–1.38) | 1.19 (0.99–1.39) | 0.790 |
| TyG | 8.37 ± 0.32 | 8.92 ± 0.50 | <0.001 |
| AIP | −0.13 ± 0.25 | 0.11 ± 0.25 | <0.001 |
| AHI (1/h) | 2.15 (1.13–3.08) | 26.05 (12.50–35.63) | <0.001 |
| ODI (1/h) | 0.90 (0.23–1.65) | 22.0 (9.33–33.40) | <0.001 |
| SPT (min) | 431.56 ± 47.41 | 447.59 ± 41.43 | 0.270 |
| TST (min) | 401.31 ± 41.52 | 415.04 ± 31.75 | 0.249 |
| TST90% (%) | 0 (0–0) | 4.5 (0.7–16.4) | <0.001 |
| MinSatO2 (%) | 91 (89–92) | 83 (75–87) | <0.001 |
| ESS | 6 (4–8) | 7 (5–10) | 0.502 |
| sLRP-1 | CALR | |||
|---|---|---|---|---|
| Age (years) | r = −0.292 | p = 0.011 | r = 0.345 | p = 0.002 |
| Male (n, %) | r = −0.061 | p = 0.603 | r = 0.023 | p = 0.845 |
| BMI (kg/m2) | r = −0.354 | p = 0.002 | r = 0.305 | p = 0.007 |
| Cigarette pack years | r = −0.306 | p = 0.008 | r = −0.039 | p = 0.738 |
| Glucose (mmol/L) | r = −0.143 | p = 0.269 | r = −0.077 | p = 0.554 |
| CRP (mg/L) | r = −0.212 | p = 0.097 | r = 0.207 | p = 0.106 |
| Cholesterol (mmol/L) | r = −0.174 | p = 0.132 | r = −0.027 | p = 0.820 |
| HDL-C (mmol/L) | r = 0.174 | p = 0.134 | r = −0.078 | p = 0.503 |
| LDL-C (mmol/L) | r = −0.233 | p = 0.043 | r = −0.030 | p = 0.799 |
| Triglyceride (mmol/L) | r = −0.265 | p = 0.021 | r = 0.139 | p = 0.233 |
| Lipoprotein (a) (mmol/l) | r = 0.105 | p = 0.486 | r = −0.234 | p = 0.118 |
| ApoA1 (g/L) | r = −0.062 | p = 0.664 | r = 0.029 | p = 0.839 |
| ApoB (g/L) | r = −0.211 | p = 0.134 | r = −0.024 | p = 0.867 |
| TyG | r = −0.367 | p = 0.004 | r = −0.008 | p = 0.949 |
| AIP | r = −0.269 | p = 0.019 | r = 0.125 | p = 0.281 |
| AHI | r = −0.177 | p = 0.126 | r = 0.041 | p = 0.722 |
| ODI | r = −0.233 | p = 0.043 | r = 0.121 | p = 0.296 |
| SPT (min) | r = −0.143 | p = 0.385 | r = −0.084 | p = 0.611 |
| TST (min) | r = −0.028 | p = 0.865 | r = 0.063 | p = 0.702 |
| TST90% | r = −0.194 | p = 0.097 | r = 0.116 | p = 0.325 |
| Min SatO2 | r = 0.198 | p = 0.091 | r = −0.154 | p = 0.190 |
| ESS | r = 0.092 | p = 0.440 | r = −0.029 | p = 0.811 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meszaros, M.; Kunos, L.; Tarnoki, A.D.; Tarnoki, D.L.; Lazar, Z.; Bikov, A. The Role of Soluble Low-Density Lipoprotein Receptor-Related Protein-1 in Obstructive Sleep Apnoea. J. Clin. Med. 2021, 10, 1494. https://doi.org/10.3390/jcm10071494
Meszaros M, Kunos L, Tarnoki AD, Tarnoki DL, Lazar Z, Bikov A. The Role of Soluble Low-Density Lipoprotein Receptor-Related Protein-1 in Obstructive Sleep Apnoea. Journal of Clinical Medicine. 2021; 10(7):1494. https://doi.org/10.3390/jcm10071494
Chicago/Turabian StyleMeszaros, Martina, Laszlo Kunos, Adam Domonkos Tarnoki, David Laszlo Tarnoki, Zsofia Lazar, and Andras Bikov. 2021. "The Role of Soluble Low-Density Lipoprotein Receptor-Related Protein-1 in Obstructive Sleep Apnoea" Journal of Clinical Medicine 10, no. 7: 1494. https://doi.org/10.3390/jcm10071494
APA StyleMeszaros, M., Kunos, L., Tarnoki, A. D., Tarnoki, D. L., Lazar, Z., & Bikov, A. (2021). The Role of Soluble Low-Density Lipoprotein Receptor-Related Protein-1 in Obstructive Sleep Apnoea. Journal of Clinical Medicine, 10(7), 1494. https://doi.org/10.3390/jcm10071494