
Conceptual Model for Using Imidazoline Derivative Solutions in Pulpal Management


Abstract
1. Overview
2. Imidazoline Derivatives
3. Pharmacology and Use
4. Efficacy
5. Systematic Safety and Contraindications
6. Anesthetic Adjunct for Intranasal Dental Anesthetic
7. Tissue Biocompatibility and Antimicrobial Activity
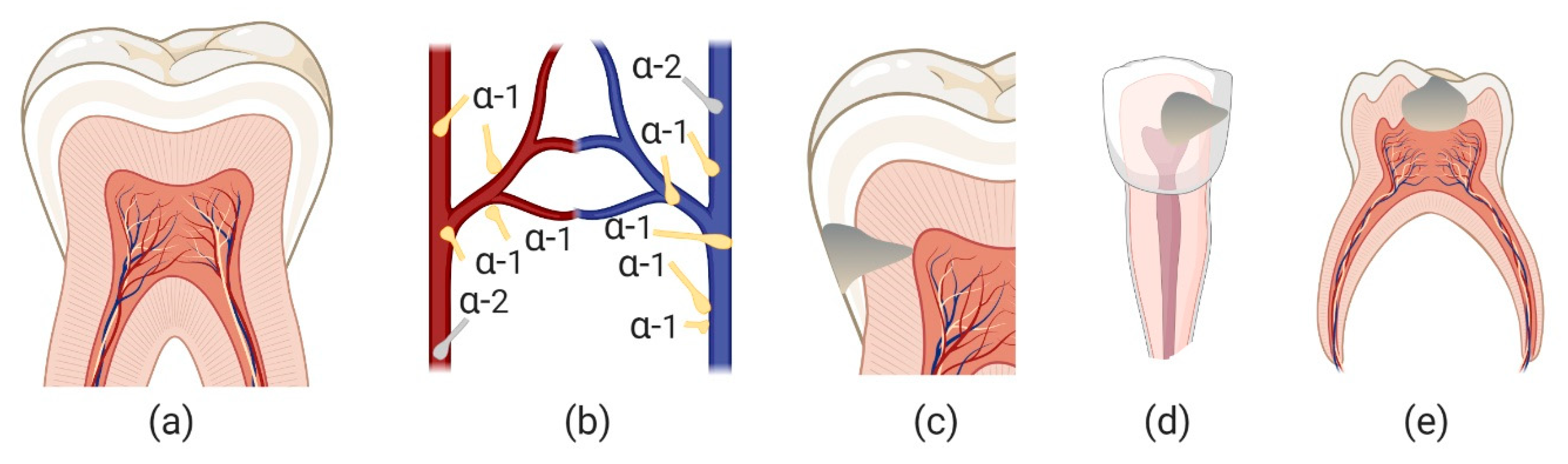
8. Pulpal Microphysiology and Management
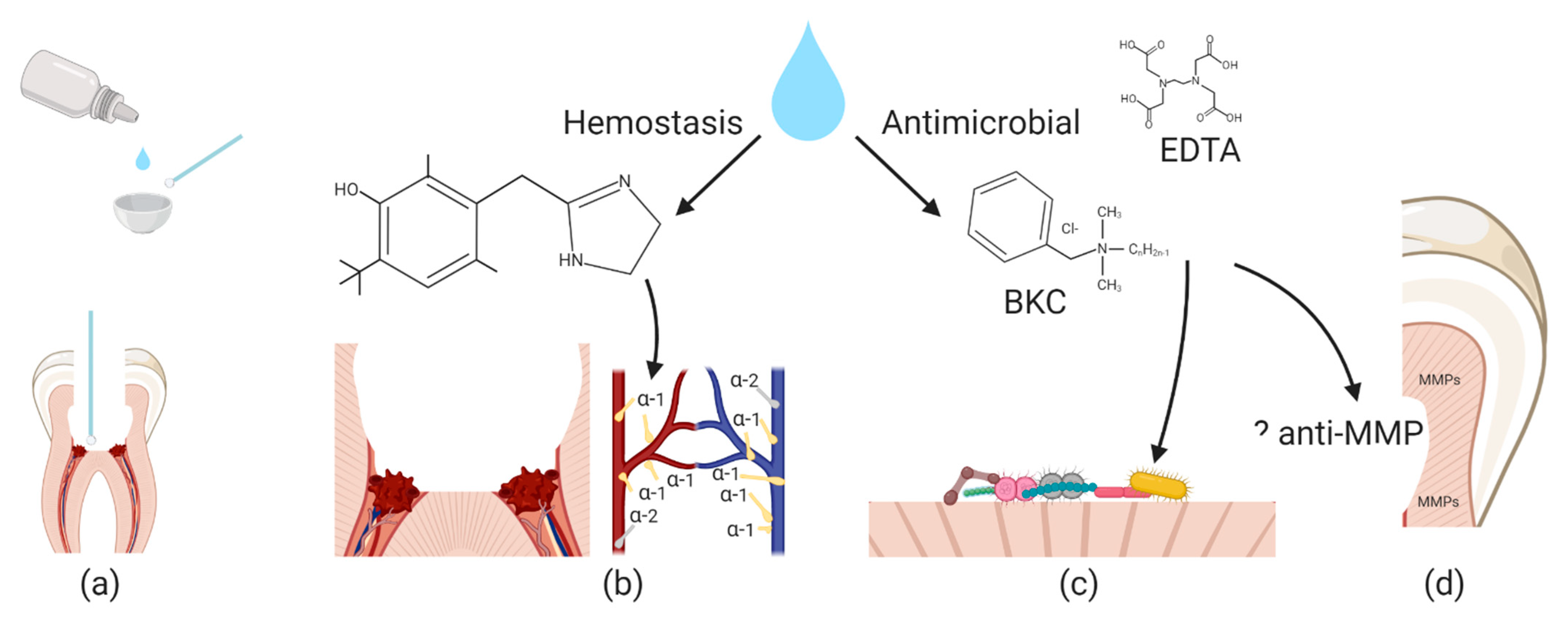
9. Conceptual Model of Pulpal Exposure Management
10. Discussion
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cartabuke, R.S.; Anderson, B.J.; Elmaraghy, C.; Rice, J.; Tumin, D.; Tobias, J.D. Hemodynamic and Pharmacokinetic Analysis of Oxymetazoline Use during Nasal Surgery in Children. Laryngoscope 2019, 129, 2775–2781. [Google Scholar] [CrossRef]
- Katz, R.I.; Hovagim, A.R.; Finkelstein, H.S.; Grinberg, Y.; Boccio, R.V.; Poppers, P.J. A Comparison of Cocaine, Lidocaine with Epinephrine, and Oxymetazoline for Prevention of Epistaxis on Nasotracheal Intubation. J. Clin. Anesth. 1990, 2, 16–20. [Google Scholar] [CrossRef]
- Higgins, T.S.; Hwang, P.H.; Kingdom, T.T.; Orlandi, R.R.; Stammberger, H.; Han, J.K. Systematic Review of Topical Vasoconstrictors in Endoscopic Sinus Surgery. Laryngoscope 2011, 121, 422–432. [Google Scholar] [CrossRef]
- Deckx, L.; De Sutter, A.I.; Guo, L.; Mir, N.A.; van Driel, M.L. Nasal Decongestants in Monotherapy for the Common Cold. Cochrane Database Syst. Rev. 2016, 10, CD009612. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez Valiente, A.; Roldan Fidalgo, A.; Laguna Ortega, D. Bleeding Control in Endoscopic Sinus Surgery: A Systematic Review of the Literature. Rhinology 2013, 51, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Bowles, W.H.; Tardy, S.J.; Vahadi, A. Evaluation of New Gingival Retraction Agents. J. Dent. Res. 1991, 70, 1447–1449. [Google Scholar] [CrossRef]
- Nowakowska, D.; Saczko, J.; Szewczyk, A.; Michel, O.; Ziętek, M.; Weżgowiec, J.; Więckiewicz, W.; Kulbacka, M. In Vitro Effects of Vasoconstrictive Retraction Agents on Primary Human Gingival Fibroblasts. Exp. Ther. Med. 2020, 19, 2037–2044. [Google Scholar] [CrossRef]
- Mehra, N.; Rathi, A.; Sharma, R.; Kaushik, M.; Sood, T. Evaluation of Alpha-Adrenomimetic Agents for Gingival Retraction: A Randomized Crossover Clinical Trial. J. Conserv. Dent. 2019, 22, 533–537. [Google Scholar] [CrossRef] [PubMed]
- Hersh, E.V.; Pinto, A.; Saraghi, M.; Saleh, N.; Pulaski, L.; Gordon, S.M.; Barnes, D.; Kaplowitz, G.; Bloom, I.; Sabti, M.; et al. Double-Masked, Randomized, Placebo-Controlled Study to Evaluate the Efficacy and Tolerability of Intranasal K305 (3% Tetracaine plus 0.05% Oxymetazoline) in Anesthetizing Maxillary Teeth. J. Am. Dent. Assoc. 2016, 147, 278–287. [Google Scholar] [CrossRef] [PubMed]
- Andersson, K.E.; Bende, M. Adrenoceptors in the Control of Human Nasal Mucosal Blood Flow. Ann. Otol. Rhinol. Laryngol. 1984, 93, 179–182. [Google Scholar] [CrossRef]
- Haenisch, B.; Walstab, J.; Herberhold, S.; Bootz, F.; Tschaikin, M.; Ramseger, R.; Bönisch, H. Alpha-Adrenoceptor Agonistic Activity of Oxymetazoline and Xylometazoline. Fundam. Clin. Pharmacol. 2010, 24, 729–739. [Google Scholar] [CrossRef] [PubMed]
- Minyan, W.; Dunn, W.R.; Blaylock, N.A.; Chan, S.L.; Wilson, V.G. Evidence for a Non-Adrenoceptor, Imidazoline-Mediated Contractile Response to Oxymetazoline in the Porcine Isolated Rectal Artery. Br. J. Pharmacol. 2001, 132, 1359–1363. [Google Scholar] [CrossRef]
- Abelson, M.B.; Yamamoto, G.K.; Allansmith, M.R. Effects of Ocular Decongestants. Arch. Ophthalmol. 1980, 98, 856–858. [Google Scholar] [CrossRef]
- Johnson, D.A.; Hricik, J.G. The Pharmacology of Alpha-Adrenergic Decongestants. Pharmacotherapy 1993, 13, 110S–115S; discussion 143S–146S. [Google Scholar] [PubMed]
- Hosten, L.O.; Snyder, C. Over-the-Counter Ocular Decongestants in the United States—Mechanisms of Action and Clinical Utility for Management of Ocular Redness. Clin. Optom. 2020, 12, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Hosal, B.M.; Hosal, S.A.; Hurwitz, J.J.; Freeman, J.L. A Rationale for the Selection of Nasal Decongestants in Lacrimal Drainage Surgery. Ophthal. Plast. Reconstr. Surg. 1995, 11, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, E.O. An Overview of Current Pharmacotherapy in Perennial Rhinitis. J. Allergy Clin. Immunol. 1995, 95, 1097–1110. [Google Scholar] [CrossRef]
- Şahin, M.İ.; Kökoğlu, K.; Güleç, Ş.; Ketenci, İ.; Ünlü, Y. Premedication Methods in Nasal Endoscopy: A Prospective, Randomized, Double-Blind Study. Clin. Exp. Otorhinolaryngol. 2017, 10, 158–163. [Google Scholar] [CrossRef]
- Reid, J.W.; Rotenberg, B.W.; Sowerby, L.J. Contemporary Decongestant Practices of Canadian Otolaryngologists for Endoscopic Sinus Surgery. J. Otolaryngol head neck Surg. Le J. d’oto-rhino-Laryngol. Chir. Cervico-Faciale 2019, 48, 15. [Google Scholar] [CrossRef]
- Popovic, M.; Chan, C.; Lattanzio, N.; El-Defrawy, S.; Schlenker, M.B. Comparative Cost Evaluation of Brand Name and Generic Ophthalmology Medications in Ontario. Can. J. Ophthalmol. 2018, 53, 173–187. [Google Scholar] [CrossRef]
- Hochban, W.; Althoff, H.; Ziegler, A. Nasal Decongestion with Imidazoline Derivatives: Acoustic Rhinometry Measurements. Eur. J. Clin. Pharmacol. 1999, 55, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Connell, J.T.; Linzmayer, M.I. Comparison of Nasal Airway Patency Changes after Treatment with Oxymetazoline and Pseudoephedrine. Am. J. Rhinol. 1987, 1, 87–94. [Google Scholar] [CrossRef]
- Eskiizmir, G.; Hirçin, Z.; Ozyurt, B.; Unlü, H. A Comparative Analysis of the Decongestive Effect of Oxymetazoline and Xylometazoline in Healthy Subjects. Eur. J. Clin. Pharmacol. 2011, 67, 19–23. [Google Scholar] [CrossRef]
- Riegle, E.V.; Gunter, J.B.; Lusk, R.P.; Muntz, H.R.; Weiss, K.L. Comparison of Vasoconstrictors for Functional Endoscopic Sinus Surgery in Children. Laryngoscope 1992, 102, 820–823. [Google Scholar] [CrossRef]
- Hite, D.; Mullen, N. Effects of Intranasal Oxymetazoline on the Pediatric Population Aged 1 to 12 Month: An Interim Analysis. Ann. Emerg. Med. 2008, 52, S165. [Google Scholar] [CrossRef]
- Joganathan, V.; Beigi, B. Safety of the Use of Xylometazoline Nasal Spray in Young Children Undergoing Lacrimal Surgery: An Observational Study. Eur. J. Ophthalmol. 2018, 28, 279–281. [Google Scholar] [CrossRef]
- Latham, G.J. In Reference to Hemodynamic and Pharmacokinetic Analysis of Oxymetazoline Use during Nasal Surgery in Children. Laryngoscope 2019, 129, E347. [Google Scholar] [CrossRef]
- Thrush, D.N. Cardiac Arrest after Oxymetazoline Nasal Spray. J. Clin. Anesth. 1995, 7, 512–514. [Google Scholar] [CrossRef]
- Ramesh, A.S.; Cartabuke, R.; Essig, G.; Tobias, J.D. Oxymetazoline-Induced Postoperative Hypertension. Pediatr Anesth Crit Care J 2013, 1, 72–77. [Google Scholar]
- Latham, G.J.; Jardine, D.S. Oxymetazoline and Hypertensive Crisis in a Child: Can We Prevent It? Pediatr. Anesth. 2013, 23, 952–956. [Google Scholar] [CrossRef]
- Nordt, S.P.; Vivero, L.E.; Cantrell, F.L. Not Just a Drop in the Bucket-Inversion of Oxymetazoline Nasal Decongestant Container Increases Potential for Severe Pediatric Poisoning. J Pediatr. 2016, 168, 240–241. [Google Scholar] [CrossRef] [PubMed]
- Jensen, P.; Edgren, B.; Hall, L.; Ring, J.C. Hemodynamic Effects Following Ingestion of an Imidazoline-Containing Product. Pediatr. Emerg. Care 1989, 5, 110–112. [Google Scholar] [CrossRef] [PubMed]
- Mahieu, L.M.; Rooman, R.P.; Goossens, E. Imidazoline Intoxication in Children. Eur. J. Pediatr. 1993, 152, 944–946. [Google Scholar] [CrossRef] [PubMed]
- Lev, R.; Clark, R.F. Visine® Overdose: Case Report of an Adult with Hemodynamic Compromise. J. Emerg. Med. 1995, 13, 649–652. [Google Scholar] [CrossRef]
- Fabi, M.; Formigari, R.; Picchio, F.M. Are Nasal Decongestants Safer than Rhinitis? A Case of Oxymetazoline-Induced Syncope. Cardiol. Young 2009, 19, 633–634. [Google Scholar] [CrossRef]
- Bellew, S.D.; Johnson, K.L.; Nichols, M.D.; Kummer, T. Effect of Intranasal Vasoconstrictors on Blood Pressure: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Emerg. Med. 2018, 55, 455–464. [Google Scholar] [CrossRef]
- Daggy, A.; Kaplan, R.; Roberge, R.; Akhtar, J. Pediatric Visine (Tetrahydrozoline) Ingestion: Case Report and Review of Imidazoline Toxicity. Vet. Hum. Toxicol. 2003, 45, 210–212. [Google Scholar]
- Spiller, H.; Griffith, J. Prolonged Cardiovascular Effects after Unintentional Ingestion of Tetrahydrozoline. Clin. Toxicol. (Phila). 2008, 46, 171–172. [Google Scholar] [CrossRef]
- Dokuyucu, R.; Gokce, H.; Sahan, M.; Sefil, F.; Tas, Z.A.; Tutuk, O.; Ozturk, A.; Tumer, C.; Cevik, C. Systemic Side Effects of Locally Used Oxymetazoline. Int. J. Clin. Exp. Med. 2015, 8, 2674–2678. [Google Scholar]
- Giannakopoulos, H.; Levin, L.M.; Chou, J.C.; Cacek, A.T.; Hutcheson, M.; Secreto, S.A.; Moore, P.A.; Hersh, E.V. The Cardiovascular Effects and Pharmacokinetics of Intranasal Tetracaine plus Oxymetazoline: Preliminary Findings. J. Am. Dent. Assoc. 2012, 143, 872–880. [Google Scholar] [CrossRef]
- Isaacson, G.; Buttaro, B.A.; Mazeffa, V.; Li, G.; Frenz, D.A. Oxymetazoline Solutions Inhibit Middle Ear Pathogens and Are Not Ototoxic. Ann. Otol. Rhinol. Laryngol. 2005, 114, 645–651. [Google Scholar] [CrossRef]
- Daniel, S.J.; Akinpelu, O.V.; Sahmkow, S.; Funnell, W.R.J.; Akache, F. Oxymetazoline Ototoxicity in a Chinchilla Animal Model. Otolaryngol. Neck Surg. 2011, 146, 114–118. [Google Scholar] [CrossRef]
- Kumar, V.V.; Gaughan, J.; Isaacson, G.; Szeremeta, W. Oxymetazoline Is Equivalent to Ciprofloxacin in Preventing Postoperative Otorrhea or Tympanostomy Tube Obstruction. Laryngoscope 2005, 115, 363–365. [Google Scholar] [CrossRef]
- Isaacson, G. Further Evidence of Oxymetazoline’s Safety in Otologic Surgery. Otolaryngol. Neck Surg. 2012, 147, 179. [Google Scholar] [CrossRef]
- Olgart, L. Neural Control of Pulpal Blood Flow. Crit. Rev. Oral Biol. Med. An Off. Publ. Am. Assoc. Oral Biol. 1996, 7, 159–171. [Google Scholar] [CrossRef]
- Sasano, T.; Shoji, N.; Kuriwada, S.; Sanjo, D.; Izumi, H.; Karita, K. Absence of Parasympathetic Vasodilatation in Cat Dental Pulp. J. Dent. Res. 1995, 74, 1665–1670. [Google Scholar] [CrossRef] [PubMed]
- Edwall, L.; Kindlová, M. The Effect of Sympathetic Nerve Stimulation on the Rate of Disappearance of Tracers from Various Oral Tissues. Acta Odontol. Scand. 1971, 29, 387–400. [Google Scholar] [CrossRef] [PubMed]
- Ricketts, D.N.J.; Kidd, E.A.M.; Innes, N.; Clarkson, J. Complete or Ultraconservative Removal of Decayed Tissue in Unfilled Teeth. Cochrane database Syst. Rev. 2006, CD003808. [Google Scholar] [CrossRef]
- Meyer, M.W.; Path, M.G. Blood Flow in the Dental Pulp of Dogs Determined by Hydrogen Polarography and Radioactive Microsphere Methods. Arch. Oral Biol. 1979, 24, 601–605. [Google Scholar] [CrossRef]
- Berman, L.H.; Hargreaves, K.M. Cohen’s Pathways of the Pulp-E-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2020; ISBN 032367304X. [Google Scholar]
- Tezvergil-Mutluay, A.; Mutluay, M.M.; Gu, L.; Zhang, K.; Agee, K.A.; Carvalho, R.M.; Manso, A.; Carrilho, M.; Tay, F.R.; Breschi, L.; et al. The Anti-MMP Activity of Benzalkonium Chloride. J. Dent. 2011, 39, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Simard-Savoie, S.; Lemay, H.; Taleb, L. The Effect of Epinephrine on Pulpal Microcirculation. J. Dent. Res. 1979, 58, 2074–2079. [Google Scholar] [CrossRef]
- Hilton, T.J. Keys to Clinical Success with Pulp Capping: A Review of the Literature. Oper. Dent. 2009, 34, 615–625. [Google Scholar] [CrossRef]
- Garcia-Godoy, F.; Murray, P.E. Systemic Evaluation of Various Haemostatic Agents Following Local Application Prior to Direct Pulp Capping. Brazilian J. Oral Sci. 2016, 4, 791–797. [Google Scholar]
- Woody, R.D.; Miller, A.; Staffanou, R.S. Review of the PH of Hemostatic Agents Used in Tissue Displacement. J. Prosthet. Dent. 1993, 70, 191–192. [Google Scholar] [CrossRef]
- Vargas, K.G.; Packham, B. Radiographic Success of Ferric Sulfate and Formocresol Pulpotomies in Relation to Early Exfoliation. Pediatr. Dent. 2005, 27, 233–237. [Google Scholar]
- Merchel Piovesan Pereira, B.; Tagkopoulos, I. Benzalkonium Chlorides: Uses, Regulatory Status, and Microbial Resistance. Appl. Environ. Microbiol. 2019, 85. [Google Scholar] [CrossRef] [PubMed]
- Marple, B.; Roland, P.; Benninger, M. Safety Review of Benzalkonium Chloride Used as a Preservative in Intranasal Solutions: An Overview of Conflicting Data and Opinions. Otolaryngol. Head Neck Surg. 2004, 130, 131–141. [Google Scholar] [CrossRef]
- Watrobska–Swietlikowska, D. Distribution of Benzalkonium Chloride into the Aqueous Phases of Submicron Dispersed Systems: Emulsions, Aqueous Lecithin Dispersion and Nanospheres. AAPS PharmSciTech 2019, 21, 7. [Google Scholar] [CrossRef]
- Bernstein, I.L. Is the Use of Benzalkonium Chloride as a Preservative for Nasal Formulations a Safety Concern? A Cautionary Note Based on Compromised Mucociliary Transport. J. Allergy Clin. Immunol. 2000, 105, 39–44. [Google Scholar] [CrossRef]
- Richards, R.M.; Cavill, R.H. Electron Microscope Study of Effect of Benzalkonium Chloride and Edetate Disodium on Cell Envelope of Pseudomonas Aeruginosa. J. Pharm. Sci. 1976, 65, 76–80. [Google Scholar] [CrossRef]
- Asl Aminabadi, N.; Satrab, S.; Najafpour, E.; Samiei, M.; Jamali, Z.; Shirazi, S. A Randomized Trial of Direct Pulp Capping in Primary Molars Using MTA Compared to 3Mixtatin: A Novel Pulp Capping Biomaterial. Int. J. Paediatr. Dent. 2016, 26, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Caprioglio, A.; Conti, V.; Caprioglio, C.; Caprioglio, D. A Long-Term Retrospective Clinical Study on MTA Pulpotomies in Immature Permanent Incisors with Complicated Crown Fractures. Eur. J. Paediatr. Dent. 2014, 15, 29–34. [Google Scholar]
- Coll, J.A.; Seale, N.S.; Vargas, K.; Marghalani, A.A.; Al Shamali, S.; Graham, L. Primary Tooth Vital Pulp Therapy: A Systematic Review and Meta-Analysis. Pediatr. Dent. 2017, 39, 16–123. [Google Scholar]
- FDA Drug Safety Communication: Serious Adverse Events from Accidental Ingestion by Children of over-the-Counter Eye Drops and Nasal Sprays. US Food and Drug Administration Website. Available online: Http://Www.Fda.Gov/Drugs/DrugSafety/Ucm325257.Htm (accessed on 13 January 2021).
- Jaramillo, D.E.; Arriola, A.; Safavi, K.; Chávez de Paz, L.E. Decreased Bacterial Adherence and Biofilm Growth on Surfaces Coated with a Solution of Benzalkonium Chloride. J. Endod. 2012, 38, 821–825. [Google Scholar] [CrossRef] [PubMed]
- Kurt, A.; Tüzüner, T.; Baygın, Ö. Antibacterial Characteristics of Glass Ionomer Cements Containing Antibacterial Agents: An in Vitro Study. Eur. Arch. Paediatr. Dent. Off. J. Eur. Acad. Paediatr. Dent. 2020. [Google Scholar] [CrossRef] [PubMed]
- Saito, K.; Hayakawa, T.; Kawabata, R.; Meguro, D.; Kasai, K. In Vitro Antibacterial and Cytotoxicity Assessments of an Orthodontic Bonding Agent Containing Benzalkonium Chloride. Angle Orthod. 2009, 79, 331–337. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Compound | Primary Uses | USA Availability | Surgical Hemostasis | Duration (h) |
|---|---|---|---|---|
| 0.05% Oxymetazoline HCL | Nasal Congestion | Yes | Yes | 8 |
| 0.1% Xylometazoline HCL | Nasal Congestion | No | Yes | 8 |
| 0.02% Naphazoline HCL | Conjunctivitis | Yes | No | 4 |
| 0.1% Tetrahydrozoline HCL | Conjunctivitis | Yes | No | 4 |
| Medical Precautions | Drug Class Interactions | |
|---|---|---|
| severe or unstable cardiovascular disease | uncontrolled hypertension or hypotension | fentanyl |
| beta adrenergic antagonist | ||
| cerebral insufficiency | coronary disease | monoamine oxidase inhibitors (MAOIs) |
| Sjögren’s syndrome | narrow-angle glaucoma | |
| Raynaud’s phenomenon | thromboangiitis obliterans | tricyclic antidepressant (TCAs) |
| scleroderma | diabetes mellitus | |
| prostatic enlargement | thyroid disease | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jones, R.S. Conceptual Model for Using Imidazoline Derivative Solutions in Pulpal Management. J. Clin. Med. 2021, 10, 1212. https://doi.org/10.3390/jcm10061212
Jones RS. Conceptual Model for Using Imidazoline Derivative Solutions in Pulpal Management. Journal of Clinical Medicine. 2021; 10(6):1212. https://doi.org/10.3390/jcm10061212
Chicago/Turabian StyleJones, Robert S. 2021. "Conceptual Model for Using Imidazoline Derivative Solutions in Pulpal Management" Journal of Clinical Medicine 10, no. 6: 1212. https://doi.org/10.3390/jcm10061212
APA StyleJones, R. S. (2021). Conceptual Model for Using Imidazoline Derivative Solutions in Pulpal Management. Journal of Clinical Medicine, 10(6), 1212. https://doi.org/10.3390/jcm10061212