
Long-Term Outcomes of Abdominal Wall Reconstruction with Expanded Polytetrafluoroethylene Mesh in Pediatric Liver Transplantation

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
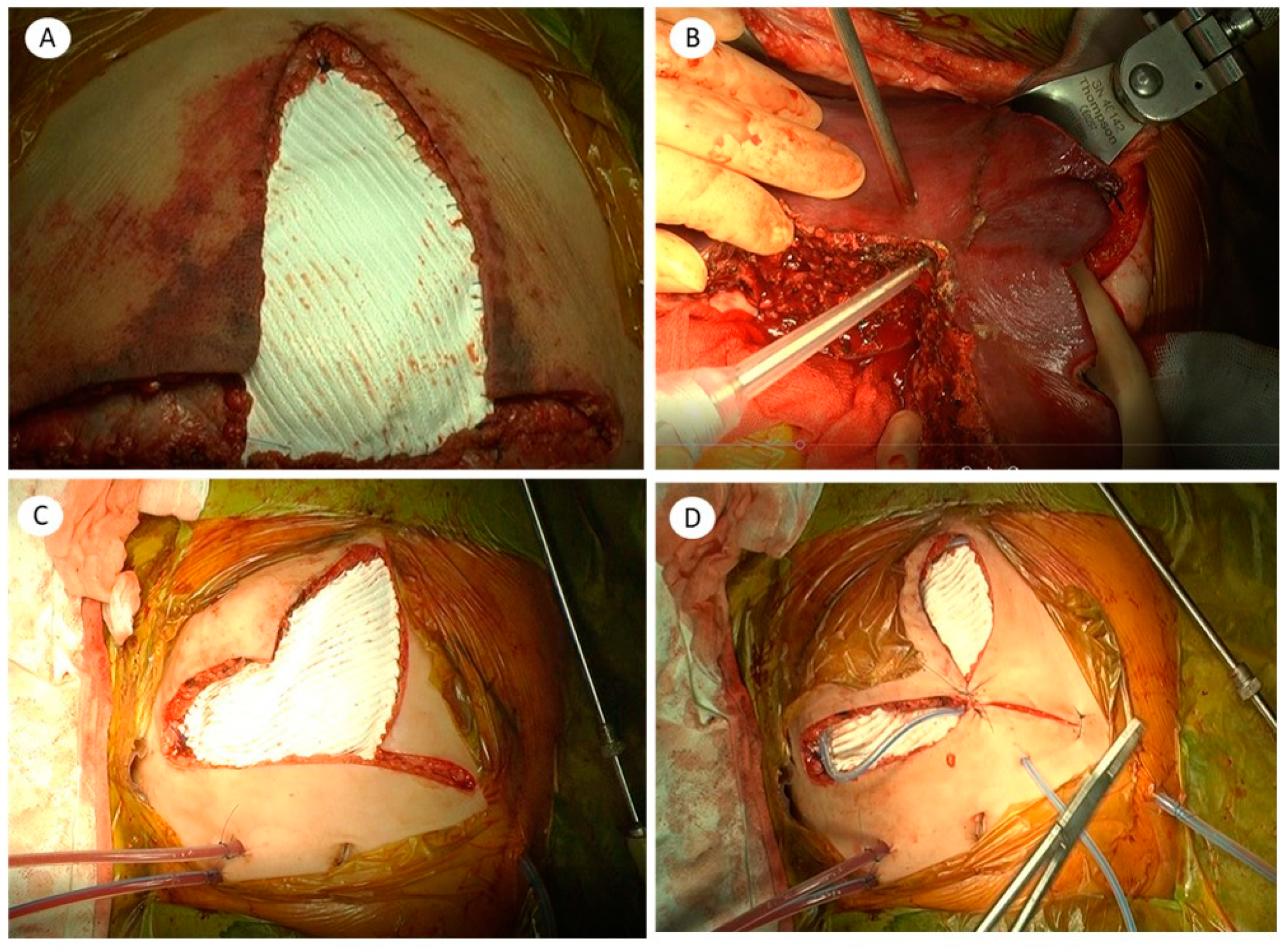
2.1. Surgical Technique for Abdominal Wall Reconstruction with ePTFE (Gore-Tex)
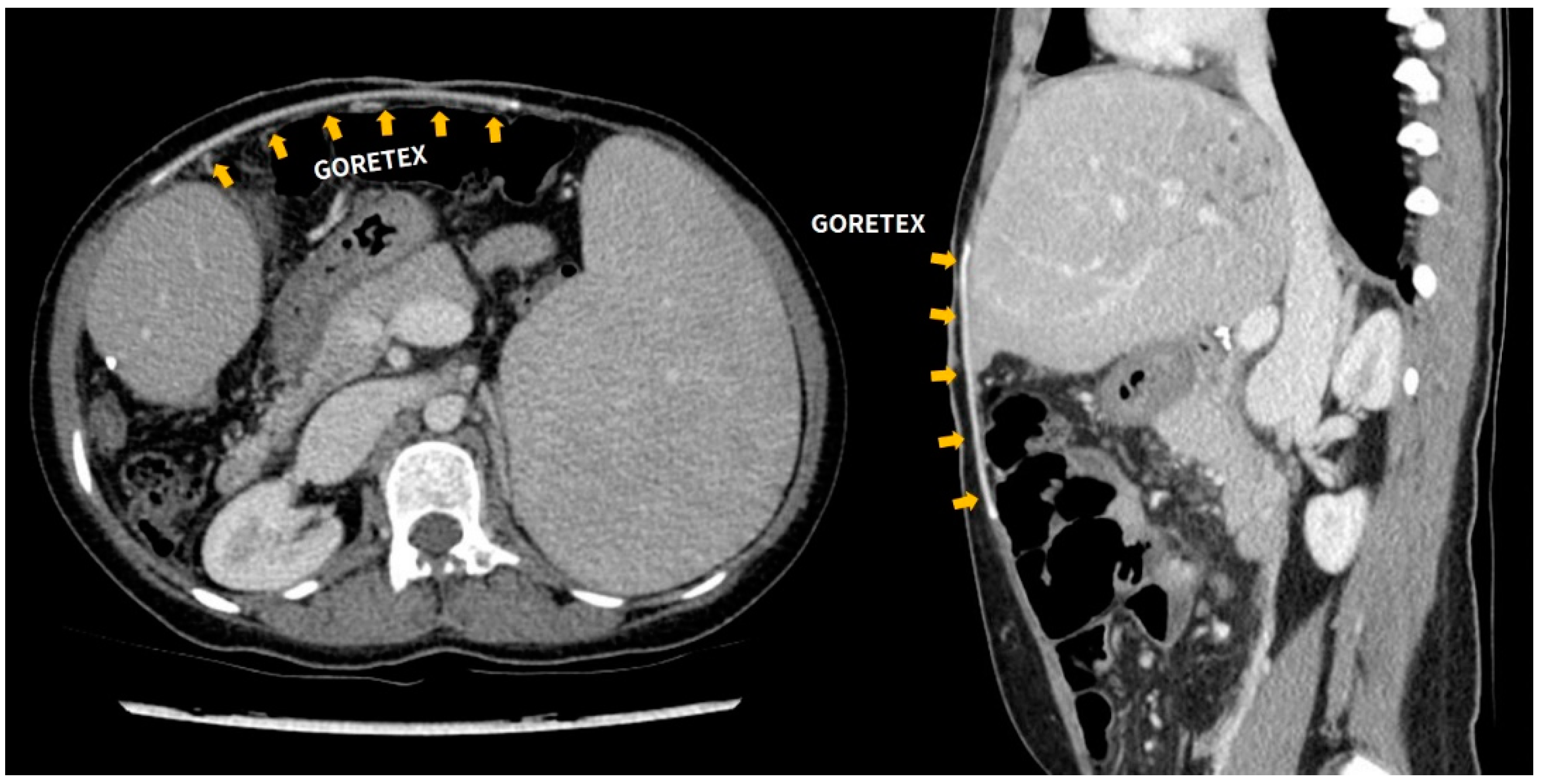
2.2. Postoperative Evaluation and Follow-up after LT
2.3. Statistical Analyses
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yamada, N.; Sanada, Y.; Hirata, Y.; Okada, N.; Wakiya, T.; Ihara, Y.; Miki, A.; Kaneda, Y.; Sasanuma, H.; Urahashi, T.; et al. Selection of living donor liver grafts for patients weighing 6 kg or less. Liver Transplant. 2015, 21, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Alim, A.; Erdogan, Y.; Yuzer, Y.; Tokat, Y.; Oezcelik, A. Graft-to-recipient weight ratio threshold adjusted to the model for end-stage liver disease score for living donor liver transplantation. Liver Transplant. 2016, 22, 1643–1648. [Google Scholar] [CrossRef] [PubMed]
- Dahm, F.; Georgiev, P.; Clavien, P.-A. Small-for-Size Syndrome after Partial Liver Transplantation: Definition, Mechanisms of Disease and Clinical Implications. Arab. Archaeol. Epigr. 2005, 5, 2605–2610. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, H.D.; Liu, Z.W.; Cashman, S.; Fusai, G.K. Small for size syndrome following living donor and split liver transplantation. World J. Gastrointest. Surg. 2010, 2, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.-S.; Pruett, T.L.; Jones, R.S. Study of Donor-Recipient Liver Size Match for Transplantation. Ann. Surg. 1994, 219, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Levesque, E.; Duclos, J.; Ciacio, O.; Adam, R.; Castaing, D.; Vibert, E. Influence of larger graft weight to recipient weight on the post-liver transplantation course. Clin. Transplant. 2013, 27, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Leal, A.J.G.; Tannuri, A.C.A.; Belon, A.R.; Guimarães, R.R.N.; Coelho, M.C.M.; Gonçalves, J.D.O.; Sokol, S.S.; De Melo, E.S.; Otoch, J.P.; Tannuri, U. A simplified experimental model of large-for-size liver transplantation in pigs. Clinics 2013, 68, 1152–1156. [Google Scholar] [CrossRef]
- Moreira, D.D.A.R.; Tannuri, A.C.A.; Belon, A.R.; Coelho, M.C.M.; Gonçalves, J.O.; Serafini, S.; Lima, F.R.; Agostini, L.O.; Guimarães, R.R.; Tannuri, U. Large-for-size liver transplantation: A flowmetry study in pigs. J. Surg. Res. 2014, 189, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Biancofiore, G.; Bindi, M.L.; Romanelli, A.M.; Bisà, M.; Boldrini, A.; Consani, G.; Filipponi, F.; Mosca, F. Postoperative Intra-abdominal Pressure and Renal Function After Liver Transplantation. Arch. Surg. 2003, 138, 703–706. [Google Scholar] [CrossRef] [PubMed]
- Fukazawa, K.; Nishida, S. Size mismatch in liver transplantation. J. Hepato-Biliary-Pancreatic Sci. 2016, 23, 457–466. [Google Scholar] [CrossRef] [PubMed]
- Jafri, M.A.; Tevar, A.D.; Lucia, M.; Thambi-Pillai, T.; Karachristos, A.; Trumbull, L.; Buell, J.F.; Thomas, M.J.; Hanaway, M.J.; Woodle, E.S.; et al. Temporary silastic mesh closure for adult liver transplantation: A safe alternative for the difficult abdomen. Liver Transplant. 2007, 13, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Lafosse, A.; De Magnée, C.; Brunati, A.; Bayet, B.; Vanwijck, R.; Manzanares, J.; Reding, R. Combination of tissue expansion and porcine mesh for secondary abdominal wall closure after pediatric liver transplantation. Pediatr. Transplant. 2011, 16, E150–E152. [Google Scholar] [CrossRef] [PubMed]
- Seaman, D.S.; Newell, K.A.; Piper, J.B.; Bruce, D.S.; Woodle, E.S.; Cronin, D.C.; Alonso, E.M.; Whitington, P.F.; Thistlethwaite, J.R.; Millis, J.M. Use of polytetrafluoroethylene patch for temporary wound closure after pediatric liver transplantation. Transplantation 1996, 62, 1034–1036. [Google Scholar] [CrossRef] [PubMed]
- Kirkpatrick, A.W.; The Pediatric Guidelines Sub-Committee for the World Society of the Abdominal Compartment Syndrome; Roberts, D.J.; De Waele, J.; Jaeschke, R.; Malbrain, M.L.N.G.; De Keulenaer, B.; Duchesne, J.; Bjorck, M.; Leppaniemi, A.; et al. Intra-abdominal hypertension and the abdominal compartment syndrome: Updated consensus definitions and clinical practice guidelines from the World Society of the Abdominal Compartment Syndrome. Intensive Care Med. 2013, 39, 1190–1206. [Google Scholar] [CrossRef] [PubMed]
- Pearson, E.G.; Rollins, M.D.; Vogler, S.A.; Mills, M.K.; Lehman, E.L.; Jacques, E.; Barnhart, D.C.; Scaife, E.R.; Meyers, R.L. Decompressive laparotomy for abdominal compartment syndrome in children: Before it is too late. J. Pediatr. Surg. 2010, 45, 1324–1329. [Google Scholar] [CrossRef] [PubMed]
- Addeo, P.; Noblet, V.; Naegel, B.; Bachellier, P. Large-for-Size Orthotopic Liver Transplantation: A Systematic Review of Definitions, Outcomes, and Solutions. J. Gastrointest. Surg. 2020, 24, 1192–1200. [Google Scholar] [CrossRef] [PubMed]
- Akdur, A.; Kirnap, M.; Ozcay, F.; Sezgin, A.; Soy, H.E.A.; Yarbug, F.K.; Yildirim, S.; Moray, G.; Arslan, G.; Haberal, M. Large-for-size liver transplant: A single-center experience. Exp. Clin. Transplant. 2015, 13, 108–110. [Google Scholar] [PubMed]
- Giele, H.; Vaidya, A.; Reddy, S.; Vrakas, G.; Friend, P. Current state of abdominal wall transplantation. Curr. Opin. Organ. Transplant. 2016, 21, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Divkovic, D.; Kvolik, S.; Sipl, M.; Sego, K.; Pušeljić, S.; Rakipovic-Stojanovic, A.; Kovačić, B. A successful early gore-tex reconstruction of an abdominal wall defect in a neonate with Cantrell pentalogy: A case report and literature review. Clin. Case Rep. 2014, 3, 19–23. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Case | Sex | Age (mo) at LT | Type of LT | Graft Type | Diagnosis | Blood Type | Retransplantation | PELD | CTP Score | Previous Operation | Ascites before LT |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | F | 12 | DDLT | Whole liver | Glycogen storage disease | AB+ | Y | 6.43 | A | Y | N |
| 2 | M | 6 | DDLT (SLT) | Lt.lat. | Biliary atresia | AB+ | Y | 16.67 | B | Y | N |
| 3 | M | 9 | LDLT | Lt.lat. | Fulminant hepatic failure | B+ | N | 57.72 | C | N | N |
| 4 | F | 17 | LDLT | Rt.liver | Urea cycle metabolism disorder | B+ | Y | 25.04 | B | Y | N |
| 5 | M | 8 | LDLT | Lt.lat. | Intrahepatic cholestasis | A+ | N | 15.05 | B | N | N |
| 6 | F | 19 | DDLT (SLT) | Lt.lat. | Biliary atresia | A+ | N | 22.45 | B | N | N |
| 7 | M | 12 | DDLT (SLT) | Lt.lat. | Biliary atresia | B+ | Y | 23.28 | C | Y | Y |
| 8 | M | 10 | DDLT (SLT) | Lt.lat. | Glycogen storage disease | B+ | N | 1.98 | A | N | N |
| 9 | F | 5 | DDLT (SLT) | Lt.lat. | Fulminant hepatic failure | B+ | N | 36.26 | C | N | Y |
| 10 | F | 144 | LDLT | Lt.liver | Choledochal cyst | A+ | Y | 11.9 | B | Y | N |
| 11 | M | 72 | DDLT (SLT) | Lt.lat. | Hyperoxaluria | A+ | Y | 10.37 | A | Y | N |
| 12 | F | 9 | LDLT | Lt.lat. | Biliary atresia | AB+ | N | 18.85 | C | Y | Y |
| 13 | F | 18 | DDLT (SLT) | Lt.lat. | Progressive familialintrahepatic cholestasis | B+ | N | 20.19 | B | N | N |
| 14 | M | 17 | DDLT (SLT) | Lt.lat. | Hyperoxaluria | B+ | N | 6.61 | A | N | N |
| 15 | M | 5 | LDLT (SLT) | Lt.lat. | Biliary atresia | O+ | Y | 36.04 | C | Y | Y |
| Case | GRWR | ICU Stay (Days) | Operative Time (Minute) | EBL (cc) | Hospital Stay (Days) | Gore-Tex Related Complication | Graft Survival | Patient Survival | OS (Days) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 1.66 | 21 | 455 | 55 | N | Y | Y | 3926 | |
| 2 | 4.19 | 43 | 300 | 50 | 61 | N | Y | Y | 3735 |
| 3 | 3.41 | 7 | 410 | 210 | 52 | N | Y | Y | 3364 |
| 4 | 1.62 | 41 | 415 | 2500 | 121 | N | Y | Y | 3111 |
| 5 | 2.27 | 11 | 415 | 530 | 16 | N | Y | Y | 2738 |
| 6 | 2.72 | 17 | 405 | 280 | 39 | N | Y | Y | 2591 |
| 7 | 3.75 | 10 | 505 | 300 | 24 | N | Y | Y | 2498 |
| 8 | 1.03 | 7 | 420 | 200 | 23 | N | Y | Y | 1816 |
| 9 | 4.44 | 17 | 325 | 620 | 17 | N | N | N | 17 |
| 10 | 0.96 | 30 | 310 | 1200 | 195 | Y † | Y | Y | 1135 |
| 11 | 1.04 | 18 | 240 | 100 | 97 | Y ‡ | Y | Y | 962 |
| 12 | 2.22 | 5 | 323 | 730 | 25 | N | Y | Y | 312 |
| 13 | 2.06 | 20 | 390 | 100 | 29 | N | Y | Y | 273 |
| 14 | 2.1 | 11 | 360 | 1000 | 32 | N | Y | Y | 150 |
| 15 | 2.6 | 9 | 210 | 300 | 40 | N | Y | Y | 124 |
| 2.42 ± 1.08 | 17.8 ± 11.4 | 365.5 ± 77.6 | 300 a (200–730) | 55.1 ± 47.1 | 2/15 13.3% | 14/15 93.3% | 14/15 93.3% | 1816 a (273–2738) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Lee, J.-M.; Yi, N.-J.; Hong, S.K.; Choi, Y.; Hong, K.; Han, E.S.; Lee, K.-W.; Suh, K.-S. Long-Term Outcomes of Abdominal Wall Reconstruction with Expanded Polytetrafluoroethylene Mesh in Pediatric Liver Transplantation. J. Clin. Med. 2021, 10, 1462. https://doi.org/10.3390/jcm10071462
Kim J, Lee J-M, Yi N-J, Hong SK, Choi Y, Hong K, Han ES, Lee K-W, Suh K-S. Long-Term Outcomes of Abdominal Wall Reconstruction with Expanded Polytetrafluoroethylene Mesh in Pediatric Liver Transplantation. Journal of Clinical Medicine. 2021; 10(7):1462. https://doi.org/10.3390/jcm10071462
Chicago/Turabian StyleKim, Jiyoung, Jeong-Moo Lee, Nam-Joon Yi, Suk Kyun Hong, YoungRok Choi, Kwangpyo Hong, Eui Soo Han, Kwang-Woong Lee, and Kyung-Suk Suh. 2021. "Long-Term Outcomes of Abdominal Wall Reconstruction with Expanded Polytetrafluoroethylene Mesh in Pediatric Liver Transplantation" Journal of Clinical Medicine 10, no. 7: 1462. https://doi.org/10.3390/jcm10071462
APA StyleKim, J., Lee, J.-M., Yi, N.-J., Hong, S. K., Choi, Y., Hong, K., Han, E. S., Lee, K.-W., & Suh, K.-S. (2021). Long-Term Outcomes of Abdominal Wall Reconstruction with Expanded Polytetrafluoroethylene Mesh in Pediatric Liver Transplantation. Journal of Clinical Medicine, 10(7), 1462. https://doi.org/10.3390/jcm10071462