
Comparing Intensive Trauma-Focused Treatment Outcome on PTSD Symptom Severity in Older and Younger Adults

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Therapies
2.4. Measures
2.5. Data Analysis
3. Results
3.1. Baseline Sample Characteristics
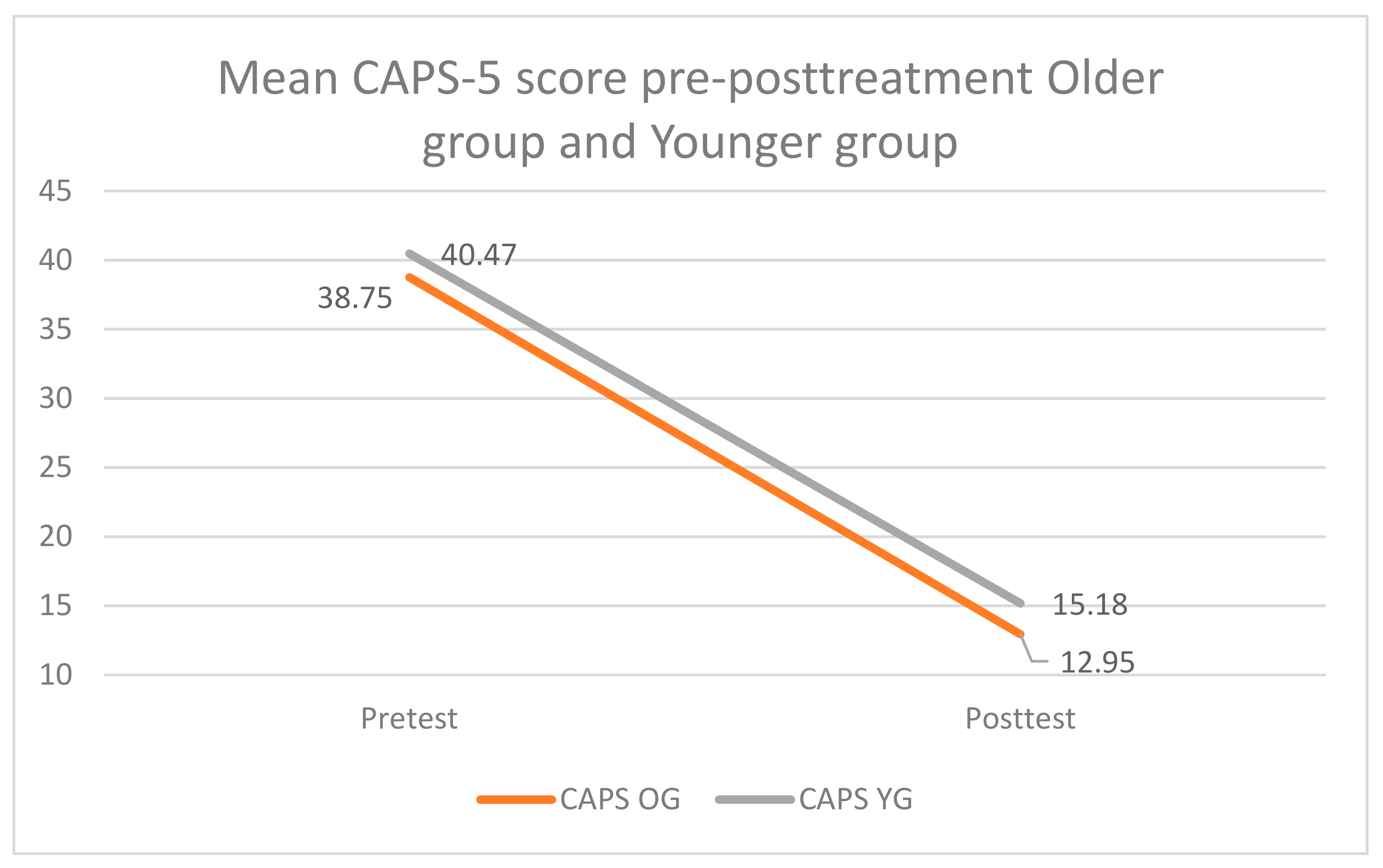
3.2. Treatment Effect from Pre- to Post-Treatment for the Total Group (n = 124)
3.3. Treatment Effect at Six-Month Follow-Up for a Subsample (n = 62)
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pietrzak, R.H.; Goldstein, R.B.; Southwick, S.M.; Grant, B.F. Prevalence and axis i comorbidity of full and partial post-traumatic stress disorder in the united states: Results from wave 2 of the national epidemiologic survey on alcohol and related conditions. J. Anxiety Disord. 2011, 25, 456–465. [Google Scholar] [CrossRef]
- Chopra, M.P.; Zhang, H.; Pless Kaiser, A.; Moye, J.A.; Llorente, M.D.; Oslin, D.W.; Spiro, A., 3rd. PTSD is a chronic, fluctuating disorder affecting the mental quality of life in older adults. Am. J. Geriatr. Psychiatry 2014, 22, 86–97. [Google Scholar] [CrossRef]
- van Zelst, W.H.; de Beurs, E.; Beekman, A.T.; van Dyck, R.; Deeg, D.D. Well-being, physical functioning, and use of health services in the elderly with PTSD and subthreshold PTSD. Int. J. Geriatr. Psychiatry 2006, 21, 180–188. [Google Scholar] [CrossRef]
- Kang, B.; Xu, H.; McConnell, E.S. Neurocognitive and psychiatric comorbidities of post-traumatic stress disorder among older veterans: A systematic review. Int. J. Geriatr. Psychiatry 2019, 34, 522–538. [Google Scholar] [CrossRef]
- Lohr, J.B.; Palmer, B.W.; Eidt, C.A.; Aailaboyina, S.; Mausbach, B.T.; Wolkowitz, O.M.; Thorp, S.R.; Jeste, D.V. Is post-traumatic stress disorder associated with premature senescence? A review of the literature. Am. J. Geriatr. Psychiatry 2015, 23, 709–725. [Google Scholar] [CrossRef]
- Dinnen, S.; Simiola, V.; Cook, J.M. Post-traumatic stress disorder in older adults: A systematic review of the psychotherapy treatment literature. Aging Ment. Health 2015, 19, 144–150. [Google Scholar] [CrossRef]
- Pless Kaiser, A.; Cook, J.M.; Glick, D.M.; Moye, J. Posttraumatic stress disorder in older adults: A conceptual review. Clin. Gerontol. 2019, 42, 359–376. [Google Scholar] [CrossRef] [PubMed]
- Kessler, E.M.; Blachetta, C. Age cues in patients’ descriptions influence treatment attitudes. Aging Ment. Health 2020, 24, 193–196. [Google Scholar] [CrossRef] [PubMed]
- Mody, L.; Miller, D.K.; McGloin, J.M.; Freeman, M.; Marcantonio, E.R.; Magaziner, J.; Studenski, S. Recruitment and retention of older adults in aging research. J. Am. Geriatr. Soc. 2008, 56, 2340–2348. [Google Scholar] [CrossRef] [PubMed]
- Thorp, S.R.; Glassman, L.H.; Wells, S.Y.; Walter, K.H.; Gebhardt, H.; Twamley, E.; Golshan, S.; Pittman, J.; Penski, K.; Allard, C.; et al. A randomized controlled trial of prolonged exposure therapy versus relaxation training for older veterans with military-related PTSD. J. Anxiety Disord. 2019, 64, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Lely, J.C.G.; Knipscheer, J.W.; Moerbeek, M.; Ter Heide, F.J.J.; van den Bout, J.; Kleber, R.J. Randomised controlled trial comparing narrative exposure therapy with present-centred therapy for older patients with post-traumatic stress disorder. Br. J. Psychiatry 2019, 214, 369–377. [Google Scholar] [CrossRef]
- Bichescu, D.; Neuner, F.; Schauer, M.; Elbert, T. Narrative exposure therapy for political imprisonment-related chronic posttraumatic stress disorder and depression. Behav. Res. Ther. 2007, 45, 2212–2220. [Google Scholar] [CrossRef] [PubMed]
- Knaevelsrud, C.; Böttche, M.; Pietrzak, R.H.; Freyberger, H.J.; Kuwert, P. Efficacy and feasibility of a therapist-guided internet-based intervention for older persons with childhood traumatization: A randomized controlled trial. Am. J. Geriatr. Psychiatry 2017, 25, 878–888. [Google Scholar] [CrossRef]
- Kline, A.C.; Cooper, A.A.; Rytwinski, N.K.; Feeny, N.C. The effect of concurrent depression on ptsd outcomes in trauma-focused psychotherapy: A meta-analysis of randomized controlled trials. Behav. Ther. 2021, 52, 250–266. [Google Scholar] [CrossRef]
- Chard, K.M.; Schumm, J.A.; Owens, G.P.; Cottingham, S.M. A comparison of OEF and OIF veterans and Vietnam veterans receiving cognitive processing therapy. J. Trauma. Stress 2010, 23, 25–32. [Google Scholar] [CrossRef]
- Sabey, A.K.; Jensen, J.; Major, S.; Zinbarg, R.; Pinsof, W. Are older adults unique? Examining presenting issues and changes in therapy across the life span. J. Appl. Gerontol. 2020, 39, 250–258. [Google Scholar] [CrossRef] [PubMed]
- Cuijpers, P.; Karyotaki, E.; Eckshtain, D.; Ng, M.Y.; Corteselli, K.A.; Noma, H.; Quero, S.; Weisz, J.R. Psychotherapy for depression across different age groups: A systematic review and meta-analysis. JAMA Psychiatry 2020, 77, 694–702. [Google Scholar] [CrossRef] [PubMed]
- Kishita, N.; Laidlaw, K. Cognitive behaviour therapy for generalized anxiety disorder: Is CBT equally efficacious in adults of working age and older adults? Clin. Psychol. Rev. 2017, 52, 124–136. [Google Scholar] [CrossRef]
- Gutner, C.A.; Suvak, M.K.; Sloan, D.M.; Resick, P.A. Does timing matter? Examining the impact of session timing on outcome. J. Consult. Clin. Psychol. 2016, 84, 1108–1115. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.W.; Taylor, G.; Drummond, P. The active ingredient in EMDR; is it traditional exposure or dual focus of attention? Clin. Psychol. Psychother. 2006, 13, 97–107. [Google Scholar] [CrossRef]
- Rosenbaum, S.; Vancampfort, D.; Steel, Z.; Newby, J.; Ward, P.B.; Stubbs, B. Physical activity in the treatment of Post-traumatic stress disorder: A systematic review and meta-analysis. Psychiatry Res. 2015, 230, 130–136. [Google Scholar] [CrossRef]
- Wagenmans, A.; Van Minnen, A.; Sleijpen, M.; De Jongh, A. The impact of childhood sexual abuse on the outcome of intensive trauma-focused treatment for PTSD. Eur. J. Psychotraumatol. 2018, 9, 1430962. [Google Scholar] [CrossRef] [PubMed]
- Van Woudenberg, C.; Voorendonk, E.M.; Bongaerts, H.; Zoet, H.A.; Verhagen, M.; Lee, C.W.; van Minnen, A.; De Jongh, A. Effectiveness of an intensive treatment programme combining prolonged exposure and eye movement desensitization and reprocessing for severe post-traumatic stress disorder. Eur. J. Psychotraumatol. 2018, 9, 1487225. [Google Scholar] [CrossRef] [PubMed]
- Böttche, M.; Kuwert, P.; Knaevelsrud, C. Posttraumatic stress disorder in older adults: An overview of characteristics and treatment approaches. Int. J. Geriatr. Psychiatry 2012, 27, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Boeschoten, M.A.; Van der Aa, N.; Bakker, A.; Ter Heide, F.J.J.; Hoofwijk, M.C.; Jongedijk, R.A.; Van Minnen, A.; Elzinga, B.M.; Olff, M. Development and evaluation of the dutch clinician-administered PTSD scale for DSM-5 (CAPS-5). Eur. J. Psychotraumatol. 2018, 9, 1546085. [Google Scholar] [CrossRef]
- Association, A.P. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Olff, M. Choosing the right instruments for psychotrauma related research. Eur. J. Psychotraumatol. 2015, 6, 30585. [Google Scholar] [CrossRef]
- Arifin, W.N. Random sampling and allocation using SPSS. Educ. Med. J. 2012, 4, 1546085. [Google Scholar] [CrossRef]
- Van Minnen, A.; Hendriks, L.; Kleine, R.; Hendriks, G.J.; Verhagen, M.; De Jongh, A. Therapist rotation: A novel approach for implementation of trauma-focused treatment in post-traumatic stress disorder. Eur. J. Psychotraumatol. 2018, 9, 1492836. [Google Scholar] [CrossRef]
- Foa, E.B.; Hembree, E.A.; Rothbaum, B.O. Prolonged Exposure Therapy for PTSD: Emotional Processing of Traumatic Experiences: Therapist Guide.; Oxford University Press: New York, NY, USA, 2007. [Google Scholar]
- De Jongh, A.; Ten Broeke, E. Handboek EMDR: Een Geprotocolleerde Behandelmethode voor de Gevolgen van Psychotrauma [Handbook EMDR: A Protocolized Treatment Method for the Consequences of Psychotrauma]; Pearson Assessment and Information B.V: Amsterdam, The Netherlands, 2013. [Google Scholar]
- Shapiro, F. Eye Movement Desesitization and Reprocessing: Basic Principles, Protocols and Procedures, 2nd ed.; Guilford Press: New York, NY, USA, 2001. [Google Scholar]
- Logie, R.D.J.; De Jongh, A. The “flashforward procedure”: Confronting the catastrophe. J. EMDR Pract. Res. 2014, 8, 25–32. [Google Scholar] [CrossRef]
- Weathers, F.W.; Blake, B.D.; Schnurr, P.P.; Kaloupek, D.G.; Marx, B.P.; Keane, T.M. The Life Events Checklist for DSM-5 (LEC-5). 2013. Available online: www.ptsd.va.gov (accessed on 14 August 2013).
- Gray, M.J.; Litz, B.T.; Hsu, J.L.; Lombardo, T.W. Psychometric properties of the life events checklist. Assessment 2004, 11, 330–341. [Google Scholar] [CrossRef]
- Lecrubier, Y.; Sheehan, D.V.; Weiller, E.; Amorim, P.; Bonora, I.; Sheehan, K.H.; Dunbar, G.C. The mini international neuropsychiatric interview (MINI). A short diagnostic structured interview: Reliability and validity according to the CIDI. Eur. Psychiatry 1997, 12, 224–231. [Google Scholar] [CrossRef]
- Van Vliet, I.M.; De Beurs, E. The MINI international neuropsychiatric interview: A brief structured diagnostic psychiatric interview for DSM-IV and ICD-10 psychiatric disorders. Tijdschr. Voor Psychiatr. 2006, 49, 393–397. [Google Scholar]
- Overbeek, T.; Schruers, K.; Griez, E. MINI: Mini International Neuropsychiatric Interview, Dutch Version 5.0.0 (DSM-IV); Maastricht Univisity: Maastricht, The Netherlands, 1999; pp. 1–15. [Google Scholar]
- Weathers, F.W.; Bovin, M.J.; Lee, D.J.; Sloan, D.M.; Schnurr, P.P.; Kaloupek, D.G.; Keane, T.M.; Marx, B.P. The clinician-administered PTSD scale for DSM-5 (CAPS-5): Development and initial psychometric evaluation in military veterans. Psychol. Assess. 2018, 30, 383–395. [Google Scholar] [CrossRef]
- Nicholson, A.A.; Densmore, M.; Frewen, P.A.; Théberge, J.; Neufeld, R.W.; McKinnon, M.C.; Lanius, R.A. The dissociative subtype of posttraumatic stress disorder: Unique resting-state functional connectivity of basolateral and centromedial amygdala complexes. Neuropsychopharmacology 2015, 40, 2317–2326. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates Inc.: Hissdale, NJ, USA, 1998. [Google Scholar]
- Schneider, B.A.; Avivi-Reich, M.; Mozuraitis, M. A cautionary note on the use of the Analysis of Covariance (ANCOVA) in classification designs with and without within-subject factors. Front. Psychol. 2015, 6, 474. [Google Scholar] [CrossRef] [PubMed]
- Field, A. Discovering Statistics Using IBM SPSS Statistics; SAGE Publications: London, UK, 2018. [Google Scholar]
- Wetherell, J.L.; Petkus, A.J.; Thorp, S.R.; Stein, M.B.; Chavira, D.A.; Campbell-Sills, L.; Craske, M.G.; Sherbourne, C.; Bystritsky, A.; Sullivan, G.; et al. Age differences in treatment response to a collaborative care intervention for anxiety disorders. Br. J. Psychiatry 2013, 203, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Labinsky, E.; Blair, W.; Yehuda, R. Longitudinal assessment of dissociation in Holocaust survivors with and without PTSD and nonexposed aged Jewish adults. Ann. N. Y. Acad. Sci. 2006, 1071, 459–462. [Google Scholar] [CrossRef] [PubMed]
- Hoeboer, C.M.; De Kleine, R.A.; Molendijk, M.L.; Schoorl, M.; Oprel, D.A.C.; Mouthaan, J.; Van der Does, W.; Van Minnen, A. Impact of dissociation on the effectiveness of psychotherapy for post-traumatic stress disorder: Meta-analysis. BJPsych Open 2020, 6, e53. [Google Scholar] [CrossRef] [PubMed]
- Mackenzie, C.S.; Reynolds, K.; Cairney, J.; Streiner, D.L.; Sareen, J. Disorder-specific mental health service use for mood and anxiety disorders: Associations with age, sex, and psychiatric comorbidity. Depress. Anxiety 2012, 29, 234–242. [Google Scholar] [CrossRef]
- Gielkens, E.M.J.; Vink, M.; Sobczak, S.; Rosowsky, E.; Van Alphen, S.P.J. EMDR in older adults with posttraumatic stress disorder. J. EMDR Pract. Res. 2018, 12, 132–141. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study | n | Mean Age | % Female | Trauma Type | Outcome Measure | Treatment Type | Number of Sessions | Outcome/Effect Sizes Cohen’s d |
|---|---|---|---|---|---|---|---|---|
| Lely et al. [11] (2019) | 33 | 63.8 | 27.3 | Mixed | CAPS | NET vs. PCT | 11 sessions | Between group 0.44, disappears at follow up |
| Thorp et al. [10] (2019) | 87 | 66.5 | 0 | War | CAPS | PE vs. Relaxation | 12 sessions | Within group 0.89, lost at 6 months follow up |
| Knaevelsrud et al. [13] (2017) | 94 | 71.4 | 64.9 | Childhood trauma | PDS | Therapist-Guided Internet-based Intervention vs. Waiting list | 6 weeks intervention program, 11 sessions | Between group 0.42 maintained at 12 months follow-up |
| Bichescu et al. [12] (2007) | 18 | 69.4 | 5.5 | Political prisoner | CIDI | C1 NET vs. C2 psychoeducation | C1 5 sessions C2 1 session | Within group 3.15 (pre treatment-6 months follow up) |
| Total OG and YG | OG | YG | Significance Level | Effect Size | |
|---|---|---|---|---|---|
| Mean CAPS score | 39.61 (SD = 7.83) | 38.75 (SD = 8.54) | 40.47 (SD = 7.02) | p = 0.23 | d = 0.22 |
| Total comorbidity rates | 74.2% | 66.1% | 82.3% | p = 0.12 | h = 0.37 |
| 1 comorbidity | 42.7% | 37.1% | 48.4% | p = 0.20 | h = 0.22 |
| 2 or more comorbidities | 31.5% | 29% | 33.9% | p = 0.56 | h = 0.11 |
| Moderate-high suicide risk | 41.9% | 38.7% | 45.2% | p = 0.47 | h = 0.12 |
| Dissociative subtype | 30.6% | 21.0% | 40.3% | p = 0.02 | h = 0.42 |
| More than 5 traumatic experiences | 80.60% | 82.30% | 79.00% | p = 0.65 | h = 0.08 |
| More than 10 traumatic experiences | 22.60% | 22.60% | 22.60% | p > 0.99 | h = 0.00 |
| Sexual abuse | 83.10% | 87.10% | 79.00% | p = 0.23 | h = 0.21 |
| Physical | 92.70% | 90.30% | 95.20% | p = 0.30 | h = 0.19 |
| Natural disasters, accidents, and victims of war | 83.10% | 85.50% | 80.60% | p = 0.47 | h = 0.06 |
| Life-threatening illness, severe suffering, sudden death | 89.50% | 90.30% | 88.70% | p = 0.77 | h = 0.03 |
| Any other stressful event, captivity, (satanic) torture | 74.20% | 74.20% | 74.20% | p > 0.99 | h = 0.00 |
| Pre-test | Post-test | FU | ||||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |
| CAPS OG | 40.06 | 9.88 | 15.90 | 14.26 | 16.10 | 15.28 |
| CAPS YG | 39.52 | 7.23 | 15.16 | 15.97 | 13.65 | 15.24 |
| CAPS total group | 39.79 | 8.59 | 15.53 | 15.02 | 14.87 | 15.19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gielkens, E.M.J.; de Jongh, A.; Sobczak, S.; Rossi, G.; van Minnen, A.; Voorendonk, E.M.; Rozendaal, L.; van Alphen, S.P.J. Comparing Intensive Trauma-Focused Treatment Outcome on PTSD Symptom Severity in Older and Younger Adults. J. Clin. Med. 2021, 10, 1246. https://doi.org/10.3390/jcm10061246
Gielkens EMJ, de Jongh A, Sobczak S, Rossi G, van Minnen A, Voorendonk EM, Rozendaal L, van Alphen SPJ. Comparing Intensive Trauma-Focused Treatment Outcome on PTSD Symptom Severity in Older and Younger Adults. Journal of Clinical Medicine. 2021; 10(6):1246. https://doi.org/10.3390/jcm10061246
Chicago/Turabian StyleGielkens, Ellen M. J., Ad de Jongh, Sjacko Sobczak, Gina Rossi, Agnes van Minnen, Eline M. Voorendonk, Linda Rozendaal, and Sebastiaan P. J. van Alphen. 2021. "Comparing Intensive Trauma-Focused Treatment Outcome on PTSD Symptom Severity in Older and Younger Adults" Journal of Clinical Medicine 10, no. 6: 1246. https://doi.org/10.3390/jcm10061246
APA StyleGielkens, E. M. J., de Jongh, A., Sobczak, S., Rossi, G., van Minnen, A., Voorendonk, E. M., Rozendaal, L., & van Alphen, S. P. J. (2021). Comparing Intensive Trauma-Focused Treatment Outcome on PTSD Symptom Severity in Older and Younger Adults. Journal of Clinical Medicine, 10(6), 1246. https://doi.org/10.3390/jcm10061246