
Balneotherapy for Fibromyalgia Syndrome: A Systematic Review and Meta-Analysis

 ,
,  and
and
Abstract
1. Introduction
2. Methods
2.1. Protocol and Registration
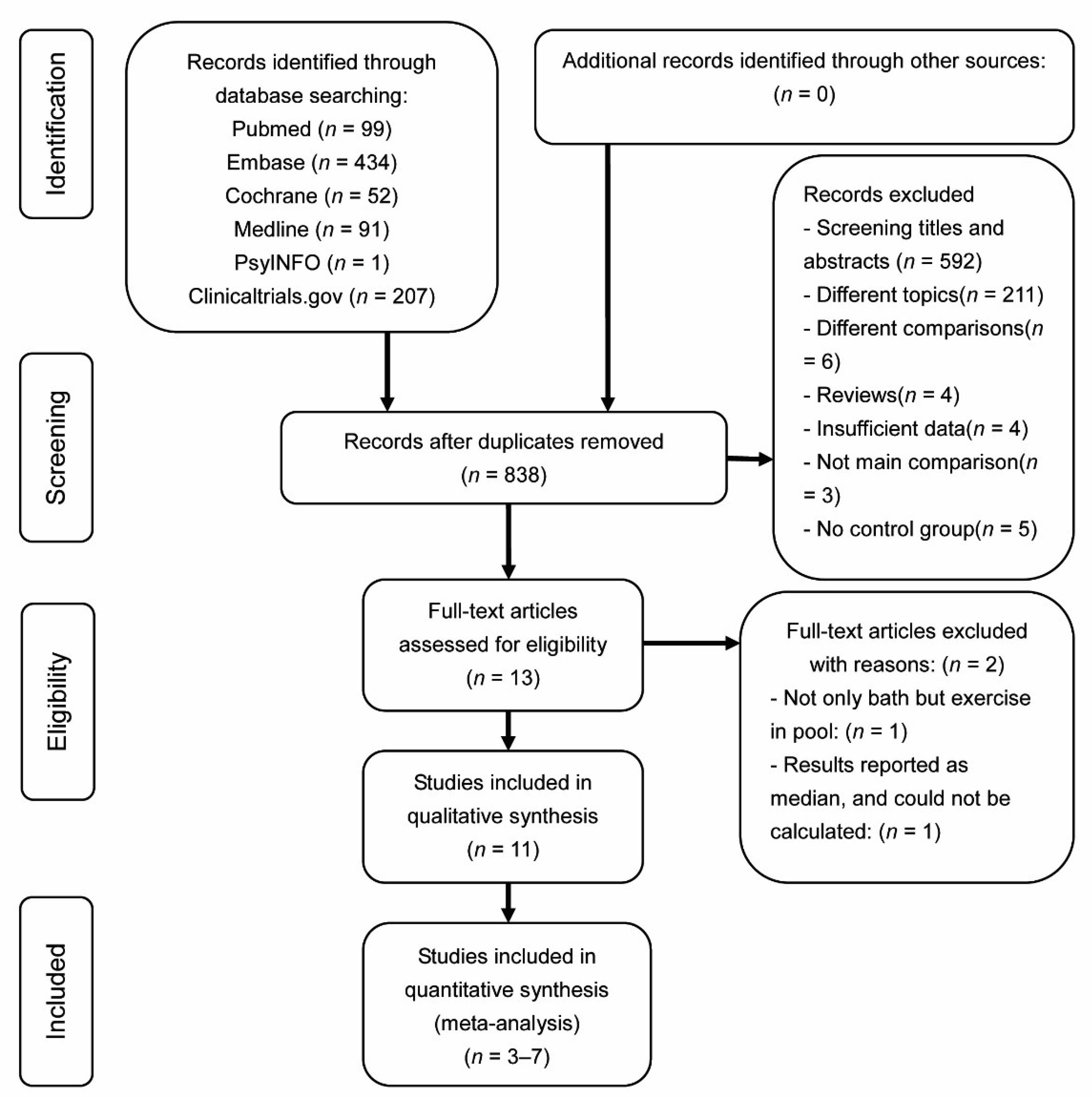
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction and Management
2.5. Assessment of Risk of Bias (ROB) in Included Studies
2.6. Assessment of Treatment Effect
2.7. Assessment of Heterogeneity
2.8. Sensitivity Analysis
3. Results
3.1. Hallmarks of Included Studies
3.2. Location Hallmarks
3.3. Participant Hallmarks
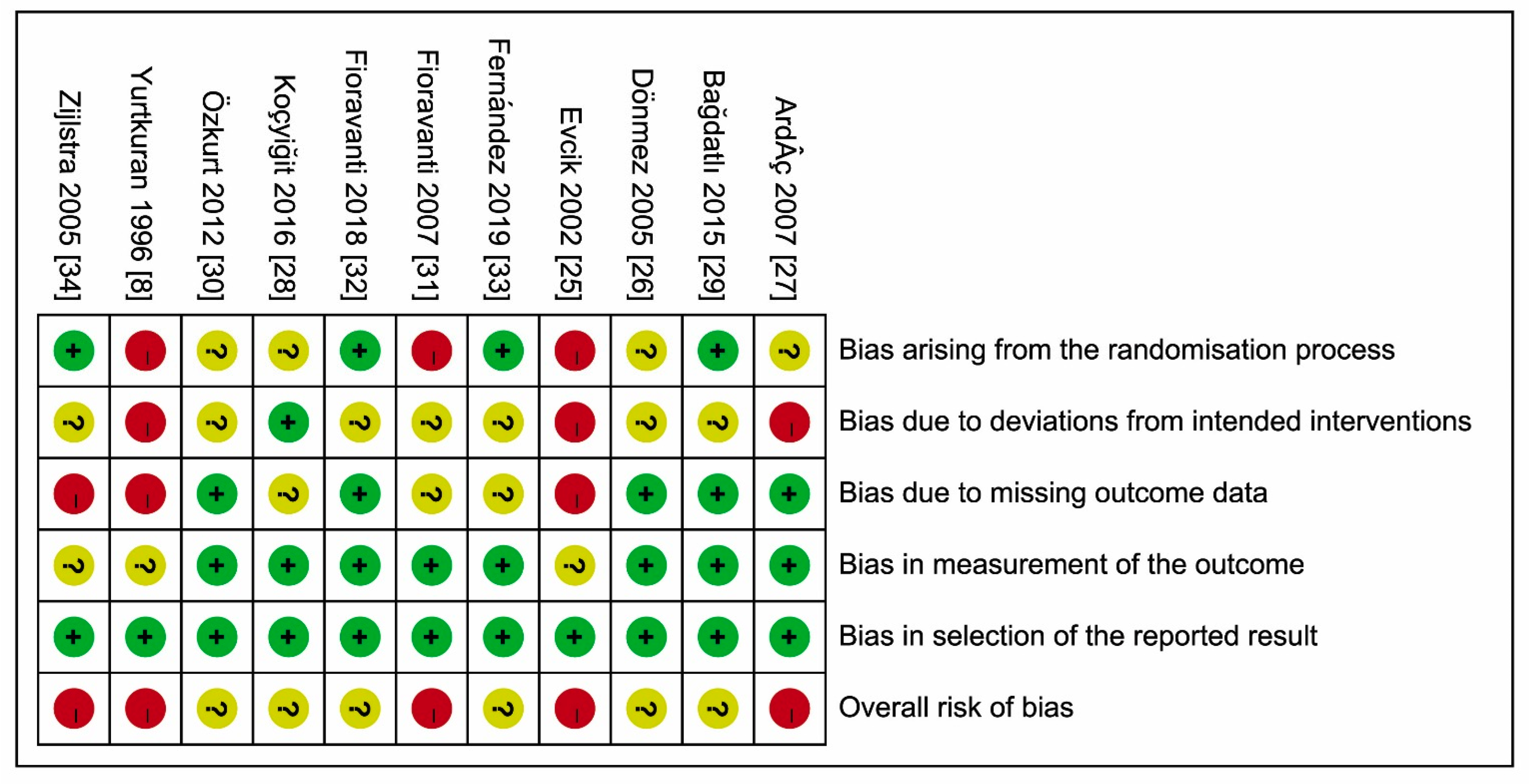
3.4. ROBs of Included Studies
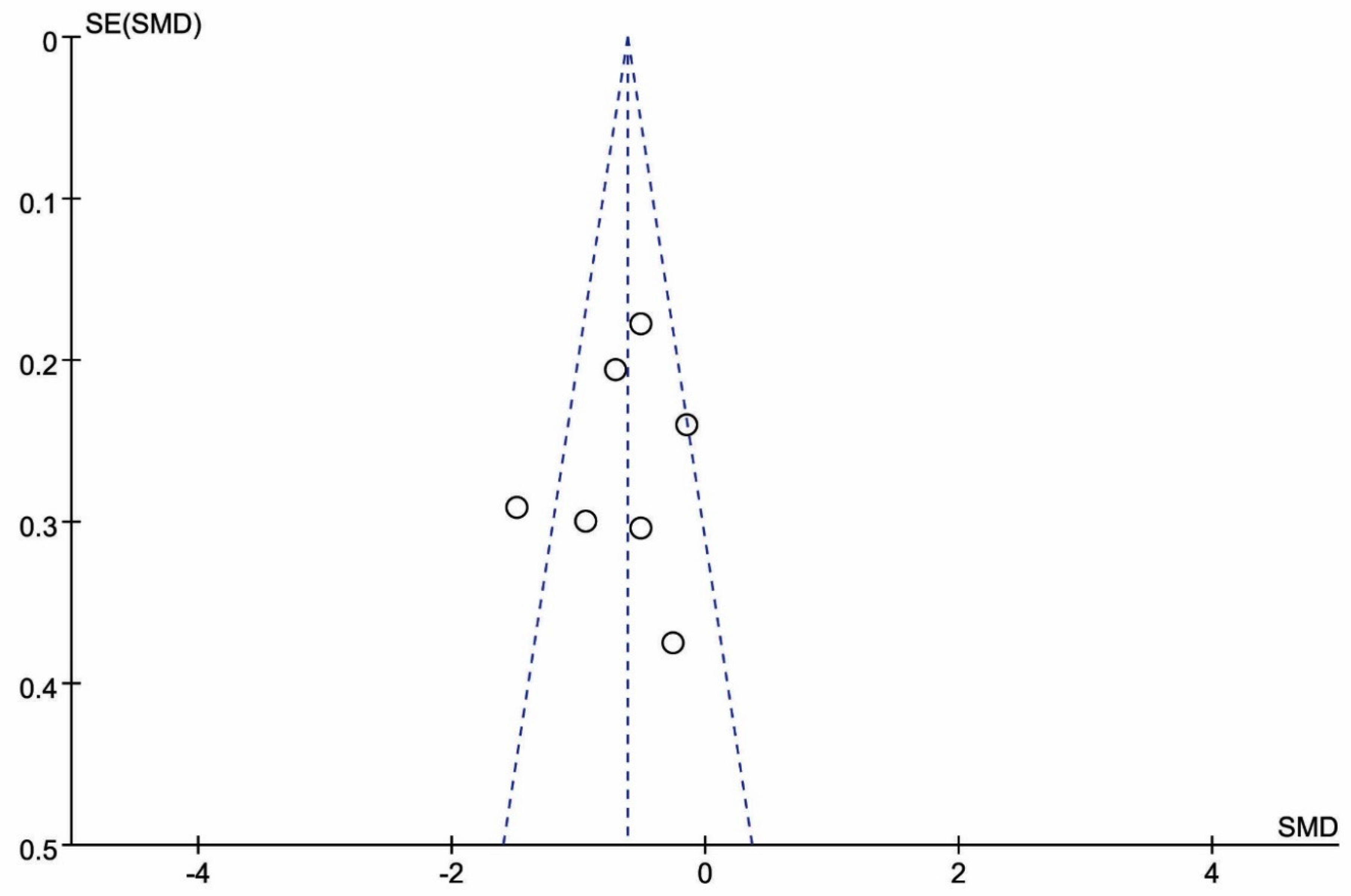
3.5. Publication Bias
3.6. Effects of BT Interventions
3.6.1. BT Intervention Sessions and Data Analysis Time Points
3.6.2. Primary Outcome Measures
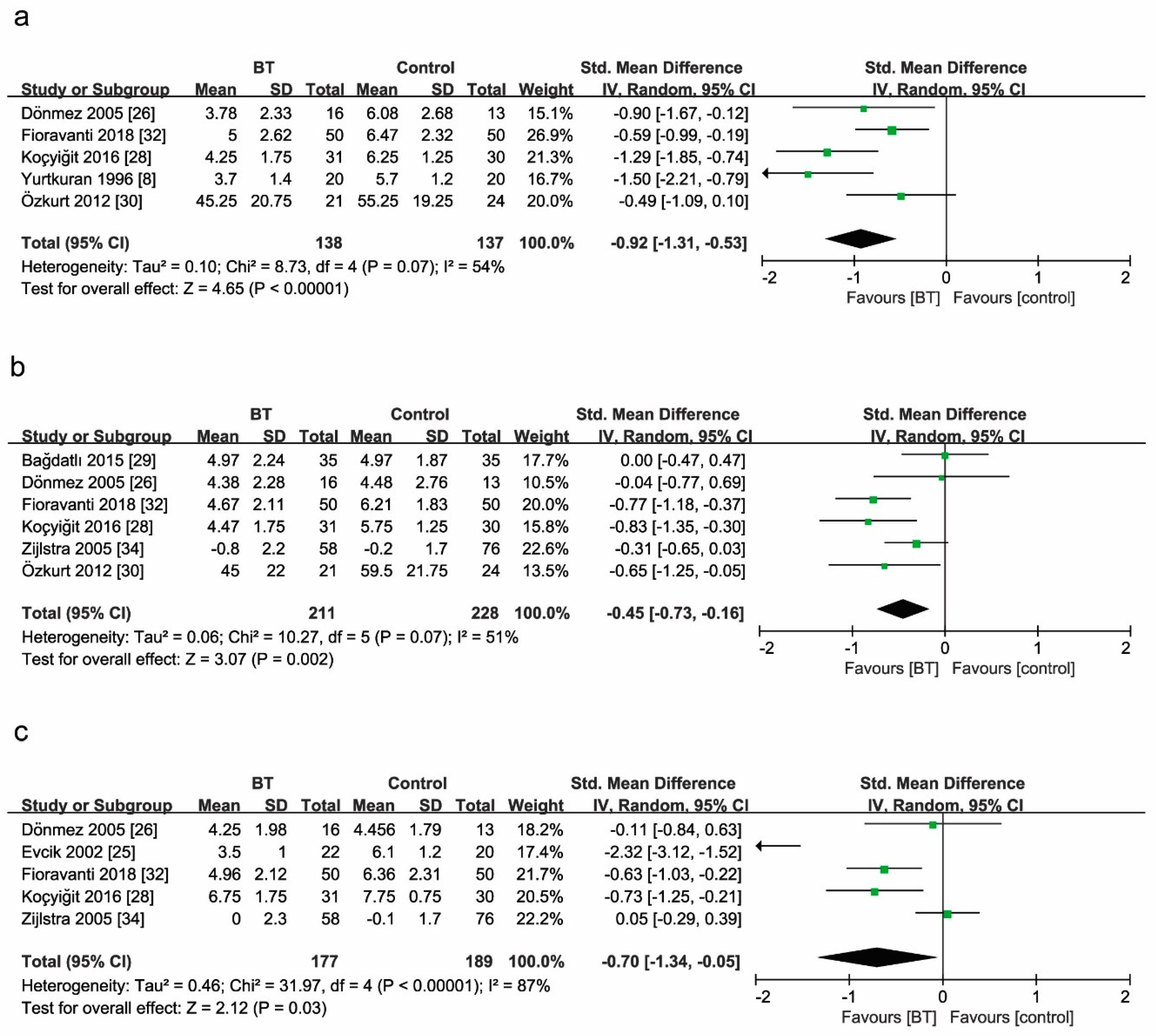
Pain
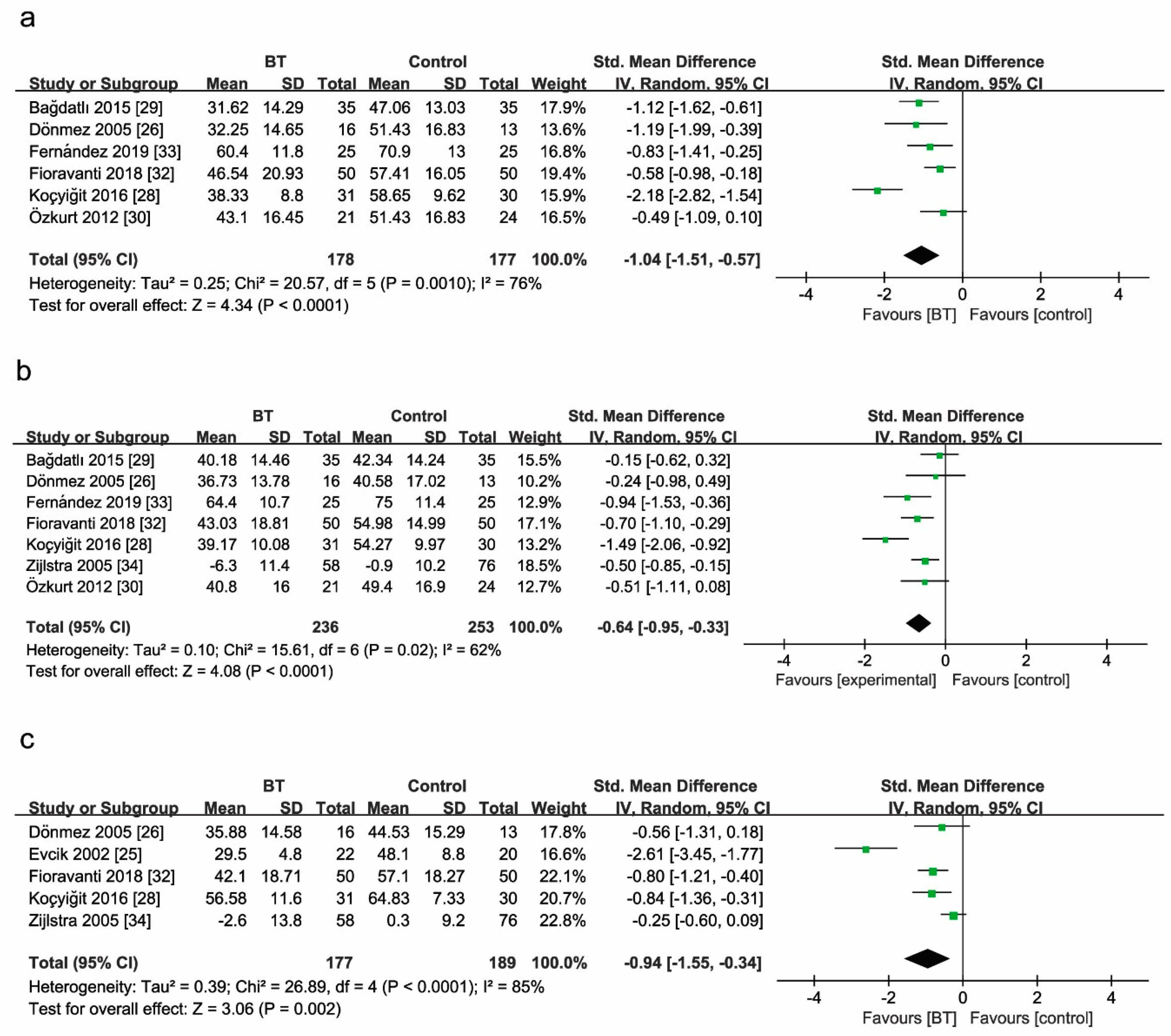
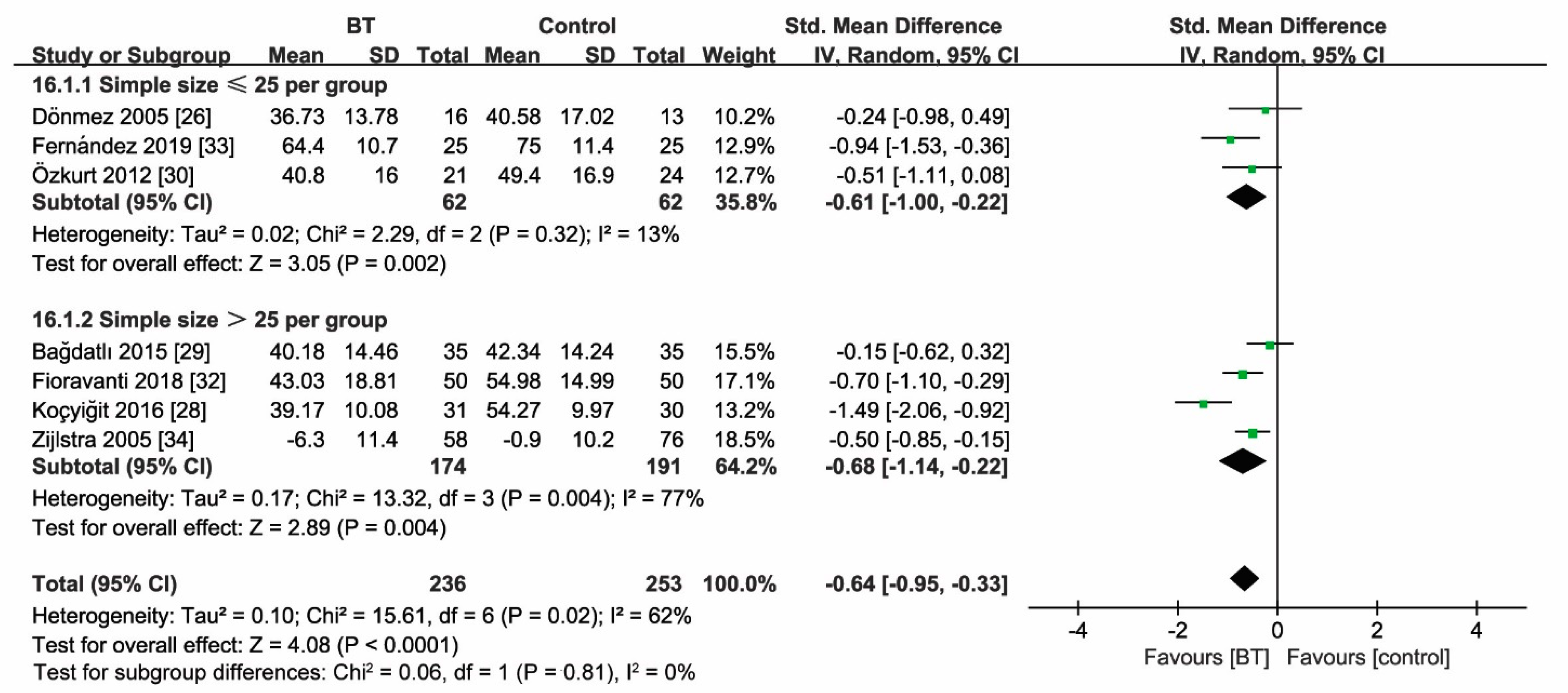
Fibromyalgia Impact Questionnaire
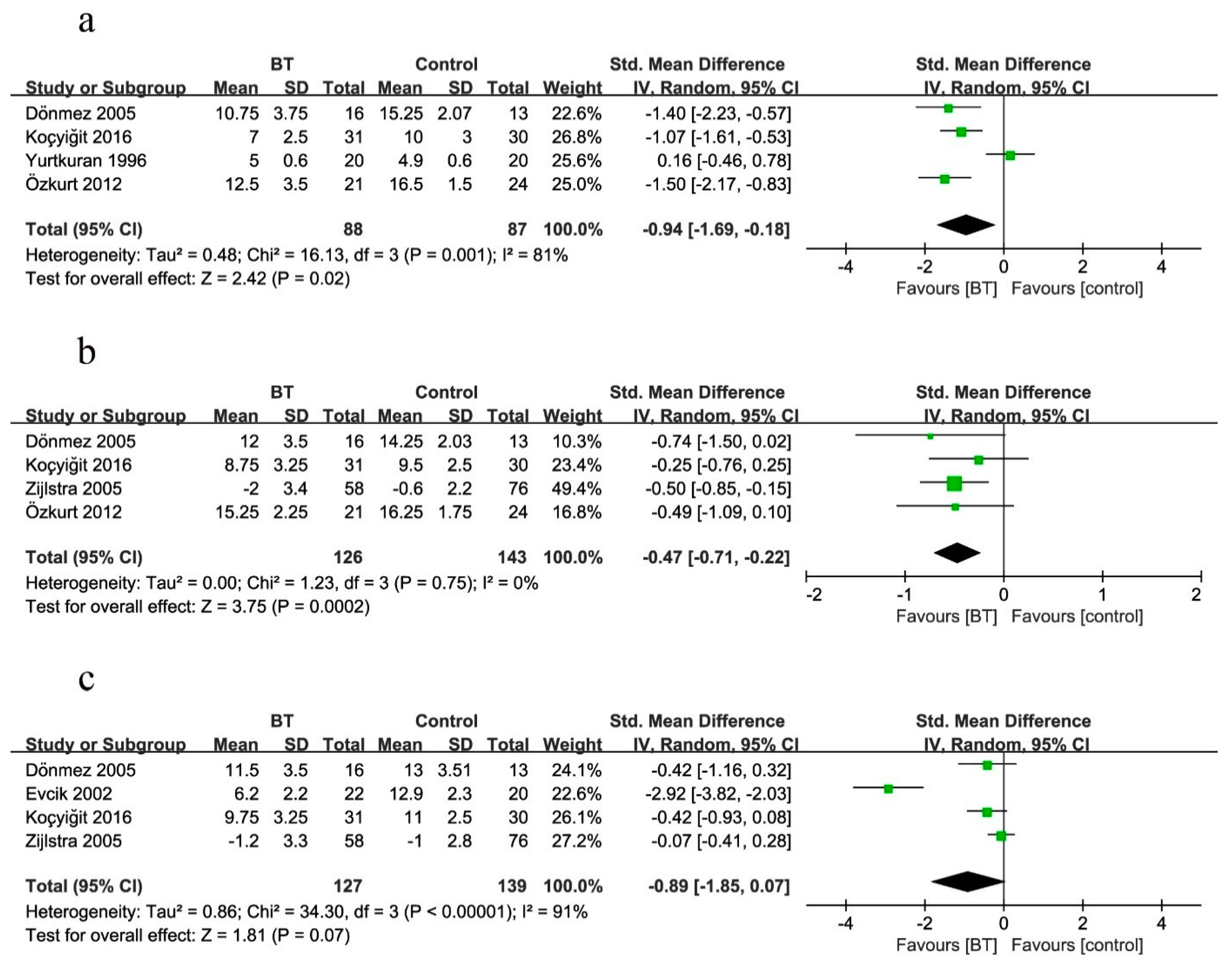
Tender Points Count
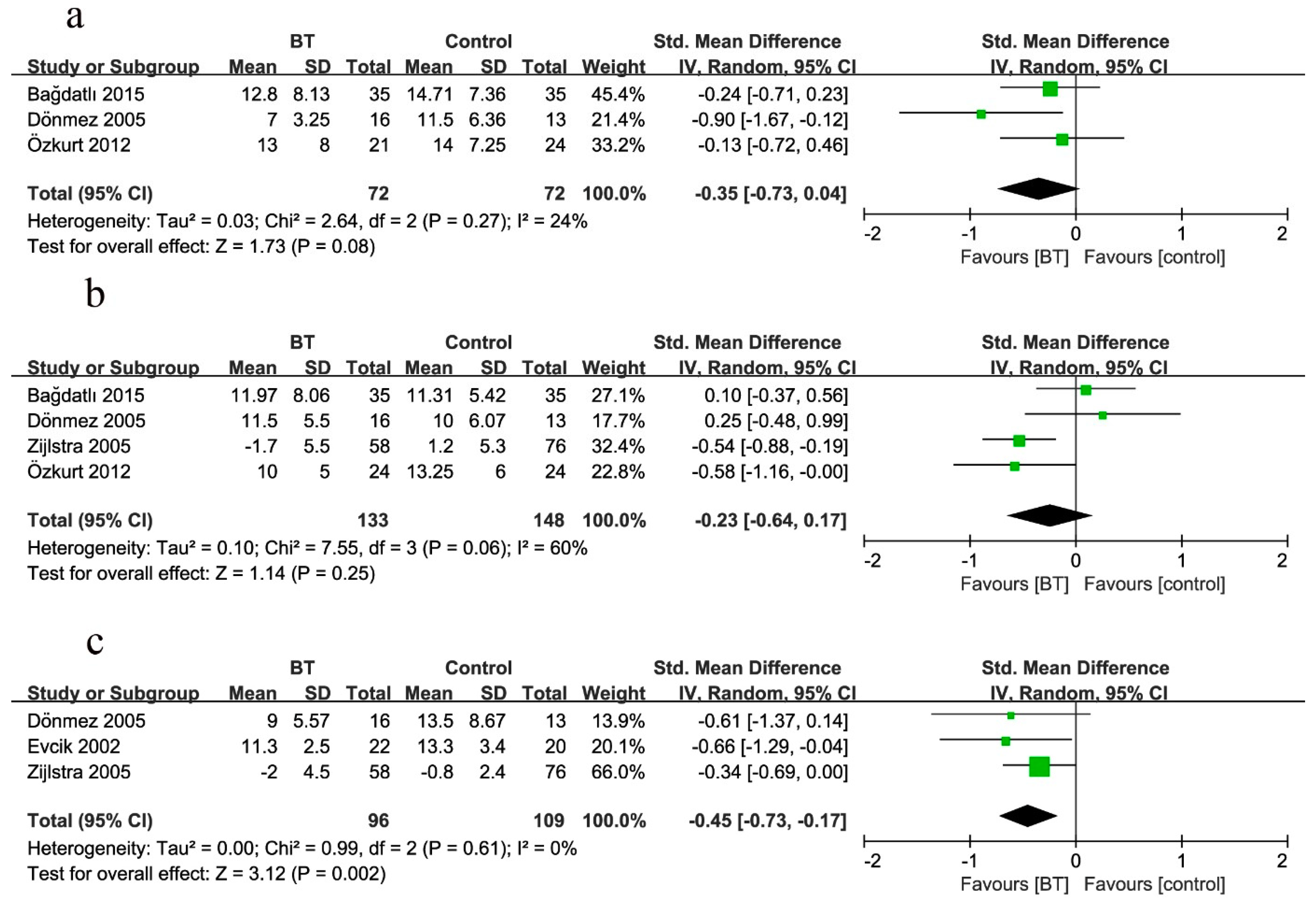
Beck’s Depression Index
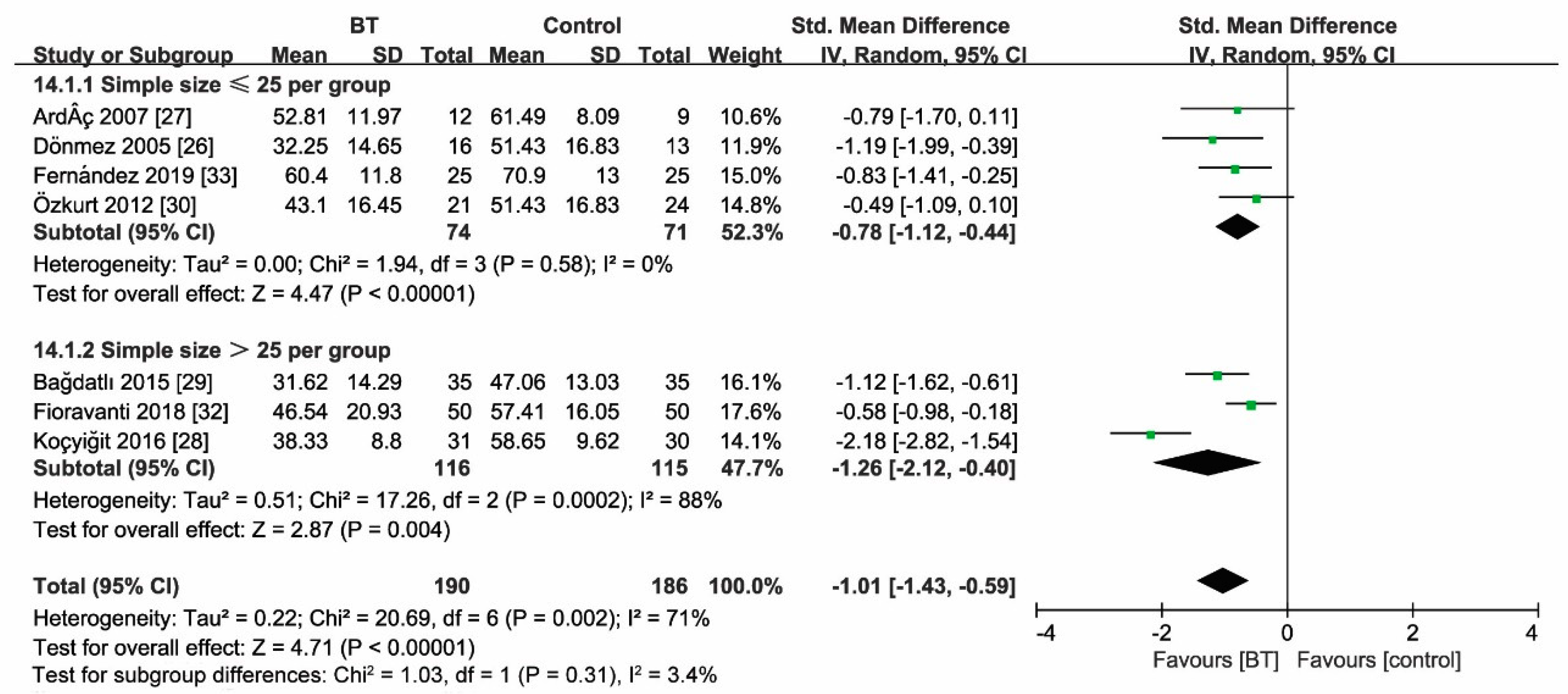
3.7. Sensitivity Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Clauw, D.J. Fibromyalgia: A clinical review. JAMA 2014, 311, 1547–1555. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Brahler, E.; Hinz, A.; Hauser, W. Fibromyalgia prevalence, somatic symptom reporting, and the dimensionality of polysymptomatic distress: Results from a survey of the general population. Arthr. Care Res. 2013, 65, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Del Giorno, R.; Skaper, S.; Paladini, A.; Varrassi, G.; Coaccioli, S. Palmitoylethanolamide in Fibromyalgia: Results from Prospective and Retrospective Observational Studies. Pain Ther. 2015, 4, 169–178. [Google Scholar] [CrossRef] [PubMed]
- McVeigh, J.G.; McGaughey, H.; Hall, M.; Kane, P. The effectiveness of hydrotherapy in the management of fibromyalgia syndrome: A systematic review. Rheumatol. Int. 2008, 29, 119–130. [Google Scholar] [CrossRef]
- Macfarlane, G.J.; Kronisch, C.; Dean, L.E.; Atzeni, F.; Häuser, W.; Fluß, E.; Choy, E.; Kosek, E.; Amris, K.; Branco, J.; et al. EULAR revised recommendations for the management of fibromyalgia. Ann. Rheum. Dis. 2016, 76, 318–328. [Google Scholar] [CrossRef]
- Miyamoto, G.C.; Lin, C.-W.C.; Cabral, C.M.N.; Van Dongen, J.M.; Van Tulder, M.W. Cost-effectiveness of exercise therapy in the treatment of non-specific neck pain and low back pain: A systematic review with meta-analysis. Br. J. Sports Med. 2018, 53, 172–181. [Google Scholar] [CrossRef]
- Arnold, L.M.; Bennett, R.M.; Crofford, L.J.; Dean, L.E.; Clauw, D.J.; Goldenberg, D.L.; Fitzcharles, M.-A.; Paiva, E.S.; Staud, R.; Sarzi-Puttini, P.; et al. AAPT Diagnostic Criteria for Fibromyalgia. J. Pain 2019, 20, 611–628. [Google Scholar] [CrossRef]
- Yurtkuran, M.; Celiktas, M. A randomized, controlled trial of balneotherapy in the treatment of patients with primary fibromyalgia syndrome. Phys. Med. Rehabil. Kurortmed. 1996, 6, 109–112. [Google Scholar] [CrossRef]
- Sukenik, S.; Flusser, D.; Abu-Shakra, M. The Role of Spa Therapy in Various Rheumatic Diseases. Rheum. Dis. Clin. N. Am. 1999, 25, 883–897. [Google Scholar] [CrossRef]
- Eroksuz, R.; Erol Forestier, F.B.; Karaaslan, F.; Forestier, R.; Issever, H.; Erdogan, N.; Karagulle, M.Z.; Donmez, A. Comparison of intermittent and consecutive balneological outpatient treatment (hydrotherapy and peloidotherapy) in fibromyalgia syndrome: A randomized, single-blind, pilot study. Int. J. Biometeorol. 2020, 64, 513–520. [Google Scholar] [CrossRef]
- Rapoliene, L.; Razbadauskas, A.; Mockeviciene, D.; Varzaityte, L.; Skarbaliene, A. Balneotherapy for musculoskeletal pain: Does the mineral content matter? Int. J. Biometeorol. 2020, 64, 965–979. [Google Scholar] [CrossRef] [PubMed]
- Naumann, J.; Sadaghiani, C. Therapeutic benefit of balneotherapy and hydrotherapy in the management of fibromyalgia syndrome: A qualitative systematic review and meta-analysis of randomized controlled trials. Arthr. Res. Ther. 2014, 16, R141. [Google Scholar] [CrossRef]
- Fraioli, A.; Grassi, M.; Mennuni, G.; Geraci, A.; Petraccia, L.; Fontana, M.; Conte, S.; Serio, A. Clinical researches on the efficacy of spa therapy in fibromyalgia. A systematic review. Ann. Dell’Ist. Super. Sanità 2013, 49, 219–229. [Google Scholar]
- Verhagen, A.P.; de Vet, H.C.; de Bie, R.A.; Kessels, A.G.; Boers, M.; Knipschild, P.G. Balneotherapy for rheumatoid arthritis and osteoarthritis. Cochrane Database Syst. Rev. 2000. [Google Scholar] [CrossRef]
- Guidelli, G.M.; Tenti, S.; De Nobili, E.; Fioravanti, A. Fibromyalgia Syndrome and Spa Therapy: Myth or Reality? Clin. Med. Insights Arthr. Musculoskelet. Disord. 2012, 5, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clark, P.; et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthr. Rheum. 1990, 33, 160–172. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthr. Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Puhan, A.M.; Schünemann, H.J.; Murad, M.H.; Li, T.; Brignardello-Petersen, R.; A Singh, J.; Kessels, A.G.; Guyatt, G.H. A GRADE Working Group approach for rating the quality of treatment effect estimates from network meta-analysis. BMJ 2014, 349, g5630. [Google Scholar] [CrossRef]
- Deeks, J.J.; Higgins, J.P.T.; Altman, D.G. Analysing Data and Undertaking Meta-Analyses. In Cochrane Handbook for Systematic Review of Interventions; Higgins, J.P.T., Ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2011; pp. 243–296. [Google Scholar]
- Buskila, D.; Abu-Shakra, M.; Neumann, L.; Odes, L.; Shneider, E.; Flusser, D.; Sukenik, S. Balneotherapy for fibromyalgia at the Dead Sea. Rheumatol. Int. 2001, 20, 105–108. [Google Scholar] [CrossRef]
- De Andrade, S.C.; de Carvalho, R.F.; Soares, A.S.; de Abreu Freitas, R.P.; de Medeiros Guerra, L.M.; Vilar, M.J. Thalassotherapy for fibromyalgia: A randomized controlled trial comparing aquatic exercises in sea water and water pool. Rheumatol. Int. 2008, 29, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Evcik, D.; Kızılay, B.; Gökçen, E. The effects of balneotherapy on fibromyalgia patients. Rheumatol. Int. 2002, 22, 56–59. [Google Scholar] [CrossRef] [PubMed]
- Dönmez, A.; Karagülle, M.Z.; Tercan, N.; Dinler, M.; Issever, H.; Turan, M.; Karagülle, M. SPA therapy in fibromyalgia: A randomised controlled clinic study. Rheumatol. Int. 2005, 26, 168–172. [Google Scholar] [CrossRef] [PubMed]
- Ardıç, F.; Özgen, M.; Aybek, H.; Rota, S.; Çubukçu, D.; Gökgöz, A. Effects of balneotherapy on serum IL-1, PGE2 and LTB4 levels in fibromyalgia patients. Rheumatol. Int. 2006, 27, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Kocyigit, B.F.; Gur, A.; Altindag, O.; Akyol, A.; Gursoy, S. Comparison of education and balneotherapy efficacy in patients with fibromyalgia syndrome: A randomized, controlled clinical study. Agri 2016, 28, 72–78. [Google Scholar] [CrossRef]
- Bağdatlı, A.O.; Donmez, A.; Eröksüz, R.; Bahadır, G.; Turan, M.; Erdoğan, N. Does addition of ‘mud-pack and hot pool treatment’ to patient education make a difference in fibromyalgia patients? A randomized controlled single blind study. Int. J. Biometeorol. 2015, 59, 1905–1911. [Google Scholar] [CrossRef] [PubMed]
- Özkurt, S.; Dönmez, A.; Karagülle, M.Z.; Uzunoglu, E.; Turan, M.; Erdoğan, N. Balneotherapy in fibromyalgia: A single blind randomized controlled clinical study. Rheumatol. Int. 2011, 32, 1949–1954. [Google Scholar] [CrossRef]
- Fioravanti, A.; Perpignano, G.; Tirri, G.; Cardinale, G.; Gianniti, C.; Lanza, C.E.; Loi, A.; Tirri, E.; Sfriso, P.; Cozzi, F. Effects of mud-bath treatment on fibromyalgia patients: A randomized clinical trial. Rheumatol. Int. 2007, 27, 1157–1161. [Google Scholar] [CrossRef]
- Fioravanti, A.; Manica, P.; Bortolotti, R.; Cevenini, G.; Tenti, S.; Paolazzi, G. Is balneotherapy effective for fibromyalgia? Results from a 6-month double-blind randomized clinical trial. Clin. Rheumatol. 2018, 37, 2203–2212. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Fernández, M.R.; Calvo-Ayuso, N.; Martínez-Reglero, C.; Salgado-Barreira, Á.; López-Álvarez, J.L.M. Efficacy of baths with mineral-medicinal water in patients with fibromyalgia: A randomized clinical trial. Int. J. Biometeorol. 2019, 63, 1161–1170. [Google Scholar] [CrossRef] [PubMed]
- Zijlstra, T.R.; Van De Laar, M.A.F.J.; Moens, H.J.B.; Taal, E.; Zakraoui, L.; Rasker, J.J. Spa treatment for primary fibromyalgia syndrome: A combination of thalassotherapy, exercise and patient education improves symptoms and quality of life. Rheumatology 2005, 44, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Häuser, W.; Ablin, J.; Perrot, S.; Fitzcharles, M.-A. Management of fibromyalgia: Practical guides from recent evidence-based guidelines. Pol. Arch. Intern. Med. 2017, 127, 47–56. [Google Scholar] [CrossRef]
- Burckhardt, C.S.; Clark, S.R.; Bennett, R.M. The fibromyalgia impact questionnaire: Development and validation. J. Rheumatol. 1991, 18, 728–733. [Google Scholar]
- Altan, L.; Bingöl, U.; Aykaç, M.; Koç, Z.; Yurtkuran, M. Investigation of the effects of pool-based exercise on fibromyalgia syndrome. Rheumatol. Int. 2003, 24, 272–277. [Google Scholar] [CrossRef]
- Falagas, M.E.; Zarkadoulia, E.; Rafailidis, P.I. The therapeutic effect of balneotherapy: Evaluation of the evidence from randomised controlled trials. Int. J. Clin. Pract. 2009, 63, 1068–1084. [Google Scholar] [CrossRef]
- Langhorst, J.; Musial, F.; Klose, P.; Hauser, W. Efficacy of hydrotherapy in fibromyalgia syndrome—A meta-analysis of randomized controlled clinical trials. Rheumatology 2009, 48, 1155–1159. [Google Scholar] [CrossRef]
- Hedenberg-Magnusson, B.; Ernberg, M.; Alstergren, P.; Kopp, S. Effect on prostaglandin E2 and leukotriene B4 levels by local administration of glucocorticoid in human masseter muscle myalgia. Acta Odontol. Scand. 2002, 60, 29–36. [Google Scholar] [CrossRef]
- Hauser, W.; Ablin, J.; Fitzcharles, M.A.; Littlejohn, G.; Luciano, J.V.; Usui, C.; Walitt, B. Fibromyalgia. Nat. Rev. Dis. Primers 2015, 1, 15022. [Google Scholar] [CrossRef]
- Varrassi, G.; Pergolizzi, J.V.; Dowling, P.; Paladini, A. Ibuprofen Safety at the Golden Anniversary: Are all NSAIDs the Same? A Narrative Review. Adv. Ther. 2020, 37, 61–82. [Google Scholar] [CrossRef] [PubMed]
- O’Hare, J.P.; Heywood, A.; Summerhayes, C.; Lunn, G.; Evans, J.M.; Walters, G.; Corrall, R.J.; Dieppe, A.P. Observations on the effect of immersion in Bath spa water. BMJ 1985, 291, 1747–1751. [Google Scholar] [CrossRef] [PubMed]
- Fioravanti, A.; Cantarini, L.; Guidelli, G.M.; Galeazzi, M. Mechanisms of action of spa therapies in rheumatic diseases: What scientific evidence is there? Rheumatol. Int. 2011, 31, 1–8. [Google Scholar] [CrossRef]
- Becker, B.E. The Biologic Aspects of Hydrotherapy. J. Back Musculoskelet. Rehabilit. 1994, 4, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Joung, J.-Y.; Lee, N.-H.; Son, C.-G. An Evolutionary Theory to Explain the Mechanism of Pain Control by Acupuncture Therapy. J. Altern. Complement. Med. 2018, 24, 743–744. [Google Scholar] [CrossRef]
- Mooventhan, A.; Nivethitha, L. Scientific evidence-based effects of hydrotherapy on various systems of the body. N. Am. J. Med. Sci. 2014, 6, 199–209. [Google Scholar] [CrossRef]
- Bender, T.; Bariska, J.; Vághy, R.; Gomez, R.; Kovács, I. Effect of Balneotherapy on the Antioxidant System—A Controlled Pilot Study. Arch. Med. Res. 2007, 38, 86–89. [Google Scholar] [CrossRef]
- Rekatsina, M.; Paladini, A.; Piroli, A.; Zis, P.; Pergolizzi, J.V.; Varrassi, G. Pathophysiology and Therapeutic Perspectives of Oxidative Stress and Neurodegenerative Diseases: A Narrative Review. Adv. Ther. 2020, 37, 113–139. [Google Scholar] [CrossRef] [PubMed]
- Morer, C.; Roques, C.-F.; Françon, A.; Forestier, R.; Maraver, F. The role of mineral elements and other chemical compounds used in balneology: Data from double-blind randomized clinical trials. Int. J. Biometeorol. 2017, 61, 2159–2173. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Step | Search Algorithm | Items Found |
|---|---|---|---|
| PubMed | #1 | “fibromyalgia” [Mesh] | 8416 |
| #2 | “musculoskeletal disease” | 1718 | |
| #3 | “chronic pain syndrome” | 675 | |
| #4 | “FMS” | 9012 | |
| #5 | #1 OR #2 OR #3 OR #4 | 21,981 | |
| #6 | “balneotherapy” | 1397 | |
| #7 | “spa therapy” | 314 | |
| #8 | “thermal water” | 298 | |
| #9 | “balneology” | 6116 | |
| #10 | “BT” | 23,370 | |
| #11 | #6) OR #7 OR #8 OR #9 OR #10 | 25,239 | |
| #12 | #5 AND #11 | 99 | |
| Embase | #1 | ‘fibromyalgia’/exp | 20,842 |
| #2 | ‘musculoskeletal disease’ | 35,937 | |
| #3 | ‘chronic pain syndrome’ | 1133 | |
| #4 | ‘FMS’ | 12,213 | |
| #5 | #1 OR #2 OR #3 OR #4 | 67,541 | |
| #6 | “balneotherapy”/exp | 16,620 | |
| #7 | “spa therapy” | 602 | |
| #8 | “thermal water” | 484 | |
| #9 | “balneology” | 1471 | |
| #10 | “BT” | 35,106 | |
| #11 | #6 OR #7 OR #8 OR #9 OR #10 | 52,736 | |
| #12 | #5 AND #11 | 434 | |
| Cochrane | #1 | MeSH descriptor: [fibromyalgia] explode all trees | 2927 |
| #2 | musculoskeletal disease: ti,ab,kw (Word variations have been searched) | 4114 | |
| #3 | chronic pain syndrome: ti,ab,kw (Word variations have been searched) | 280 | |
| #4 | FMS: ti,ab,kw (Word variations have been searched) | 649 | |
| #5 | #1 or #2 or #3 or #4 | 7576 | |
| #6 | MeSH descriptor: [balneotherapy] explode all trees | 261 | |
| #7 | spa therapy: ti,ab,kw (Word variations have been searched) | 122 | |
| #8 | thermal water: ti,ab,kw (Word variations have been searched) | 79 | |
| #9 | nalneology: ti,ab,kw (Word variations have been searched) | 211 | |
| #10 | BT: ti,ab,kw (Word variations have been searched) | 1373 | |
| #11 | #6 or #7 or #8 or #9 or #10 | 1848 | |
| #12 | #5 and #11 restricted as clinical trials | 52 | |
| Medline | #1 | “fibromyalgia” | 6926 |
| #2 | “musculoskeletal disease” | 6294 | |
| #3 | “chronic pain syndrome” | 329 | |
| #4 | “FMS” | 7109 | |
| #5 | fibromyalgia OR musculoskeletal disease OR chronic pain syndrome OR FMS | 26,976 | |
| #6 | “balneotherapy” | 472 | |
| #7 | “spa therapy” | 273 | |
| #8 | “thermal water” | 2131 | |
| #9 | “nalneology” | 562 | |
| #10 | “BT” | 21,713 | |
| #11 | nalneotherapy OR spa therapy OR thermal water OR balneology OR BT | 38,850 | |
| #12 | #5 and #11 | 91 | |
| PsycINFO | #1 | “fibromyalgia” | 46 |
| #2 | “musculoskeletal disease” | 26 | |
| #3 | “chronic pain syndrome” | 47 | |
| #4 | “FMS” | 19 | |
| #5 | fibromyalgia OR musculoskeletal disease OR chronic pain syndrome OR FMS | 116 | |
| #6 | “nalneotherapy” | 0 | |
| #7 | “spa therapy” | 1 | |
| #8 | “thermal water” | 13 | |
| #9 | “nalneology” | 1 | |
| #10 | “BT” | 0 | |
| #11 | nalneotherapy OR spa therapy OR thermal water OR balneology OR BT | 15 | |
| #12 | #5 and #11 | 1 | |
| Clinicaltrials.gov | #1 | “fibromyalgia” | 958 |
| #2 | “musculoskeletal disease” | 17,031 | |
| #3 | “chronic pain syndrome” | 44 | |
| #4 | “FMS” | 1026 | |
| #5 | fibromyalgia OR musculoskeletal disease OR Chronic pain syndrome OR FMS | 17,308 | |
| #6 | “balneotherapy” | 16 | |
| #7 | “spa therapy” | 22 | |
| #8 | “thermal water” | 3 | |
| #9 | “balneology” | 6 | |
| #10 | “BT” | 45 | |
| #11 | balneotherapy OR spa therapy OR thermal water OR balneology OR BT | 107 | |
| #12 | balneotherapy OR spa therapy OR thermal water OR balneology OR BT|fibromyalgia OR musculoskeletal disease OR chronic pain syndrome OR FMS | 207 |
| Studies | Country | Age (y) | Female/Male | Sample Size (n) | Duration | Follow-Up (w) | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| BT | con | BT | con | BT | con | BT | con | |||
| Fioravanti et al., 2018 [32] | Italy | 56.16 ± 8.74 | 55.9 ± 6.61 | 48/2 | 47/3 | 50 | 50 | 16.02 ± 12.58 m | 15.08 ± 10.87 m | 24 |
| Fernández et al., 2019 [33] | Spain | 52.4 ± 8.6 | 53.4 ± 11.3 | 23/2 | 25/0 | 25 | 25 | NA | NA | 12 |
| Dönmez et al., 2005 [26] | Turkey | 43.3 ± 7.5 | 43.1 ± 6.9 | NA | NA | 16 | 13 | 11.5 ± 8.5 y | 11.8 ± 7.5 y | 36 |
| Özkurt et al., 2012 [30] | Italy | 50.8 ± 6 | 46.87 ± 8.8 | 21/0 | 24/0 | 21 | 24 | 12.9 ± 7 y | 11.29 ± 6.2 y | 12 |
| Zijlstra et al., 2005 [34] | The Netherlands | 48 | 47 | 55/3 | 73/3 | 58 | 76 | 10 m | 10 m | 48 |
| Bağdatlı et al., 2015 [29] | Turkey | 45.17 ± 9.09 | 42.77 ± 9.59 | 35/0 | 35/0 | 35 | 35 | 8.83 ± 4.74 y | 8.37 ± 5.49 y | 12 |
| Evcik et al., 2002 [25] | Turkey | 42 ± 6.8 | 41.5 ± 7.1 | 16/6 | 15/5 | 22 | 20 | 15.5 ± 7.2 m | 14.1 ± 8.7 m | 24 |
| Ardıç et al., 2007 [27] | Turkey | 43.5 ± 10.2 | 48.8 ± 8.8 | NA | NA | 12 | 9 | 23.4 ± 21.5 m | 30.6 ± 28.6 m | 3 |
| Yurtkuran et al., 1996 [8] | Turkey | 37.5 | 33.4 | 19/1 | 18/2 | 20 | 20 | NA | NA | 6 |
| Fioravanti et al., 2007 [31] | Italy | 46.2 ± 10.5 | 48.6 ± 9.4 | 39/1 | 39/1 | 40 | 40 | 2.21 ± 1.35 y | 2.30 ± 1.42 y | 16 |
| Koçyiğit et al., 2016 [28] | Turkey | 42.45 ± 9.93 | 41.77 ± 10.5 | 31/0 | 30/0 | 31 | 30 | 73.65 ± 59.15 m | 69.40 ± 40.1 m | 24 |
| Studies | Intervention | Duration (min) | Sessions (w) | Temperature (°C) | Ingredients | |
|---|---|---|---|---|---|---|
| BT | con | |||||
| Fioravanti et al., 2018 [32] | Vetriolo’s water | Tap water | 15 | 2 | 36 | Highly mineralized, pH 5.7, sulfate, calcium, magnesium, and iron |
| Fernández et al., 2019 [33] | Bicarbonate sodium water | Pharmacological | 30 | 2 | 38 | Medium mineralization, alkaline, lithic, fluorinated, silicated |
| Dönmez et al., 2005 [26] | Thermal water | Pharmacological | 20 | 2 | 36 ± 1 | Sodium, chlorine, bicarbonate and fluoride |
| Özkurt et al., 2012 [30] | Thermal baths | Pharmacological | 20 | 2 | 36 ± 1 | Sodium, chloride, and calcium with a total mineralization of 3367 mg/L |
| Zijlstra et al., 2005 [34] | Seawater | NA | NA | 21/2 | NA | NA |
| Bağdatlı et al., 2015 [29] | Pool baths and mud pack | Exercise, education, and pharmacological | 20 | 2 | 38 | NA |
| Evcik et al., 2002 [25] | Thermal baths | Pharmacological and exercise | 20 | 3 | 36 | NA |
| Ardıç et al., 2007 [27] | Thermal pool water | Exercise or walking | 20 | 3 | 36 | NA |
| Yurtkuran et al., 1996 [8] | Therapeutic pool | Relaxation exercises | 20 | 2 | 37 | HCO3−, Cl−, F−, SO4−2, Ca+2, Mg+2, K+, Li+1 |
| Fioravanti et al., 2007 [31] | Mud packs and thermal baths | Pharmacological | 15 | 2 | 37–38 | NA |
| Koçyiğit et al., 2016 [28] | Thermomineral water | Education | 20 | 4 | 34.8 | Na, K, Mg, Ca, F, CI, Bromur, I, NO2, NO3, SO4, HCO3, S, HPO4 |
| Outcome | Certainty Assessment | No. of Patients | Effect | Certainty | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | Balneotherapy | Control | Relative(95% CI) | Absolute (95% CI) | ||
| Pain at 2 weeks | 5 | Randomized trials | Serious | Very serious | Not serious | Not serious | None | 138 | 137 | - | SMD 0.92 lower (1.13 lower to 0.53 lower) | ⨁◯◯◯ VERY LOW |
| Pain at 3 months | 6 | Randomized trials | Serious | Not serious | Not serious | Not serious | None | 211 | 228 | - | SMD 0.45 lower (0.73 lower to 0.16 lower) | ⨁⨁⨁◯ MODERATE |
| Pain at 6 months | 5 | Randomized trials | Serious | Serious | Not serious | Not serious | None | 177 | 189 | - | SMD 0.7 lower (1.34 lower to 0.05 lower) | ⨁⨁◯◯ LOW |
| FIQ at 2 weeks | 7 | Randomized trials | Serious | Serious | Not serious | Not serious | None | 190 | 186 | - | SMD 1.01 lower (1.43 lower to 0.59 lower) | ⨁⨁◯◯ LOW |
| FIQ at 3 months | 7 | Randomized trials | Serious | Serious | Not serious | Not serious | None | 236 | 253 | - | SMD 0.64 lower (0.95 lower to 0.33 lower) | ⨁⨁◯◯ LOW |
| FIQ at 6 months | 4 | Randomized trials | Serious | Very serious | Not serious | Not serious | None | 155 | 169 | - | SMD 0.59 lower (0.91 lower to 0.27 lower) | ⨁◯◯◯ VERY LOW |
| TPC at 2 weeks | 3 | Randomized trials | Serious | Very serious | Not serious | Not serious | None | 57 | 57 | - | SMD 0.9 lower (2.02 lower to 0.23 higher) | ⨁◯◯◯ VERY LOW |
| TPC at 3 months | 4 | Randomized trials | Serious | Not serious | Not serious | Not serious | None | 126 | 143 | - | SMD 0.47 lower (0.71 lower to 0.22 lower) | ⨁⨁⨁◯ MODERATE |
| TPC at 6 months | 4 | Randomized trials | Serious | Very serious | Not serious | Not serious | None | 127 | 139 | - | SMD 0.89 lower (1.85 lower to 0.07 higher) | ⨁◯◯◯ VERY LOW |
| BDI at 2 weeks | 4 | Randomized trials | Serious | Not serious | Not serious | Not serious | None | 84 | 81 | - | SMD 0.32 lower (0.63 lower to 0.01 lower) | ⨁⨁⨁◯ MODERATE |
| BDI at 3 months | 4 | Randomized trials | Serious | Serious | Not serious | Not serious | None | 133 | 148 | - | SMD 0.23 lower (0.64 lower to 0.17 higher) | ⨁⨁◯◯ LOW |
| BDI at 6 months | 3 | Randomized trials | Serious | Not serious | Not serious | Not serious | None | 96 | 109 | - | SMD 0.45 lower (0.73 lower to 0.17 lower) | ⨁⨁⨁◯ MODERATE |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cao, C.-F.; Ma, K.-L.; Li, Q.-L.; Luan, F.-J.; Wang, Q.-B.; Zhang, M.-H.; Viswanath, O.; Myrcik, D.; Varrassi, G.; Wang, H.-Q. Balneotherapy for Fibromyalgia Syndrome: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 1493. https://doi.org/10.3390/jcm10071493
Cao C-F, Ma K-L, Li Q-L, Luan F-J, Wang Q-B, Zhang M-H, Viswanath O, Myrcik D, Varrassi G, Wang H-Q. Balneotherapy for Fibromyalgia Syndrome: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2021; 10(7):1493. https://doi.org/10.3390/jcm10071493
Chicago/Turabian StyleCao, Chun-Feng, Kun-Long Ma, Qian-Lu Li, Fu-Jun Luan, Qun-Bo Wang, Ming-Hua Zhang, Omar Viswanath, Dariusz Myrcik, Giustino Varrassi, and Hai-Qiang Wang. 2021. "Balneotherapy for Fibromyalgia Syndrome: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 10, no. 7: 1493. https://doi.org/10.3390/jcm10071493
APA StyleCao, C.-F., Ma, K.-L., Li, Q.-L., Luan, F.-J., Wang, Q.-B., Zhang, M.-H., Viswanath, O., Myrcik, D., Varrassi, G., & Wang, H.-Q. (2021). Balneotherapy for Fibromyalgia Syndrome: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 10(7), 1493. https://doi.org/10.3390/jcm10071493