
The Outbreak of SARS-CoV-2 Pandemic and the Well-Being of Polish Students: The Risk Factors of the Emotional Distress during COVID-19 Lockdown


 , , , , and
, , , , and 
Abstract
1. Introduction
2. Psychological Consequences of the Pandemic
3. Materials and Methods
3.1. Study Design and Survey Description
3.2. Measures
3.3. DASS-21 Scale
3.4. Description of the Study Group
3.5. Characteristic of the Respondents’ Health Status
3.6. Employment Status and Economic Situation of the Respondents
4. Statistical Analysis
5. Ethical Considerations
6. Results
6.1. DASS-21
6.1.1. Total DASS Score
6.1.2. Depression
6.1.3. Anxiety
6.1.4. Stress
6.2. Factors Correlating with the Emotional Distress in the Study Group
6.2.1. Demographic Factors
6.2.2. The Most Difficult Problem during the Pandemic
6.2.3. Suffering from Chronic Diseases
6.2.4. Psychological/Psychiatric Support before the Pandemic Broke-Out
6.2.5. Economic Situation during a Pandemic
6.2.6. Employment Status during a Pandemic
6.2.7. Living Situation
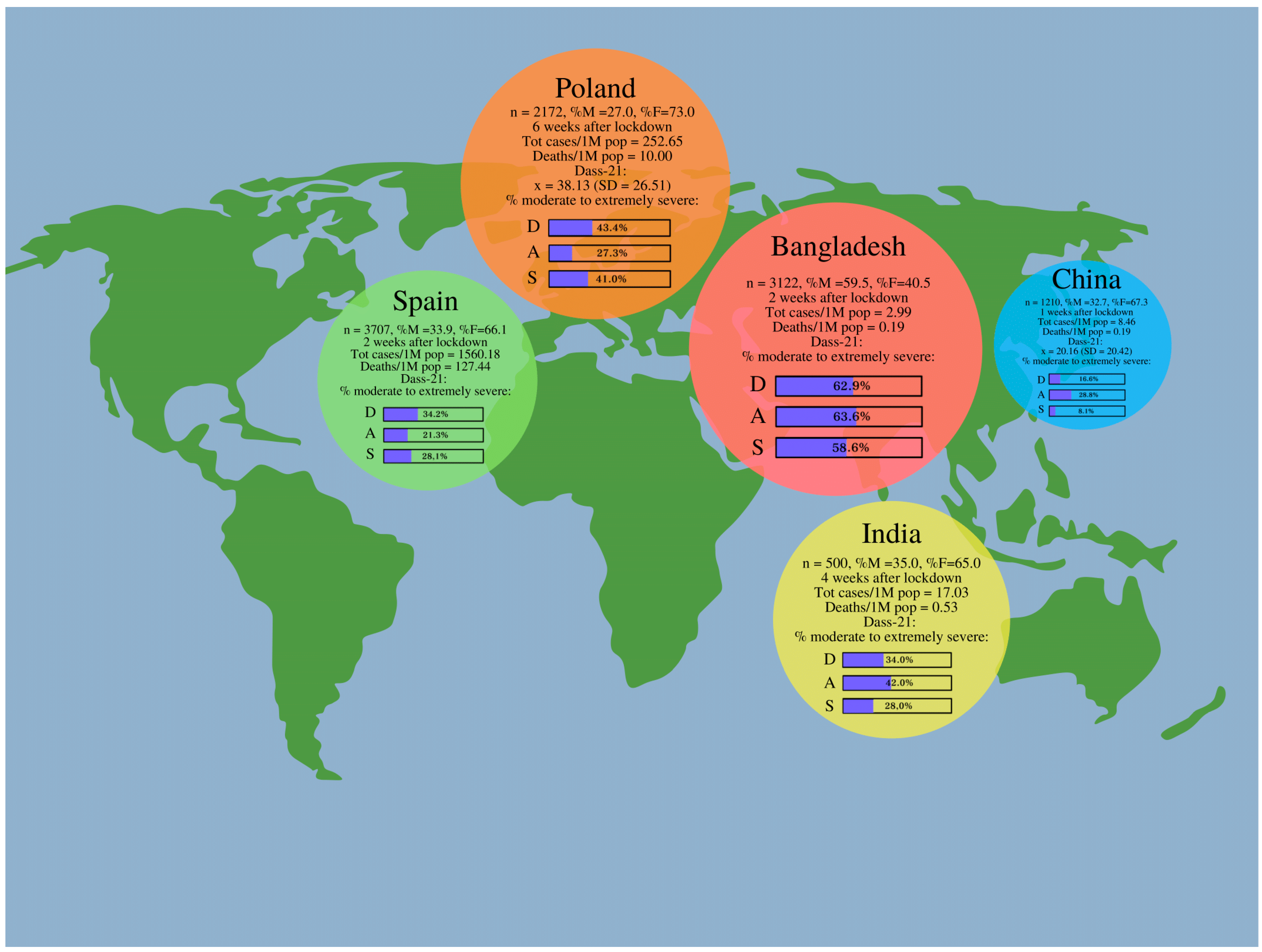
6.3. Comparison with the Results of Other Authors’ Studies
7. The Portrait of a Student who May Potentially Require Special Psychiatric and/or Psychological Support during the Pandemic
8. Discussion
9. Limitations of the Study
10. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| COVID-19 | Coronavirus disease 2019 |
| DASS-21 | Depression, Anxiety, and Stress Scale-21 Items |
| M | Mean |
| Me | Median |
| MERS-CoV | Middle East Respiratory Syndrome Coronavirus |
| OR | Odds ratio |
| SARS-CoV | Severe Acute Respiratory Syndrome Coronavirus |
| SARS-CoV-2 | Severe Acute Respiratory Syndrome Coronavirus-2 |
| WHO | World Health Organization |
References
- Lu, H.; Stratton, C.W.; Tang, Y.W. Outbreak of pneumonia of unknown etiology in Wuhan, China: The mystery and the miracle. J. Med. Virol. 2020, 92, 401–402. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- World Health Organization. Rolling Updates On Coronavirus Disease (COVID-19) [Internet]. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen (accessed on 27 April 2020).
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19–11 March 2020 [Internet]. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 27 March 2020).
- Di Gennaro, F.; Pizzol, D.; Marotta, C.; Antunes, M.; Racalbuto, V.; Veronese, N.; Smith, L. Coronavirus Diseases (COVID-19) Current Status and Future Perspectives: A Narrative Review. Int. J. Environ. Res. Public Health. 2020, 17, 2690. [Google Scholar] [CrossRef] [PubMed]
- Nadeem, M.S.; Zamzami, M.A.; Choudhry, H.; Murtaza, B.N.; Kazmi, I.; Ahmad, H.; Shakoori, A.-R. Origin, Potential Therapeutic Targets and Treatment for Coronavirus Disease (COVID-19). Pathogens 2020, 9, 307. [Google Scholar] [CrossRef] [PubMed]
- Mungroo, M.R.; Khan, N.A.; Siddiqui, R. Novel Coronavirus: Current Understanding of Clinical Features, Diagnosis, Pathogenesis, and Treatment Options. Pathogens 2020, 9, 297. [Google Scholar] [CrossRef]
- Baj, J.; Karakuła-Juchnowicz, H.; Teresiński, G.; Buszewicz, G.; Ciesielka, M.; Sitarz, E.; Forma, A.; Karakuła, K.; Flieger, W.; Portincasa, P.; et al. COVID-19: Specific and Non-Specific Clinical Manifestations and Symptoms: The Current State of Knowledge. J. Clin. Med. 2020, 9, 1753. [Google Scholar] [CrossRef]
- Grant, B.W.; Lahore, H.; McDonnell, L.S.; Baggerly, A.C.; French, B.C.; Aliano, L.J.; Bhattoa, H.P. Evidence that Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths. Nutrients 2020, 12, 988. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease (COVID-19) Pandemic [Internet]. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 27 April 2020).
- British Broadcasting Company. Coronavirus: The World in Lockdown in Maps and Charts [Internet]. Available online: https://www.bbc.com/news/world-52103747 (accessed on 28 April 2020).
- Government of Poland. Mapa Zarażeń Koronawirusem (SARS-CoV-2). [Map of coronavirus infection (SARS-CoV-2).] [Internet]. Available online: https://www.gov.pl/web/koronawirus/wykaz-zarazen-koronawirusem-sars-cov-2 (accessed on 26 April 2020).
- Government of Poland. Wprowadzamy Stan Epidemii w Polsce [Introducing the Epidemic State in Poland] [Internet]. Available online: https://www.gov.pl/web/koronawirus/wprowadzamy-stan-epidemii-w-polsce (accessed on 28 April 2020).
- Government of Poland. Kolejne Kroki W Walce Z Koronawirusem–W Sklepie Mniej Osób, Ograniczenia W Poruszaniu Nieletnich, a Parki, Plaże I Bulwary Zamknięte. [Next Steps in the Fight Against Coronavirus-fewer People in the Store, Restrictions on the Movement of Minors, and Parks, Beaches and Boulevards closed.] [Internet]. Available online: https://www.gov.pl/web/koronawirus/kolejne-kroki (accessed on 28 April 2020).
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, S.C.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; You, M. Psychological and Behavioral Responses in South Korea During the Early Stages of Coronavirus Disease 2019 (COVID-19). Int. J. Environ. Res. Public Health 2020, 17, 2977. [Google Scholar] [CrossRef]
- Cao, W.; Fang, Z.; Guoqiang, H.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef] [PubMed]
- He, J.; He, L.; Zhou, W.; Nie, X.; He, M. Discrimination and Social Exclusion in the Outbreak of COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 2933. [Google Scholar] [CrossRef] [PubMed]
- Sim, K.; Chan, Y.; Phui-Nah, C.; Chua, H.; Soon, S. Psychosocial and coping responses within the community health care setting towards a national outbreak of an infectious disease. J. Psychosom. Res. 2010, 68, 195–202. [Google Scholar] [CrossRef]
- Saeed, S.A.; Hebishi, K. The psychiatric consequences of COVID-19: 8 Studies. Curr. Psychiatry 2020, 19, 22–24, 28–30, 32–35. [Google Scholar] [CrossRef]
- Pérez-Fuentes, D.M.; Molero Jurado, D.M.; Oropesa Ruiz, F.N.; Martos Martínez, Á.; Simón Márquez, D.M.; Herrera-Peco, I.; Linares, J.J.G. Questionnaire on Perception of Threat from COVID-19. J. Clin. Med. 2020, 9, 1146. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, C.H.; Nguyen, H.M.; Do, N.B.; Tran, Q.C.; Nguyen, T.P.T.; Pham, M.K.; Pham, L.V.; Tran, K.V.; Duong, T.T.; Tran, T.V.; et al. People with Suspected COVID-19 Symptoms Were More Likely Depressed and Had Lower Health-Related Quality of Life: The Potential Benefit of Health Literacy. J. Clin. Med. 2020, 9, 965. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 epidemic in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depres- sion among the general population dur- ing the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health. 2020, 16, 57. [Google Scholar] [CrossRef]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef]
- Lakhan, R.; Agrawal, A.; Sharma, M. Prevalence of Depression, Anxiety, and Stress during COVID-19 Pandemic. J. Neurosci. Rural. Pr. 2020, 11, 519–525. [Google Scholar] [CrossRef]
- Pieh, C.; Budimir, S.; Probst, T. The effect of age, gender, income, work, and physical activity on mental health during coronavirus disease (COVID-19) lockdown in Austria. J. Psychosom. Res. 2020, 136, 110186. [Google Scholar] [CrossRef]
- García-Fernández, L.; Romero-Ferreiro, V.; López-Roldán, P.D.; Padilla, S.; Rodriguez-Jimenez, R. Mental Health in Elderly Spanish People in Times of COVID-19 Outbreak. Am. J. Geriatr. Psychiatry 2020, 28, 1040–1045. [Google Scholar] [CrossRef]
- Mamun, M.A.; Akter, S.; Hossain, I.; Faisal, M.T.H.; Rahman, A.; Arefin, A.; Khan, I.; Hossain, L.; Haque, A.; Hossain, S.; et al. Financial threat, hardship and distress predict depression, anxiety and stress among the unemployed youths: A Bangladeshi multi-city study. J. Affect. Disord. 2020, 276, 1149–1158. [Google Scholar] [CrossRef]
- Achdut, N.; Refaeli, T. Unemployment and Psychological Distress among Young People during the COVID-19 Pandemic: Psychological Resources and Risk Factors. Int. J. Environ. Res. Public Health 2020, 17, 7163. [Google Scholar] [CrossRef]
- Wang, C.; Chudzicka-Czupała, A.; Grabowski, D.; Pan, R.; Adamus, K.; Wan, X.; Hetnał, M.; Tan, Y.; Olszewska-Guizzo, A.; Xu, L.; et al. The Association Between Physical and Mental Health and Face Mask Use During the COVID-19 Pandemic: A Comparison of Two Countries With Different Views and Practices. Front. Psychiatry 2020, 11, 569981. [Google Scholar] [CrossRef]
- Kazmi, S.S.H.; Hasan, K.; Talib, S.; Saxena, S. COVID-19 and Lockdwon: A Study on the Impact on Mental Health. 2020. Available online: https://ssrn.com/abstract=3577515 (accessed on 8 November 2020).
- Wu, M.; Xu, W.; Yao, Y.; Zhang, L.; Guo, L.; Fan, J.; Chen, J. Mental health status of students’ parents during COVID-19 pandemic and its influence factors. Gen Psychiatr. 2020, 33, e100250. [Google Scholar] [CrossRef]
- Epifanio, M.S.; Andrei, F.; Mancini, G.; Agostini, F.; Piombo, M.A.; Spicuzza, V.; Riolo, M.; Lavanco, G.; Trombini, E.; La Grutta, S. The Impact of COVID-19 Pandemic and Lockdown Measures on Quality of Life among Italian General Population. J. Clin. Med. 2021, 10, 289. [Google Scholar] [CrossRef] [PubMed]
- Hoyt, L.T.; Cohen, A.K.; Dull, B.; Castro, E.M.; Yazdani, N. “Constant Stress Has Become the New Normal”: Stress and Anxiety Inequalities Among, U.S. College Students in the Time of COVID-19. J. Adolesc. Health 2020. [Google Scholar] [CrossRef]
- Sundarasen, S.; Chinna, K.; Kamaludin, K.; Nurunnabi, M.; Baloch, G.M.; Khoshaim, H.B.; Hossain, S.F.A.; Sukayt, A. Psychological Impact of COVID-19 and Lockdown among University Students in Malaysia: Implications and Policy Recommendations. Int. J. Environ. Res. Public Health. 2020, 17, 6206. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wang, Y.; Jiang, J.; Valdimarsdóttir, U.A.; Fall, K.; Fang, F.; Song, H.; Lu, D.; Zhang, W. Psychological distress among health professional students during the COVID-19 outbreak. Psychol. Med. 2020, 11, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Dratva, J.; Zysset, A.; Schlatter, N.; von Wyl, A.; Huber, M.; Volken, T. Swiss University Students’ Risk Perception and General Anxiety during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health. 2020, 17, 7433. [Google Scholar] [CrossRef] [PubMed]
- Odriozola-González, P.; Planchuelo-Gómez, Á.; Irurtia, M.J.; de Luis-García, R. Psychological effects of the COVID-19 outbreak and lockdown among students and workers of a Spanish university. Psychiatry Res. 2020, 290, 113108. [Google Scholar] [CrossRef]
- Polish Translation of DASS. Available online: http://www2.psy.unsw.edu.au/Groups/Dass/Polish/Polish.htm (accessed on 8 November 2020).
- DASS Translations. Available online: http://www2.psy.unsw.edu.au/groups/dass/translations.htm (accessed on 8 November 2020).
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scales; Sydney Psychology Foundation Australia: Sydney, Australia, 1995. [Google Scholar]
- Antony, M.M.; Bieling, P.J.; Cox, B.J.; Enns, M.W.; Swinson, R.P. Psychometric properties of the 42-item and 21-item versions of the depression anxiety stress scales in clinical groups and a community sample. Psychol. Assess. 1998, 10, 176–181. [Google Scholar] [CrossRef]
- Depression Anxiety Stress Scales–Short Form (DASS-21) [Internet]. NovoPsych Psychometrics. Available online: https://novopsych.com.au/assessments/depression-anxiety-stress-scales-short-form-dass-21/ (accessed on 19 June 2020).
- Ruiz, F.; Garcia-Martin, M.; Suárez, F.; Juan, C.; Odriozola-González, P. The hierarchical factor structure of the Spanish version of the Depression Anxiety and Stress Scale-21 (DASS-21). Int. J. Psychol. Psychol. Ther. 2017, 17, 93–101. [Google Scholar]
- Henry, J.D.; Crawford, J.R. The short-form version of the Depression Anxiety Stress Scales (DASS-21): Construct validity and normative data in a large non-clinical sample. Br. J. Clin. Psychol. 2005, 44, 227–239. [Google Scholar] [CrossRef]
- Steel, Z.; Marnane, C.; Iranpour, C.; Chey, T.; Jackson, J.W.; Patel, V.; Silove, D. The global prevalence of common mental disorders: A systematic review and meta-analysis 1980–2013. Int. J. Epidemiol. 2014, 43, 476–493. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.M.A.; Mohammad, D.; Quereshi, M.F.H.; Abbas, M.Z.; Aleem, S. Prevalence, Psychological Responses and Associated Correlates of Depression, Anxiety and Stress in a Global Population, During the Coronavirus Disease (COVID-19) Pandemic. Community Ment. Health J. 2021, 57, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Zawislak, D.; Zur-Wyrozumska, K.; Habera, M.; Skrzypiec, K.; Pac, A.; Cebula, G. Evaluation of a Polish Version of the Depression Anxiety Stress Scales (DASS-21). J. Neurosci. Cogn. Stud. 2020, 4, 101. [Google Scholar]
- Martinotti, G.; Alessi, M.C.; Di Natale, C.; Sociali, A.; Ceci, F.; Lucidi, L.; Picutti, E.; Di Carlo, F.; Corbo, M.; Vellante, F.; et al. Psychopathological Burden and Quality of Life in Substance Users During the COVID-19 Lockdown Period in Italy. Front. Psychiatry 2020, 11, 572245. [Google Scholar] [CrossRef] [PubMed]
- Moroń, M.; Biolik-Moroń, M. Trait emotional intelligence and emotional experiences during the COVID-19 pandemic outbreak in Poland: A daily diary study. Personal. Individ. Differ. 2021, 168, 110348. [Google Scholar] [CrossRef]
- Selye, I. The general adaptation syndrome and the diseases of adaptation. J. Allergy. 1946, 17, 289–323. [Google Scholar] [CrossRef]
- Suryadevara, V.; Adusumalli, C.; Adusumilli, P.K.; Chalasani, S.H.; Radhakrishnan, R. Mental Health Status among the South Indian Pharmacy Students during Covid-19 Pandemic Quarantine Period: A Cross-Sectional Study. 2020. Available online: https://www.x-mol.com/paper/1260295362728624128 (accessed on 8 November 2020).
- Islam, M.; Sujan, S.H.; Tasnim, R.; Sikder, T.; Potenza, M.N.; Os, J.V. Psychological Responses during the COVID-19 Outbreak among University Students in Bangladesh. 2020. Available online: https://psyarxiv.com/cndz7/ (accessed on 8 November 2020).
- Lim, G.Y.; Tam, W.W.; Lu, Y.; Ho, C.S.; Zhang, M.W.; Ho, R.C. Prevalence of Depression in the Community from 30 Countries between 1994 and 2014. Sci. Rep. 2018, 8, 2861. [Google Scholar]
- McLean, C.P.; Asnaani, A.; Litz, B.T.; Hofmann, S.G. Gender differences in anxiety disorders: Prevalence, course of illness, comorbidity and burden of illness. J. Psychiatr. Res. 2011, 45, 1027–1035. [Google Scholar]
- Bahrami, F.; Yousefi, N. Females are more anxious than males: A metacognitive perspective. Iran. J. Psychiatry Behav. Sci. 2011, 5, 83–90. [Google Scholar] [PubMed]
- Wathelet, M.; Duhem, S.; Vaiva, G.; Baubet, T.; Habran, E.; Veerapa, E.; Debien, C.; Molenda, S.; Horn, M.; Grandgenèvre, P.; et al. Factors Associated With Mental Health Disorders Among University Students in France Confined During the COVID-19 Pandemic. JAMA Netw. Open 2020, 3, e2025591. [Google Scholar]
- Wang, X.; Hegde, S.; Son, C.; Keller, B.; Smith, A.; Sasangohar, F. Investigating Mental Health of US College Students During the COVID-19 Pandemic: Cross-Sectional Survey Study. J. Med. Internet. Res. 2020, 22, e22817. [Google Scholar] [CrossRef]
- Hawkley, L.C.; Cacioppo, J.T. Loneliness matters: A theoretical and empirical review of consequences and mechanisms. Ann. Behav. Med. 2010, 40, 218–227. [Google Scholar] [PubMed]
- Losda-Baltar, A.; Jiménez-Gonzalo, L.; Gallego-Alberto, L.; Pedroso-Chaparro, M.D.S.; Fernandes-Pires, J.; Márquez-González, M. “We’re Staying at Home”. Association of Self-Perceptions of Aging, Personal and Family Resources and Loneliness With Psychological Distress During the Lock-Down Period of COVID-19. J. Gerontol. B Psychol. Sci. Soc. Sci. 2021, 76, e10–e16. [Google Scholar]
- Groarke, J.M.; Berry, E.; Graham-Wisener, L.; Mckenna-Plumley, P.E.; Mcglinchey, E.; Armour, C. Loneliness in the UK during the COVID-19 pandemic: Cross-sectional results from the COVID-19 Psychological Wellbeing Study. PLoS ONE 2020, 15, e0239698. [Google Scholar] [CrossRef]
- Loades, M.E.; Chatburn, E.; Higson-Sweeney, N.; Reynolds, S.; Shafran, R.; Brigden, A.; Linney, C.; McManus, M.N.; Borwick, C.; Crawley, E. Rapid Systematic Review: The Impact of Social Isolation and Loneliness on the Mental Health of Children and Adolescents in the Context of COVID-19. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 1218–1239.e3. [Google Scholar] [CrossRef]
- Herbert, J. Stress, the brain, and mental illness. BMJ 1997, 315, 530–535. [Google Scholar] [CrossRef]
- Cattaneo, A.; Riva, M.A. Stress-induced mechanisms in mental illness: A role for glucocorticoid signalling. J. Steroid. Biochem. Mol. Biol. 2016, 160, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Vindegaard, N.; Benros, M.E. COVID-19 pan-demic and mental health consequences: Sys-tematic review of the current evidence. Brain. Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef] [PubMed]
- Orpana, H.M.; Lemyre, L.; Gravel, R. Income and psychological distress: The role of the social environment. Health Rep. 2009, 20, 21–28. [Google Scholar] [PubMed]
- Larionov, P.; Mudło-Głagolska, K. Mental Health Risk Factors during COVID-19 Pandemic in the Polish Population. 2020. Available online: https://psyarxiv.com/3ku8w/ (accessed on 8 November 2020).


{kind=link}
| Depression | Anxiety | Stress | |
|---|---|---|---|
| Normal | 0–8 | 0–7 | 0–14 |
| Mild | 8–13 | 8–9 | 15–18 |
| Moderate | 14–20 | 10–14 | 19–25 |
| Severe | 21–27 | 15–19 | 26–33 |
| Extremely severe | 28+ | 20+ | 34+ |
| Question | Answer | Number of Respondents | % of Respondents |
|---|---|---|---|
| Sex | Women | 1585 | 73.0 |
| Men | 587 | 27.0 | |
| Field of study | Arts and humanities | 110 | 5.0 |
| Sciences | 96 | 4.4 | |
| Medicine | 1314 | 60.5 | |
| Engineering | 219 | 10.0 | |
| Social sciences | 416 | 19.2 | |
| Year of study | I | 511 | 23.5 |
| II | 444 | 20.4 | |
| III | 507 | 23.3 | |
| IV | 322 | 14.8 | |
| V | 277 | 12.8 | |
| VI | 106 | 4.9 | |
| Place of residence (number of inhabitants) [in thousands] | Village | 497 | 22.9 |
| Less than 20 | 219 | 10.1 | |
| 20–100 | 344 | 15.8 | |
| 100–300 | 276 | 12.7 | |
| 300–600 | 409 | 18.8 | |
| More than 600 | 427 | 19.7 | |
| Marital status | Single | 1426 | 65.6 |
| Informal relationship | 667 | 30.7 | |
| Married | 54 | 2.5 | |
| Do you have children? | No | 2130 | 98.1 |
| One child | 20 | 0.9 | |
| I live with: | Alone | 231 | 10.6 |
| Parents | 1049 | 48.3 | |
| Roommates | 565 | 26.0 | |
| Partner or spouse | 301 | 13.9 | |
| Partner/spouse and children | 21 | 1.0 |
| Question | Answer | Number of Respondents | % of Respondents |
|---|---|---|---|
| Did you get COVID-19? | No | 2112 | 97.2 |
| Yes | 28 | 1.3 | |
| Did any of your relatives/friends get COVID-19? | No | 1943 | 89.5 |
| Yes, a family member | 52 | 2.4 | |
| Yes, a friend | 161 | 7.4 | |
| Did any of your relatives/friends die because of COVID-19? | No | 2142 | 98.6 |
| Yes, a family member | 12 | 0.6 | |
| Yes, a friend | 14 | 0.6 | |
| Are you actively joining the fight against the COVID-19 epidemic? | No | 1733 | 79.8 |
| Yes | 439 | 20.2 | |
| Did you use psychological/psychiatric help before the beginning of the pandemic? | No | 1800 | 82.9 |
| Yes, I used psychological support | 162 | 7.5 | |
| Yes, I used psychiatric support | 80 | 3.7 | |
| Yes, I used psychological and psychiatric support | 130 | 6.0 | |
| Do you take any supplements/medicines that increase immunity? | No | 1506 | 69.3 |
| Yes | 665 | 30.6 | |
| What was most difficult for you during the pandemic? | Changes awaiting the world after the pandemic | 440 | 20.3 |
| Change of the lifestyle | 265 | 12.2 | |
| Fear of being infected | 66 | 3.0 | |
| Fear of infection of the loved ones | 728 | 33.5 | |
| Financial instability | 149 | 6.9 | |
| Isolation | 211 | 9.7 | |
| Loneliness | 149 | 6.9 | |
| Do you have any chronic disease? | No | 1837 | 84.6 |
| Allergy | 32 | 1.5 | |
| Asthma | 54 | 2.5 | |
| Diabetes | 15 | 0.7 | |
| Mental disorders | 41 | 1.9 | |
| Thyroid diseases | 88 | 4.1 | |
| Other | 105 | 4.8 |
| Question | Answer | Number of Respondents | % of Respondents |
|---|---|---|---|
| Did you work before the pandemic outbreak? | I did not work | 1469 | 67.6 |
| I worked mentally | 356 | 16.4 | |
| I worked physically | 316 | 14.5 | |
| I ran my own business | 30 | 1.2 | |
| Do you work currently? | No, I do not work | 1799 | 82.8 |
| I work mentally | 249 | 11.5 | |
| I work physically | 96 | 4.4 | |
| I run my own business | 28 | 1.3 | |
| How do you assess your economic situation during the pandemic? | I have a stable family income, nothing has changed | 1278 | 58.8 |
| I have a stable family income, but the situation is worse than before | 647 | 29.8 | |
| I have to start using savings | 191 | 8.8 | |
| I have to borrow money from my family/friends during the outbreak of the pandemic because I do not have enough money to support myself | 21 | 1.0 | |
| I barely have enough money for living | 27 | 1.2 |
| Normal | Mild | Moderate | Severe | Extremely Severe | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | |
| Depression | 948 | 43.6 | 282 | 13 | 432 | 19.9 | 221 | 10.2 | 289 | 13.3 |
| Anxiety | 1307 | 60.2 | 273 | 12.5 | 195 | 9.0 | 144 | 6.6 | 253 | 11.7 |
| Stress | 1026 | 47.2 | 255 | 11.8 | 333 | 15.3 | 364 | 16.8 | 194 | 8.9 |
| Country | Poland | Spain | China | India | Bangladesh | ||
|---|---|---|---|---|---|---|---|
| Date of the start and closure of the survey | 20 April–26 April | 28 March–4 April | 31 January–2 February | 23 April–30 April | 11 April–24 April | ||
| The time that has from the confinement till the start of the survey | 6 weeks | 2 weeks | 3 days after the WHO announced COVID-19 as a public health emergency | One month | 2 weeks | ||
| Number of the respondents | 2172 | 3707 | 1210 | 500 | 3122 | ||
| Females (%) | 73 | 66.1 | 67.3 | 65 | 40.5 | ||
| Males (%) | 27 | 33.9 | 32.7 | 35 | 59.5 | ||
| Mean age/age range | 22.1 ± 2.2 | 27.9 ± 12.4 | 12–21.4—28.4% 21.4–30.8—53.2% 30.8–40.2—7.8% 40.2–49.6—7.4% 49.6–59—3.2% | 21.2 ± 1.3 | 21.4 ± 2 | ||
| Mean and SD of the DASS-21 total score ** | 38.13 ± 26.51 | ND | 20.16 ± 20.42 | ND | ND | ||
| DASS-21 (mean and SD for each of the subscales) *** | Depression | 14.04 ± 10.44 | 5.52 ± 4.92 | ND | ND | 17.4 ± 10.7 | |
| Anxiety | 7.71 ± 8.29 | 3.34 ± 3.87* | ND | ND | 13.8 ± 9.8 | ||
| Stress | 16.93 ± 10.98 | 6.81 ± 4.72 | ND | ND | 21.3 ± 11 | ||
| DASS-21 (% of the respondents with a particular degree of severity of depression, anxiety, and stress) | Depression | Normal | 43.6 | ND | 69.7 | 57.5 | 23.9 |
| Mild | 13.0 | 13.8 | 8.5 | 13.2 | |||
| Moderate | 19.9 | 12.2 | 8.0 | 27.7 | |||
| Severe | 10.2 | 4.3 * | 8.0 | 15.5 | |||
| Extremely severe | 13.3 | 18.0 | 19.7 | ||||
| Anxiety | Normal | 60.2 | 63.6 | 53.0 | 28.5 | ||
| Mild | 12.5 | 7.5 | 5.0 | 7.9 | |||
| Moderate | 9.0 | 20.4 | 10.5 | 23.3 | |||
| Severe | 6.6 | 8.4 * | 4.0 | 12.8 | |||
| Extremely severe | 11.7 | 27.5 | 27.5 | ||||
| Stress | Normal | 47.2 | 67.9 | 68.0 | 29.9 | ||
| Mild | 11.8 | 24.1 | 4.0 | 11.5 | |||
| Moderate | 15.3 | 5.5 | 9.0 | 20.9 | |||
| Severe | 16.8 | 2.6 * | 6.5 | 21.2 | |||
| Extremely severe | 8.9 | 12.5 | 16.5 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Juchnowicz, D.; Baj, J.; Forma, A.; Karakuła, K.; Sitarz, R.; Bogucki, J.; Karakula-Juchnowicz, H. The Outbreak of SARS-CoV-2 Pandemic and the Well-Being of Polish Students: The Risk Factors of the Emotional Distress during COVID-19 Lockdown. J. Clin. Med. 2021, 10, 944. https://doi.org/10.3390/jcm10050944
Juchnowicz D, Baj J, Forma A, Karakuła K, Sitarz R, Bogucki J, Karakula-Juchnowicz H. The Outbreak of SARS-CoV-2 Pandemic and the Well-Being of Polish Students: The Risk Factors of the Emotional Distress during COVID-19 Lockdown. Journal of Clinical Medicine. 2021; 10(5):944. https://doi.org/10.3390/jcm10050944
Chicago/Turabian StyleJuchnowicz, Dariusz, Jacek Baj, Alicja Forma, Kaja Karakuła, Ryszard Sitarz, Jacek Bogucki, and Hanna Karakula-Juchnowicz. 2021. "The Outbreak of SARS-CoV-2 Pandemic and the Well-Being of Polish Students: The Risk Factors of the Emotional Distress during COVID-19 Lockdown" Journal of Clinical Medicine 10, no. 5: 944. https://doi.org/10.3390/jcm10050944
APA StyleJuchnowicz, D., Baj, J., Forma, A., Karakuła, K., Sitarz, R., Bogucki, J., & Karakula-Juchnowicz, H. (2021). The Outbreak of SARS-CoV-2 Pandemic and the Well-Being of Polish Students: The Risk Factors of the Emotional Distress during COVID-19 Lockdown. Journal of Clinical Medicine, 10(5), 944. https://doi.org/10.3390/jcm10050944